
Effectiveness and Safety of Botulinum Toxin Type A in Treatment of Restless Legs Syndrome: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Selection and Description
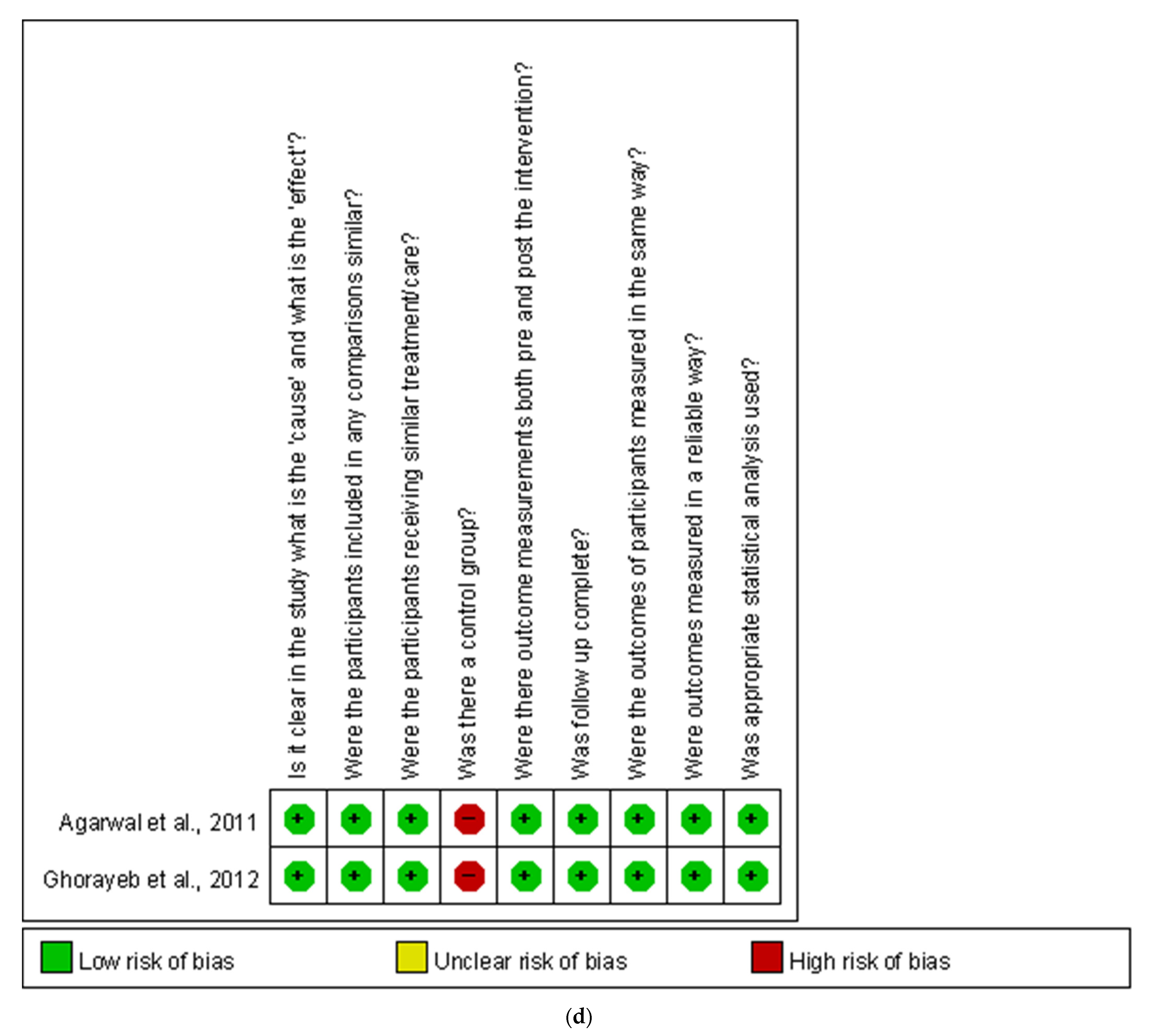
3.2. Risk of Bias Assessment
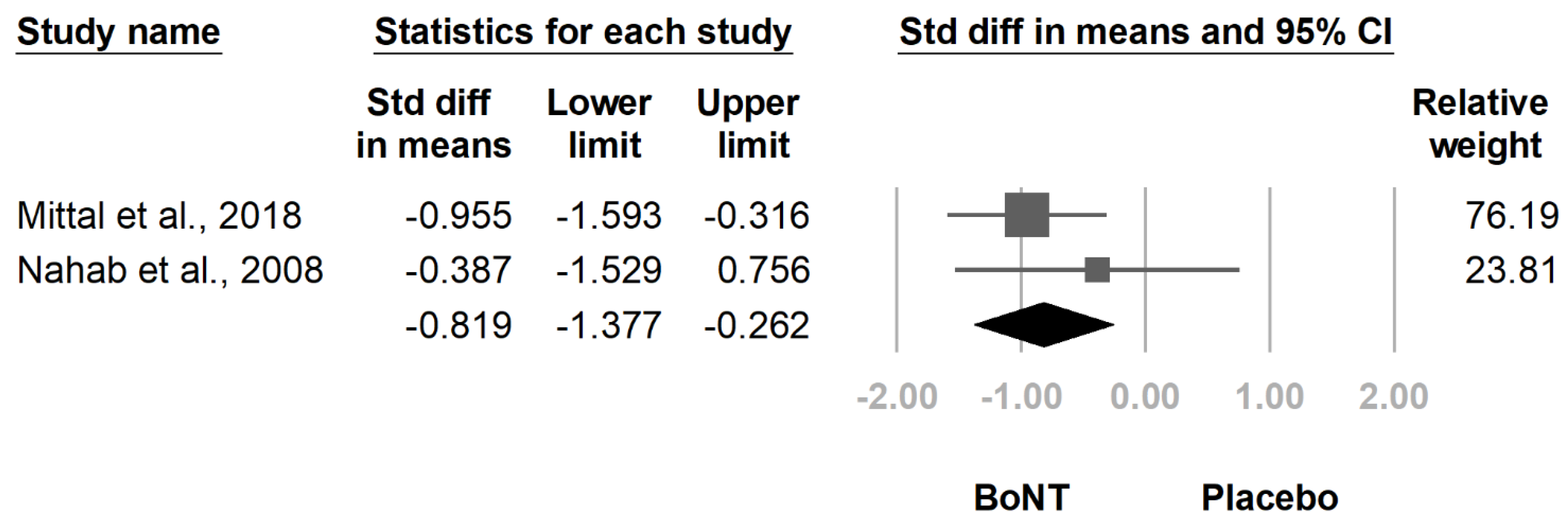
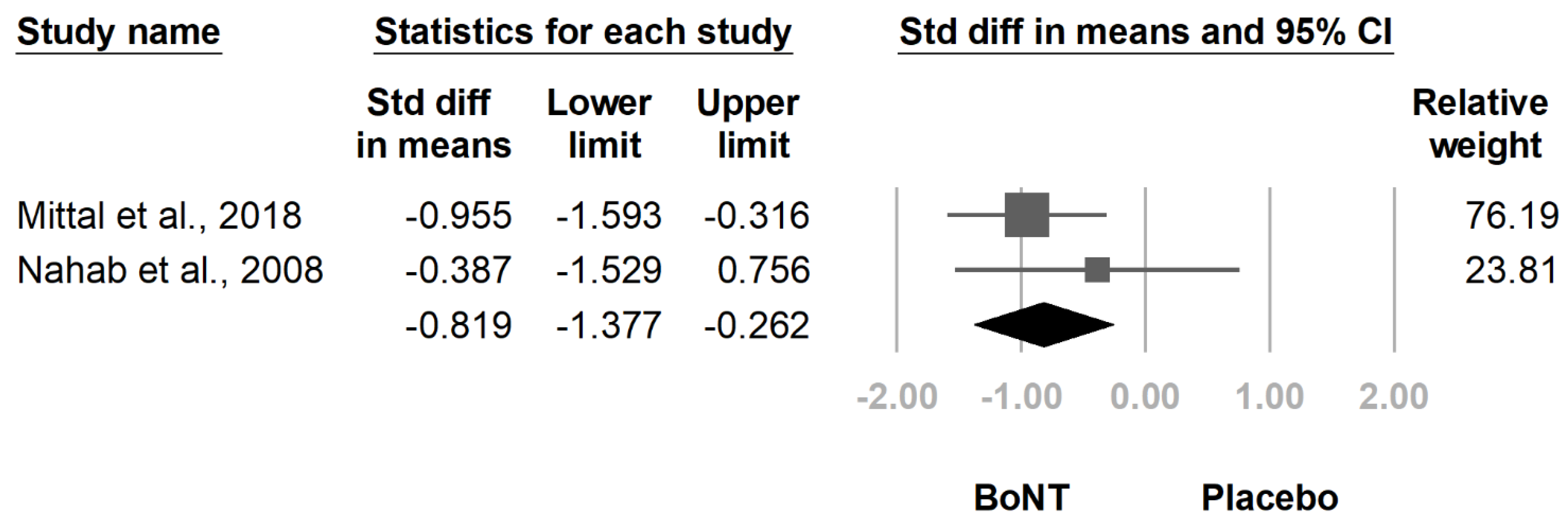
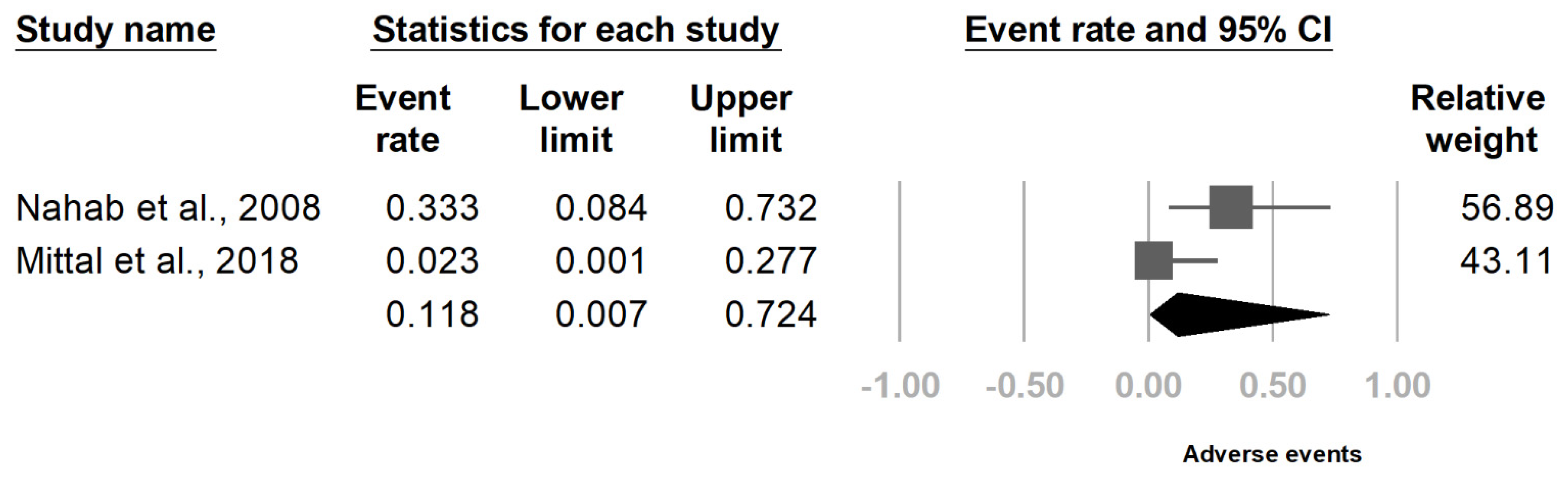
3.3. Results of Quantitative Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yeh, P.; Walters, A.S.; Tsuang, J.W. Restless legs syndrome: A comprehensive overview on its epidemiology, risk factors, and treatment. Sleep Breath. 2012, 16, 987–1007. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M. International Classification of Sleep Disorders-Third Edition. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Allen, R.P.; Picchietti, D.L.; Garcia-Borreguero, D.; Ondo, W.G.; Walters, A.S.; Winkelman, J.W.; Zucconi, M.; Ferri, R.; Trenkwalder, C.; Lee, H.B. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: Updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria--history, rationale, description, and significance. Sleep Med. 2014, 15, 860–873. [Google Scholar] [CrossRef] [PubMed]
- Abetz, L.; Arbuckle, R.; Allen, R.P.; Garcia-Borreguero, D.; Hening, W.; Walters, A.S.; Mavraki, E.; Kirsch, J.M. The reliability, validity and responsiveness of the International Restless Legs Syndrome Study Group rating scale and subscales in a clinical-trial setting. Sleep Med. 2006, 7, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Wilt, T.J.; MacDonald, R.; Ouellette, J.; Khawaja, I.S.; Rutks, I.; Butler, M.; Fink, H.A. Pharmacologic Therapy for Primary Restless Legs Syndrome: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2013, 173, 496–505. [Google Scholar] [CrossRef] [Green Version]
- Harrison, E.G.; Keating, J.L.; Morgan, P.E. Non-pharmacological interventions for restless legs syndrome: A systematic review of randomised controlled trials. Disabil. Rehabil. 2019, 41, 2006–2014. [Google Scholar] [CrossRef] [PubMed]
- Silber, M.H.; Becker, P.M.; Earley, C.; Garcia-Borreguero, D.; Ondo, W.G. Willis-Ekbom Disease Foundation Revised Consensus Statement on the Management of Restless Legs Syndrome. Mayo Clin. Proc. 2013, 88, 977–986. [Google Scholar] [CrossRef] [Green Version]
- Mitterling, T.; Heidbreder, A.; Stefani, A.; Fritz, J.; Ulmer, H.; Poewe, W.; Högl, B. Natural course of restless legs syndrome/Willis-Ekbom disease: Long-term observation of a large clinical cohort. Sleep Med. 2015, 16, 1252–1258. [Google Scholar] [CrossRef]
- Lanza, G.; Bachmann, C.G.; Ghorayeb, I.; Wang, Y.; Ferri, R.; Paulus, W. Central and peripheral nervous system excitability in restless legs syndrome. Sleep Med. 2017, 31, 49–60. [Google Scholar] [CrossRef]
- Stiasny-Kolster, K.; Pfau, D.B.; Oertel, W.H.; Treede, R.D.; Magerl, W. Hyperalgesia and functional sensory loss in restless legs syndrome. Pain 2013, 154, 1457–1463. [Google Scholar] [CrossRef]
- Stiasny-Kolster, K.; Magerl, W.; Oertel, W.H.; Möller, J.C.; Treede, R.D. Static mechanical hyperalgesia without dynamic tactile allodynia in patients with restless legs syndrome. Brain 2004, 127, 773–782. [Google Scholar] [CrossRef]
- Kerr, S.; McKinon, W.; Dafkin, C.; Bentley, A. Characterization of painful Restless Legs Syndrome sensations in an English-speaking South African population. Scand. J. Pain 2019, 19, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Argoff, C.E. A focused review on the use of botulinum toxins for neuropathic pain. Clin. J. Pain 2002, 18, S177–S181. [Google Scholar] [CrossRef]
- Mittal, S.O.; Safarpour, D.; Jabbari, B. Botulinum Toxin Treatment of Neuropathic Pain. Semin. Neurol. 2016, 36, 73–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Chung, M.E. Botulinum Toxin for Central Neuropathic Pain. Toxins 2018, 10, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazerani, P.; Staahl, C.; Drewes, A.M.; Arendt-Nielsen, L. The effects of Botulinum Toxin type A on capsaicin-evoked pain, flare, and secondary hyperalgesia in an experimental human model of trigeminal sensitization. Pain 2006, 122, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Rotenberg, J.S.; Canard, K.; Difazio, M. Successful treatment of recalcitrant restless legs syndrome with botulinum toxin type-A. J. Clin. Sleep Med. 2006, 2, 275–278. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, P.; Sia, C.; Vaish, N.; Roy-Faderman, I. Pilot trial of onabotulinumtoxina (Botox) in moderate to severe restless legs syndrome. Int. J. Neurosci. 2011, 121, 622–625. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.O.; Machado, D.; Richardson, D.; Dubey, D.; Jabbari, B. Botulinum Toxin in Restless Legs Syndrome-A Randomized Double-Blind Placebo-Controlled Crossover Study. Toxins 2018, 10, 401. [Google Scholar] [CrossRef] [Green Version]
- Richardson, D.; Bajwa, R.; Eisa, M.; Miller, D.; Mohsenin, V.; Jabbari, B. Botulinum toxin a treatment can improve symptoms of Restlesslegs syndrome. Mov. Disord. 2007, 22, S269. [Google Scholar] [CrossRef]
- Ghorayeb, I.; Burbaud, P. Failure of botulinum toxin A to relieve restless legs syndrome. Sleep Med. 2009, 10, 394–395. [Google Scholar] [CrossRef] [PubMed]
- Ghorayeb, I.; Bénard, A.; Vivot, A.; Tison, F.; Burbaud, P. A phase II, open-label, non-comparative study of Botulinum toxin in Restless Legs Syndrome. Sleep Med. 2012, 13, 1313–1316. [Google Scholar] [CrossRef]
- Nahab, F.B.; Peckham, E.L.; Hallett, M. Double-blind, placebo-controlled, pilot trial of botulinum toxin A in restless legs syndrome. Neurology 2008, 71, 950–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Durieux, N.; Pasleau, F.; Howick, J. OCEBM Levels of Evidence. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 10 September 2021).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Catalá-López, F.; Tobías, A. Meta-analysis of randomized trials, heterogeneity and prediction intervals. Med. Clin. 2014, 142, 270–274. [Google Scholar] [CrossRef]
- van Enst, W.A.; Ochodo, E.; Scholten, R.J.P.M.; Hooft, L.; Leeflang, M.M. Investigation of publication bias in meta-analyses of diagnostic test accuracy: A meta-epidemiological study. BMC Med. Res. Methodol. 2014, 14, 70. [Google Scholar] [CrossRef] [Green Version]
- Silva, M.A.; Duarte, G.S.; Camara, R.; Rodrigues, F.B.; Fernandes, R.M.; Abreu, D.; Mestre, T.; Costa, J.; Trenkwalder, C.; Ferreira, J.J. Placebo and nocebo responses in restless legs syndrome. A systematic review and meta-analysis. Neurology 2017, 88, 2216–2224. [Google Scholar] [CrossRef]
- Scaglione, F. Conversion Ratio between Botox®, Dysport®, and Xeomin® in Clinical Practice. Toxins 2016, 8, 65. [Google Scholar] [CrossRef] [Green Version]
- Tsang, R.; Colley, L.; Lynd, L.D. Inadequate statistical power to detect clinically significant differences in adverse event rates in randomized controlled trials. J. Clin. Epidemiol. 2009, 62, 609–616. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Diagnosis Criteria | Age at the Time of BTI (Years) | Mean of Disease Duration (Years) | Enrolled Sample Number (Male/Female) | Post-BTI Follow-Up (Weeks) | Other Treatments Besides BTI |
|---|---|---|---|---|---|---|---|
| Nahab et al., 2008 [23] | Randomized controlled crossover study | IRLSSG Consensus Criteria | 57.7 (8.8) | 33.5 (14.4) | 6 (3/3) | 12 | NR |
| Agarwal et al., 2011 [18] | Non-comparative study | NR | 62.75 (9.13) | NR | 8 (NR) | 12 | NR |
| Ghorayeb et al., 2012 [22] | Non-comparative study | IRLSSG Consensus Criteria | 57.6 (14.3) | 11 (6–25) a | 27 (15/12) | 24 | NR |
| Mittal et al., 2018 [19] | Randomized controlled crossover study | IRLSSG Consensus Criteria | BoNT: 64 (13.49) Control: 60.5 (14.75) | NR | BoNT: 14 (8/6) Control: 10 (5/5) | 8 | NR |
| Study | Interval of Continuous Intervention | Commercial Forms | Injection Dose (U) | Dilution Method | Injection Site | Tools for Injection | Outcome Measurement |
|---|---|---|---|---|---|---|---|
| Nahab et al., 2008 [23] | 12 weeks (crossover) | onabotulinumtoxinA | 90 U per leg | 50 U/mL | Intramuscular | EMG | IRLS score, CGI, AE score a, adverse events |
| Agarwal et al., 2011 [18] | NR | onabotulinumtoxinA | 50 U per leg | 100 U/mL | Intramuscular | NR | IRLS score, CGI-S, PGI-S, VAS, ESS; CGI-C, PGI-C; adverse events |
| Ghorayeb et al., 2012 [22] | NR | abobotulinumtoxinA | 500 U–1000 U per patient | 250 U/ml | Intradermal | NR | IRLS score, CGI-I; number of responders and duration; adverse events |
| Mittal et al., 2018 [19] | 12 weeks (crossover) | incobotulinumtoxinA | 100 U per leg | 100 U/ml | Intramuscular | EMG | IRLS score, VAS, QoL, ESS, MOS, PGI-C; adverse events |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, Y.-C.; Guo, Y.-H.; Liao, C.-L.; Lin, Y.-C. Effectiveness and Safety of Botulinum Toxin Type A in Treatment of Restless Legs Syndrome: A Systematic Review and Meta-Analysis. Healthcare 2021, 9, 1538. https://doi.org/10.3390/healthcare9111538
Su Y-C, Guo Y-H, Liao C-L, Lin Y-C. Effectiveness and Safety of Botulinum Toxin Type A in Treatment of Restless Legs Syndrome: A Systematic Review and Meta-Analysis. Healthcare. 2021; 9(11):1538. https://doi.org/10.3390/healthcare9111538
Chicago/Turabian StyleSu, Yu-Chi, Yao-Hong Guo, Chung-Lun Liao, and Yu-Ching Lin. 2021. "Effectiveness and Safety of Botulinum Toxin Type A in Treatment of Restless Legs Syndrome: A Systematic Review and Meta-Analysis" Healthcare 9, no. 11: 1538. https://doi.org/10.3390/healthcare9111538
APA StyleSu, Y.-C., Guo, Y.-H., Liao, C.-L., & Lin, Y.-C. (2021). Effectiveness and Safety of Botulinum Toxin Type A in Treatment of Restless Legs Syndrome: A Systematic Review and Meta-Analysis. Healthcare, 9(11), 1538. https://doi.org/10.3390/healthcare9111538