
Impact of Sensitization of Family Caregivers upon Treatment Compliance among Geriatric Patients Suffering from Elder Abuse and Neglect

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Study Design
2.3. Operational Definition
2.4. Sample Preparation, Selection and Grouping
2.5. Measures, Data Evaluation, Collection and Analysis
3. Results
4. Discussion
4.1. Ever-Changing Role of Healthcare Workers (HCW) in Detecting Elder Abuse
4.2. Need of Recognizing the Clinical Impact of EAN on Routine Medical/Dental Treatment Plans
4.3. FCG’s Parameters and Caregiving
4.4. EAN and the Type of Intervention
5. Strength and Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Atetwe, L.K. Prevalence of elder abuse in Emuhaya sub-county, Vihiga County, Kenya. In International Handbook of Elder Abuse and Mistreatment; Shankardass, M., Ed.; Springer: Singapore, 2020. [Google Scholar] [CrossRef]
- Randel, J.; German, T.; Ewing, D. The Ageing and Development Report: Poverty, Independence and the World’s Older People; Earthscan: London, UK, 1999. [Google Scholar]
- Fougère, B.; Morley, J.E.; Decavel, F.; Nourhashémi, F.; Abele, P.; Resnick, B.; Rantz, M.; Lai, C.K.Y.; Moyle, W.; Pédra, M.; et al. Development and implementation of the advanced practice nurse worldwide with an interest in geriatric care. J. Am. Med Dir. Assoc. 2016, 17, 782–788. [Google Scholar] [CrossRef]
- Mattoo, K.A.; Garg, R.; Dhingra, S. Classifying elder abuse—A review. Gerontol. Geriatr. Res. 2019, 2, 118. [Google Scholar]
- Mattoo, K.A.; Shalabh, K.; Khan, A. Geriatric forensics: A dentist′s perspective and contribution to identify existence of elder abuse among his patients. J. Forensic Dent. Sci. 2010, 2, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Shubayr, M.A.; Mattoo, K.A. Parental neglect of feeding in obese individuals. A review of scientific evidence and its application among Saudi population. Saudi Med. J. 2020, 41, 451–458. [Google Scholar] [CrossRef]
- Okoye, U.O.; Asa, S.S. Caregiving and stress: Experience of people taking care of elderly relations in south-eastern Nigeria. Arts Soc. Sci. J. 2011, 29, 1–9. [Google Scholar]
- Senanarong, V.; Jamjumras, P.; Harmphadungkit, K.; Klubwongs, M.; Udomphanthurak, S.; Poungvarin, N.; Vannasaeng, S.; Cummings, J.L. A counseling intervention for caregivers: Effect on neuropsychiatric symptoms. Int. J. Geriatr. Psychiatry 2004, 19, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Epstein, R.M. Virtual physicians, health systems, and the healing relationship. J. Gen. Intern. Med. 2003, 18, 404–406. [Google Scholar] [CrossRef][Green Version]
- Fulmer, T.; Paveza, G.; Abraham, I.; Fairchild, S. Elder neglect assessment in the emergency department. J. Emerg. Nurs. 2000, 26, 436–443. [Google Scholar] [CrossRef]
- Mattoo, K.A.; Shalabh, K.; Khan, A. Prevelance of elder abuse among completely edentulous patients seeking complete denture prosthesis—A survey. J. Indian Acad. Geriatr. 2009, 5, 177–180. [Google Scholar]
- Hullick, C.; Carpenter, C.R.; Critchlow, R.; Burkett, E.; Arendts, G.; Nagaraj, G.; Rosen, T. Abuse of the older person: Is this the case you missed last shift? Emerg. Med. Australas. 2017, 29, 223–228. [Google Scholar] [CrossRef]
- Dong, X. Medical implications of elder abuse and neglect. Clin. Geriatr. Med. 2005, 21, 293–313. [Google Scholar] [CrossRef]
- Mattoo, K.A.; Garg, R.; Kumar, S. Geriatric forensics—Part 2. Prevalence of elder abuse and their potential forensic markers among medical and dental patients. J. Forensic Dent. Sci. 2015, 7, 201–207. [Google Scholar] [CrossRef]
- Dong, X.; Simon, M.; Odwazny, R.; Gorbien, M. Depression and elder abuse and neglect among a community-dwelling Chinese elderly population. J. Elder Abus. Negl. 2008, 20, 25–41. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Arch. Intern. Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef]
- Lee, K.L.; Mustaffa, M.S. Using art in counselling adults: A pilot study. Asia Pac. J. Couns. Psychother. 2011, 2, 98–114. [Google Scholar] [CrossRef]
- Werth, J.L.; Kopera-Frye, K.; Blevins, D.; Bossick, B. Older adult representation in the counseling psychology literature. Couns. Psychol. 2003, 31, 789–814. [Google Scholar] [CrossRef]
- Johnson, T.F. Critical issues in the definition of Elder mistreatment. In Elder Abuse: Conflict in the Family; Pillemer, K., Wolf, R., Eds.; Auburn House Publishing Company: Dover, MA, USA, 1986; pp. 167–196. [Google Scholar]
- Kua, E.H.; Ko, S.M. A questionnaire to screen for cognitive impairment among elderly people in developing countries. Acta Psychiatr. Scand. 1992, 85, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, M.J.; Tazkarji, B. Understanding elder abuse in family practice. Can. Fam. Physician 2012, 58, 1336–1340. [Google Scholar]
- Altman, D.G. Why we need confidence intervals. World J. Surg. 2005, 29, 554–556. [Google Scholar] [CrossRef]
- Jeganathan, S.; Thean, H.P.; Thong, K.T.; Chan, Y.C.; Singh, M. A clinically viable index for quantifying denture plaque. Quintessence Int. 1996, 27, 569–573. [Google Scholar] [PubMed]
- McCunniff, M.; Liu, W.; Dawson, D.; Marchini, L. Patients’ esthetic expectations and satisfaction with complete dentures. J. Prosthet. Dent. 2017, 118, 159–165. [Google Scholar] [CrossRef]
- Yon, M.Y.; Mikton, C.R.; Gassoumis, Z.D.; Wilber, K.H. Elder abuse prevalence in community settings: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e147–e156. [Google Scholar] [CrossRef]
- Arora, H.; Singhal, A.; Goyal, A.; Kashyap, H.; Dhingra, G.; Kumar, A.; Kumar, D.; Ahmad, S. Knowledge, attitude and practices about the elderly care and elderly abuse among the medical and dental students. Indian J. Public Health Res. Dev. 2020, 11, 127–132. [Google Scholar] [CrossRef]
- Sooryanarayana, R.; Choo, W.-Y.; Hairi, N.N. A review on the prevalence and measurement of elder abuse in the community. Trauma Violence Abus. 2013, 14, 316–325. [Google Scholar] [CrossRef]
- Anand, A. Exploring the role of socioeconomic factors in abuse and neglect of elderly population in Maharashtra, India. J. Geriatr. Ment. Health 2016, 3, 150. [Google Scholar] [CrossRef]
- Nisha, C.; Manjaly, S.; Kiran, P.; Mathew, B.; Kasturi, A. Study on elder abuse and neglect among patients in a medical college hospital, Bangalore, India. J. Elder Abus. Negl. 2015, 28, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Platts-Mills, T.F.; Barrio, K.; Isenberg, E.E.; Glickman, L.T. Emergency physician identification of a cluster of elder abuse in nursing home residents. Ann. Emerg. Med. 2014, 64, 99–100. [Google Scholar] [CrossRef]
- Ahmed, A.; Choo, W.-Y.; Othman, S.; Hairi, N.N.; Hairi, F.M.; Mydin, F.H.M.; Jaafar, S.N.I. Understanding of elder abuse and neglect among healthcare professionals in Malaysia: An exploratory survey. J. Elder Abus. Negl. 2016, 28, 163–177. [Google Scholar] [CrossRef] [PubMed]
- McLellan, A. Nurses have a key role to play in tackling elder abuse. Nurs. Times 2008, 104, 1. [Google Scholar]
- Schofield, M.J.; Powers, J.R.; Loxton, D. Mortality and disability outcomes of self-reported elder abuse: A 12-year prospective investigation. J. Am. Geriatr. Soc. 2013, 61, 679–685. [Google Scholar] [CrossRef]
- Dong, X.; Simon, M.A. Elder abuse as a risk factor for hospitalization in older persons. JAMA Intern. Med. 2013, 173, 911–917. [Google Scholar] [CrossRef]
- Storey, J.E. Risk factors for elder abuse and neglect: A review of the literature. Aggress. Violent Behav. 2020, 50, 101339. [Google Scholar] [CrossRef]
- Mouton, C.P.; Rodabough, R.J.; Rovi, S.L.D.; Brzyski, R.G.; Katerndahl, D.A. Psychosocial effects of physical and verbal abuse in postmenopausal women. Ann. Fam. Med. 2010, 8, 206–213. [Google Scholar] [CrossRef]
- Dyer, C.B.; Pavlik, V.N.; Murphy, K.P.; Hyman, D.J. The high prevalence of depression and dementia in elder abuse or neglect. J. Am. Geriatr. Soc. 2000, 48, 205–208. [Google Scholar] [CrossRef]
- Wells, K.B.; Rogers, W.; Burnam, A.; Greenfield, S.; Ware, J.E. How the medical comorbidity of depressed patients differs across health care settings: Results from the Medical Outcomes Study. Am. J. Psychiatry 1991, 148, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- John, M.; Micheelis, W.; Steele, J. Depression as a risk factor for denture dissatisfaction. J. Dent. Res. 2007, 86, 852–856. [Google Scholar] [CrossRef]
- Roberto, K.A. The complexities of elder abuse. Am. Psychol. 2016, 71, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Lachs, M.S.; Pillemer, K.A. Elder Abuse. N. Engl. J. Med. 2015, 373, 1947–1956. [Google Scholar] [CrossRef]
- Johansson, A. Risk Markers Sssociated with Caregiver Elder Abuse: A Meta-Analytic Study. Ph.D. Thesis, Loma Linda University, Loma Linda, CA, USA, June 2018. [Google Scholar]
- Chang, H.-Y.; Chiou, C.-J.; Chen, N.-S. Impact of mental health and caregiver burden on family caregivers’ physical health. Arch. Gerontol. Geriatr. 2010, 50, 267–271. [Google Scholar] [CrossRef] [PubMed]
- MacNeil, G.; Kosberg, J.I.; Durkin, M.D.W.; Dooley, W.K.; DeCoster, J.; Williamson, G.M. Caregiver mental health and potentially harmful caregiving behavior: The central role of caregiver anger. Gerontologist 2009, 50, 76–86. [Google Scholar] [CrossRef]
- Beneken, G.; Kolmer, D.M.; Tellings, A.; Gelissen, J. Partnership in health care: Views of family caregivers on sharing care responsibility with government, clients and health insurers. Med. Law. 2008, 27, 705–730. [Google Scholar]
- Andrén, S.; Elmståhl, S. Relationships between income, subjective health and caregiver burden in caregivers of people with dementia in group living care: A cross-sectional community-based study. Int. J. Nurs. Stud. 2007, 44, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Son, J.; Erno, A.; Shea, D.G.; Femia, E.E.; Zarit, S.H.; Stephens, M.A.P. The caregiver stress process and health outcomes. J. Aging Health 2007, 19, 871–887. [Google Scholar] [CrossRef]
- Lee, J.L.; Burnett, J.; Dyer, C.B. Frailty in self-neglecting older adults: A secondary analysis. J. Elder Abus. Negl. 2016, 28, 152–162. [Google Scholar] [CrossRef]
- Rosen, T.; Makaroun, L.K.; Conwell, Y.; Betz, M. Violence in older adults: Scope, impact, challenges, and strategies for prevention. Health Aff. 2019, 38, 1630–1637. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; O’Brien, A.; Czaja, S.; Ory, M.; Norris, R.; Martire, L.M.; Belle, S.H.; Burgio, L.; Gitlin, L.; Coon, D.; et al. Dementia caregiver intervention research. Gerontologist 2002, 42, 589–602. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, M.; Kupfer, R.; Reissmann, D.R.; Mühlhauser, I.; Köpke, S. Oral health educational interventions for nursing home staff and residents. Cochrane Database Syst. Rev. 2016, 9, CD010535. [Google Scholar] [CrossRef]
- Chen, X.; Clark, J.J.; Chen, H.; Naorungroj, S. Cognitive impairment, oral self-care function and dental caries severity in community-dwelling older adults. Gerodontology 2015, 32, 53–61. [Google Scholar] [CrossRef]
- Covinsky, K.E.; Fortinsky, R.H.; Palmer, R.M.; Kresevic, D.M.; Landefeld, C.S. Relation between symptoms of depression and health status outcomes in acutely ill hospitalized older persons. Ann. Intern. Med. 1997, 126, 417–425. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Score | Grade | The Total Amount of Plaque Disclosed on the Denture Surface |
|---|---|---|
| 1 | Good | No plaque |
| 2 | Average | Moderate plaque (25% to 50% of the fitting surface and tooth surface was covered) |
| 3 | Poor | Heavy plaque (51% to 75% of the fitting surface and tooth surface was covered) |
| 4 | Very poor | Very heavy plaque (76% to 100% of the fitting surface and tooth surface was covered) |
| Characteristic | Parameters | Main Survey n (%) | Sample Subjects n (%) | |
|---|---|---|---|---|
| Group A (Control) | Group B (Test) | |||
| Prevalence | Total number of subjects | n = 860 | n = 75 | n = 75 |
| Suspected elder abuse (EASI) | 332 (38.6) | N.A. | N.A. | |
| Confirmed (self-revelation) | 312 (36.27) | N.A. | N.A. | |
| Gender (abused) | Male | 198 (63.4) | 64 (85.33) | 64 (85.33) |
| Female | 114 (36.5) | 11 (14.67) | 11 (14.67) | |
| Age distribution of abused (in years) | 41–50 | 42 (13.46) | 1 (1.33) | 3 (4) |
| 51–60 | 117 (37.5) | 26 (34.66) | 32 (42.67) | |
| 61–70 | 94 (30.12) | 26 (34.66) | 20 (26.67) | |
| 71–80 | 59 (18.9) | 22 (29.33) | 20 (26.67) | |
| Abuse type distribution | Neglect | 119 (38.14) | 59 (78.66) | 51 (68) |
| Psychological | 53 (16.98) | N.A. | N.A. | |
| Financial | 31 (9.93) | N.A. | N.A. | |
| Physical | 64 (20.51) | N.A. | N.A. | |
| Sexual | 1 (0.32) | N.A. | N.A. | |
| Combination (neglect and one or more) | 44 (14.10) | 16 (21.33) | 24 (32) | |
| Level of education of abused subjects | Illiterate/primary school | 267 (85.57) | 62 (82.67) | 68 (90.67) |
| Literate/secondary school/graduate/postgraduate | 45 (14.42) | 13 (17.33) | 7 (9.33) | |
| Abuser (family caregiver) types (n = 312) | Son | 165 (52.88) | 41 (54.66) | 42 (56) |
| Daughter-in-law | 97 (31.08) | 26 (34.66) | 23 (30.6) | |
| Spouse | 24 (7.69) | 8 (10.67) | 6 (8) | |
| Brother/Sister | 12 (3.84) | 0 (0) | 2 (2.66) | |
| Others | 2 (0.65) | 0 (0) | 2 (2.66) | |
| Age distribution of family caregiver | ≤20 | 45 (14.42) | 5 (6.67) | 6 (8) |
| 21–30 | 162 (51.9) | 31 (41.33) | 44 (58.6) | |
| 31–40 | 90 (28.84) | 34 (45.33) | 20 (26.67) | |
| 41–50 | 10 (3.2) | 4 (5.3) | 2 (2.66) | |
| ≥51 | 5 (1.6) | 1 (1.33) | 3 (4) | |
| Income of family caregiver * | Low | 235 (75.32) | 56 (74.6) | 50 (66.67) |
| Average | 65 (20.83) | 12 (16) | 20 (26.67) | |
| High | 12 (3.84) | 7 (9.34) | 5 (6.67) | |
| Level of education of family caregiver | Illiterate/primary school | 215 (68.9) | 57 (76) | 59 (78.67) |
| Literate/secondary school/graduate/postgraduate | 97 (31.08) | 18 (24) | 16 (21.34) | |
| Scores | Group A (Control) | Group B (Test) | Probable Value of t (Unpaired) | Karl Pearson Correlation Coefficient (r) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n (75) | % | Mean ± SD | SEM | n (75) | % | Mean ± SD | SEM | 0.0000 * | −0.0017 (NS) | |
| Good | 4 | 5.3 | 2.92 ± 0.892 | 0.1564 | 52 | 69.33 | 1.38 ± 0.618 | 0.1084 | ||
| Average | 23 | 30.6 | 18 | 24 | ||||||
| Poor | 27 | 36 | 5 | 6.67 | ||||||
| Very Poor | 21 | 28 | 0 | 0 | ||||||
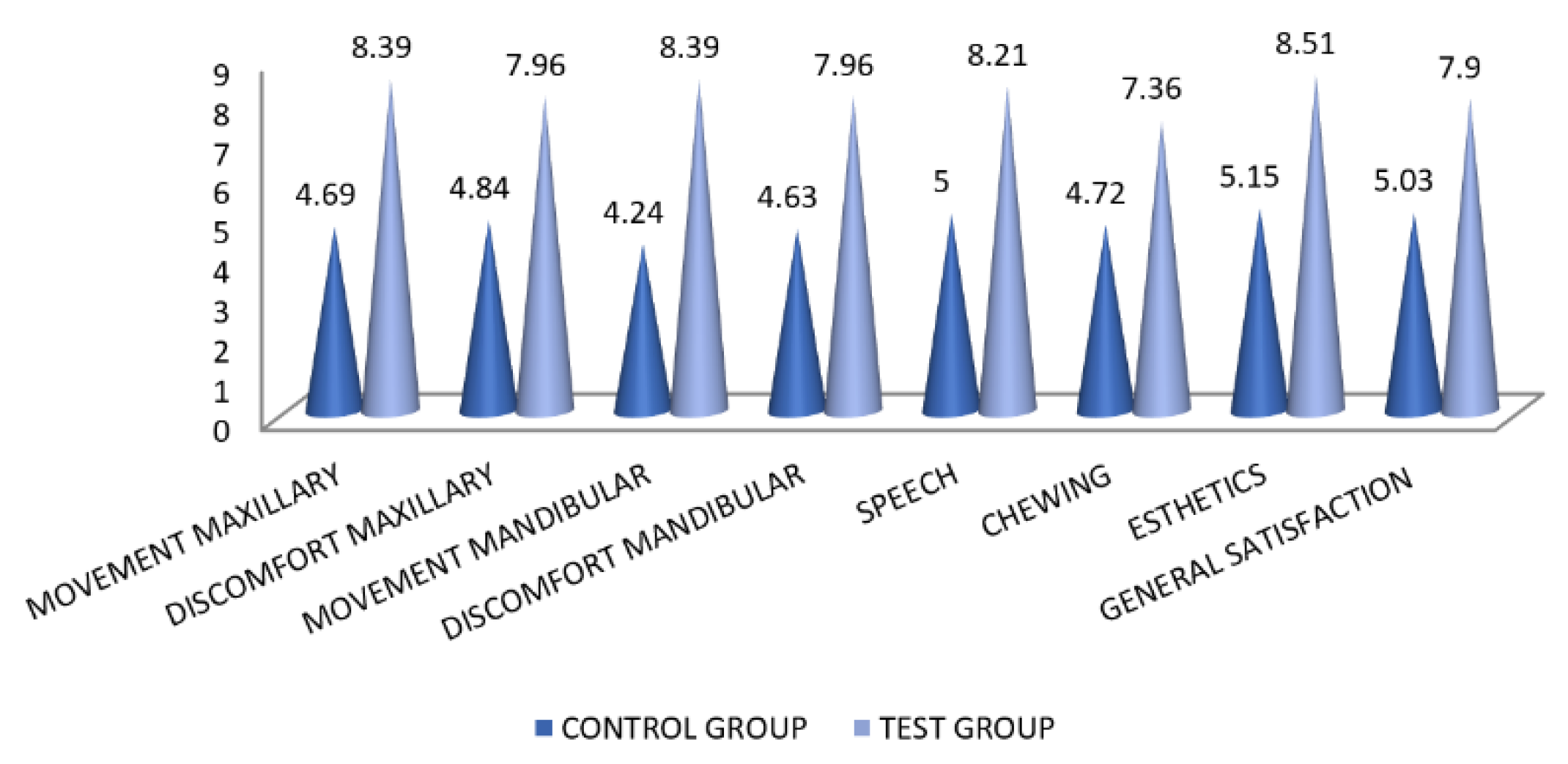
| Group A (Control) | Group B (Test) | Probable Value of t (Unpaired) | KP Correlation Coefficient (r) | |||
|---|---|---|---|---|---|---|
| Parameters | Mean ± SD | SEM | Mean ± SD | SEM | ||
| Movement Maxillary Denture Comfort Maxillary Denture Movement Mandibular Denture Comfort Mandibular Denture Speech Ease of chewing Esthetics General Satisfaction | 4.69 ± 1.286 | 0.2256 | 8.39 ± 0.658 | 0.2256 | 0.0000 * | 0.0715 |
| 4.84 ± 1.372 | 0.2407 | 7.96 ± 0.918 | 0.2407 | 0.0000 * | 0.1699 | |
| 4.24 ± 1.031 | 0.1808 | 8.39 ± 0.658 | 0.1808 | 0.0000 * | 0.0390 * | |
| 4.64 ± 1.245 | 0.2184 | 7.96 ± 0.918 | 0.2184 | 0.0000 * | 0.1465 | |
| 5 ± 1.118 | 0.1961 | 8.21 ± 0.780 | 0.1961 | 0.0000 * | 0.0002 * | |
| 4.72 ± 1.125 | 0.1973 | 7.36 ± 0.895 | 0.1973 | 0.0000 * | 0.1946 | |
| 5.15 ± 1.121 | 0.1966 | 8.51 ± 0.667 | 0.1966 | 0.0000 * | −0.2329 | |
| 5.03 ± 1.103 | 0.1935 | 7.90 ± 0.630 | 0.1935 | 0.0000 * | 0.0408 * | |
| Parameter | Clinical Guidelines |
|---|---|
| Attitude | Patience and tolerance during history taking Clear and slow speech (words) that have low tone Do not infantilize the patient Do not subscribe patient to any ageing myth or attitude (forgetfulness, dependency, unproductivity, unattractiveness) Respect ethnic, cultural, and religious differences between the patient and yourself Do not disbelieve in what patients say (initially, patients will deny any harm done by someone with them) Interview the patients in the absence of a caregiver Use questions that are neutral and non judgmental in nature Do not allow caregiver to answer questions for the patient |
| Scrutiny | Cuts, bruises, lacerations, dehydration, nutritional deficiency, weight loss, burns Pay close attention to patient–caregiver interactions (verbal and non-verbal—discomfort, silent patient, monosyllabic responses, anxiety, palpitation) Observe the patients’ behavioral responses and body language (fear, disorientation while responding, anger, infantile behavior, agitation, sucking) Look for confusion, withdrawal, frequent denial, implausible tales, and failing to talk openly |
| Ethics | Respect options and choices patient make regarding their situation or about the caregiver Provide a source of emergency assistance and or a safety plan if the need arises Any intervention by a psychologist should be after consulting the patient and the patient’s doctor before deciding any course of action All decisions should be made on weighing the beneficence and maleficence |
| History taking | Look for clues of transgenerational violence (history of domestic violence as perpetrator or victim) Past relationships (death of spouse, partner, child) Family dynamics (number of household members, sources of income, resources)Education levels, employment, and financial status, Substance abuse among patient and/or family member Sexual history |
| Intervention | Psychoeducational—improves caregiver’s knowledge about themselves, care recipients, and the environment. Focus on teaching caregiver to develop skills to deal with stress Psychotherapeutic—involves individual counselling to caregivers by trained professionals and teaches coping skills and problem solving Supportive—to build support systems or networks among caregivers and create an environment for them to discuss and share Service based—facilitate caregivers’ use of formal services, improving competence of care recipients and delaying institutionalization of care recipients |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garg, R.; Mattoo, K.; Kumar, L.; Khalid, I.; Baig, F.; Elnager, M.; Faridi, M.A. Impact of Sensitization of Family Caregivers upon Treatment Compliance among Geriatric Patients Suffering from Elder Abuse and Neglect. Healthcare 2021, 9, 226. https://doi.org/10.3390/healthcare9020226
Garg R, Mattoo K, Kumar L, Khalid I, Baig F, Elnager M, Faridi MA. Impact of Sensitization of Family Caregivers upon Treatment Compliance among Geriatric Patients Suffering from Elder Abuse and Neglect. Healthcare. 2021; 9(2):226. https://doi.org/10.3390/healthcare9020226
Chicago/Turabian StyleGarg, Rishabh, Khurshid Mattoo, Lakshya Kumar, Imran Khalid, Fawaz Baig, Mutassim Elnager, and Mukram Ali Faridi. 2021. "Impact of Sensitization of Family Caregivers upon Treatment Compliance among Geriatric Patients Suffering from Elder Abuse and Neglect" Healthcare 9, no. 2: 226. https://doi.org/10.3390/healthcare9020226
APA StyleGarg, R., Mattoo, K., Kumar, L., Khalid, I., Baig, F., Elnager, M., & Faridi, M. A. (2021). Impact of Sensitization of Family Caregivers upon Treatment Compliance among Geriatric Patients Suffering from Elder Abuse and Neglect. Healthcare, 9(2), 226. https://doi.org/10.3390/healthcare9020226