
Effects of Rehabilitation Exercise on Cardiovascular Risk Factors and Muscle Cross-Sectional Area in Overweight Patients with Low Back Pain



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Outcome Assessments
2.2.1. Body Composition
2.2.2. Blood Profile
2.2.3. Cross-Sectional Area
2.2.4. Oswestry Disability Index (ODI)
2.3. Rehabilitation Exercise Programs
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wasser, J.G.; Vasilopoulos, T.; Zdziarski, L.A.; Vincent, H.K. Exercise benefits for chronic low back pain in overweight and obese individuals. PM R 2017, 9, 181–192. [Google Scholar] [CrossRef]
- Han, T.S.; Schouten, J.S.; Lean, M.E.; Seidell, J.C. The prevalence of low back pain and associations with body fatness, fat distribution and height. Int. J. Obes. Relat. Metab. Disord. 1997, 21, 600–607. [Google Scholar] [CrossRef] [Green Version]
- Kostova, V.; Koleva, M. Back disorders (low back pain, cervicobrachial and lumbosacral radicular syndromes) and some related risk factors. J. Neurol. Sci. 2001, 192, 17–25. [Google Scholar] [CrossRef]
- Jensen, G.L.; Friedmann, J.M. Obesity is associated with functional decline in community- dwelling rural older persons. J. Am. Geriatr. Soc. 2002, 50, 918–923. [Google Scholar] [CrossRef]
- Srdic, B.; Stokic, E.; Babovic, S.; Polzovic, A.; Vlaskalic, Z. Variations in body fat mass in normally fed individuals. Bull. Anthropol. Soc. Yugosl. 2006, 41, 429–437. [Google Scholar]
- Roubenoff, R. Sarcopenia and its implications for the elderly. Eur. J. Clin. Nutr. 2000, 54, S40–S47. [Google Scholar] [CrossRef]
- França, F.R.; Burke, T.N.; Hanada, E.S.; Marques, A.P. Segmental stabilization and muscular strengthening in chronic low back pain: A comparative study. Clinics 2010, 65, 1013–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, P.M.; Keating, J.L. The epidemiology of low back pain in primary care. Chiropr. Osteopat. 2005, 13, 13. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.D.; Han, G.S. Effects of rehabilitation exercise on the body composition, lumbar extension strength, ratio of lumbar flexion/extension and VAS change in female low back pain patient of abdominal obesity. J. Coach. Dev. 2014, 16, 93–103. [Google Scholar]
- Baena-Beato, P.Á.; Artero, E.G.; Arroyo-Morales, M.; Robles-Fuentes, A.; Gatto-Cardia, M.C.; Delgado-Fernández, M. Aquatic therapy improves pain, disability, quality of life, body composition and fitness in sedentary adults with chronic low back pain. A controlled clinical trial. Clin. Rehabil. 2014, 28, 350–360. [Google Scholar] [CrossRef]
- Irandoust, K.; Taheri, M. The effects of aquatic exercise on body composition and nonspecific low back pain in elderly males. J. Phys. Ther. Sci. 2015, 27, 433–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danneels, L.A.; Vanderstraeten, G.G.; Cambier, D.C.; Witvrouw, E.E.; Bourgois, J.; Dankaerts, W.; de Cuyper, J.H. Effects of three different training modalities on the cross-sectional area of the lumbar multifidus muscle in patients with chronic low back pain. Br. J. Sports Med. 2001, 35, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Koumantakis, G.A.; Watson, P.J.; Oldham, J.A. Trunk muscle stabilization training plus general exercise versus general exercise only: Randomized controlled trial of patients with recurrent low back pain. Phys. Ther. 2005, 85, 209–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicholas, M.; Wilson, P.; Goyen, J. Comparison of cognitive-behavioral group treatment and an alternative non-psychological treatment for chronic low back pain. Pain 1992, 48, 339–347. [Google Scholar] [CrossRef]
- Hansen, F.; Bendix, T.; Skov, P.; Jensen, C.V.; Kristensen, J.H.; Krohn, L.; Schioeler, H. Intensive, dynamic back-muscle exercises, conventional physiotherapy, or placebo-control treatment of low-back pain: A randomized, observer-blind trial. Spine 1993, 18, 98–108. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pi-Sunyer, F.X. Obesity: Criteria and classification. Proc. Nutr. Soc. 2000, 59, 505–509. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of concentration of low-density lipoprotein cholesterol in plasma without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and B-cell function from fasting plasma glucose and insulin concentration in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2953. [Google Scholar] [CrossRef]
- Akuthota, V.; Ferreiro, A.; Moore, T.; Fredericson, M. Core stability exercise principles. Curr. Sports Med. Rep. 2008, 7, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Mills, J.D.; Taunton, J.E.; Mills, W.A. The effect of a 10-week training regimen on lumbo-pelvic stability and athletic performance in female athletes: A randomized-controlled trial. Phys. Ther. Sport 2005, 6, 60–66. [Google Scholar] [CrossRef]
- Felson, D.T. Weight and osteoarthritis. Am. J. Clin. Nutr. 1996, 63, 430S–432S. [Google Scholar] [CrossRef] [Green Version]
- Bowerman, S.; Bellman, M.; Saltsman, P.; Garvey, D.; Pimstone, K.; Skootsky, S.; Wang, J.H.; Elashoff, R.; Heber, D. Implementation of a primary care physician network obesity management program. Obes. Res. 2001, 9, 321S–325S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.E.; Kim, J.W.; Seo, H.K. The effects of pain, lumbar flexibility and abdominal obesity of patient with low back pain and abdominal obesity after lumbar strengthening exercise. Korean J. Orthop. Manu. Ther. 2009, 15, 25–34. [Google Scholar]
- Arad, Y.; Newstein, D.; Cadet, F.; Roth, M.; Guerci, A.D. Association of multiple risk factors and insulin resistance with increased prevalence of asymptomatic coronary artery disease by an electron-beam computed tomographic study. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 2051–2058. [Google Scholar] [CrossRef] [Green Version]
- Melissas, J.; Volakakis, E.; Hadjipavlou, A. Low-back pain in morbidly obese patients and the effect of weight loss following surgery. Obes. Surg. 2003, 13, 389–393. [Google Scholar] [CrossRef]
- Boardley, D.; Fahlman, M.; Topp, R.; Morgan, A.L.; McNevin, N. The impact of exercise training on blood lipids in older adults. Am. J. Geriatr. Cardiol. 2007, 16, 30–35. [Google Scholar] [CrossRef]
- Choi, E.Y. The association of low back pain with obesity and abdominal obesity among Koreans aged 50 years or more. Korean J. Health Promot. 2018, 18, 119–126. [Google Scholar] [CrossRef]
- Silfies, S.P.; Squillante, D.; Maurer, P.; Westcott, S.; Karduna, A.R. Trunk muscle recruitment patterns in specific chronic low back pain populations. Clin. Biomech. 2005, 20, 465–473. [Google Scholar] [CrossRef]
- Kim, C.H.; Kim, W.M.; Lee, H.W. Effects of 8 weeks lumbar stabilization program on the muscle’s cross-sectional area, pain and dynamic balancing capability of patients with lumbar disk herniation. Korean J. Phys. Educ. 2012, 51, 451–461. [Google Scholar]
- Barker, K.L.; Shamley, D.R.; Jackson, D. Changes in the cross-sectional area of multifidus and psoas in patients with unilateral back pain: The relationship to pain and disability. Spine 2004, 29, E515–E519. [Google Scholar] [CrossRef]
- Motta, M.H.; Santos, T.M.; Alencar, G.G.; Freitas, R.K.; Siqueira, G.R. Association between body composition and fat infiltration in the lumbar multifidus in young adults. Rev. Bras. Med. Esporte 2020, 26, 39–42. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, D.J.; Erskine, R.M.; Winwood, K.; Morse, C.I.; Onambele, G.L. The impact of obesity on skeletal muscle architecture in untrained young vs. old women. J. Anat. 2014, 225, 675–684. [Google Scholar] [CrossRef]
- Urquhart, D.M.; Berry, P.; Wluka, A.E.; Strauss, B.J.; Wang, Y.; Proietto, J.; Jones, G.; Dixon, J.B.; Cicuttini, F.M. 2011 Young Investigator Award winner: Increased fat mass is associated with high levels of low back pain intensity and disability. Spine 2011, 36, 1320–1325. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.G.; Holli, S.; Jayson, M.I. Gender variation of human spinal and paraspinal structures. Clin. Biomech. 1992, 7, 120–124. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Rehabilitation Exercise Program | |||
|---|---|---|---|
| Exercise Types | Exercise Modes | Time | Intensity |
| Warm-up | Stretching for upper and lower body | 5 min | RPE (10–13) |
| Main exercise (Phase 1) | Abdominal bracing | 30 min | RPE (13–15) 20–30 reps 3 sets |
| Bracing with bridge exercise in supine position | |||
| Bracing with side bridge exercise in side lying position | |||
| Bracing with bird dog exercise in quadruped position | |||
| Bracing with sit-up exercise in supine position | |||
| Main exercise (Phase 2) | Front plank with knees extended | 30 min | RPE (13–15) 20–30 reps 3 sets |
| Side plank with knees extended | |||
| Upper/lower back extension exercise in prone position | |||
| Transverse plane core exercise in standing position | |||
| Step-up in standing position | |||
| Cool-down | Stretching for upper and lower body | 5 min | |
| Characteristics | OLG | NLG | p-Value |
|---|---|---|---|
| Numbers | 14 | 15 | – |
| Sex (female/male) | 14/0 | 15/0 | – |
| Age (years) | 40.29 ± 2.89 | 40.13 ± 3.45 | 0.709 |
| Height (cm) | 158.18 ± 5.25 | 160.95 ± 5.08 | 0.160 |
| Weight (kg) | 64.13 ± 6.95 | 61.56 ± 4.23 | 0.235 |
| ODI (score) | 26.0 ± 3.26 | 24.0 ± 2.88 | 0.091 |
| BMI (kg/m2) | 26.62 ± 1.50 | 23.83 ± 0.81 | 0.000 *** |
| Variables | Group | Pre | Post | t-Value | p-Value |
|---|---|---|---|---|---|
| Body weight (kg) | OLG | 64.13 ± 6.95 | 61.79 ± 6.30 | 5.232 | 0.000 *** |
| NLG | 61.27 ± 4.23 | 60.41 ± 3.82 | 1.578 | 0.137 | |
| Body mass index (kg/m2) | OLG | 26.62 ± 1.50 | 25.12 ± 1.71 | 5.916 | 0.000 *** |
| NLG | 23.83 ± 0.81 | 23.46 ± 0.76 | 1.721 | 0.107 | |
| Body fat percentage (%) | OLG | 35.72 ± 3.15 | 33.51 ± 3.00 | 6.101 | 0.000 *** |
| NLG | 27.41 ± 2.97 | 27.00 ± 2.91 | 2.357 | 0.034 * | |
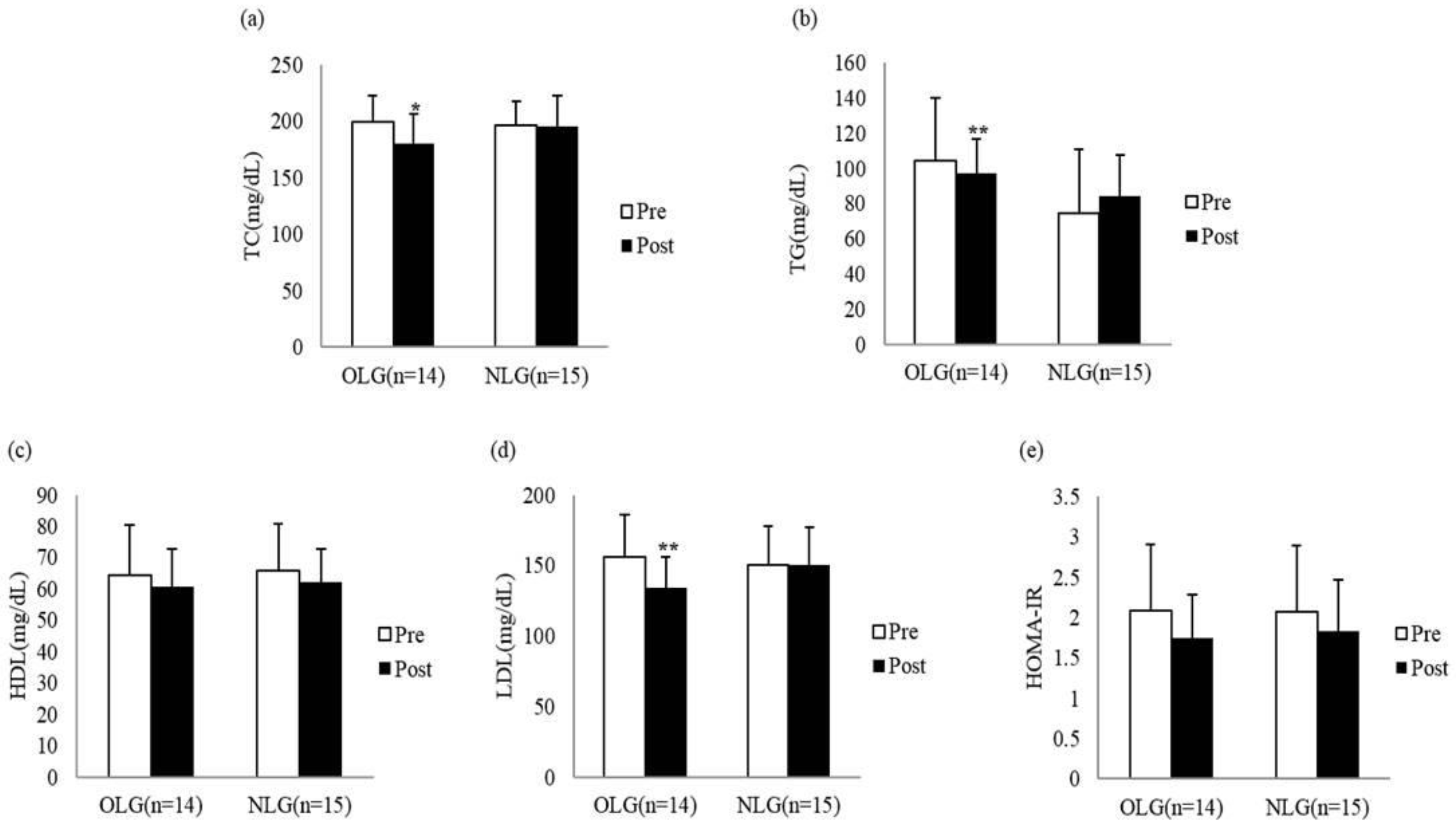
| Total cholesterol (mg/dL) | OLG | 199.24 ± 23.22 | 180.29 ± 21.71 | 2.863 | 0.013 * |
| NLG | 199.07 ± 24.74 | 197.71 ± 27.17 | 0.205 | 0.840 | |
| Triglyceride (mg/dL) | OLG | 104.64 ± 35.29 | 74.57 ± 19.97 | 3.829 | 0.002 ** |
| NLG | 96.87 ± 36.32 | 84.07 ± 23.22 | 1.386 | 0.187 | |
| HDL (mg/dL) | OLG | 64.50 ± 15.94 | 60.71 ± 11.96 | 0.906 | 0.381 |
| NLG | 65.80 ± 15.13 | 62.20 ± 10.67 | 1.488 | 0.159 | |
| LDL (mg/dL) | OLG | 155.64 ± 30.47 | 134.49 ± 21.92 | 3.794 | 0.002 ** |
| NLG | 150.04 ± 27.79 | 150.15 ± 26.54 | −0.020 | 0.984 | |
| HOMA-IR | OLG | 2.09 ±0.82 | 1.74 ± 0.54 | 1.939 | 0.075 |
| NLG | 2.07 ± 0.82 | 1.83 ± 0.64 | 1.249 | 0.232 | |
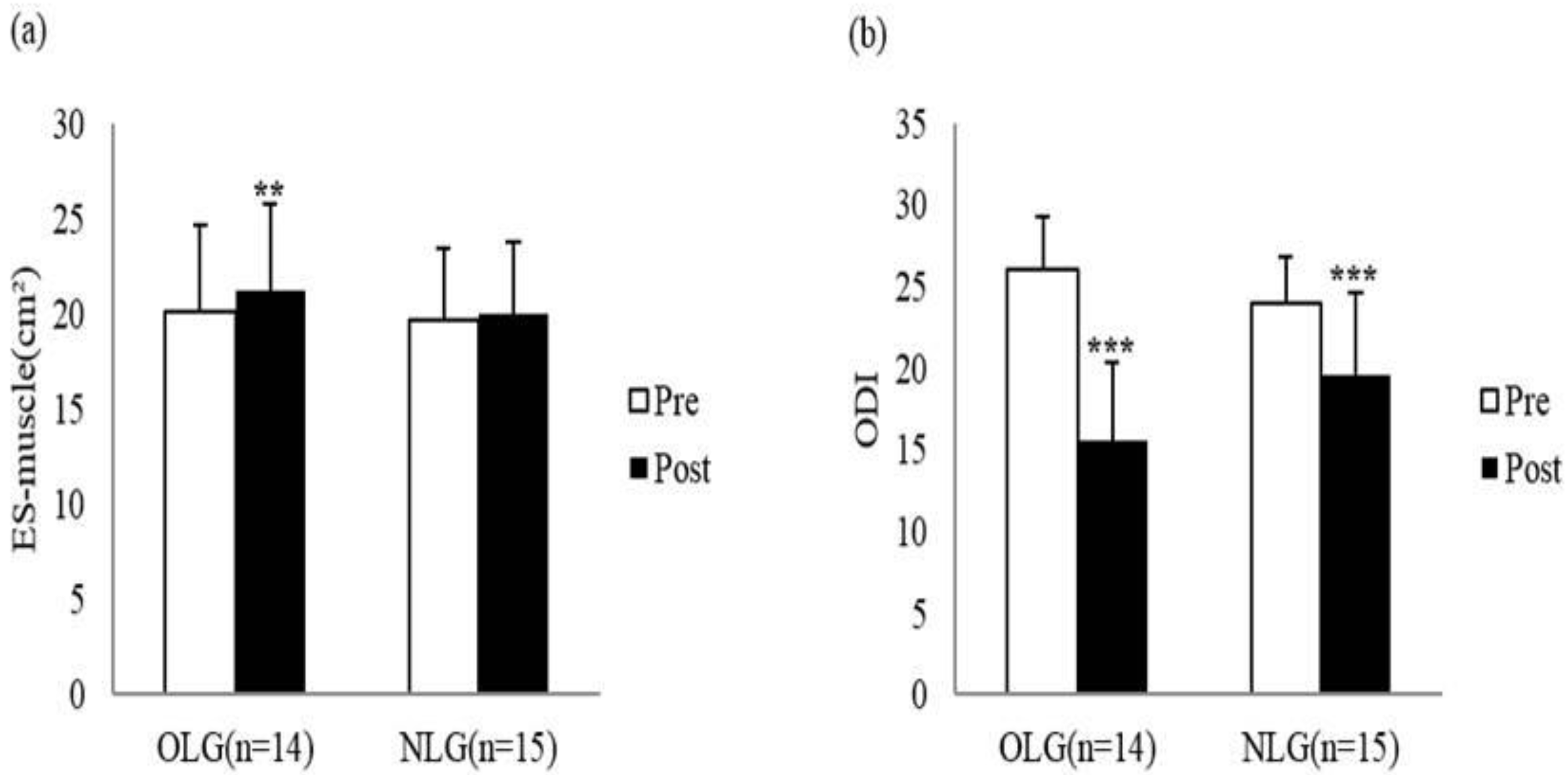
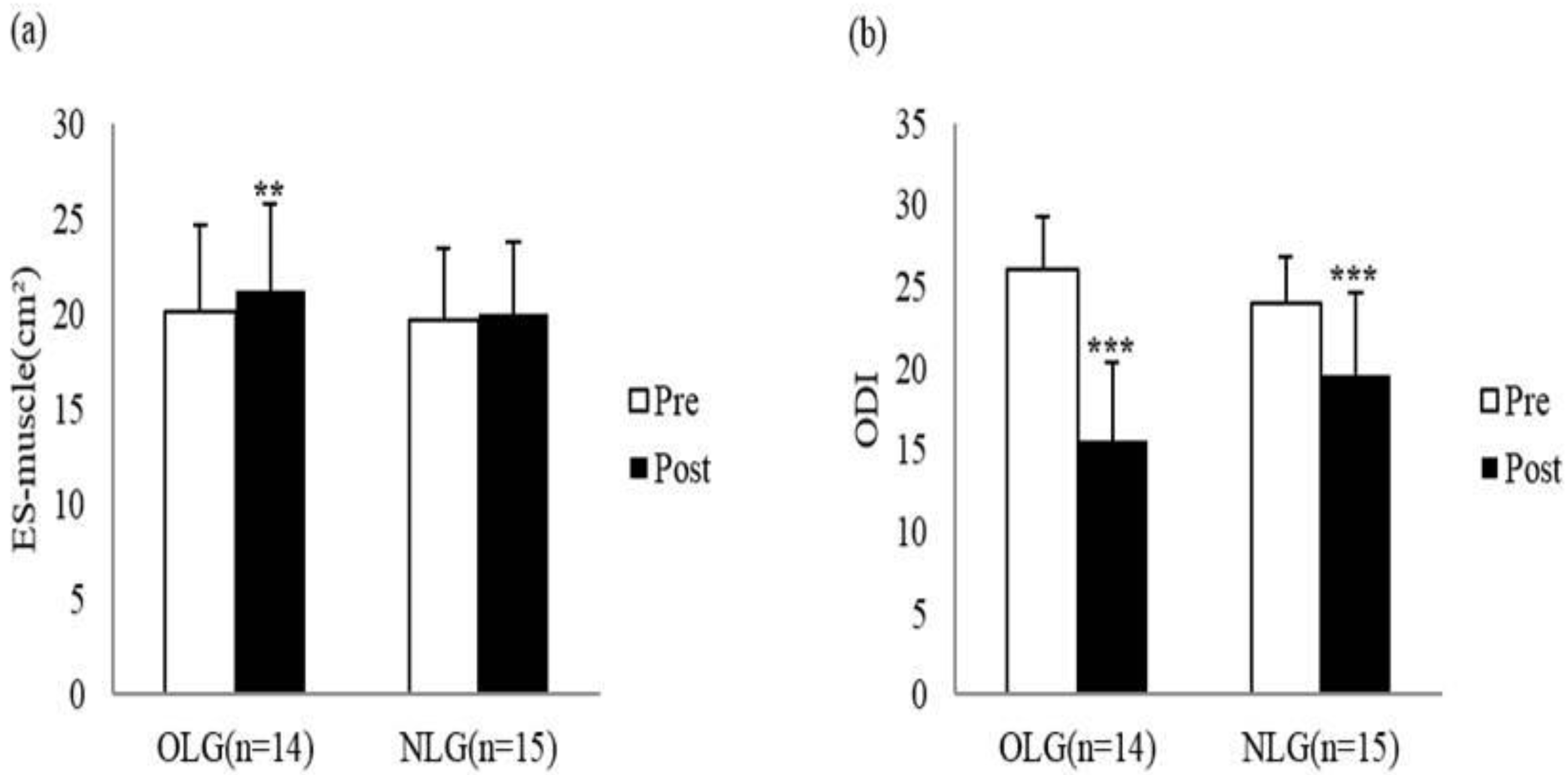
| Lumbar CSA (cm2) | OLG | 20.16 ± 4.48 | 21.25 ± 4.74 | −3.623 | 0.003 ** |
| NLG | 19.71 ± 3.68 | 20.01 ± 3.77 | −0.814 | 0.429 | |
| ODI (score) | OLG | 26.00 ± 3.25 | 15.57 ± 4.78 | 10.013 | 0.000 *** |
| NLG | 24.14 ± 2.93 | 19.50 ± 5.25 | 5.399 | 0.000 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, W.-M.; Lee, S.-A.; Park, Y.-J.; Seo, Y.-G. Effects of Rehabilitation Exercise on Cardiovascular Risk Factors and Muscle Cross-Sectional Area in Overweight Patients with Low Back Pain. Healthcare 2021, 9, 809. https://doi.org/10.3390/healthcare9070809
Kim W-M, Lee S-A, Park Y-J, Seo Y-G. Effects of Rehabilitation Exercise on Cardiovascular Risk Factors and Muscle Cross-Sectional Area in Overweight Patients with Low Back Pain. Healthcare. 2021; 9(7):809. https://doi.org/10.3390/healthcare9070809
Chicago/Turabian StyleKim, Won-Moon, Su-Ah Lee, Yun-Jin Park, and Yong-Gon Seo. 2021. "Effects of Rehabilitation Exercise on Cardiovascular Risk Factors and Muscle Cross-Sectional Area in Overweight Patients with Low Back Pain" Healthcare 9, no. 7: 809. https://doi.org/10.3390/healthcare9070809
APA StyleKim, W.-M., Lee, S.-A., Park, Y.-J., & Seo, Y.-G. (2021). Effects of Rehabilitation Exercise on Cardiovascular Risk Factors and Muscle Cross-Sectional Area in Overweight Patients with Low Back Pain. Healthcare, 9(7), 809. https://doi.org/10.3390/healthcare9070809