
Using Design Thinking Principles to Improve Outpatients’ Experiences in Hospital Pharmacies: A Case Study of Two Hospitals in Asir Region, Saudi Arabia

 , ,
, ,
Abstract
:1. Introduction
2. Methodology
2.1. Stage I (Empathize)
2.2. Stage II (Define)
2.3. Stage III (Ideate)
2.4. Stage IV (Prototype)
2.5. Stage V: Testing (Validation with Collaborators)
3. Result
3.1. Stage I (Empathize) and Stage II (Define)
- Lack of a queue management system in hospital 2, causing improper queue management (Figure 3C).
- Lack of equity in waiting times between the two genders (more windows serving male patients than females) in hospital 1 (Figure 2C).
- Workflow inefficiencies through ordering and supplies; medicines are slow to arrive between physicians and pharmacies, and patients are using hand-written prescriptions in hospital 2 (lack of e-prescriptions) (Figure 3D).
3.2. Stage III (IDEATE) and Stage IV (Prototype)
- Software solutions:
- ○
- Introduce electronic-prescribing initiatives for physicians so they can communicate directly with the pharmacy in hospital 2
- ○
- Establish a queue management system in hospital 2.
- Interior design solutions:
- ○
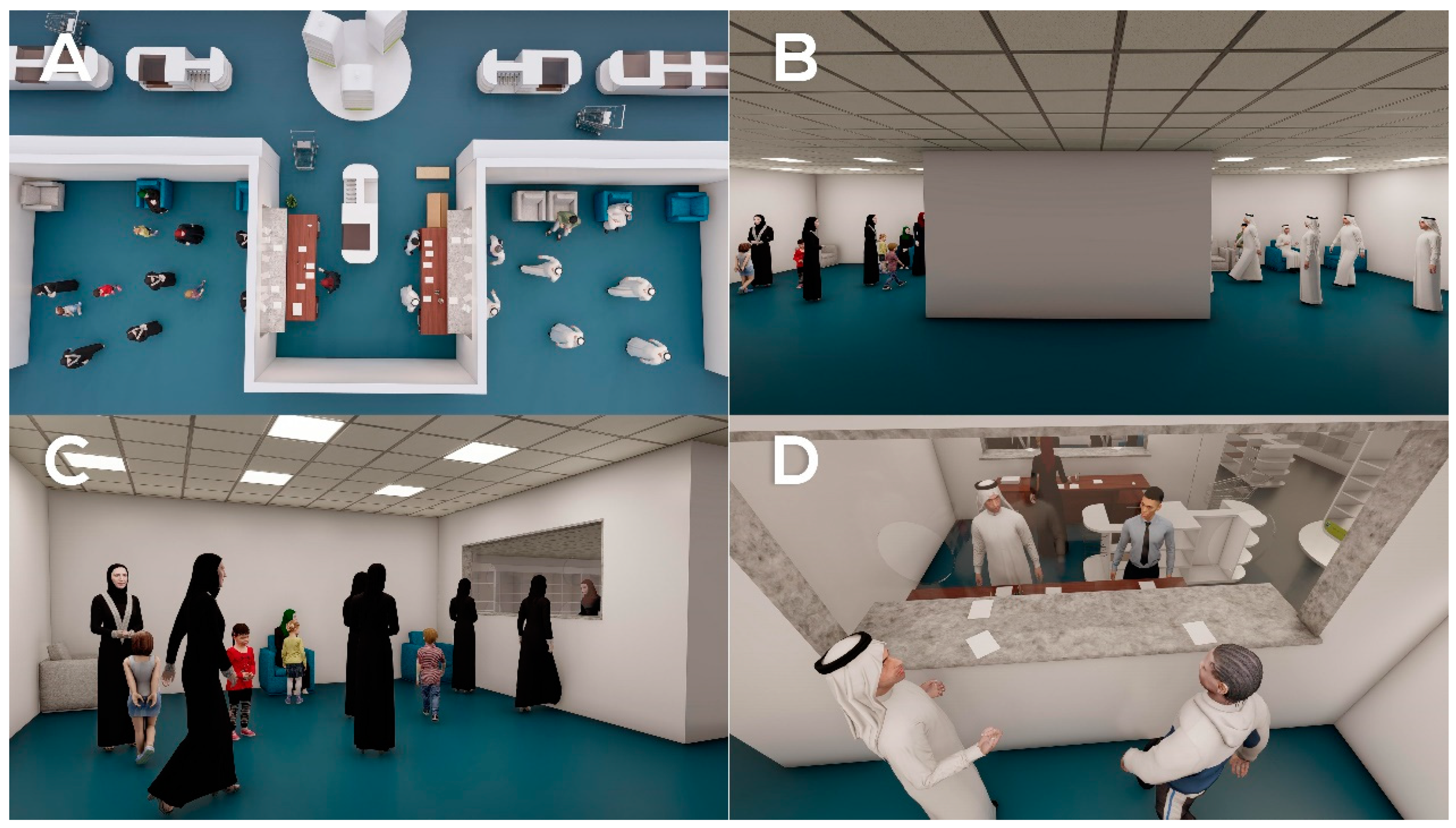
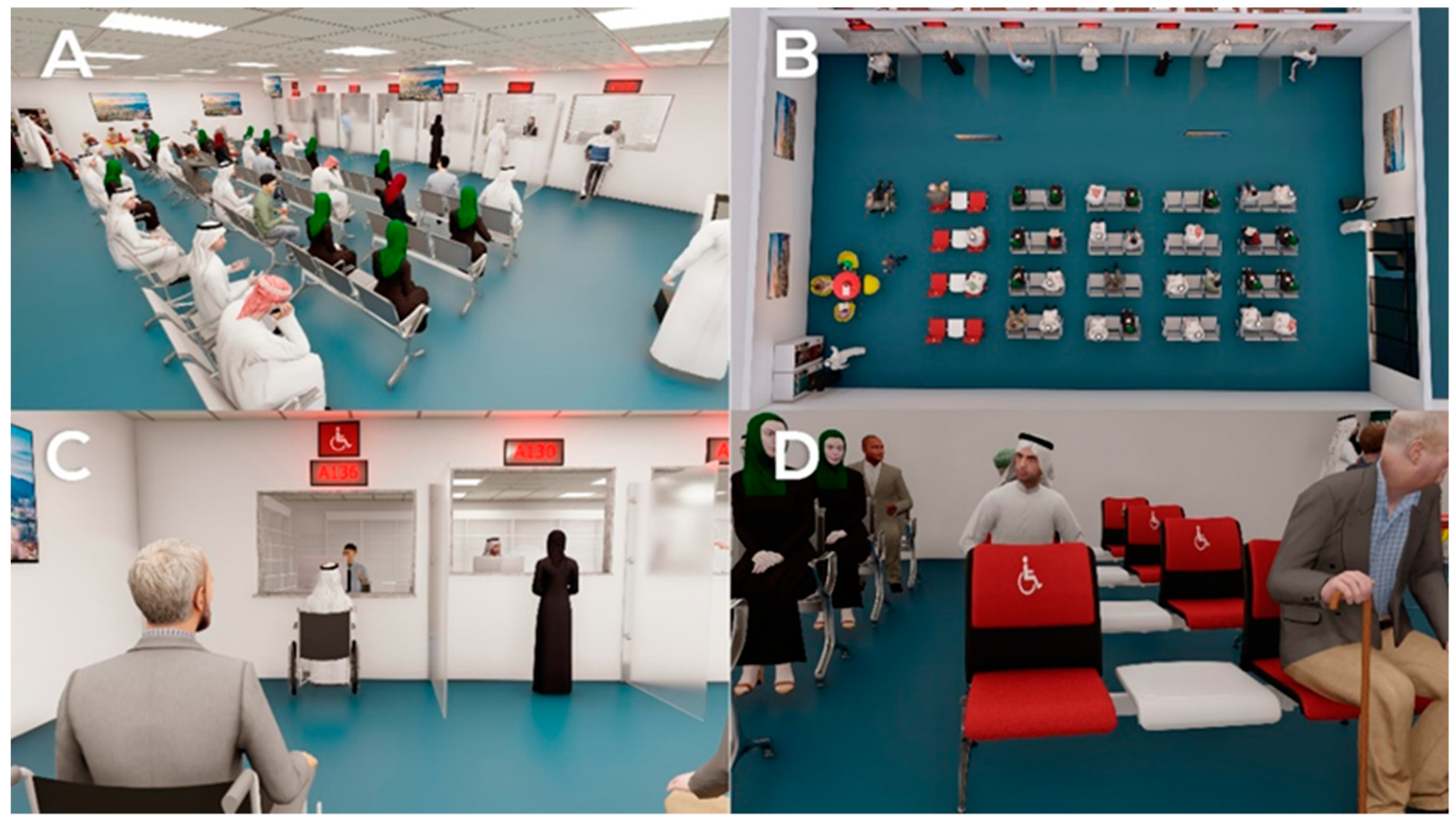
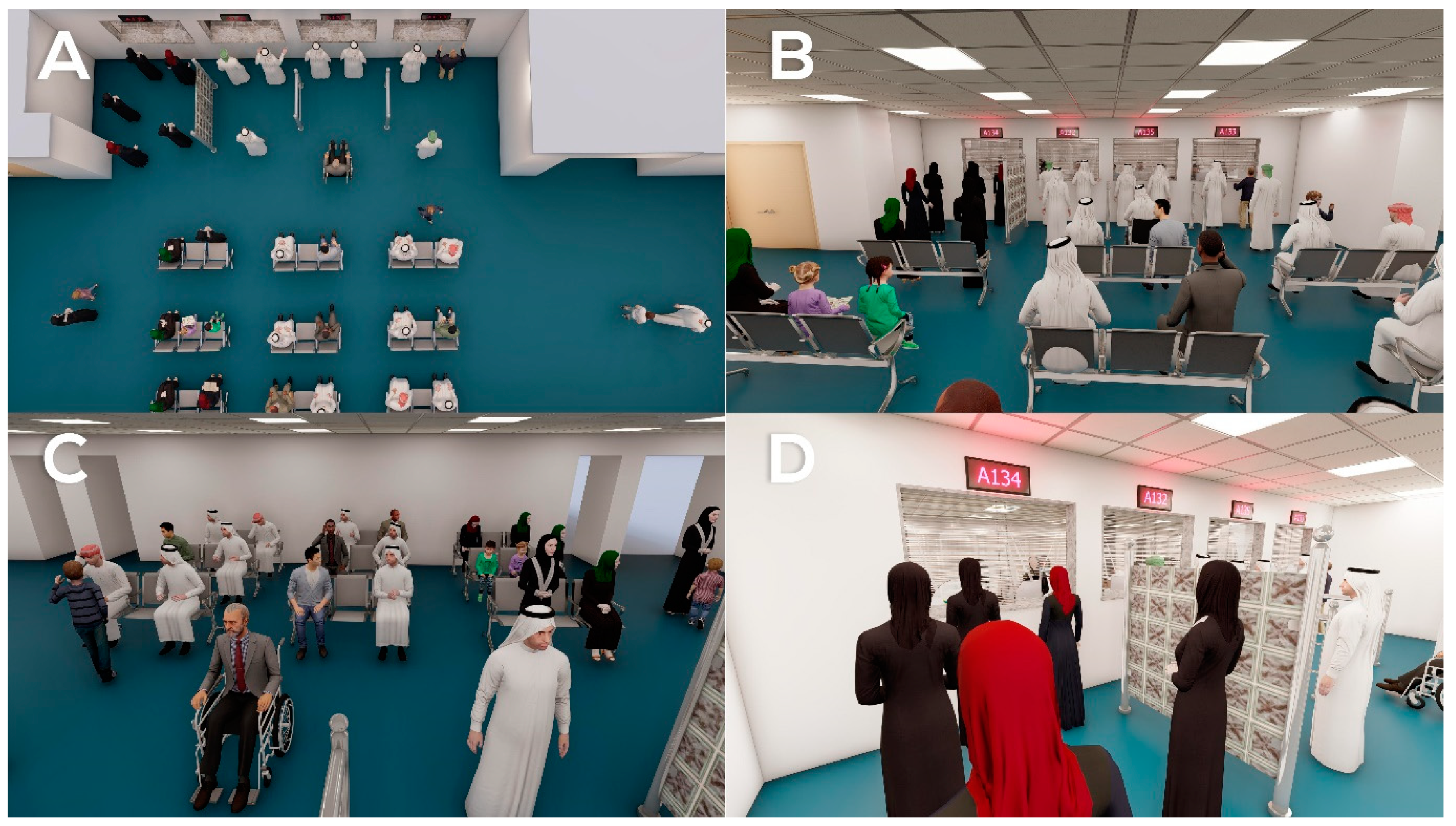
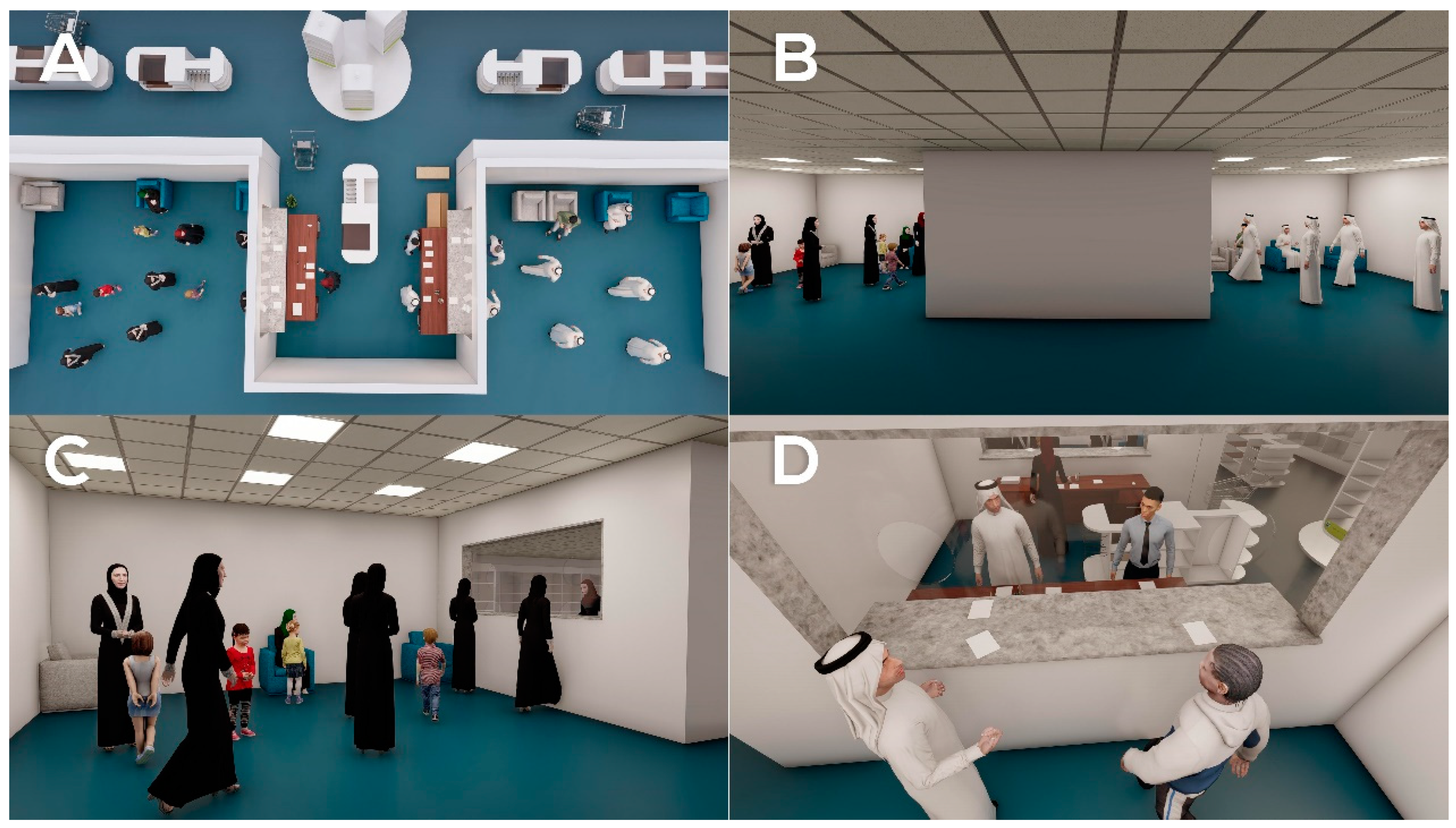
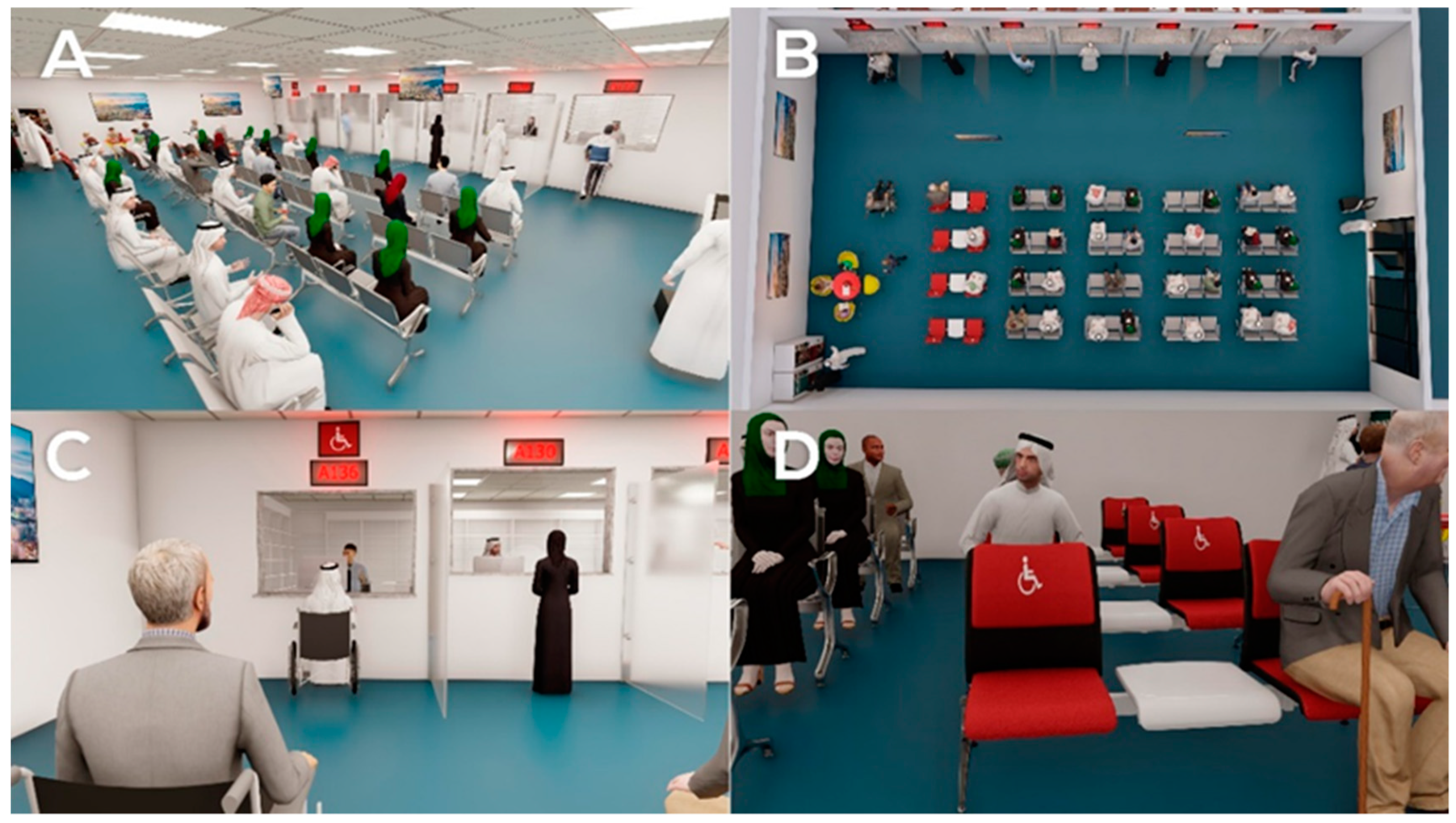
- Redesign the pharmacy waiting areas, increasing the number of seats allotted for female patients in both hospitals 1 and 2 (Figure 4A,B).
- ○
- Introduce adaptive arrangements for disabled patients (i.e., wheelchair accessible space in waiting rooms, dispensing windows to be height appropriate for wheelchair users in both hospitals (Figure 4C,D).
- ○
- Provide vending machines for refreshments in both hospitals (Figure 5A).
- ○
- Establish children’s corner in the waiting room in in both hospitals (Figure 5A).
- ○
- Provide TV screens in waiting rooms in both hospitals (Figure 5B).
- ○
- Brighten the dark waiting area in hospital 2 (Figure 4A,B).
- ○
- Provide partitions at the end of the counter (Figure 5C).
3.3. Stage V: Testing (Validation with Collaborators)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roberts, J.P.; Fisher, T.R.; Trowbridge, M.J.; Bent, C. A design thinking framework for healthcare management and innovation. Healthcare 2016, 4, 11–14. [Google Scholar] [CrossRef]
- Eines, T.F.; Vatne, S. Nurses and nurse assistants’ experiences with using a design thinking approach to innovation in a nursing home. J. Nurs. Manag. 2018, 26, 425–431. [Google Scholar] [CrossRef]
- Chan, K. A Design Thinking Mindset Beyond the Public Health Model. World Med. Heal. Policy 2018, 10, 111–119. [Google Scholar] [CrossRef]
- Valentine, L.; Kroll, T.; Bruce, F.; Lim, C.; Mountain, R. Design Thinking for Social Innovation in Health Care. Des. J. 2017. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, J.E.; Wolcott, M.D.; Hubbard, D.; Umstead, K.; Rider, T.R. A qualitative review of the design thinking framework in health professions education. BMC Med. Educ. 2019, 19, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taisuke, U.; Carl, K. Using design thinking to improve patient experiences in Japanese hospitals: A case study. J. Bus. Strategy 2009, 30, 6–12. [Google Scholar] [CrossRef]
- Kim, S.H.; Myers, C.G.; Allen, L. Health care providers can use design thinking to improve patient experiences. Harv. Bus. Rev. 2017. [Google Scholar]
- Chanpuypetch, W.; Kritchanchai, D. A design pattern for modelling and simulation in hospital pharmacy management. In Proceedings of the 31st European Conference on Modelling and Simulation, ECMS 2017, Budapest, Hungary, 23–26 May 2017. [Google Scholar]
- Yeager, D.S.; Romero, C.; Paunesku, D.; Hulleman, C.S.; Schneider, B.; Hinojosa, C.; Lee, H.Y.; Brien, J.O.; Flint, K.; Roberts, A.; et al. Using design thinking to improve psychological interventions: The case of the growth mindset during the transition to high school. J. Educ. Psychol. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, V.A.; Barr, K.L.C.; An, L.C.; Guajardo, C.; Newhouse, W.; Mase, R.; Heisler, M. Community-based participatory research and user-centered design in a diabetes medication information and decision tool. Prog. Community Heal. Partnersh. Res. Educ. Action 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, C.H.; Parsons, J.A.; Hall, S.; Newton, D.; Jovicic, A.; Lottridge, D.; Shah, B.R.; Straus, S.E. User-centered design of a web-based self-management site for individuals with type 2 diabetes—Providing a sense of control and community. BMC Med. Inform. Decis. Mak. 2014, 14, 60. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, R.S.; Girone, G. Design Thinking In Pharmacy Education: Inspiring Creative Problem Solving in the Next Generation of Pharmacists. Inov. Pharm. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Sabban, H.; Al-Jedai, A.; Bajis, D.; Penm, J. The Revised Basel Statements on the Future of Hospital Pharmacy: What Do They Mean for Saudi Arabia? Int. J. Pharm. Pract. 2018, 26, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Alsultan, M.S.; Khurshid, F.; Al-jedai, A.H.; Mayet, A.Y. Hospital pharmacy practice in Saudi Arabia: Dispensing and administration in the Riyadh region. Saudi Pharm. J. 2012, 20, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altyar, A.E.; Sadoun, S.A.; Alradadi, R.S.; Aljohani, S.S. Evaluating Pharmacy Practice in Hospital Settings in Jeddah City, Saudi Arabia: Prescribing and Transcribing—2018. Hosp. Pharm. 2019. [Google Scholar] [CrossRef] [PubMed]
- Alsultan, M.S.; Khurshid, F.; Salamah, H.J.; Mayet, A.Y.; Al-jedai, A.H. Hospital pharmacy practice in Saudi Arabia: Prescribing and transcribing in the Riyadh region. Saudi Pharm. J. 2012, 20, 203–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsultan, M.S.; Mayet, A.Y.; Khurshid, F.; Al-jedai, A.H. Hospital pharmacy practice in Saudi Arabia: Drug monitoring and patient education in the Riyadh region. Saudi Pharm. J. 2013, 21, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almaghaslah, D.; Alsayari, A.; Asiri, R.; Albugami, N. Pharmacy workforce in Saudi Arabia: Challenges and opportunities: A cross-sectional study. Int. J. Health Plann. Manag. 2018, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Jedai, A.; Qaisi, S.; Al-Meman, A. Pharmacy practice and the health care system in Saudi Arabia. Can. J. Hosp. Pharm. 2016, 69, 231. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Questions |
|---|---|
| 1 | How was your experience in the outpatient pharmacy today? Could you tell us more? |
| 2 | How were the services? Waiting area, waiting time etc.? |
| 3 | Can you elaborate? |
| 4 | How was the pharmacist? |
| 5 | Was there any particular thing that you liked/disliked? |
| 6 | How would your experience be better? |
| 7 | Out of ten, how would you rate the service today? |
| Hospitals and Participants Information | Hospital 1 | Hospital 2 |
|---|---|---|
| Hospital type | Government | Government |
| Level of expertise | General tertiary | Specialized |
| Number of beds | 600 | 300 |
| Number of interviews | 21 | 20 |
| Gender of participants | Male = 8 Female = 13 | Male = 8 Female = 12 |
| Age of participants | ||
| 20–29 | 4 | 2 |
| 30–39 | 6 | 8 |
| 40–49 | 3 | 4 |
| 50–59 | 4 | 3 |
| >60 | 4 | 3 |
| Reason for visiting | ||
| Patient | 18 | 6 |
| Caregiver | 3 | 13 |
| Visitor | - | 1 |
| End-User Prospective | Key Problem | Hospital | Key Management |
|---|---|---|---|
| Patient 10 (M) I suggest expanding the female waiting area as sometimes there are no seats inside the female designated area, so I have sat in the common seats with men around. Patient 4 (M) I wish there was a number waiting system Patient 15(A) The waiting area is overcrowded and full with patients sometimes. | Lack of queue management system, causing improper queue management and overcrowded waiting area. | Hospital 2 |
|
| Patient 14 (A) There is not enough space in the pharmacy waiting area, and there is only a single female dispensing windows. Patient 2 (A) There is only one window for females compared to three for males which makes the place packed with people. | Female patients experience of longer waiting times (lack of equity in waiting times between the two genders). | Hospital 1 |
|
| Patient 2 (M) There are not enough seats and the waiting area is gloomy and depressing. Patient 15(A) The waiting area is very small and cannot accommodate the large number of patients There are no refreshments or even drinking water. I would suggest adding TV screens and kids play corner to entertain patients while waiting for their prescriptions. Patient 16(A) There is no drinking water for me to take my medications while I’m here. Patient 4 (M) The chairs are wobbly and not in suitable condition, the room is dark. Patient 3 (M) It would be great to have free refreshments like tea or coffee. Patient 12 (M) There is not enough space for my son’s wheelchair. | Lack of comfortable environment in the pharmacies waiting area (limited seating, lack of refreshments, poor lighting, lack of adjustment for disabled patients) | Hospital 1, 2 |
|
| Patient 15 (M) I wish there was a direct communication between the physician and the pharmacist as well as number waiting system. Patient 4 (M) It would be great if electronic prescribing was implemented as it would reduce the medication errors, and order for prescription filling | Workflow inefficiencies through ordering and supply of medicines that is slow to arrive between physicians and pharmacists (lack of e-prescribing) | Hospital 2 |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almaghaslah, D.; Alsayari, A.; Alyahya, S.A.; Alshehri, R.; Alqadi, K.; Alasmari, S. Using Design Thinking Principles to Improve Outpatients’ Experiences in Hospital Pharmacies: A Case Study of Two Hospitals in Asir Region, Saudi Arabia. Healthcare 2021, 9, 854. https://doi.org/10.3390/healthcare9070854
Almaghaslah D, Alsayari A, Alyahya SA, Alshehri R, Alqadi K, Alasmari S. Using Design Thinking Principles to Improve Outpatients’ Experiences in Hospital Pharmacies: A Case Study of Two Hospitals in Asir Region, Saudi Arabia. Healthcare. 2021; 9(7):854. https://doi.org/10.3390/healthcare9070854
Chicago/Turabian StyleAlmaghaslah, Dalia, Abdulrhman Alsayari, Saleh Ali Alyahya, Rana Alshehri, Khawlah Alqadi, and Sumiah Alasmari. 2021. "Using Design Thinking Principles to Improve Outpatients’ Experiences in Hospital Pharmacies: A Case Study of Two Hospitals in Asir Region, Saudi Arabia" Healthcare 9, no. 7: 854. https://doi.org/10.3390/healthcare9070854
APA StyleAlmaghaslah, D., Alsayari, A., Alyahya, S. A., Alshehri, R., Alqadi, K., & Alasmari, S. (2021). Using Design Thinking Principles to Improve Outpatients’ Experiences in Hospital Pharmacies: A Case Study of Two Hospitals in Asir Region, Saudi Arabia. Healthcare, 9(7), 854. https://doi.org/10.3390/healthcare9070854