
Postural Sway in Older Patients with Sagittal Imbalance and Young Adults during Local Vibratory Proprioceptive Stimulation

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Postural Control Assessment
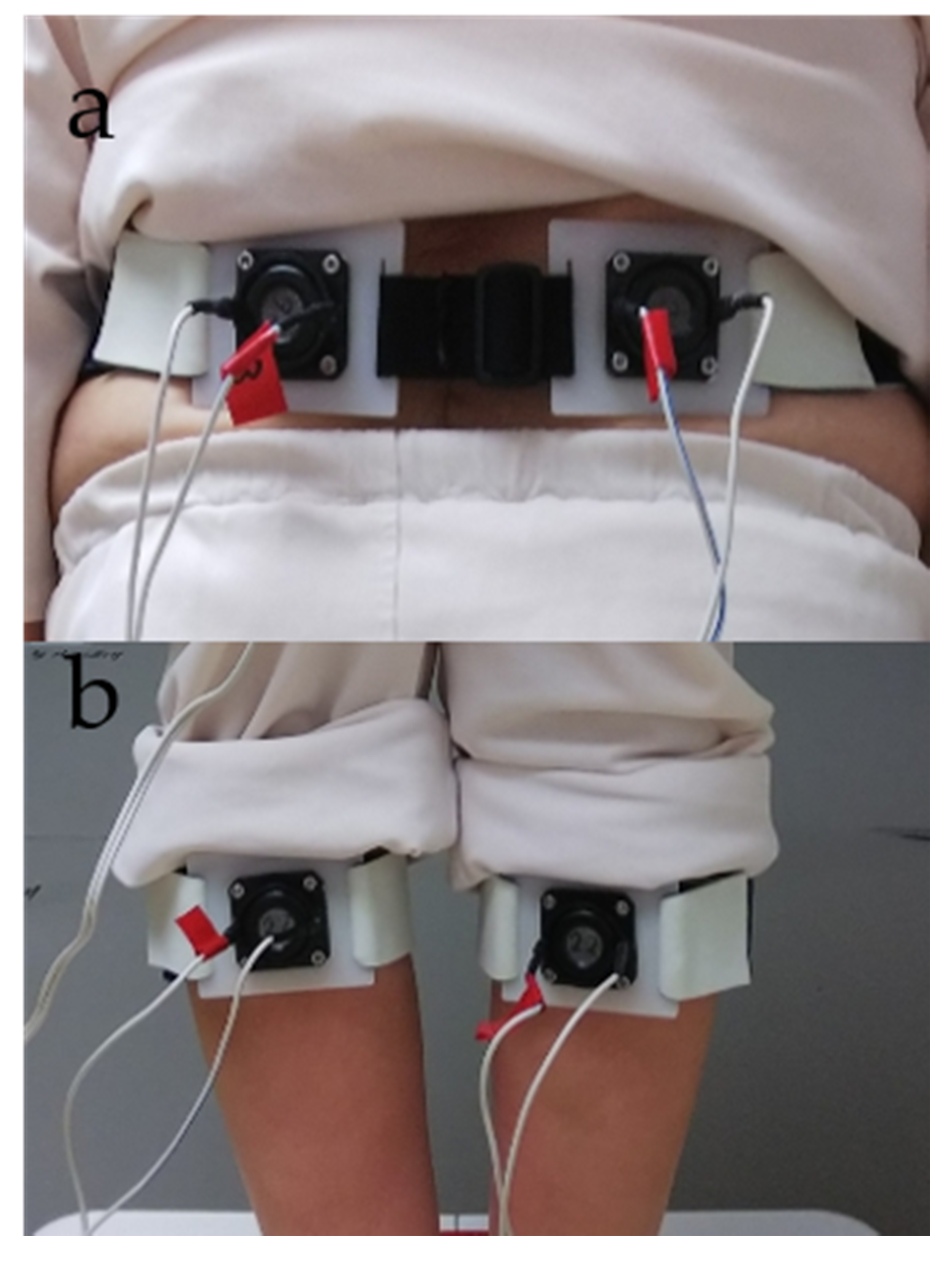
2.3. Muscle Vibration
- Measurement of postural sway during stimulation to GS or LM (30 s)
- A sitting rest (60 s)
- Measurement of postural sway during stimulation to GS or LM (30 s).
2.4. Low Back Pain Assessment
2.5. Sagittal Imbalance
2.6. Statistical Analysis
2.7. Sample Size
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schwab, F.; Patel, A.; Ungar, B.; Farcy, J.-P.; Lafage, V. Adult Spinal Deformity—Postoperative Standing Imbalance. Spine 2010, 35, 2224–2231. [Google Scholar] [CrossRef] [PubMed]
- Vaugoyeau, M.; Viel, S.; Amblard, B.; Azulay, J.; Assaiante, C. Proprioceptive contribution of postural control as assessed from very slow oscillations of the support in healthy humans. Gait Posture 2008, 27, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Schwab, F.; Dubey, A.; Gamez, L.; El Fegoun, A.B.; Hwang, K.; Pagala, M.; Farcy, J.-P. Adult Scoliosis: Prevalence, SF-36, and Nutritional Parameters in an Elderly Volunteer Population. Spine 2005, 30, 1082–1085. [Google Scholar] [CrossRef] [PubMed]
- Glassman, S.D.; Bridwell, K.; Dimar, J.R.; Horton, W.; Berven, S.; Schwab, F. The Impact of Positive Sagittal Balance in Adult Spinal Deformity. Spine 2005, 30, 2024–2029. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Miyakoshi, N.; Kasukawa, Y.; Hongo, M.; Shimada, Y. Spinal sagittal contour affecting falls: Cut-off value of the lumbar spine for falls. Gait Posture 2013, 38, 260–263. [Google Scholar] [CrossRef]
- Ito, T.; Sakai, Y.; Ito, Y.; Yamazaki, K.; Morita, Y. Association Between Back Muscle Strength and Proprioception or Mechanoreceptor Control Strategy in Postural Balance in Elderly Adults with Lumbar Spondylosis. Healthcare 2020, 8, 58. [Google Scholar] [CrossRef]
- Jackson, R.P.; McManus, A.C. Radiographic Analysis of Sagittal Plane Alignment and Balance in Standing Volunteers and Patients with Low Back Pain Matched for Age, Sex, and Size. Spine 1994, 19, 1611–1618. [Google Scholar] [CrossRef]
- Diebo, B.G.; Henry, J.; Lafage, V.; Berjano, P. Sagittal deformities of the spine: Factors influencing the outcomes and complications. Eur. Spine J. 2014, 24, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Diebo, B.G.; Shah, N.V.; Stroud, S.G.; Paulino, C.B.; Schwab, F.J.; Lafage, V. Realignment surgery in adult spinal deformity. Der Orthopäde 2018, 47, 301–309. [Google Scholar] [CrossRef]
- Lamartina, C.; Berjano, P. Classification of sagittal imbalance based on spinal alignment and compensatory mechanisms. Eur. Spine J. 2014, 23, 1177–1189. [Google Scholar] [CrossRef]
- Maciałczyk-Paprocka, K.; Krzyżaniak, A.; Kotwicki, T.; Kałużny, Ł.I.; Przybylski, J. The body posture of preschool children. Probl. Hig. Epidemiol. 2011, 92, 286–290. [Google Scholar]
- Rajnics, P.; Templier, A.; Skalli, W.; Lavaste, F.; Illés, T. The Association of Sagittal Spinal and Pelvic Parameters in Asymptomatic Persons and Patients with Isthmic Spondylolisthesis. J. Spinal Disord. Tech. 2002, 15, 24–30. [Google Scholar] [CrossRef]
- Vaz, G.; Roussouly, P.; Berthonnaud, E.; Dimnet, J. Sagittal morphology and equilibrium of pelvis and spine. Eur. Spine J. 2001, 11, 80–87. [Google Scholar] [CrossRef]
- Weiss, H.-R.; Turnbull, D.; Bohr, S. Brace treatment for patients with Scheuermann’s disease—A review of the literature and first experiences with a new brace design. Scoliosis 2009, 4, 22. [Google Scholar] [CrossRef]
- Simoneau, M.; Mercier, P.; Blouin, J.; Allard, P.; Teasdale, N. Altered sensory-weighting mechanisms is observed in adolescents with idiopathic scoliosis. BMC Neurosci. 2006, 7, 68. [Google Scholar] [CrossRef]
- Yagi, M.; Ohne, H.; Kaneko, S.; Machida, M.; Yato, Y.; Asazuma, T. Does corrective spine surgery improve the standing balance in patients with adult spinal deformity? Spine J. 2018, 18, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Arima, H.; Yamato, Y.; Hasegawa, T.; Kobayashi, S.; Yoshida, G.; Yasuda, T.; Banno, T.; Oe, S.; Mihara, Y.; Togawa, D.; et al. Extensive Corrective Fixation Surgeries for Adult Spinal Deformity Improve Posture and Lower Extremity Kinematics During Gait. Spine 2017, 42, 1456–1463. [Google Scholar] [CrossRef]
- Lee, M.-Y.; Lee, H.-Y.; Yong, M.-S. Characteristics of Cervical Position Sense in Subjects with Forward Head Posture. J. Phys. Ther. Sci. 2014, 26, 1741–1743. [Google Scholar] [CrossRef]
- Ito, T.; Sakai, Y.; Morita, Y.; Yamazaki, K.; Igarashi, K.; Nishio, R.; Sato, N. Proprioceptive Weighting Ratio for Balance Control in Static Standing Is Reduced in Elderly Patients With Non–Specific Low Back Pain. Spine 2018, 43, 1704–1709. [Google Scholar] [CrossRef]
- Brumagne, S.; Cordo, P.; Verschueren, S. Proprioceptive weighting changes in persons with low back pain and elderly persons during upright standing. Neurosci. Lett. 2004, 366, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Brumagne, S.; Janssens, L.; Janssens, E.; Goddyn, L. Altered postural control in anticipation of postural instability in persons with recurrent low back pain. Gait Posture 2008, 28, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Godzik, J.; Frames, C.W.; Hussain, V.S.; Olson, M.C.; Kakarla, U.K.; Uribe, J.S.; Lockhart, T.E.; Turner, J.D. Postural Stability and Dynamic Balance in Adult Spinal Deformity: Prospective Pilot Study. World Neurosurg. 2020, 141, e783–e791. [Google Scholar] [CrossRef]
- Brumagne, S.; Lysens, R.; Swinnen, S.; Verschueren, S. Effect of Paraspinal Muscle Vibration on Position Sense of the Lumbosacral Spine. Spine 1999, 24, 1328–1331. [Google Scholar] [CrossRef] [PubMed]
- Hay, L.; Bard, C.; Fleury, M.; Teasdale, N. Availability of visual and proprioceptive afferent messages and postural control in elderly adults. Exp. Brain Res. 1996, 108, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Mientjes, M.; Frank, J.S. Balance in chronic low back pain patients compared to healthy people under various conditions in upright standing. Clin. Biomech. 1999, 14, 710–716. [Google Scholar] [CrossRef]
- Mok, N.W.; Brauer, S.G.; Hodges, P.W. Hip Strategy for Balance Control in Quiet Standing Is Reduced in People With Low Back Pain. Spine 2004, 29, E107–E112. [Google Scholar] [CrossRef]
- Ito, T.; Sakai, Y.; Yamazaki, K.; Nishio, R.; Ito, Y.; Morita, Y. Postural Strategy in Elderly, Middle-Aged, and Young People during Local Vibratory Stimulation for Proprioceptive Inputs. Geriatrics 2018, 3, 93. [Google Scholar] [CrossRef]
- Ito, T.; Sakai, Y.; Nishio, R.; Ito, Y.; Yamazaki, K.; Morita, Y. Postural sway in adults and elderly individuals during local vibratory stimulation of the somatosensory system. S.N. Compr. Clin. Med. 2020, 2, 753–758. [Google Scholar] [CrossRef]
- Pinto, S.M.; Cheung, J.P.Y.; Samartzis, D.; Karppinen, J.; Zheng, Y.-P.; Pang, M.Y.C.; Wong, A.Y.L. Differences in Proprioception Between Young and Middle-Aged Adults With and Without Chronic Low Back Pain. Front. Neurol. 2020, 11, 605787. [Google Scholar] [CrossRef]
- Claeys, K.; Brumagne, S.; Dankaerts, W.; Kiers, H.; Janssens, L. Decreased variability in postural control strategies in young people with non-specific low back pain is associated with altered proprioceptive reweighting. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 111, 115–123. [Google Scholar] [CrossRef]
- Bacciu, D.; Chessa, S.; Gallicchio, C.; Micheli, A.; Pedrelli, L.; Ferro, E.; Fortunati, L.; La Rosa, D.; Palumbo, F.; Vozzi, F.; et al. A learning system for automatic Berg Balance Scale score estimation. Eng. Appl. Artif. Intell. 2017, 66, 60–74. [Google Scholar] [CrossRef]
- Clark, R.A.; Bryant, A.L.; Pua, Y.; McCrory, P.; Bennell, K.; Hunt, M. Validity and reliability of the Nintendo Wii Balance Board for assessment of standing balance. Gait Posture 2010, 31, 307–310. [Google Scholar] [CrossRef]
- Young, W.; Ferguson, S.; Brault, S.; Craig, C. Assessing and training standing balance in older adults: A novel approach using the ‘Nintendo Wii’ Balance Board. Gait Posture 2011, 33, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Nishio, R.; Ito, Y.; Morita, Y.; Ito, T.; Yamazaki, K.; Sakai, Y. Ito Investigation of the Functional Decline in Proprioceptors for Low Back Pain Using the Sweep Frequency Method. Appl. Sci. 2019, 9, 4988. [Google Scholar] [CrossRef]
- Ito, T.; Sakai, Y.; Nishio, R.; Ito, Y.; Yamazaki, K.; Morita, Y. Relationship between postural stability and fall risk in elderly people with lumbar spondylosis during local vibratory stimulation for proprioception: A retrospective study. Somatosens. Mot. Res. 2020, 37, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Dąbrowska, A.; Olszewska-Karaban, M.A.; Permoda-Białozorczyk, A.K.; Szalewska, D.A. The Postural Control Indexes during Unipodal Support in Patients with Idiopathic Scoliosis. BioMed Res. Int. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Willigenburg, N.W.; Kingma, I.; Van Dieën, J.H. Center of pressure trajectories, trunk kinematics and trunk muscle activation during unstable sitting in low back pain patients. Gait Posture 2013, 38, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Poulain, I.; Giraudet, G. Age-related changes of visual contribution in posture control. Gait Posture 2008, 27, 1–7. [Google Scholar] [CrossRef]
- Nashner, L.M. Practical biomechanics and physiology of balance. In Handbook of Balance Function Testing; Jacobson, G.P., Newman, C.W., Kartush, J.M., Eds.; Mosby Year Book: St. Louis, MO, USA, 1993; pp. 261–279. [Google Scholar]
- Goldberg, A.; Hernandez, M.E.; Alexander, N.B. Trunk Repositioning Errors Are Increased in Balance-Impaired Older Adults. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2005, 60, 1310–1314. [Google Scholar] [CrossRef]
- Newcomer, K.L.; Laskowski, E.R.; Yu, B.; Johnson, J.C.; An, K.-N. Differences in Repositioning Error Among Patients With Low Back Pain Compared With Control Subjects. Spine 2000, 25, 2488–2493. [Google Scholar] [CrossRef] [PubMed]
- Refshauge, K.M.; Fitzpatrick, R.C. Perception of movement at the human ankle: Effects of leg position. J. Physiol. 1995, 488, 243–248. [Google Scholar] [CrossRef]
- Burke, D.; Hagbarth, K.E.; Löfstedt, L.; Wallin, B.G. The responses of human muscle spindle endings to vibration of non-contracting muscles. J. Physiol. 1976, 261, 673–693. [Google Scholar] [CrossRef] [PubMed]
- Lao, M.L.; Chow, D.H.; Guo, X.; Cheng, J.C.; Holmes, A.D. Impaired Dynamic Balance Control in Adolescents With Idiopathic Scoliosis and Abnormal Somatosensory Evoked Potentials. J. Pediatr. Orthop. 2008, 28, 846–849. [Google Scholar] [CrossRef] [PubMed]
- Gruber, A.H.; Busa, M.A.; Iii, G.E.G.; Van Emmerik, R.E.; Masso, P.D.; Hamill, J. Time-to-contact and multiscale entropy identify differences in postural control in adolescent idiopathic scoliosis. Gait Posture 2011, 34, 13–18. [Google Scholar] [CrossRef]
- Reeves, N.P.; Narendra, K.S.; Cholewicki, J. Spine stability: The six blind men and the elephant. Clin. Biomech. 2007, 22, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Bergmark, A. Stability of the lumbar spine. Acta Orthop. Scand. 1989, 60, 1–54. [Google Scholar] [CrossRef] [PubMed]
- Drzał-Grabiec, J.; Rachwał, M.; Podgórska-Bednarz, J.; Rykała, J.; Snela, S.; Truszczyńska, A.; Trzaskoma, Z. The effect of spinal curvature on the photogrammetric assessment on static balance in elderly women. BMC Musculoskelet. Disord. 2014, 15, 186. [Google Scholar] [CrossRef]
- Carlsöö, S. The static muscle load in different work positions: An electromyographic study. Ergonomics 1961, 4, 193–211. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Older Patients (n = 27) | Young Adults (n = 27) | Effect Size (r or Cramer’s V) | p-Value |
|---|---|---|---|---|
| Age (years) | 78.0 (65–83) | 20.0 (18–28) | −0.9 | 0.001 |
| Sex (male/female) | 15/12 | 15/12 | 0.0001 | 1.000 |
| Height (cm) | 155.7 (6.8) | 165.2 (6.8) | 0.5 | 0.0001 |
| Weight (kg) | 58.0 (31.6–79.4) | 60.2 (41.7–77.9) | 0.1 | 0.562 |
| BMI (kg/m2) | 23.9 (4.3) | 22.1 (2.4) | 0.3 | 0.059 |
| VAS (cm) | 6.7 (0–10) | 0 (0–2.7) | −0.9 | 0.0001 |
| Older Patients (n = 27) | Young Adults (n = 27) | Effect Size (r) | p-Value | |
|---|---|---|---|---|
| RMS no vibration (mm) | 8.4 (2.8–18.1) | 6.2 (3.1–16.4) | −0.3 | 0.023 |
| RMSGS (mm) | 13.3 (5.0–24.3) | 8.9 (2.9–21.6) | −0.4 | <0.005 |
| RMSLM (mm) | 8.4 (3.2–24.3) | 7.7 (3.3–15.4) | −0.04 | 0.789 |
| RPW (%) | 59.8 (11.1) | 52.3 (14.4) | 0.3 | 0.038 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, T.; Sakai, Y.; Yamazaki, K.; Ito, Y.; Kawai, K.; Kato, Y.; Sugiura, H.; Morita, Y. Postural Sway in Older Patients with Sagittal Imbalance and Young Adults during Local Vibratory Proprioceptive Stimulation. Healthcare 2021, 9, 210. https://doi.org/10.3390/healthcare9020210
Ito T, Sakai Y, Yamazaki K, Ito Y, Kawai K, Kato Y, Sugiura H, Morita Y. Postural Sway in Older Patients with Sagittal Imbalance and Young Adults during Local Vibratory Proprioceptive Stimulation. Healthcare. 2021; 9(2):210. https://doi.org/10.3390/healthcare9020210
Chicago/Turabian StyleIto, Tadashi, Yoshihito Sakai, Kazunori Yamazaki, Yohei Ito, Keitaro Kawai, Yoshiji Kato, Hideshi Sugiura, and Yoshifumi Morita. 2021. "Postural Sway in Older Patients with Sagittal Imbalance and Young Adults during Local Vibratory Proprioceptive Stimulation" Healthcare 9, no. 2: 210. https://doi.org/10.3390/healthcare9020210
APA StyleIto, T., Sakai, Y., Yamazaki, K., Ito, Y., Kawai, K., Kato, Y., Sugiura, H., & Morita, Y. (2021). Postural Sway in Older Patients with Sagittal Imbalance and Young Adults during Local Vibratory Proprioceptive Stimulation. Healthcare, 9(2), 210. https://doi.org/10.3390/healthcare9020210