
Impact of Economic Accessibility on Realized Utilization of Home-Based Healthcare Services for the Older Adults in China



Abstract
1. Introduction
2. Literature Review and Hypothesis
2.1. Realized Utilization
2.2. Economic Accessibility
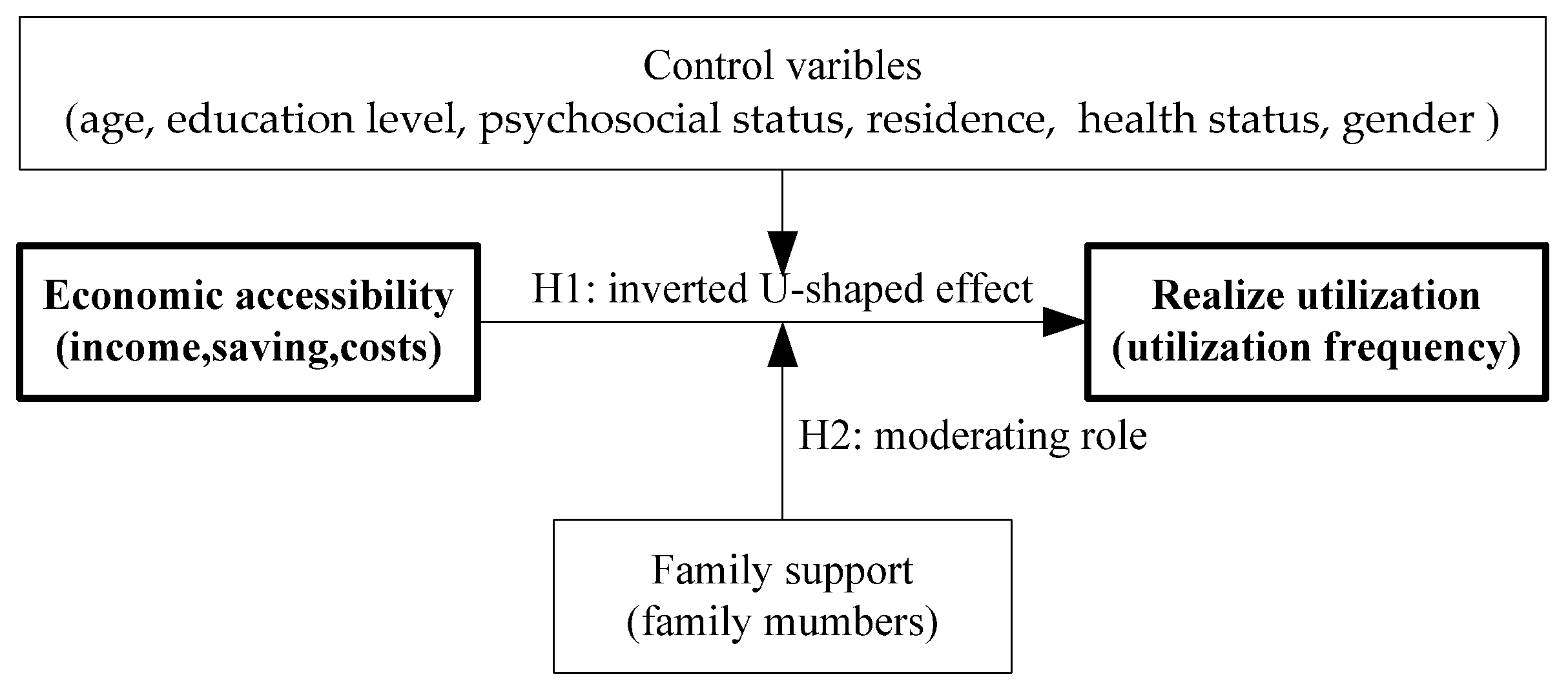
2.3. Economic Accessibility and Realized Utilization
2.4. Family Support, Economic Accessibility and Realized Utilization
3. Data and Variables
3.1. Data Resource
3.2. Variable Description
4. Results and Discussion
4.1. Accessibility on Realized Utilization
4.2. The Moderating Role of Family Support
4.3. Discussion
5. Conclusion and Limitations
5.1. Conclusion
5.2. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feng, J.; Song, H.; Wang, Z. The elderly’s response to a patient cost-sharing policy in health insurance: Evidence from China. J. Econ. Behav. Organ. 2019, 169, 189–207. [Google Scholar] [CrossRef]
- Esther, P.; Archibong, G.E.; Bassey, B.E.; Eneji, R. Income level and healthcare utilization in Calabar Metropolis of Cross River State, Nigeria. Heliyon 2020, 6, e04983. [Google Scholar] [CrossRef]
- Ren, J.; Ding, D.; Wu, Q.; Liu, C.; Hao, Y.; Cui, Y.; Sun, H.; Ning, N.; Li, Y.; Kang, Z.; et al. Financial Affordability, Health Insurance, and Use of Health Care Services by the Elderly: Findings from the China Health and Retirement Longitudinal Study. Asia Pac. J. Public Health 2019, 31, 510–521. [Google Scholar] [CrossRef] [PubMed]
- Bridget, M.J.; Burke, S.; Barry, S.; Normand, C.; Fhallúin, M.N.; Thomas, S. Private health expenditure in Ireland: Assessing the affordability of private financing of health care. Health Policy 2019, 123, 963–969. [Google Scholar] [CrossRef]
- Call, K.T.; Conmy, A.; Alarcon, G.; Hagge, S.L.; Simon, A.B. Health insurance literacy: How best to measure and does it matter to health care access and affordability? Res. Soc. Adm. Pharm. 2020. [Google Scholar] [CrossRef]
- Anderson, R. A Behavioral Model of Families’ Use of Health Services; Research Series No. A25; Center for Health Administration Studies; University of Chicago: Chicago, IL, USA, 1968; p. 125. [Google Scholar]
- Bronkhorst, B. How ‘healthy’ are healthcare organizations? Exploring employee healthcare utilization rates among Dutch healthcare organizations. Health Serv. Manag. Res. 2017, 30, 156–167. [Google Scholar] [CrossRef]
- Lehnert, T. Review: Health Care Utilization and Costs of Elderly Persons with Multiple Chronic Conditions. Med Care Res. Rev. 2011, 68, 387–420. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Xu, X.; Zhang, C.; Chen, L. Factors Influencing Long-Term Care Service Needs among the Elderly Based on the Latest Anderson Model: A Case Study from the Middle and Upper Reaches of the Yangtze River. Healthcare 2019, 7, 157. [Google Scholar] [CrossRef] [PubMed]
- Gyasi, R.M.; Phillips, D.R.; Buor, D. The Role of a Health Protection Scheme in Health Services Utilization Among Community-Dwelling Older Persons in Ghana. J. Gerontol. Ser. B 2020, 75, 661–673. [Google Scholar] [CrossRef]
- Bähler, C.; Huber, C.A.; Brüngger, B.; Reiche, O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: A claims data based observational study. BMC Health Serv. Res. 2015, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.B.; Hsu, J.; Boerma, T. Universal health coverage and universal access. Bull. World Health Organ. 2013, 91, 546. [Google Scholar] [CrossRef]
- Niëns, L.M.; Brouwer, W.B.F. Measuring the affordability of medicines: Importance and challenges. Health Policy 2013, 112, 45–52. [Google Scholar] [CrossRef]
- Ronelle, B.; Carmen, C. Access to health care in post-apartheid South Africa: Availability, affordability, acceptability. Health Econ. Policy Law 2020, 15, 43–55. [Google Scholar] [CrossRef]
- Osborn, R.; Squires, D.; Doty, M.M.; Sarnak, D.O.; Schneider, E.C. In New Survey of Eleven Countries, US Adults Still Struggle with Access to And Affordability of Health Care. Health Aff. 2016, 35, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- Rinshu, D.; Jalandhar, P. Does affordability matter? Examining the trends and patterns in health care expenditure in India. Health Serv. Manag. Res. 2020, 33, 207–218. [Google Scholar] [CrossRef]
- Snowden, M.; Blankenau, J.; Nitzke, J. Healthcare Affordability and Access in Nebraska after the Great Recession. Great Plains Res. 2014, 24, 23–35. [Google Scholar] [CrossRef]
- Bose, M.; Banerjee, S. Equity in distribution of public subsidy for non-communicable diseases among the elderly in India: An application of benefit incidence analysis. BMC Public Health 2019, 19, 1735. [Google Scholar] [CrossRef] [PubMed]
- Zavras, D. Studying Healthcare Affordability during an Economic Recession: The Case of Greece. Int. J. Environ. Res. Public Health 2020, 17, 7790. [Google Scholar] [CrossRef]
- Mukherjee, K. Impact of affordability on accessibility of medical care post affordable care act in the USA. J. Pharm. Health Serv. Res. 2016, 7, 123–128. [Google Scholar] [CrossRef]
- Siddiquee, M.S.H.; Ali, A.M. Healthcare-Seeking Behavior and Out-of-Pocket Payments in Rural Bangladesh: A Cross-Sectional Analysis. Psychol. Behav. Sci. 2018, 7, 45. [Google Scholar] [CrossRef]
- Haw, N.J.L.; Uy, J.; Ho, B.L. Association of SHI coverage and level of healthcare utilization and costs in the Philippines: A 10-year pooled analysis. J. Public Health 2020, 42, e496–e505. [Google Scholar] [CrossRef]
- Tsuchiya-Ito, R.; Ishizaki, T.; Mitsutake, S.; Hamada, S.; Yoshie, S.; Iijima, K.; Tamiya, N. Association of household income with home-based rehabilitation and home help service utilization among long-term home care service users. BMC Geriatr. 2020, 20, 314. [Google Scholar] [CrossRef]
- Habibov, N. What determines healthcare utilization and related out-of-pocket expenditures in Tajikistan? Lessons from a national survey. Int. J. Public Health 2009, 54, 260–266. [Google Scholar] [CrossRef]
- Haans, R.F.; Pieters, C.; He, Z.L. Thinking about U: Theorizing and testing U-and inverted U-shaped relationships in strategy research. Strateg. Manag. J. 2016, 37, 1177–1195. [Google Scholar] [CrossRef]
- Miyawaki, A.; Kobayashi, Y.; Noguchi, H.; Watanabe, T.; Takahashi, H.; Tamiya, N. Effect of reduced formal care availability on formal/informal care patterns and caregiver health: A quasi-experimental study using the Japanese long-term care insurance reform. BMC Geriatr. 2020, 20, 207. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Liu, J.; Liu, C. Changes in Perceived Accessibility to Healthcare from the Elderly between 2005 and 2014 in China: An Oaxaca–Blinder Decomposition Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3824. [Google Scholar] [CrossRef] [PubMed]
- Nekehia, Q.T.; Pothisiri, W. Rural-urban gaps in health care utilization among older Thais: The role of family support. Arch. Gerontol. Geriatr. 2019, 81, 201–208. [Google Scholar] [CrossRef]
- Chen, J.; Vargas-Bustamante, A.; Mortensen, K.; Ortega, A.N. Racial and Ethnic Disparities in Health Care Access and Utilization Under the Affordable Care Act. Med. Care 2016, 54, 140–146. [Google Scholar] [CrossRef]
- Beal, D.; Foli, K.J. Affordability in individuals’ healthcare decision making: A concept analysis. Nurs. Forum 2020, 56, 188–193. [Google Scholar] [CrossRef]
- Wang, L.; Yang, L.; Di, X.; Dai, X. Family Support, Multidimensional Health, and Living Satisfaction among the Elderly: A Case from Shaanxi Province, China. Int. J. Environ. Res. Public Health 2020, 17, 8434. [Google Scholar] [CrossRef]
- Ma, L. Research on the Elderly’s Demands for the Old-age Care Services. Soc. Sci. 2019, 8, 44. [Google Scholar] [CrossRef]
- Mulaa, O.E.; Odhiambo, O.M. Out-Of-Pocket Health Expenditure Among the Elderly in Kenya. Glob. J. Health Sci. 2020, 12, 53. [Google Scholar] [CrossRef]
- Lundberg, J.; Kristenson, M. Is Subjective Status Influenced by Psychosocial Factors? Soc Indic. Res. 2008, 89, 375–390. [Google Scholar] [CrossRef]
- Bifan, Z.; Fen, L.; Linan, W.; Changying, W.; Chunlin, J. Patterns of Expenditure in Healthcare for Elderly in Shanghai. China Rep. 2020, 56, 334–353. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Indicator | Item | Options (Data) | Frequency | Percentage (%) | Mean | Median | Standard Deviation |
|---|---|---|---|---|---|---|---|---|
| Dependent variable | Realized utilization | The utilization frequency of healthcare services | ① seldom(1) ② sometimes(2) ③ often (3) ④ usually(4) ⑤ always(5) | 56 243 270 183 80 | 6.73 29.21 32.45 21.99 9.62 | 2.99 | 3 | 1.08 |
| Independent variable | Economic accessibility | Affordability of healthcare services costs | ① totally not(1) ② partly not(2) ③ can(3) ④ most(4) ⑤ totally(5) | 226 161 159 232 54 | 27.16 19.35 19.11 27.89 6.49 | 3.65 | 4 | 1.21 |
| Moderating variable | Family support | Family members | quantity | 2.67 | 2 | 1.59 | ||
| Control variable | Individual characteristics | Gender | ① male (1) ② female (0) | 346 486 | 41.59 58.41 | |||
| Education level | ① Elementary (1) school and below ② Junior high school(2) ③ high school(3) ④ college(4) ⑤ bachelor degree and above (5) | 373 226 164 48 21 | 44.83 27.17 19.71 5.77 2.52 | |||||
| Psychosocial status | ① very bad(1) ② bad (2) ③ neither good, nor bad (3) ④ good (4) ⑤ very good (5) | 6 51 91 303 381 | 0.72 6.13 10.94 36.42 45.79 | 4.20 | 4 | 0.92 | ||
| Residence | ① urban (1) ② rural (0) | 472 360 | 56.73 43.27 | |||||
| Health status | ① very bad(1) ② bad (2) ③ neither good, nor bad (3) ④ good (4) ⑤ very good(5) | 39 153 227 278 134 | 4.69 18.39 27.40 33.41 16.11 | 3.38 | 3 | 1.10 | ||
| Age | ① 60–64 (1) ② 65–69 (2) ③ 70–74 (3) ④ 75–79 (4) ⑤ 80 and above (5) | 164 193 172 127 176 | 19.71 23.20 20.67 15.27 21.15 |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | |
|---|---|---|---|---|---|---|
| 1- squared | −0.0721 * (−1.8441) | −0.0699 * (−1.7848) | −0.0720 * (−1.8346) | −0.0699 * (−1.7823) | −0.0717 * (−1.8261) | −0.0677 * (−1.7208) |
| economic accessibility | 0.5767 ** (2.2655) | 0.5903 ** (2.3149) | 0.5448 ** (2.1296) | 0.5358 ** (2.0952) | 0.5447 ** (2.1279) | 0.5352 ** (2.0915) |
| gender | 0.1190 (0.9418) | 0.2275 * (1.7518) | 0.1976 (1.5184) | 0.1825 (1.3995) | 0.1737 (1.3279) | 0.1691 (1.2918) |
| education level | −0.2328 *** (−3.7377) | −0.2453 *** (−3.9377) | −0.2045 *** (−3.0451) | −0.2120 *** (−3.1281) | −0.2039 *** (−3.0021) | |
| psychosocial status | 0.3214 *** (4.5541) | 0.3261 *** (4.6127) | 0.3081 *** (4.1870) | 0.2935 *** (3.9624) | ||
| residence | −0.2228 (−1.6250) | −0.2278 * (−1.6612) | −0.2537 * (−1.8395) | |||
| health status | 0.0543 (0.8849) | 0.0788 (1.2569) | ||||
| age | 0.0851 * (1.8716) | |||||
| cut1 | −1.5637 *** (−3.9130) | −1.9115*** (−4.6472) | −0.8414** (−1.7814) | −0.8818* (−1.8660) | −0.7914 (−1.6363) | −0.4993 (−0.9828) |
| cut2 | 0.5021 (1.2921) | 0.1744 (0.4371) | 1.2704 *** (2.7250) | 1.2348 *** (2.6482) | 1.3236 *** (2.7733) | 1.6210 *** (3.2227) |
| cut3 | 1.8654 *** (4.7270) | 1.5517 ** (3.8433) | 2.6774 *** (5.6404) | 2.6453 *** (5.5730) | 2.7354 *** (5.6299) | 3.0392 *** (5.9293) |
| cut 4 | 3.3402 *** (8.2046) | 3.0361 *** (7.3066) | 4.1831 *** (8.5784) | 4.1527 *** (8.5168) | 4.2457 *** (8.5039) | 4.5514 *** (8.6552) |
| log likelihood | −1213.74 | −1206.69 | −1196.19 | −1194.87 | −1194.48 | −1192.73 |
| LR | 9.65 ** | 23.67 *** | 44.66 *** | 47.30 *** | 48.09 *** | 51.59 *** |
| Model 7 | Model 8 | Model 9 | Model 10 | Model 11 | Model 12 | Model 13 | |
|---|---|---|---|---|---|---|---|
| economic accessibility(squared) | −0.1412 *** (−2.6179) | −0.1321 ** (−2.4531) | −0.1456 *** (−2.6961) | −0.1388 ** (−2.5617) | −0.1444 *** (−2.6580) | −0.1395 ** (−2.5643) | −0.2321 *** (−3.8797) |
| economic accessibility | 0.9848 *** (3.2557) | 0.9672 *** (3.2044) | 0.9749 *** (3.2200) | 0.9455 *** (3.1200) | 0.9753 *** (3.2094) | 0.9597 *** (3.1589) | 1.6330 *** (4.6535) |
| family members×economic accessibility(squared) | 0.0259 ** (1.9984) | 0.0238 * (1.8381) | 0.0276 ** (2.1269) | 0.0260 ** (1.9959) | 0.0270 ** (2.0697) | 0.0266 ** (2.0419) | 0.0593 *** (3.6903) |
| family members×economic accessibility | −0.1486 *** (−2.6752) | −0.1407 ** (−2.5278) | −0.1586 *** (−2.8448) | −0.1524 *** (−2.7239) | −0.1580 *** (−2.8155) | −0.1557 *** (−2.7798) | −0.3911 *** (−4.4584) |
| gender | 0.1624 (1.2769) | 0.2702 ** (2.0678) | 0.2390 * (1.8259) | 0.2260 * (1.7234) | 0.2135 (1.6230) | 0.2093 (1.5906) | 0.0222 (0.5296) |
| education level | −0.2320 *** (−3.7091) | −0.2437 *** (−3.8941) | −0.2042 *** (−3.0300) | −0.2158 *** (−3.1706) | −0.2077 *** (−3.0450) | −0.0305 (−1.3707) | |
| psychosocial status | 0.3420 *** (4.8255) | 0.3461 *** (4.8766) | 0.3186 *** (4.3223) | 0.3053 *** (4.1160) | 0.0599 ** (2.5125) | ||
| residence | −0.2171 (−1.5781) | −0.2256 (−1.6389) | −0.2503 * (−1.8082) | −0.0814 * (−1.8505) | |||
| health status | 0.0853 (1.3819) | 0.1077 * (1.7066) | 0.0400 * (1.9148) | ||||
| age | 0.0790 * (1.7313) | 0.0307 ** (2.0870) | |||||
| cut 1 | −1.5387 *** (−3.8366) | −1.8959 *** (−4.5853) | −0.7427 ** (−1.5612) | −0.7889 * (−1.6569) | −0.6418 (−1.3146) | −0.3713 (−0.7246) | −0.6485 (−1.3665) |
| cut 2 | 0.5476 (1.4049) | 0.2082 (0.5193) | 1.3897 *** (2.9594) | 1.3475 *** (2.8679) | 1.4929 *** (3.0974) | 1.7677 *** (3.4833) | 1.4695 *** (3.1356) |
| cut 3 | 1.9368 *** (4.8881) | 1.6116 *** (3.9698) | 2.8267 *** (5.9054) | 2.7878 *** (5.8224) | 2.9362 *** (5.9755) | 3.2166 *** (6.2131) | 2.8881 *** (6.0420) |
| cut 4 | 3.4287 *** (8.3813) | 3.1158 *** (7.4538) | 4.3558 *** (8.8495) | 4.3190 *** (8.7728) | 4.4726 *** (8.8476) | 4.7544 *** (8.9429) | 4.3987 *** (8.9516) |
| log likelihood | −1204.70 | −1197.76 | −1185.96 | −1184.72 | −1183.76 | −1182.26 | −1193.62 |
| LR | 27.65 *** | 41.53 *** | 65.12 *** | 67.62 *** | 69.53 *** | 72.53 *** | 49.80 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di, X.; Wang, L.; Yang, L.; Dai, X. Impact of Economic Accessibility on Realized Utilization of Home-Based Healthcare Services for the Older Adults in China. Healthcare 2021, 9, 218. https://doi.org/10.3390/healthcare9020218
Di X, Wang L, Yang L, Dai X. Impact of Economic Accessibility on Realized Utilization of Home-Based Healthcare Services for the Older Adults in China. Healthcare. 2021; 9(2):218. https://doi.org/10.3390/healthcare9020218
Chicago/Turabian StyleDi, Xiaodong, Lijian Wang, Liu Yang, and Xiuliang Dai. 2021. "Impact of Economic Accessibility on Realized Utilization of Home-Based Healthcare Services for the Older Adults in China" Healthcare 9, no. 2: 218. https://doi.org/10.3390/healthcare9020218
APA StyleDi, X., Wang, L., Yang, L., & Dai, X. (2021). Impact of Economic Accessibility on Realized Utilization of Home-Based Healthcare Services for the Older Adults in China. Healthcare, 9(2), 218. https://doi.org/10.3390/healthcare9020218