
A Simple Bedside Exercise Method to Enhance Lower Limb Muscle Strength in Moderate Alzheimer’s Disease Patients with Sarcopenia



Abstract
1. Introduction
2. Methods
2.1. Subjects
2.2. Study Design
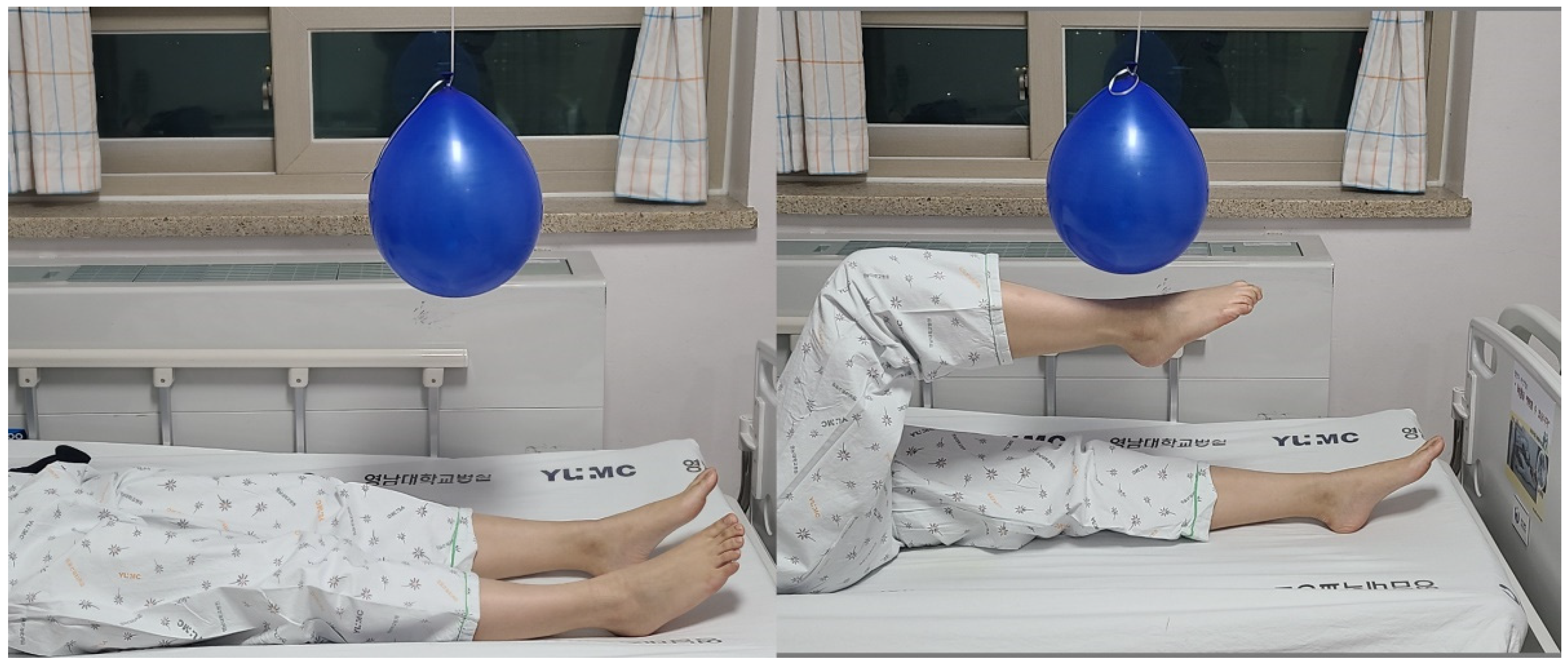
2.3. Exercise (Kicking a Ballon)
2.4. Muscle Strength Evaluation
2.5. Body Composition
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferretti, M.T.; Martinkova, J.; Biskup, E.; Benke, T.; Gialdini, G.; Nedelska, Z.; Rauen, K.; Mantua, V.; Religa, D.; Hort, J.; et al. Sex and gender differences in Alzheimer’s disease: Current challenges and implications for clinical practice: Position paper of the Dementia and Cognitive Disorders Panel of the European Academy of Neurology. Eur. J. Neurol. 2020, 27, 928–943. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Won, C.W. Sarcopenia Is Associated with Cognitive Impairment Mainly Due to Slow Gait Speed: Results from the Korean Frailty and Aging Cohort Study (KFACS). Int. J. Environ. Res. Public Health 2019, 16, 1491. [Google Scholar] [CrossRef]
- Moon, Y.; Moon, W.J.; Kim, J.O.; Kwon, K.J.; Han, S.H. Muscle Strength Is Independently Related to Brain Atrophy in Patients with Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. 2019, 47, 306–314. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Chang, M.C.; Lee, A.Y.; Kwak, S.; Kwak, S.G. Effect of Resistance Exercise on Depression in Mild Alzheimer Disease Patients With Sarcopenia. Am. J. Geriatr. Psychiatry 2020, 28, 587–589. [Google Scholar] [CrossRef]
- Yoo, S.Z.; No, M.H.; Heo, J.W.; Park, D.H.; Kang, J.H.; Kim, S.H.; Kwak, H.B. Role of exercise in age-related sarcopenia. J. Exerc. Rehabil. 2018, 14, 551–558. [Google Scholar] [CrossRef]
- Ziaaldini, M.M.; Marzetti, E.; Picca, A.; Murlasits, Z. Biochemical Pathways of Sarcopenia and Their Modulation by Physical Exercise: A Narrative Review. Front. Med. 2017, 4, 167. [Google Scholar] [CrossRef]
- Eyigor, S.; Karapolat, H.; Durmaz, B. Effects of a group-based exercise program on the physical performance, muscle strength and quality of life in older women. Arch. Gerontol. Geriatr. 2007, 45, 259–271. [Google Scholar] [CrossRef]
- Ferrucci, L.; Guralnik, J.M.; Buchner, D.; Kasper, J.; Lamb, S.E.; Simonsick, E.M.; Corti, M.C.; Bandeen-Roche, K.; Fried, L.P. Departures from linearity in the relationship between measures of muscular strength and physical performance of the lower extremities: The Women’s Health and Aging Study. J. Gerontol. A Biol. Sci. Med. Sci. 1997, 52, M275–M285. [Google Scholar] [CrossRef]
- Hong, J.; Kim, J.; Kim, S.W.; Kong, H.J. Effects of home-based tele-exercise on sarcopenia among community-dwelling elderly adults: Body composition and functional fitness. Exp. Gerontol. 2017, 87, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Marzetti, E.; Martone, A.M.; Bernabei, R.; Onder, G. Exercise as a remedy for sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Sipilä, S.; Suominen, H. Effects of strength and endurance training on thigh and leg muscle mass and composition in elderly women. J. Appl. Physiol. 1995, 78, 334–340. [Google Scholar] [CrossRef]
- Adamo, M.L.; Farrar, R.P. Resistance training, and IGF involvement in the maintenance of muscle mass during the aging process. Ageing Res. Rev. 2006, 5, 310–331. [Google Scholar] [CrossRef] [PubMed]
- Anderson, T.; Kearney, J.T. Effects of three resistance training programs on muscular strength and absolute and relative endurance. Res. Q Exerc. Sport 1982, 53, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Consitt, L.A.; Copeland, J.L.; Tremblay, M.S. Endogenous anabolic hormone responses to endurance versus resistance exercise and training in women. Sports Med. 2002, 32, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Hassan, B.H.; Hewitt, J.; Keogh, J.W.; Bermeo, S.; Duque, G.; Henwood, T.R. Impact of resistance training on sarcopenia in nursing care facilities: A pilot study. Geriatr. Nurs. 2016, 37, 116–121. [Google Scholar] [CrossRef]
- Schoenfeld, B.J. The mechanisms of muscle hypertrophy and their application to resistance training. J. Strength Cond. Res. 2010, 24, 2857–2872. [Google Scholar] [CrossRef]
- Hofmann, M.; Schober-Halper, B.; Oesen, S.; Franzke, B.; Tschan, H.; Bachl, N.; Strasser, E.M.; Quittan, M.; Wagner, K.H.; Wessner, B. Effects of elastic band resistance training and nutritional supplementation on muscle quality and circulating muscle growth and degradation factors of institutionalized elderly women: The Vienna Active Ageing Study (VAAS). Eur. J. Appl. Physiol. 2016, 116, 885–897. [Google Scholar] [CrossRef]
- Thomas, V.S.; Hageman, P.A. Can neuromuscular strength and function in people with dementia be rehabilitated using resistance-exercise training? Results from a preliminary intervention study. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 746–751. [Google Scholar] [CrossRef]
- Perpetuini, D.; Cardone, D.; Bucco, R.; Zito, M.; Merla, A. Assessment of the Autonomic Response in Alzheimer’s Patients During the Execution of Memory Tasks: A Functional Thermal Imaging Study. Curr. Alzheimer Res. 2018, 15, 951–958. [Google Scholar] [CrossRef]
- Jiskoot, L.C.; Poos, J.M.; Vollebergh, M.E.; Franzen, S.; van Hemmen, J.; Papma, J.M.; van den Berg, E. Emotion recognition of morphed facial expressions in presymptomatic and symptomatic frontotemporal dementia, and Alzheimer’s dementia. J. Neurol. 2021, 268, 102–113. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Exercise Group (n = 13) | Control Group (n = 13) | Z Statics | p | |
|---|---|---|---|---|
| Age (y) | 78.3 ± 5.3 | 78.2 ± 4.8 | −0.262 | 0.799 |
| MMSE | 18.8 ± 1.0 | 18.98 ± 1.0 | −0.211 | 0.843 |
| Weight (kg) | 49.8 ± 3.4 | 49.7 ± 2.1 | −0.232 | 0.843 |
| Height (m) | 1.53 ± 0.04 | 1.53 ± 0.03 | −0.292 | 0.799 |
| BMI (kg/m2) | 21.4 ± 0.9 | 21.4 ± 0.6 | −0.347 | 0.755 |
| Baseline SMI (kg/ m2) | 5.15 ± 0.30 | 5.16 ± 0.15 | −0.145 | 0.887 |
| MVC: hip flexor (N/kg) | 0.98 ± 0.19 | 1.03 ± 0.22 | −0.811 | 0.443 |
| MVC: knee extensor (N/kg) | 1.26 ± 0.24 | 1.30 ± 0.17 | −0.491 | 0.630 |
| Variable | Group | Pre | Post | Difference | Intragroup | Intergroup | ||
|---|---|---|---|---|---|---|---|---|
| Z Statics | p | Z Statics | p | |||||
| SMI | Exercise (n = 12) | 5.15 ± 0.30 | 5.16 ± 0.28 | 0.01 ± 0.07 | −0.708 | 0.479 | −1.449 | 0.160 |
| Control (n = 12) | 5.16 ± 0.15 | 5.15 ± 0.14 | −0.01 ± 0.02 | −1.887 | 0.590 | |||
| MVC: hip flexor (N/kg) | Exercise (n = 12) | 0.98 ± 0.19 | 1.26 ± 0.24 | 0.28 ± 0.15 | −3.062 | 0.002 | −4.170 | <0.001 |
| Control (n = 12) | 1.03 ± 0.22 | 1.02 ± 0.21 | −0.01 ± 0.02 | −1.545 | 0.122 | |||
| MVC: knee extensor (N/kg) | Exercise (n = 12) | 1.26 ± 0.24 | 1.45 ± 0.19 | 0.18 ± 0.07 | −3.063 | 0.002 | −4.165 | <0.001 |
| Control (n = 12) | 1.30 ± 0.17 | 1.27 ± 0.16 | −0.02 ± 0.04 | −1.539 | 0.124 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yun, J.H.; Kim, D.H.; Chang, M.C. A Simple Bedside Exercise Method to Enhance Lower Limb Muscle Strength in Moderate Alzheimer’s Disease Patients with Sarcopenia. Healthcare 2021, 9, 680. https://doi.org/10.3390/healthcare9060680
Yun JH, Kim DH, Chang MC. A Simple Bedside Exercise Method to Enhance Lower Limb Muscle Strength in Moderate Alzheimer’s Disease Patients with Sarcopenia. Healthcare. 2021; 9(6):680. https://doi.org/10.3390/healthcare9060680
Chicago/Turabian StyleYun, Jung Hae, Du Hwan Kim, and Min Cheol Chang. 2021. "A Simple Bedside Exercise Method to Enhance Lower Limb Muscle Strength in Moderate Alzheimer’s Disease Patients with Sarcopenia" Healthcare 9, no. 6: 680. https://doi.org/10.3390/healthcare9060680
APA StyleYun, J. H., Kim, D. H., & Chang, M. C. (2021). A Simple Bedside Exercise Method to Enhance Lower Limb Muscle Strength in Moderate Alzheimer’s Disease Patients with Sarcopenia. Healthcare, 9(6), 680. https://doi.org/10.3390/healthcare9060680