
Supporting the Regional Network for Children with Burn Injuries in a Pediatric Referral Hospital for COVID-19

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
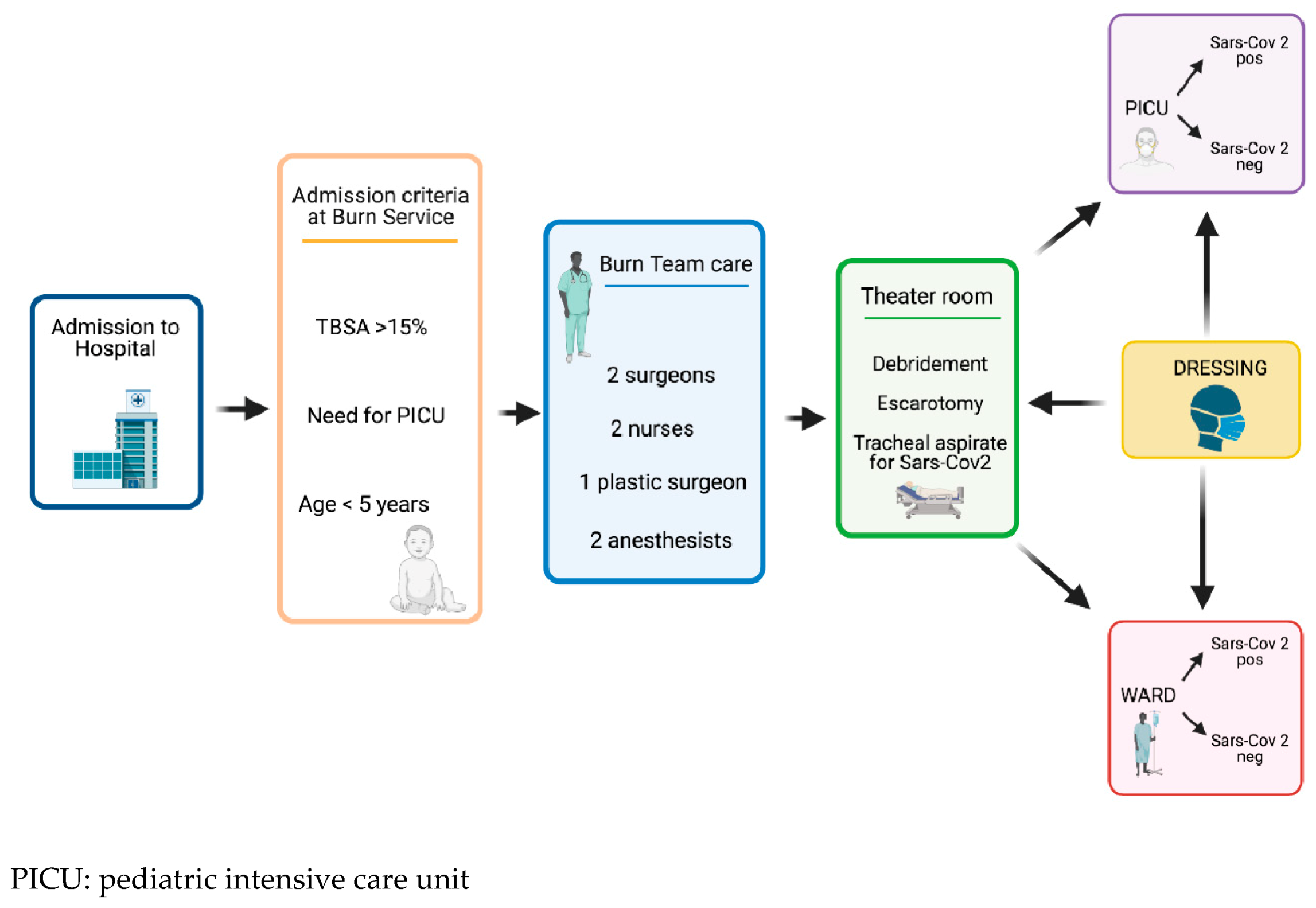
2.1. Organization of the Service
2.2. Patient Care
2.3. Postoperative Dressings
2.4. Patients and Data
2.5. Statistical Analysis
3. Results
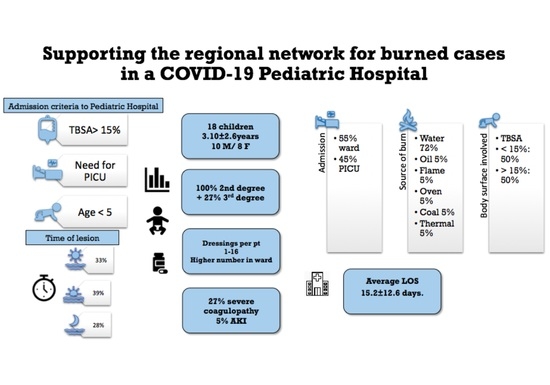
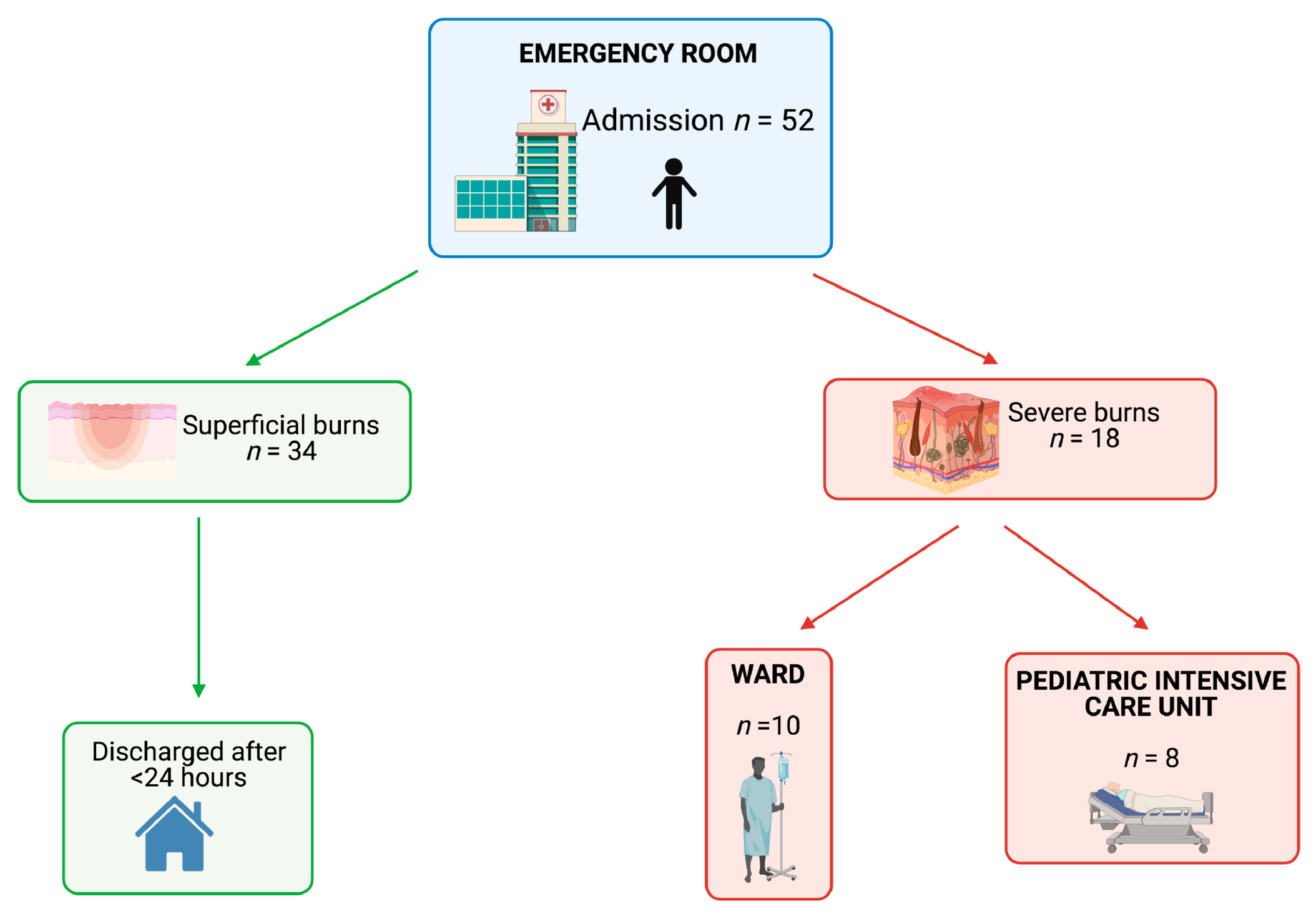
3.1. Epidemiological Data and Features of the Patients
3.2. Features of the Burns
3.3. Postoperative Follow-Up
3.4. Infection Control
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shekerdemian, L.S.; Mahmood, N.R. Characteristics and outcomes of children with coronavirus disease 2019 (COVID-19) infection admitted to US and Canadian pediatric intensive care units. JAMA Pediatrics 2020, 174, 868–8734. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.J. Pediatric burns: The forgotten trauma of childhood. Can. J. Surg. 2006, 49, 272–277. [Google Scholar] [PubMed]
- Sethuraman, U.; Stankovic, C.; Singer, A.; Vitale, L.; Krouse, C.B.; Cloutier, D.; Donoghue, L.; Klein, J.; Kannikeswaran, N. Burn visits to a pediatric burn center during the COVID-19 pandemic and ‘Stay at home’ period. Burns 2021, 47, 491–492. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.M.; Schoenfeld, D.A. Objective estimates of the probability of death from burn injuries. N. Engl. J. Med. 1998, 338, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Suman, A.; Owen, J. Update on the management of burns in paediatrics. BJA Educ. 2020, 20, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Toon, M.H.; Maybauer, D.M. Children with burn injuries—assessment of trauma, neglect, violence and abuse. INJ Violence Res. 2011, 3, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Ranno, R.; Vestita, M. Italian recommendations on enzymatic debridement in burn surgery. Burns 2020, 15, 30464–30465. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, T.L. Children are not little adults: Blood transfusion in children with burn injury. Burns Trauma 2017, 5, 24. [Google Scholar]
- Doctor, A.; Cholette, J.M.; Remy, K.E.; Argent, A.; Carson, J.L.; Valentine, S.L.; Bateman, S.T.; Lacroix, J.; Pediatric Critical Care Transfusion and Anemia Expertise Initiative (TAXI); Pediatric Critical Care Blood Research Network (BloodNet), and the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network. Recommendations on RBC transfusion in general critically ill children based on hemoglobin and/or physiologic thresholds from the Pediatric Critical Care Transfusion and Anemia Expertise Initiative. Pediatr. Crit. Care Med. 2018, 19, S98–S113. [Google Scholar] [CrossRef] [PubMed]
- Tieu, B.H.; Holcomb, J.B.; Schreiber, M.A. Coagulopathy: Its pathophysiology and treatment in the injured patient. World J. Surg. 2007, 31, 1055–1064. World J. Surg. 2007, 31, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.E.; Rose, J.K. Mortality determinants in massive pediatric burns. An analysis of 103 children with > or = 80% TBSA burns (>or = 70% full-thickness). Ann. Surg. 1997, 225, 554–569. [Google Scholar] [CrossRef] [PubMed]
- Bessey, P.Q.; Arons, R.R. The vulnerabilities of age: Burns in children and older adults. Surgery 2006, 140, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Chan, Q.E.; Barzi, F. Burn size estimation in children: Still a problem. Emerg. Med. Australas 2012, 24, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Tan Chor Lip, H.; Tan, J.H. Survival analysis and mortality predictors of hospitalized severe burn victims in a Malaysian burns intensive care unit. Burn. Trauma 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Nielson, C.B.; Duethman, N.C. Burns: Pathophysiology of systemic complications and current management. J. Burn. Care Res. 2017, 38, e469–e481. [Google Scholar] [CrossRef] [PubMed]
- Swords, D.S.; Hadley, E.D. Total body surface area overestimation at referring institutions in children transferred to a burn center. Am. Surg. 2015, 81, 56–63. [Google Scholar]
- Bittner, E.A.; Shank, E. Acute and perioperative care of the burn-injured patient. Anesthesiol 2015, 122, 448–464. [Google Scholar] [CrossRef] [PubMed]
- Lachiewicz, A.M.; Hauck, C.G.; Weber, D.J.; Cairns, B.A.; van Duin, D. Bacterial Infections After Burn Injuries: Impact of Multidrug Resistance. Clin. Infect. Dis. 2017, 65, 2130–2136. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Features | Year 2020 | Year 2019 |
|---|---|---|
| Number of admission, n | 52 | 32 |
| Sex (M/F) | 23/29 | 23/9 |
| Age | 3.9 ± 4 | 4.0 ± 4.4 |
| Burn grade n | ||
| First | 34 | 32 |
| 2nd | 13 | 0 |
| 2nd and 3rd | 5 | 0 |
| Total burn surface (%) | ||
| <10 | 32 | 32 |
| 10–15 | 11 | 0 |
| >15 | 9 | 0 |
| Features | Results |
|---|---|
| Number, n | 18 |
| Sex (M/F) | 10/8 |
| Age (years) | 3.10 ± 2.6 |
| Nationality, n (%) | |
| Italian | 6 (33.3) |
| Other | 12 (66.7) |
| Positivity SARS-CoV-2—nasopharyngeal and BAL of patient, n (%) | 1 (5%) |
| Time of accident n (%) | |
| Morning | 6 (33.3) |
| Afternoon | 7 (38.9) |
| Night | 5 (27.8) |
| Admission time (following the occurrence of the event), n (%) | |
| early (<4 h) | 13 (72.3) |
| delayed (>4 h) | 5 (27.7) |
| Features | Number of Patients (%) |
|---|---|
| Burn grade n (%) 2nd 2nd and 3rd | 13 (72.2) 5 (27.7) |
| Source, n (%) | |
| Water | 13 (72.2) |
| Oil | 1 (5.5) |
| Flame | 1 (5.5) |
| Oven | 1 (5.5) |
| Coal | 1 (5.5) |
| Thermal | 1 (5.5) |
| Total burn surface (%) <15% ≥15% | 13.0 ± 7.8 9 (50) 9 (50) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelizzo, G.; Vestri, E.; del Re, G.; Filisetti, C.; Osti, M.; Camporesi, A.; Rizzo, D.; De Angelis, A.; Zoia, E.; Tommasi, P.; et al. Supporting the Regional Network for Children with Burn Injuries in a Pediatric Referral Hospital for COVID-19. Healthcare 2021, 9, 551. https://doi.org/10.3390/healthcare9050551
Pelizzo G, Vestri E, del Re G, Filisetti C, Osti M, Camporesi A, Rizzo D, De Angelis A, Zoia E, Tommasi P, et al. Supporting the Regional Network for Children with Burn Injuries in a Pediatric Referral Hospital for COVID-19. Healthcare. 2021; 9(5):551. https://doi.org/10.3390/healthcare9050551
Chicago/Turabian StylePelizzo, Gloria, Elettra Vestri, Giulia del Re, Claudia Filisetti, Monica Osti, Anna Camporesi, Dario Rizzo, Armando De Angelis, Elena Zoia, Paola Tommasi, and et al. 2021. "Supporting the Regional Network for Children with Burn Injuries in a Pediatric Referral Hospital for COVID-19" Healthcare 9, no. 5: 551. https://doi.org/10.3390/healthcare9050551
APA StylePelizzo, G., Vestri, E., del Re, G., Filisetti, C., Osti, M., Camporesi, A., Rizzo, D., De Angelis, A., Zoia, E., Tommasi, P., Zuccotti, G., & Calcaterra, V. (2021). Supporting the Regional Network for Children with Burn Injuries in a Pediatric Referral Hospital for COVID-19. Healthcare, 9(5), 551. https://doi.org/10.3390/healthcare9050551