
Risk Scoring System of Mortality and Prediction Model of Hospital Stay for Critically Ill Patients Receiving Parenteral Nutrition

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. PN Administration
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Lewnard, J.A.; Liu, V.X.; Jackson, M.L.; Schmidt, M.A.; Jewell, B.L.; Flores, J.P.; Jentz, C.; Northrup, G.R.; Mahmud, A.; Reingold, A.L.; et al. Incidence, clinical outcomes, and transmission dynamics of severe coronavirus disease 2019 in California and Washington: Prospective cohort study. BMJ 2020, 369, m1923. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Li, S.; Fang, M.; Hu, M.; Bian, Y.; Ling, J.; Yu, S.; Jing, L.; Li, D.; Huang, J. Acute physiology and chronic health evaluation II score as a predictor of hospital mortality in patients of coronavirus disease 2019. Crit. Care Med. 2020, 48, e657–e665. [Google Scholar] [CrossRef] [PubMed]
- Halpern, N.A.; Pastores, S.M. Critical care medicine beds, use, occupancy, and costs in the United States: A methodological review. Crit. Care Med. 2015, 43, 2452–2459. [Google Scholar] [CrossRef]
- Bartsch, S.M.; Ferguson, M.C.; McKinnell, J.A.; O’Shea, K.J.; Wedlock, P.T.; Siegmund, S.S.; Lee, B.Y. The potential health care costs and resource use associated with COVID-19 in the United States. Health Aff. 2020, 39, 927–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rewa, O.G.; Stelfox, H.T.; Ingolfsson, A.; Zygun, D.A.; Featherstone, R.; Opgenorth, D.; Bagshaw, S.M. Indicators of intensive care unit capacity strain: A systematic review. Crit. Care 2018, 22, 86. [Google Scholar] [CrossRef] [Green Version]
- Ye, Y.; Zhu, B.; Jiang, L.; Jiang, Q.; Wang, M.; Hua, L.; Xi, X. A contemporary assessment of acute mechanical ventilation in Beijing: Description, costs, and outcomes. Crit. Care Med. 2017, 45, 1160–1167. [Google Scholar] [CrossRef] [Green Version]
- Lindemark, F.; Haaland, Ø.A.; Kvåle, R.; Flaatten, H.; Norheim, O.F.; Johansson, K.A. Costs and expected gain in lifetime health from intensive care versus general ward care of 30,712 individual patients: A distribution-weighted cost-effectiveness analysis. Crit. Care 2017, 21, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norris, C.; Jacobs, P.; Rapoport, J.; Hamilton, S. ICU and non-ICU cost per day. Can. J. Anaesth. 1995, 42, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Esperatti, M.; Fuentes, N.; Ferrer, M.; Ranzani, O.T.; Bassi, G.L.; Singer, M.; Gonzalez, M.E.; Peraita, G.; Urbano, M.S.; Torres, A. Association between sepsis at ICU admission and mortality in patients with ICU-acquired pneumonia: An infectious second-hit model. J. Crit. Care 2020, 59, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Moitra, V.K.; Guerra, C.; Linde-Zwirble, W.T.; Wunsch, H. Relationship between ICU length of stay and long-term mortality for elderly ICU survivors. Crit. Care Med. 2016, 44, 655–662. [Google Scholar] [CrossRef]
- Du, B.; An, Y.; Kang, Y.; Yu, X.; Zhao, M.; Ma, X.; Ai, Y.; Xu, Y.; Wang, Y.; Qian, C.; et al. Characteristics of critically ill patients in ICUs in mainland China. Crit. Care Med. 2013, 41, 84–92. [Google Scholar] [CrossRef]
- Thompson, K.; Venkatesh, B.; Finfer, S. Sepsis and septic shock: Current approaches to management. Intern. Med. J. 2019, 49, 160–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.; Gill, S.E. Improving clinical outcomes in sepsis and multiple organ dysfunction through precision medicine. J. Thorac. Dis. 2019, 11, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Godinjak, A.G.; Iglica, A.; Rama, A.; Tančica, I.; Jusufović, S.; Ajanović, A.; Kukuljac, A. Predictive value of SAPS II and APACHE II scoring systems for patient outcome in a medical intensive care unit. Acta Med. Acad. 2016, 4, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Chiang, H.-Y.; Huang, H.-C.; Chung, C.-W.; Yeh, Y.-C.; Chen, Y.-C.; Tien, N.; Lin, H.-S.; Ho, M.-W.; Kuo, C.-C. Risk prediction for 30-day mortality among patients with Clostridium difficile infections: A retrospective cohort study. Antimicrob. Resist. Infect. Control 2019, 8, 175. [Google Scholar] [CrossRef]
- Maslove, D.M.; Lamontagne, F.; Marshall, J.C.; Heyland, D.K. A path to precision in the ICU. Crit. Care 2017, 21, 79. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, F.R.; Safran, C.; Levkoff, S.E.; Minaker, K.L. Serum albumin level on admission as a predictor of death, length of stay, and readmission. Arch. Intern. Med. 1992, 152, 125–130. [Google Scholar] [CrossRef]
- Saha, I.; Paul, B. Essentials of Biostatistics & Research Methodology, 3rd ed.; Academic Publishers: Kolkata, India, 2020. [Google Scholar]
- Sprent, P. Statistics in medical research. Swiss Med. Wkly. 2003, 133, 522–529. [Google Scholar]
- Deo, R.C. Machine learning in medicine. Circulation 2015, 132, 1920–1930. [Google Scholar] [CrossRef] [Green Version]
- Knaus, W.A.; Wagner, D.P.; Draper, E.A.; Zimmerman, J.E.; Bergner, M.; Bastos, P.G.; Sirio, C.A.; Murphy, D.J.; Lotring, T.; Damiano, A.; et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest 1991, 100, 1619–1636. [Google Scholar] [CrossRef] [Green Version]
- Darabi, H.R.; Tsinis, D.; Zecchini, K.; Whitcomb, W.F.; Liss, A. Forecasting mortality risk for patients admitted to intensive care units using machine learning. Procedia Comput. Sci. 2018, 140, 306–313. [Google Scholar] [CrossRef]
- Moridani, M.K.; Setarehdan, S.K.; Nasrabadi, A.M.; Hajinasrollah, E. New algorithm of mortality risk prediction for cardiovascular patients admitted in intensive care unit. Int. J. Clin. Exp. Med. 2015, 8, 8916–8926. [Google Scholar]
- Ni, Y.-N.; Luo, J.; Yu, H.; Wang, Y.-W.; Hu, Y.-H.; Liu, D.; Liang, B.-M.; Liang, Z.-A. Can body mass index predict clinical outcomes for patients with acute lung injury/acute respiratory distress syndrome? A meta-analysis. Crit. Care 2017, 21, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinikainen, M.; Niskanen, M.; Uusaro, A.; Ruokonen, E. Impact of gender on treatment and outcome of ICU patients. Acta Anaesthesiol. Scand. 2005, 49, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.-W.; Kao, H.-K.; Yu, W.-K.; Lien, T.-C.; Chen, Y.-W.; Wang, J.-H.; Kou, Y.R. Synergistic impact of low serum albumin on intensive care unit admission and high blood urea nitrogen during intensive care unit stay on post-intensive care unit mortality in critically ill elderly patients requiring mechanical ventilation. Geriatr. Gerontol. Int. 2013, 13, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Minne, L.; Abu-Hanna, A.; de Jonge, E. Evaluation of SOFA-based models for predicting mortality in the ICU: A systematic review. Crit. Care 2008, 12, R161. [Google Scholar] [CrossRef] [Green Version]
- Haniffa, R.; Isaam, I.; De Silva, A.P.; Dondorp, A.M.; De Keizer, N.F. Performance of critical care prognostic scoring systems in low and middle-income countries: A systematic review. Crit. Care 2018, 22, 18. [Google Scholar] [CrossRef] [Green Version]
- Verburg, I.W.; Atashi, A.; Eslami, S.; Holman, R.; Abu-Hanna, A.; de Jonge, E.; Peek, N.; de Keizer, N.F. Which models can I use to predict adult ICU length of stay? A systematic review. Crit. Care Med. 2017, 45, e222–e231. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Chen, Y.X.; Guo, S.B.; Mei, X.; Yang, P. Predictive performance of quick Sepsis-related Organ Failure Assessment for mortality and ICU admission in patients with infection at the ED. Am. J. Emerg. Med. 2016, 34, 1788–1793. [Google Scholar] [CrossRef] [PubMed]
- van Beek, D.E.C.; Konigs, M.H.H.; Kuijpers, Y.A.M.; van der Horst, I.C.C.; Scheeren, T.W.L. Predictive value of serum albumin levels on noradrenaline and fluid requirements in the first 24h after admission to the Intensive Care Unit—A prospective observational study. J. Crit. Care 2018, 47, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Corti, M.C.; Guralnik, J.M.; Salive, M.E.; Sorkin, J.D. Serum albumin level and physical disability as predictors of mortality in older persons. JAMA 1994, 272, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.; Si, L.; Qin, W.; Li, C.; Zhang, J.; Yang, H.; Han, H.; Zhang, F.; Ding, S.; Zhou, M.; et al. Predictive value of serum albumin level for the prognosis of severe sepsis without exogenous human albumin administration: A prospective cohort study. J. Intensive Care Med. 2018, 33, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.J.; Taneja, A.; Niccum, D.; Kumar, G.; Jacobs, E.; Nanchal, R. The association of serum bilirubin levels on the outcomes of severe sepsis. J. Intensive Care Med. 2015, 30, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, M.F.; Soares, M.J.F.; Junior, J.A.M.; De Oliveira, M.A.B.; Faria, F.L.; Faveri, V.Z.; Iano, Y.; Guido, R.C. Predictive factors of long-term stay in the ICU after cardiac surgery: Logistic CASUS score, serum bilirubin dosage and extracorporeal circulation time. Braz. J. Cardiovasc. Surg. 2017, 32, 367–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nandivada, P.; Carlson, S.J.; Chang, M.I.; Cowan, E.; Gura, K.M.; Puder, M. Treatment of parenteral nutrition-associated liver disease: The role of lipid emulsions. Adv. Nutr. 2013, 4, 711–717. [Google Scholar] [CrossRef] [Green Version]
- Worthington, P.; Balint, J.; Bechtold, M.; Bingham, A.; Chan, L.-N.; Durfee, S.; Jevenn, A.K.; Malone, A.; Mascarenhas, M.; Robinson, D.T.; et al. When is parenteral nutrition appropriate? JPEN J. Parenter Enteral. Nutr. 2017, 41, 324–377. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total (n = 445) | Death (n = 97) | Survival (n = 348) | p |
|---|---|---|---|---|
| Sex | ||||
| Male | 280 (62.9) | 64 (66.0) | 216 (62.1) | 0.481 |
| Female | 165 (37.1) | 33 (34.0) | 132 (37.9) | |
| Age (years) | 64.1 ± 16.1 | 69.2 ± 15.1 | 62.6 ± 16.1 | <0.001 |
| APACHE II | 15.1 ± 7.9 | 19.4 ± 8.4 | 13.9 ± 7.3 | <0.001 |
| qSOFA | 0.6 ± 0.7 | 0.9 ± 0.9 | 0.5 ± 0.7 | <0.001 |
| Body weight (kg) | 61.5 ± 13.3 | 59.9 ± 12.1 | 62 ± 13.6 | 0.185 |
| Height (cm) | 163.6 ± 9.7 | 162.6 ± 9.3 | 163.8 ± 9.8 | 0.281 |
| BMI (kg/m2) | 22.9 ± 4.0 | 22.6 ± 3.8 | 23 ± 4.0 | 0.405 |
| Albumin (g/dL) | 3.7 ± 0.7 | 3.3 ± 0.8 | 3.8 ± 0.7 | <0.001 |
| ALT (U/L) | 45.4 ± 102.4 | 48.7 ± 90.1 | 44.4 ± 105.7 | 0.718 |
| AST (U/L) | 73.5 ± 169.4 | 87.9 ± 180.5 | 69.4 ± 166.2 | 0.341 |
| Creatinine clearance (mL/min) | 76.9 ± 47.4 | 68.7 ± 42.7 | 79.1 ± 48.4 | 0.056 |
| Total bilirubin (mg/dL) | 0.9 ± 0.9 | 1.0 ± 1.2 | 0.9 ± 0.8 | 0.339 |
| Number of comorbidities | 1.5 ± 1.2 | 1.6 ± 1.2 | 1.5 ± 1.2 | 0.232 |
| Previous surgery | ||||
| Yes | 205 (46.1) | 42 (43.3) | 163 (46.8) | 0.536 |
| No | 240 (53.9) | 55 (56.7) | 185 (53.2) | |
| EN treatment status † | ||||
| Yes | 51 (11.5) | 14 (14.4) | 37 (10.6) | 0.299 |
| No | 394 (88.5) | 83 (85.6) | 311 (89.4) | |
| Types of lipid emulsion | 0.510 | |||
| Olive oil-based | 230 (51.7) | 53 (54.6) | 177 (50.9) | |
| Fish oil-based | 215 (48.3) | 44 (45.4) | 171 (49.1) | |
| Admission diagnosis ‡ | ||||
| Cardiovascular disease | 0.440 | |||
| Yes | 171 (38.4) | 34 (35.1) | 137 (39.4) | |
| No | 274 (61.6) | 63 (64.9) | 211 (60.6) | |
| Respiratory disease | <0.001 | |||
| Yes | 57 (12.8) | 23 (23.7) | 34 (9.8) | |
| No | 388 (87.2) | 74 (76.3) | 314 (90.2) | |
| Gastrointestinal disease | 0.118 | |||
| Yes | 41 (9.2) | 5 (5.2) | 36 (10.3) | |
| No | 404 (90.8) | 92 (94.8) | 312 (89.7) | |
| Infectious disease | 0.017 | |||
| Yes | 14 (3.1) | 7 (7.2) | 7 (2.0) | |
| No | 431 (96.9) | 90 (92.8) | 341 (98.0) | |
| Genitourinary disease | 0.129 | |||
| Yes | 16 (3.6) | 6 (6.2) | 10 (2.9) | |
| No | 429 (96.4) | 91 (93.8) | 338 (97.1) | |
| Injury, poisoning, or other external cause | 0.395 | |||
| Yes | 82 (18.4) | 15 (15.5) | 67 (19.3) | |
| No | 363 (81.6) | 82 (84.5) | 281 (80.7) |
| Predictors | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | Attributable Risk (%) |
|---|---|---|---|
| Male | 1.185 (0.739–1.901) | ||
| Age ≥ 65 years | 1.901 (1.197–3.019) ** | ||
| APACHE II a | 2.845 (1.944–4.166) *** | 2.197 (1.464–3.297) *** | |
| qSOFA ≥ 2 | 3.429 (1.915–6.139) *** | 2.604 (1.393–4.869) ** | 61.6 |
| Albumin < 3.4 g/dL | 2.853 (1.783–4.565) *** | 1.787 (1.056–3.025) * | 44.0 |
| Admission diagnosis of respiratory or infectious disease | 3.353 (1.945–5.753) *** | 2.053 (1.111–3.793) *** | 51.3 |
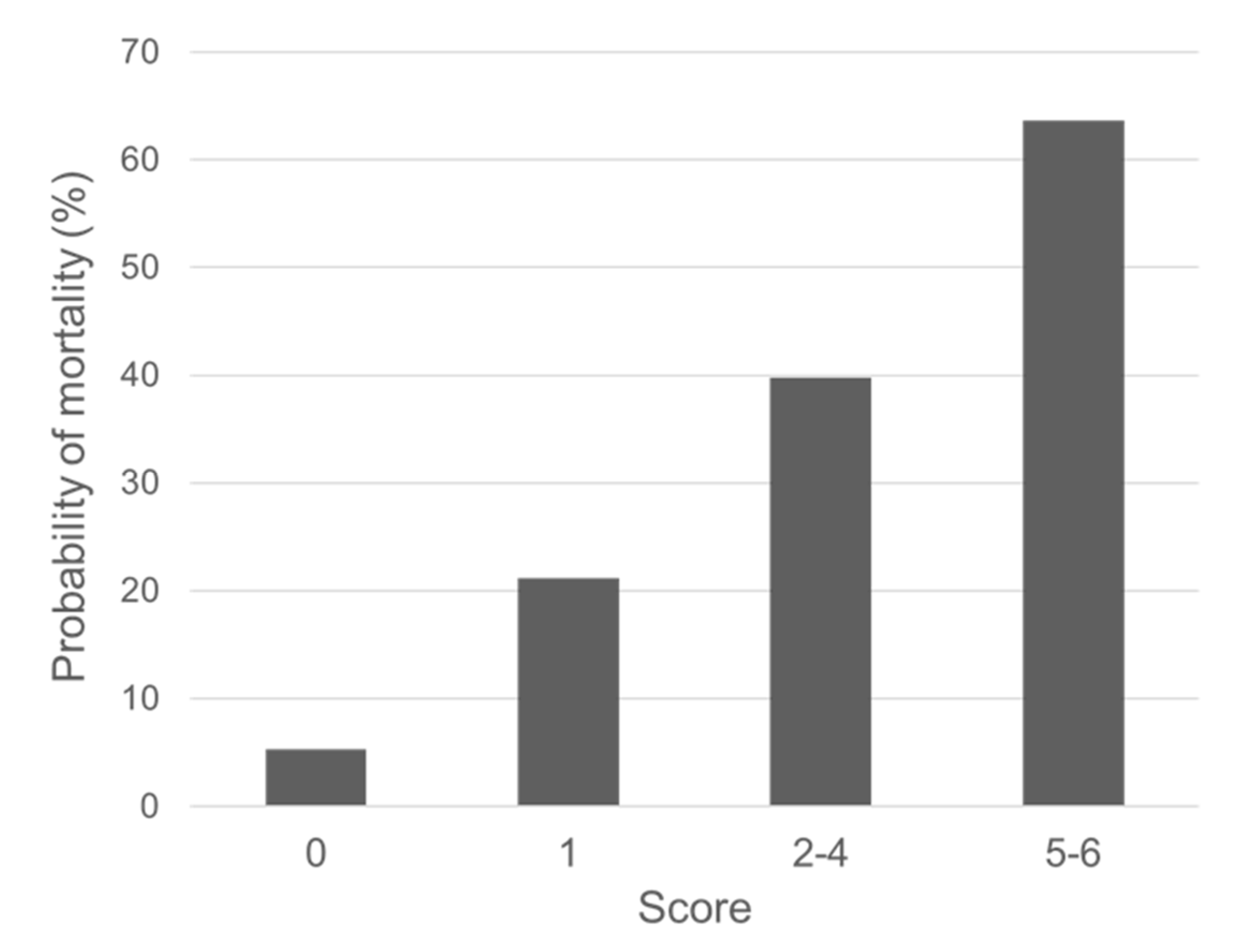
| Predictors | Beta Coefficient in Logistic Regression Model | Score |
|---|---|---|
| APACHE II | 0.787 | |
| 0–14 | 0 | |
| 15–29 | 1 | |
| ≥30 | 2 | |
| qSOFA ≥ 2 | 0.957 | 2 |
| Albumin < 3.4 g/dL | 0.581 | 1 |
| Admission diagnosis of respiratory or infectious disease | 0.719 | 1 |
| Total | 6 |
| Characteristics | N (%) | ICU Days (Mean ± SD) | p |
|---|---|---|---|
| Sex | 0.070 | ||
| Male | 280 (63.0) | 21.1 ± 24.0 | |
| Female | 165 (37.0) | 20.3 ± 25.8 | |
| Age (years) | 0.622 | ||
| ≥65 | 225 (50.5) | 19.6 ± 21.7 | |
| <65 | 220 (49.5) | 22.0 ± 27.2 | |
| APACHE II | < 0.001 | ||
| ≥15 | 201 (45.1) | 25.5 ± 29.3 | |
| <15 | 244 (54.9) | 16.9 ± 19.2 | |
| qSOFA | 0.204 | ||
| ≥2 | 57 (12.8) | 26.6 ± 38.1 | |
| <2 | 388 (87.2) | 20.0 ± 21.9 | |
| Body weight (kg) | 0.699 | ||
| ≥60 | 254 (57.0) | 20.3 ± 25.1 | |
| <60 | 191 (43.0) | 21.4 ± 23.9 | |
| Height (cm) | 0.156 | ||
| ≥165 | 224 (50.4) | 21.3 ± 24.7 | |
| <165 | 221 (49.6) | 20.3 ± 24.5 | |
| BMI (kg/m2) | 0.556 | ||
| ≥18.5 | 389 (87.4) | 20.8 ± 25.3 | |
| <18.5 | 56 (12.6) | 20.7 ± 19.4 | |
| Albumin (g/dL) | 0.004 | ||
| ≥3.4 | 319 (71.7) | 19.1 ± 21.4 | |
| <3.4 | 126 (28.3) | 25.1 ± 31.0 | |
| ALT (U/L) | 0.027 | ||
| ≥40 | 113 (25.4) | 21.9 ± 20.8 | |
| <40 | 332 (74.6) | 20.4 ± 25.8 | |
| AST (U/L) | 0.007 | ||
| ≥40 | 168 (37.8) | 23.6 ± 28.0 | |
| <40 | 277 (62.2) | 19.0 ± 22.2 | |
| Creatinine clearance (mL/min) | 0.354 | ||
| ≥30 | 382 (85.8) | 20.3 ± 24.3 | |
| <30 | 63 (14.2) | 23.8 ± 26.2 | |
| Total bilirubin (mg/dL) | 0.035 | ||
| ≥2 | 24 (5.5) | 36.1 ± 53.1 | |
| <2 | 421 (94.5) | 19.9 ± 21.7 | |
| Number of comorbidities | 0.150 | ||
| ≥2 | 192 (43.1) | 23.0 ± 29.3 | |
| <2 | 253 (56.9) | 19.1 ± 20.3 | |
| Previous surgery | 0.799 | ||
| Yes | 205 (46.1) | 21.1 ± 24.7 | |
| No | 240 (53.9) | 20.5 ± 24.6 | |
| EN treatment status † | 0.762 | ||
| Yes | 51 (11.5) | 20.0 ± 22.9 | |
| No | 394 (88.5) | 20.9 ± 24.9 | |
| Types of lipid emulsion | 0.609 | ||
| Olive oil-based | 230 (51.7) | 19.1 ± 19.8 | |
| Fish oil-based | 215 (48.3) | 22.6 ± 28.8 | |
| Admission diagnosis ‡ | |||
| Cardiovascular disease | 0.554 | ||
| Yes | 171 (38.4) | 19.8 ± 19.6 | |
| No | 274 (61.6) | 21.4 ± 27.3 | |
| Respiratory disease | 0.088 | ||
| Yes | 57 (12.8) | 20.2 ± 16.4 | |
| No | 388 (87.2) | 20.9 ± 25.6 | |
| Gastrointestinal disease | 0.022 | ||
| Yes | 41 (9.2) | 14.6 ± 16.6 | |
| No | 404 (90.8) | 21.4 ± 25.2 | |
| Infectious disease | 0.346 | ||
| Yes | 14 (3.1) | 20.9 ± 14.7 | |
| No | 431 (96.9) | 20.8 ± 24.9 | |
| Genitourinary disease | 0.712 | ||
| Yes | 16 (3.6) | 19.4 ± 17.7 | |
| No | 429 (96.4) | 20.8 ± 24.9 | |
| Injury, poisoning, or other external cause | 0.024 | ||
| Yes | 82 (18.4) | 18.1 ± 23.1 | |
| No | 363 (81.6) | 21.4 ± 24.9 |
| Predictors | Coefficient (SE) | t | p |
|---|---|---|---|
| Intercept | 0.970 (0.045) | 21.633 | <0.001 |
| APACHE II | 0.010 (0.002) | 4.543 | <0.001 |
| Total bilirubin (mg/dL) | 0.040 (0.019) | 2.146 | 0.032 |
| Admission diagnosis of gastrointestinal disease or injury, poisoning, or other external cause | −0.093 (0.039) | −2.366 | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-Y.; Yee, J.; Park, T.-I.; Shin, S.-Y.; Ha, M.-H.; Gwak, H.-S. Risk Scoring System of Mortality and Prediction Model of Hospital Stay for Critically Ill Patients Receiving Parenteral Nutrition. Healthcare 2021, 9, 853. https://doi.org/10.3390/healthcare9070853
Kim J-Y, Yee J, Park T-I, Shin S-Y, Ha M-H, Gwak H-S. Risk Scoring System of Mortality and Prediction Model of Hospital Stay for Critically Ill Patients Receiving Parenteral Nutrition. Healthcare. 2021; 9(7):853. https://doi.org/10.3390/healthcare9070853
Chicago/Turabian StyleKim, Jee-Yun, Jeong Yee, Tae-Im Park, So-Youn Shin, Man-Ho Ha, and Hye-Sun Gwak. 2021. "Risk Scoring System of Mortality and Prediction Model of Hospital Stay for Critically Ill Patients Receiving Parenteral Nutrition" Healthcare 9, no. 7: 853. https://doi.org/10.3390/healthcare9070853
APA StyleKim, J.-Y., Yee, J., Park, T.-I., Shin, S.-Y., Ha, M.-H., & Gwak, H.-S. (2021). Risk Scoring System of Mortality and Prediction Model of Hospital Stay for Critically Ill Patients Receiving Parenteral Nutrition. Healthcare, 9(7), 853. https://doi.org/10.3390/healthcare9070853