
Analysis of Facilitators and Barriers to the Delivery of Routine Care during the COVID-19 Global Pandemic: A Systematic Review


Abstract
1. Introduction
1.1. Rationale
1.2. Objectives
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search
2.4. Study Selection
2.5. Exclusion Criteria
2.6. Risk of Bias
3. Results
3.1. Study Characteristics
3.2. Summary of Evidence
4. Discussion
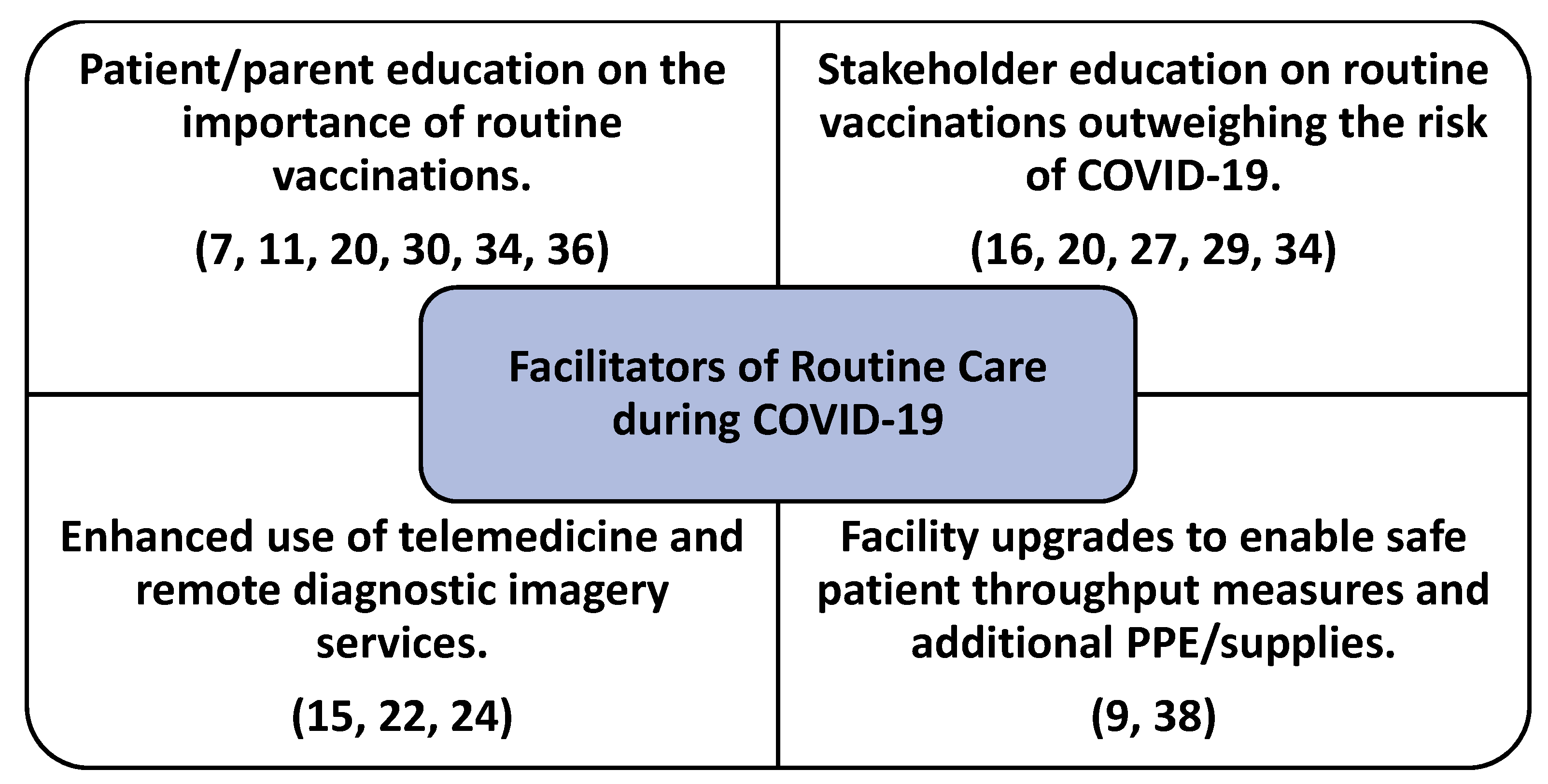
4.1. Facilitators of Routine Care
4.2. Barriers to Routine Care
4.3. Expansion of Telehealth: Pros and Cons
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- New Data Confirms Alarming Trend: COVID-19 Fears Are Causing Americans to Avoid the Doctor’s Office and Delay Routine Care. Available online: https://finance.yahoo.com/news/data-confirms-alarming-trend-covid-130000356.html?guccounter=1&guce_referer=aHR0cHM6Ly93d3cuZ29vZ2xlLmNvbS8&guce_referer_sig=AQAAACDt_jUOtyde48ntQ7S__HFN_0oK1faKF6c9By9hCZJXAjvY2xEyO4LPG3QkKythQ3pas6NWnnY_SYJPwlhYAUKBNmvTqdSDk4jS2Y4tgU_ya64xpnWxpdNdD_kPgyIZv_kLfIPuZbebnYh6ROh1N3h46Q98gt5NsNIXAjDZ9M (accessed on 30 April 2021).
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.N.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D.; et al. Delay or Avoidance of Medical Care Because of COVID-19-Related Concerns-United States, June 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef]
- Greene, J. Dental practices, routine treatments on hold during COVID-19. Crain’s Detroit Bus. 2020, 36, 0006. [Google Scholar]
- Papautsky, E.L.; Hamlish, T. Patient-reported treatment delays in breast cancer care during the COVID-19 pandemic. Breast Cancer Res. Treat. 2020, 184, 249–254. [Google Scholar] [CrossRef]
- Zintsmaster, M.P.; Myers, D.T. Patients avoided important care during the early weeks of the coronavirus pandemic: Diverticulitis patients were more likely to present with an abscess on CT. Emerg. Radiol. 2021, 28, 279–282. [Google Scholar] [CrossRef]
- Nuara, A.; Fabbri-Destro, M.; Scalona, E.; Lenzi, S.E.; Rizzolatti, G.; Avanzini, P. Telerehabilitation in response to constrained physical distance: An opportunity to rethink neurorehabilitative routines. J. Neurol. 2021, 1–12. [Google Scholar] [CrossRef]
- LSHTMCMMIDCOVID-19 Working Group; Abbas, K.; Procter, S.R.; Zandvoort, K.; van Clark, A.; Funk, S.; Mengistu, T.; Hogan, D.; Dansereau, E.; Jit, M.; et al. Routine childhood immunisation during the COVID-19 pandemic in Africa: A benefit-risk analysis of health benefits versus excess risk of SARS-CoV-2 infection. Lancet Glob. Health 2020, 8, e1264–e1272. [Google Scholar] [CrossRef]
- Abrams, S.A.; Avalos, A.; Gray, M.; Hawthorne, K.M. High Level of Food Insecurity among Families with Children Seeking Routine Care at Federally Qualified Health Centers during the Coronavirus Disease 2019 Pandemic. J. Pediatr. X 2020, 4, 100044. [Google Scholar] [CrossRef] [PubMed]
- Abu-Rustum, R.S.; Akolekar, R.; Sotiriadis, A.; Salomon, L.J.; da Costa, F.S.; Wu, Q.; Frusca, T.; Bilardo, C.M.; Prefumo, F.; Poon, L.C. ISUOG Consensus Statement on organization of routine and specialist obstetric ultrasound services in context of COVID-19. Ultrasound Obstet. Gynecol. 2020, 55, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Adamu, A.A.; Jalo, R.I.; Habonimana, D.; Wiysonge, C.S. COVID-19 and routine childhood immunization in Africa: Leveraging systems thinking and implementation science to improve immunization system performance. Int. J. Infect. Dis. 2020, 98, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Alsuhaibani, M.; Alaqeel, A. Impact of the COVID-19 Pandemic on Routine Childhood Immunization in Saudi Arabia. Vaccines 2020, 8, 581. [Google Scholar] [CrossRef]
- Ardakani, A.A.; Kanafi, A.R.; Acharya, U.R.; Khadem, N.; Mohammadi, A. Application of deep learning technique to manage COVID-19 in routine clinical practice using CT images: Results of 10 convolutional neural networks. Comput. Biol. Med. 2020, 121, 103795. [Google Scholar] [CrossRef]
- Berger-Richardson, D.; Ko, G.; Hong, N.L. Preparing for the Renaissance: Treating Breast Cancer during the COVID-19 Pandemic and Planning for a Safe Re-Emergence to Routine Surgical Care within a Universal Health Care System. Curr. Oncol. 2020, 27, 163–168. [Google Scholar] [CrossRef] [PubMed]
- De Carmelo, J.C.; Alves, T.K.C.; Khouri, M.S.; da Santos, R.P.M.; Rodrigues, L.G.; Alvarez-Leite, M.E.; Manzi, F.R. Impact of COVID-19 on the daily routine of radiology clinics. Imaging Sci. Dent. 2020, 50, 261–263. [Google Scholar] [CrossRef]
- Chan, J.Y.K.; Tsang, R.K.Y.; Yeung, K.W.; Abdullah, V.; Ku, P.; Wong, E.W.Y.; Mehta, N.; Orosco, R.K.; Holsinger, F.C. There is no routine head and neck exam during the COVID-19 pandemic. Head Neck 2020, 42, 1235–1239. [Google Scholar] [CrossRef]
- Chandir, S.; Siddiqi, D.A.; Mehmood, M.; Setayesh, H.; Siddique, M.; Mirza, A.; Soundardjee, R.; Dharma, V.K.; Shah, M.T.; Abdullah, S.; et al. Impact of COVID-19 pandemic response on uptake of routine immunizations in Sindh, Pakistan: An analysis of provincial electronic immunization registry data. Vaccine 2020, 38, 7146–7155. [Google Scholar] [CrossRef] [PubMed]
- Chudasama, Y.V.; Gillies, C.L.; Zaccardi, F.; Coles, B.; Davies, M.J.; Seidu, S.; Khunti, K. Impact of COVID-19 on routine care for chronic diseases: A global survey of views from healthcare professionals. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 965–967. [Google Scholar] [CrossRef] [PubMed]
- Corden, E.; Rogers, A.K.; Woo, W.A.; Simmonds, R.; Mitchell, C.D. A targeted response to the COVID-19 pandemic: Analysing effectiveness of remote consultations for triage and management of routine dermatology referrals. Clin. Exp. Dermatol. 2020, 45, 1047–1050. [Google Scholar] [CrossRef] [PubMed]
- Desai, U.; Kassardjian, C.D.; Del Toro, D.; Do, N.G.; Srinivasan, J.; Venesy, D.; Narayanaswami, P. The AANEM Quality and Patient Safety Committee Guidance for resumption of routine electrodiagnostic testing during the COVID-19 pandemic. Muscle Nerve 2020, 62, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Dinleyici, E.C.; Borrow, R.; Safadi, M.A.P.; van Damme, P.; Munoz, F.M. Vaccines and routine immunization strategies during the COVID-19 pandemic. Hum. Vaccines Immunother. 2021, 17, 400–407. [Google Scholar] [CrossRef]
- Ekberg, K.; Weinglass, L.; Ekberg, S.; Danby, S.; Herbert, A. The pervasive relevance of COVID-19 within routine paediatric palliative care consultations during the pandemic: A conversation analytic study. Palliat. Med. 2020, 34, 1202–1219. [Google Scholar] [CrossRef]
- Franzini, T.A.P.; Kotinda, A.P.S.T.; de Moura, D.T.H.; de Moura, E.G.H.; Badana, M.L.V.; de Medeiros, M.S.; Lima, P.G.R.; de Mello, B.F.; Kayano, R.P.; Carmona, M.J.C.; et al. Approach to endoscopic procedures: A routine protocol from a quaternary university referral center exclusively for coronavirus disease 2019 patients. Clinics 2020, 75. [Google Scholar] [CrossRef]
- Fung, A.; Irvine, M.; Ayub, A.; Ziabakhsh, S.; Amed, S.; Hursh, B.E. Evaluation of telephone and virtual visits for routine pediatric diabetes care during the COVID-19 pandemic. J. Clin. Transl. Endocrinol. 2020, 22, 100238. [Google Scholar] [CrossRef]
- Gupta, S.; Shahidi, N.; Gilroy, N.; Rex, D.K.; Burgess, N.G.; Bourke, M.J. Proposal for the return to routine endoscopy during the COVID-19 pandemic. Gastrointest. Endosc. 2020, 92, 735–742. [Google Scholar] [CrossRef]
- Howley, F.; O’Doherty, L.; McEniff, N.; O’Riordan, R. Late presentation of ‘Lemierre’s syndrome’: How a delay in seeking healthcare and reduced access to routine services resulted in widely disseminated Fusobacterium necrophorum infection during the global COVID-19 pandemic. BMJ Case Rep. 2020, 13, e239269. [Google Scholar] [CrossRef]
- Jung, J.; Kim, J.Y.; Bae, S.; Cha, H.-H.; Kim, E.O.; Kim, M.J.; Kim, S.-H. Contamination of personal protective equipment by SARS-CoV-2 during routine care of patients with mild COVID-19. J. Infect. 2020, 81, e165–e167. [Google Scholar] [CrossRef]
- Kinoshita, M.; Tanaka, M. Impact of Routine Infant BCG Vaccination on COVID-19. J. Infect. 2020, 81, 625–633. [Google Scholar] [CrossRef]
- Langdon-Embry, M.; Papadouka, V.; Cheng, I.; Almashhadani, M.; Ternier, A.; Zucker, J.R. Notes from the Field: Rebound in Routine Childhood Vaccine Administration Following Decline During the COVID-19 Pandemic—New York City, March 1–June 27, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 999–1001. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Comeau, J.L.; Dubé, È; Bucci, L.M. COVID-19 and missed routine immunizations: Designing for effective catch-up in Canada. Can. J. Public Health 2020, 111, 469. [Google Scholar] [CrossRef]
- McDonald, H.I.; Tessier, E.; White, J.M.; Woodruff, M.; Knowles, C.; Bates, C.; Parry, J.; Walker, J.L.; Scott, J.A.; Smeeth, L.; et al. Early impact of the coronavirus disease (COVID-19) pandemic and physical distancing measures on routine childhood vaccinations in England, January to April 2020. Eurosurveillance 2020, 25, 2000848. [Google Scholar] [CrossRef]
- Meyer, R.; Levin, G.; Hendin, N.; Katorza, E. Impact of the COVID-19 outbreak on routine obstetrical management: A cohort study. Authorea 2020, 22, 483–488. [Google Scholar] [CrossRef]
- Ogundele, O.A.; Omotoso, A.A.; Fagbemi, A.T. COVID-19 outbreak: A potential threat to routine vaccination programme activities in Nigeria. Hum. Vaccines Immunother. 2021, 17, 661–663. [Google Scholar] [CrossRef]
- Papanastasiou, E. The consequences of COVID-19 pandemic in the routine of Nuclear Medicine Departments. Hell. J. Nucl. Med. 2020, 23, 15–20. [Google Scholar]
- Ranganathan, R.; Khan, A.M. Routine immunization services during the coronavirus (COVID-19) pandemic. Indian J. Community Health 2020, 32, 236–239. [Google Scholar] [CrossRef]
- Rimmer, A. Covid-19: GPs can stop health checks for over 75s and routine medicine reviews. BMJ (Clin. Res. Ed.) 2020, 368, m1157. [Google Scholar] [CrossRef]
- Saxena, S.; Skirrow, H.; Bedford, H. Routine vaccination during covid-19 pandemic response. BMJ (Clin. Res. Ed.) 2020, 369, m2392. [Google Scholar] [CrossRef] [PubMed]
- Seyahi, E.; Poyraz, B.C.; Sut, N.; Akdogan, S.; Hamuryudan, V. The psychological state and changes in the routine of the patients with rheumatic diseases during the coronavirus disease (COVID-19) outbreak in Turkey: A web-based cross-sectional survey. Rheumatol. Int. 2020, 40, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- Kumari, A.; Zangmo, R.; Garg, D.; Sharma, K.A. Redesigning routine antenatal care in low resource setting during COVID-19 pandemic. J. Fam. Med. Prim. Care 2020, 9, 4547–4551. [Google Scholar] [CrossRef]
- Lieneck, C.; Garvey, J.; Collins, C.; Graham, D.; Loving, C.; Pearson, R. Rapid Telehealth Implementation during the COVID-19 Global Pandemic: A Rapid Review. Healthcare 2020, 8, 517. [Google Scholar] [CrossRef]
- Clarke, K. Lines grow outside food pantries as Covid-19 spikes again. America 2021, 2, 19. [Google Scholar]
- Kojima, N.; Klausner, J.D. Virtual House Calls: Telemedicine and Reforming the Health Care Delivery Model with Strategies Implemented in a Novel Coronavirus Pandemic. J. Gen. Intern. Med. 2020, 35, 2243. [Google Scholar] [CrossRef] [PubMed]
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med. Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Levine, L.B.; Guidry, M. Telehealth and COVID-19. EP Magazine, 6 May 2020. [Google Scholar]
- Ma, K.J.; Cohen, J.A.; Ba, M.B.; Levin, A.O.; Goyal, N.; Bs, T.L.; Chesney, M.A.; Shumay, D.M. “Soup cans, brooms, and Zoom:” Rapid conversion of a cancer survivorship program to telehealth during COVID-19. Psychooncology 2020, 29. [Google Scholar] [CrossRef]
- Hirko, K.A.; Kerver, J.M.; Ford, S.; Szafranski, C.; Beckett, J.; Kitchen, C.; Wendling, A.L. Telehealth in response to the COVID-19 pandemic: Implications for rural health disparities. J. Am. Med. Inform. Assoc. 2020, 27, 1816–1818. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author(s) | Study Participant(s) | Facilitators to Routine Care | Barriers to Routine Care | Patient Outcome(s) |
|---|---|---|---|---|
| Abbas et al. [7] | Pediatric patients in Africa seeking routine immunizations during the pandemic | Health benefits (prevention of estimated deaths) outweighed the risk of COVID-19 spread for clinic visits. | Lack of COVID-19 vaccine and other available immunizations resulted in an inability to perform routine care and increase the estimated mortality rate. | Sustainment of routine vaccinations and prevention of related diseases outweigh COVID-19 exposure risk. |
| Abrams et al. [8] | Families with children experiencing food insecurities at Federally Qualified Health Centers (FQHCs) during the pandemic | n/a | Food insecurity experienced by 60% of survey respondents. Fear of running out of food experienced by 90% of respondents. | Food insecurity affected patients’ ability to receive routine care during the pandemic at FQHCs. |
| Abu-Rustum et al. [9] | Obstetric patients | A tiered system was created to prioritize pregnant mothers needing obstetric examinations to ensure ongoing access to care. | Special modifications and a tiered system left some mothers prioritized at a lower level, thus delaying care. | General guidance issued by the ISUOG organization to ensure the highest acuity patients were seen first in a controlled environment to prevent the spread of COVID for each possible patient circumstance. |
| Adamua et al. [10] | Pediatric patients in Africa | Systems thinking an analysis demonstrates the importance of ongoing routine vaccinations in Africa, outweighing the risk of COVID-19 in the country. System re-design was implemented. | A lack of analysis on the CLD (causal loop diagram) in the study suggested potential COVID-19 spread at local clinics for routine vaccinations. | Improved control over COVID-19 outbreaks by analysis of communities, population groups, and socioeconomic data. |
| Alsuhaibani and Alaqeel [11] | Pediatrics patients in Saudi Arabia | Improved parental awareness regarding the importance of routine vaccinations led to a decreased in the prevalence of delayed routine childhood immunizations. | Lack of parental education on the importance of routine childhood immunizations and delayed appointments due to COVID-19 precautions. | While most parents had a positive perspective on routine vaccinations, 65% of parents were not concerned about ongoing delays for routine care (vaccinations). |
| Abbasian et al. [12] | COVID patients (and non-COVID patients) requiring CT imaging procedure(s) | Computerized automated detection (CAD) applications assist in the speed of diagnosis of COVID infections amongst other atypical/viral pneumonia diseases. | Risk of the spread of COVID-19 during the CT procedure was of concern. | Faster diagnosis of patients with lung conditions related to COVID-19. |
| Berger-Richardson and Hong [13] | Patients with breast cancer | Treatment recommendations for patients with breast cancer enabled a safe environment of care to help prevent the spread of COVID-19. | A delay in endocrine treatment may lead to the risk of progression in these patients. | Delays to surgical treatments for routine cancer care longer than 3–6 months require ongoing monitoring and imaging as precautional measures. |
| Carmelo et al. [14] | Patients requiring radiology/imaging during routine dental care procedures | Remote diagnosis using medical imagery is recommended versus in-person to avoid the spread of COVID-19. Additional procedures (scheduling, use of additional PPE, etc.) also was implemented. | Dentistry is prone to a high risk of transmissibility when precautions and remove diagnoses are not conducted. | Patient, as well as clinical staff and providers were able to help control the risk of spreading COVID-19. |
| Chan et al. [15] | Patients requiring a head and neck exam during the pandemic | Specific treatment guidelines established in order to treat patients requiring head and neck procedures. | Nonessential head and neck patients were categorized, and care postponed during the pandemic. | Lower-level patients (non-urgent, low acuity) experience an access to care issue during the pandemic. |
| Chandir et al. [16] | Patients requiring routine immunizations in Pakistan | A quantitative analysis (pre- and post-study) reveals that returning to normal social and school events will help facilitate routine immunization rates in rural/poorer regions. | Global lockdown due to the pandemic as related to high/low-income countries led to lower routine vaccination rates. | n/a |
| Chudasma et al. [17] | Healthcare providers (global survey) | New methods of delivering care in a virtual environment is necessary for the ongoing routine care related to chronic diseases. | A reduction of in-person visits due to the pandemic initially led to a decrease in the treatment of routine, chronic conditions. | Patients with chronic conditions able to receive care in the virtual environment, versus not receiving the required routine care at all. |
| Corden et al. [18] | Patients with routine dermatology referrals | Patient care was deemed adequate during temporary process changes through the use of patient triage and indication of COVID-19 diagnosis. | Inefficiencies noted regarding the temporary protocols established to care for these patients. | Adequate patient care established for these industry segment, while temporary process changes identified the need for follow-on, long-term solutions as the pandemic continues. |
| Desai et al. [19] | Patients requiring electrodiagnostic testing | Staying current on CDC compliant measures is required to ensure provider safety. Further organizational committee work (collaboration) to establish protocols helped ensure preventive measures were followed. | n/a | Patients requiring this routine diagnostic test were able to receive it. |
| Dinleyici et al. [20] | Pediatric patients requiring routine vaccinations during the pandemic | Analysis of COVID-19 mitigation and routine immunization services allows for an assessment of already high-risk children during the pandemic. | Children with diseases considered ‘under control’ prior to the pandemic will be put at higher risk if the population slows routine vaccinations. | n/a |
| Ekbert et al. [21] | Pediatric patients receiving palliative care | An assessment of communication between providers and patients requiring routine palliative included the relevance of COVID-19 in the treatment process. | Clinical disposition due to COVID-19 was identified at 55% and parents identified at 45%. | COVID-19 was identified as a persuasive treatment variable during provider communications with routine palliative care patients. |
| Antonio et al. [22] | Patients requiring routine endoscopic procedures | Additional PPE, separation of procedure rooms, and methods regarding room preparation assist in the return of routine endoscopic procedures during the pandemic. | Lack of quality control and detailed measures to follow will lead to increased transmissions during routine care. | n/a |
| Fung et al. [23] | Pediatric patients requiring routine diabetes care | Use of telephone only and also virtual (webinar) patient-provider visits enable access to routine care. | n/a | Survey results demonstrated patient and family member satisfaction with both telephones only and online/webinar (virtual) patient visit methods. |
| Gupta et al. [24] | Patients requiring routine endoscopic procedures | Routine point-of-care testing for COVID-19 and clinical risk assessments assisted with access to this procedure. | Patients requiring an elective endoscopic procedure were prioritized lower and/or postponed. | Access to care for high-acuity patients, while elective patients were recommended to be postponed due to the risk assessments. |
| Howley et al. [25] | Patient with Lemierre syndrome and delayed access to routine care | Enhanced awareness to the provider community regarding how delayed access to routine (‘non-essential’) care can lead to a complex illness otherwise treatable. | Delayed routine care resulted in a complex medical condition. | Patient’s disease/acuity progressed due to delayed routine care. |
| Jung et al. [26] | Medical providers and their use of PPE when providing routine care to COVID-patients | Adherence to proper protocols regarding the dawning and removal of PPE will help lower infection rate of medical providers. | PPE contamination was identified on the top of provider heads, dorsum of the foot, wrist, and abdomen. | Identification of medical provider PPE dawning/removal of PPE protocols assists with reducing COVID-19 contamination. |
| Kinoshita and Tanaka [27] | Infants receiving the Bacille Calmette-Guérin (BCG) vaccination | Awareness efforts encouraged by health officials assist in keeping the high level of vaccinations during the pandemic. | Challenges for BCG vaccination presented due to COVID-19, distancing, and vaccination processes. | Spread of tuberculosis was lowered after attention and re-education of how important routine vaccinations are during the pandemic. |
| Landgon-Embry et al. [28] | New York City routine childhood vaccination rates | Increased awareness efforts led to better routine vaccination compliance during the severe outbreak in the city. | Significant COVID-19 spread and also patient/family fear of routine care lowered routine vaccination rates across the city. | Increased education and distancing/safety protocols increased routine vaccination compliance in the city. |
| MacDonald et al. [29] | Canadian patients requiring routine vaccinations | Specific follow-up (patient communications/contact methods) for those who are due or missed a routine vaccination increase the compliance with this program. | Preventable diseases threatened to increase in prevalence if routine vaccinations are not continued during the pandemic. | Contacted patients educated on the importance of routine vaccination compliance and safety protocols in-place during COVID-19. |
| McDonald et al. [30] | Children in England | Parental education on routine vaccinations helped to increase compliance during the pandemic around week 17. | Physical distancing requirements led to delayed and canceled routine vaccination appointments as identified by the organization’s EMR system. | Physical distancing messaging and related communications can dramatically affect the compliance with routine vaccinations/care. |
| Meyer et al. [31] | Patients requiring routine obstetrical care in Israel | Analysis of routine obstetrical care referrals, discharge rate, time spend in an ED/ER, delivery unit and/or admission rate revealed information to assist in identifying and correcting obstetrical patients missing routine care appointments. | Due to physical distancing requirements, routine appointments for obstetrical care were avoided by female patients and an increase in ER/ED deliveries was also experienced. | Avoided routine obstetrical care led to an increase in ER/ED deliveries in Israel during the pandemic. |
| Ogundele et al. [32] | Patients requiring routine vaccinations in Nigeria | Observations regarding the Nigerian health system document a need to prioritize routine childhood immunizations to help alleviate already-low vaccination rates (pre-pandemic). | Communities still struggle with compliance with routine care and COVID-19 exacerbated the issue. | Hinderance on facilitating vaccinations in Nigeria will lead to an increase in morbidity and mortality due to a lack of routine care. |
| Papanstasiou [33] | Nuclear medicine providers/staff | A review of facility upgrades (additional hand sanitizer stations, plastic screens, additional PPE to be handed-out, and ensuring sufficient radio pharmaceutical supplies) helped to re-established delivery of care. | Lack of intervention and initiatives would have led to a shortage of nuclear medicine routine care. | Patients requiring routine nuclear medicine care were able to be seen as a result of these protocol changes. |
| Ranganthan and Khan [34] | Children in India | A recommendation of future telecommunication initiatives, as well as community workers and use of social media may help increase future routine vaccination compliance in challenging times. | A hesitation to give routine vaccinations in India by parents and providers initially led to a decrease in compliance. | Use of government messaging/communications enhanced routine vaccination rates in India after issues related to COVID-19. |
| Rimmer [35] | General practitioners | A recommendation of delaying routine care for patients over 75 led to additional time/availability for these providers to assist with COVID-19 patients. | Delayed care for those over 75 without a COVID-19 diagnosis was an implication of the recommendation. | General practitioner availability to assist with COVID-19 patients increased. |
| Saxena et al. [36] | Patients requiring routine vaccinations | Compliance with getting routine vaccinations on-time will ensure their efficacy. | n/a | If a shot is delayed, then it may no longer be effective as a vaccine for the patient. |
| Seyahi et al. [37] | Patients seeking routine care for rheumatic diseases in Turkey | The mental state of patients with rheumatic diseases receiving and/or canceling routine care during the pandemic was better than expected. | n/a | Patient routines changes, to including some stopping rheumatic medications altogether during the pandemic. |
| Zangmo et al. [38] | Obstetric patients requiring antenatal care | Increased use of telemedicine assisted in the continuation of this care to avoid face-to-face visits without sacrificing quality of care. | COVID-19 restrictions can decrease communication between the patient and provider. | Methods were established to help identify better methods of care for obstetric patients. |
| Identified Health Care Service Constructs in the Sample | Accurrence of Attribute (%) | Frequency of Occurrance (%) |
|---|---|---|
| Chronic care management (health disease, diabetes, obseity) | 12, 13, 16, 17, 23, 25, 35, 37 | 8 (25%) |
| Obstretical care | 9, 31, 38 | 3 (9%) |
| Routine (non-COVID-19) vaccinations | 7, 10, 11, 16, 20, 27, 28, 29, 30, 32, 34, 36 | 12 (37%) |
| Routine care, other | 8, 14, 15, 18, 19, 21, 22, 24, 26, 33 | 10 (31%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lieneck, C.; Herzog, B.; Krips, R. Analysis of Facilitators and Barriers to the Delivery of Routine Care during the COVID-19 Global Pandemic: A Systematic Review. Healthcare 2021, 9, 528. https://doi.org/10.3390/healthcare9050528
Lieneck C, Herzog B, Krips R. Analysis of Facilitators and Barriers to the Delivery of Routine Care during the COVID-19 Global Pandemic: A Systematic Review. Healthcare. 2021; 9(5):528. https://doi.org/10.3390/healthcare9050528
Chicago/Turabian StyleLieneck, Cristian, Brooke Herzog, and Raven Krips. 2021. "Analysis of Facilitators and Barriers to the Delivery of Routine Care during the COVID-19 Global Pandemic: A Systematic Review" Healthcare 9, no. 5: 528. https://doi.org/10.3390/healthcare9050528
APA StyleLieneck, C., Herzog, B., & Krips, R. (2021). Analysis of Facilitators and Barriers to the Delivery of Routine Care during the COVID-19 Global Pandemic: A Systematic Review. Healthcare, 9(5), 528. https://doi.org/10.3390/healthcare9050528