
Spatial Patterns and Multilevel Analysis of Factors Associated with Antenatal Care Visits in Nigeria: Insight from the 2018 Nigeria Demographic Health Survey

 ,
,  , ,
, ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Methods and Materials
2.1. Data Source
2.2. Sample Size Determination and Inclusion Criteria
2.3. Outcome Variable
2.4. Independent Variables
2.5. Individual-Level Factors
2.6. Household-Level Factors
2.7. Statistical Analyses
2.7.1. Multi-Level Analysis
2.7.2. Spatial Analysis
Spatial Autocorrelation
Hot Spot Analysis (Getis-OrdGi* Statistic)
Spatial Interpolation or Prediction
Spatial Scan Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of Respondents
3.2. Spatial Autocorrelation
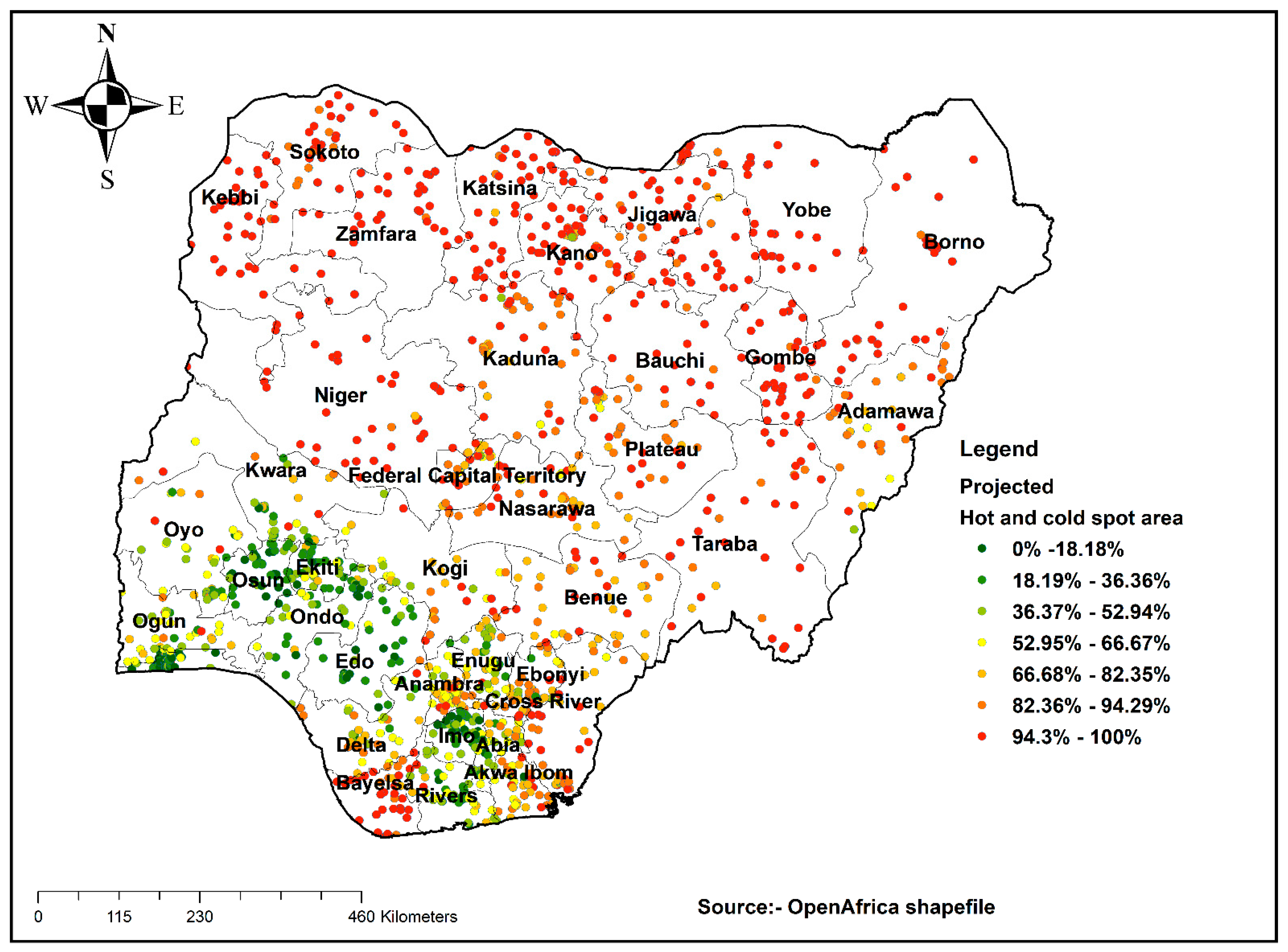
3.3. Hot Spot Analysis
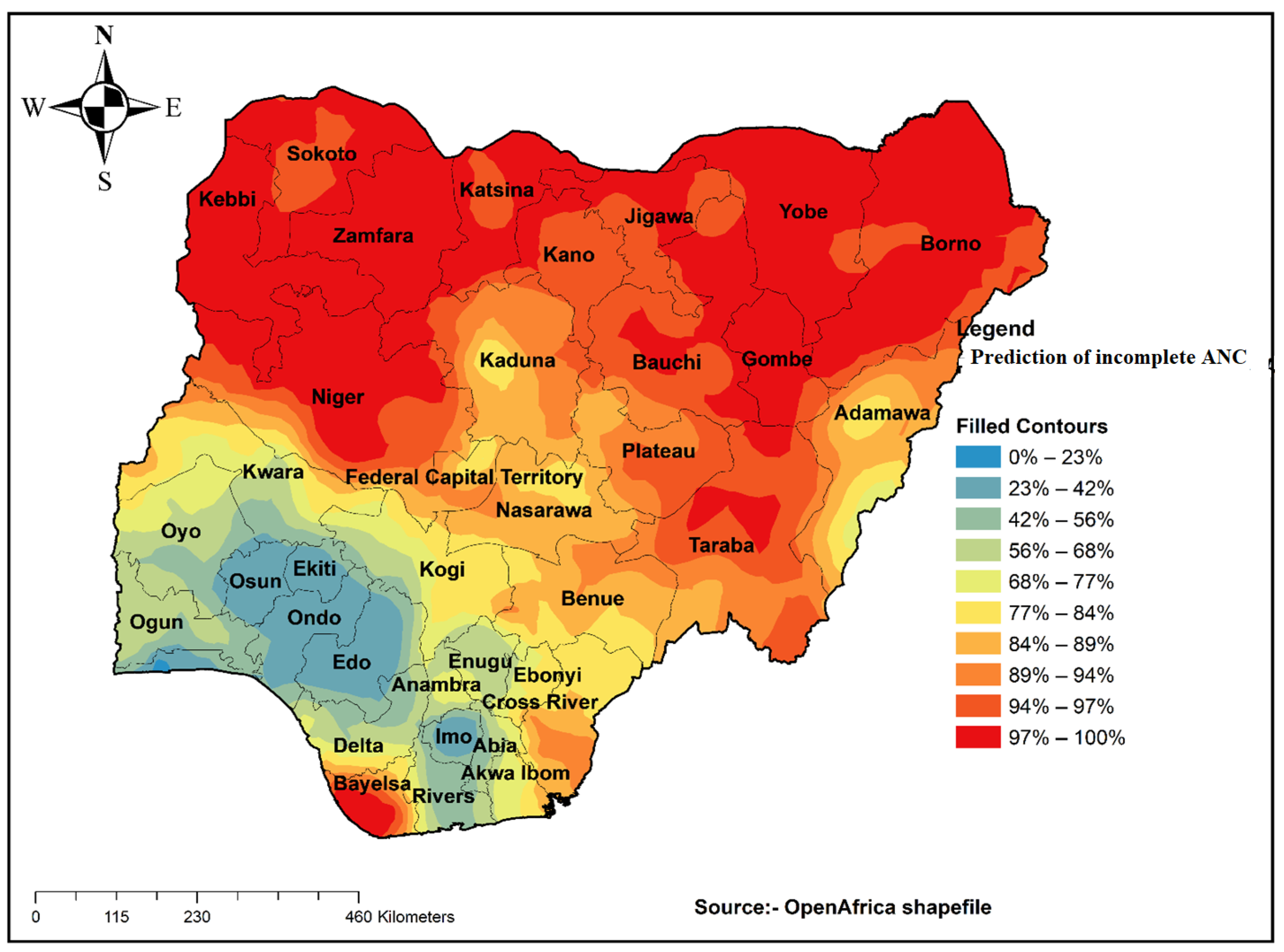
3.4. Prediction of an Incomplete ANC Visit
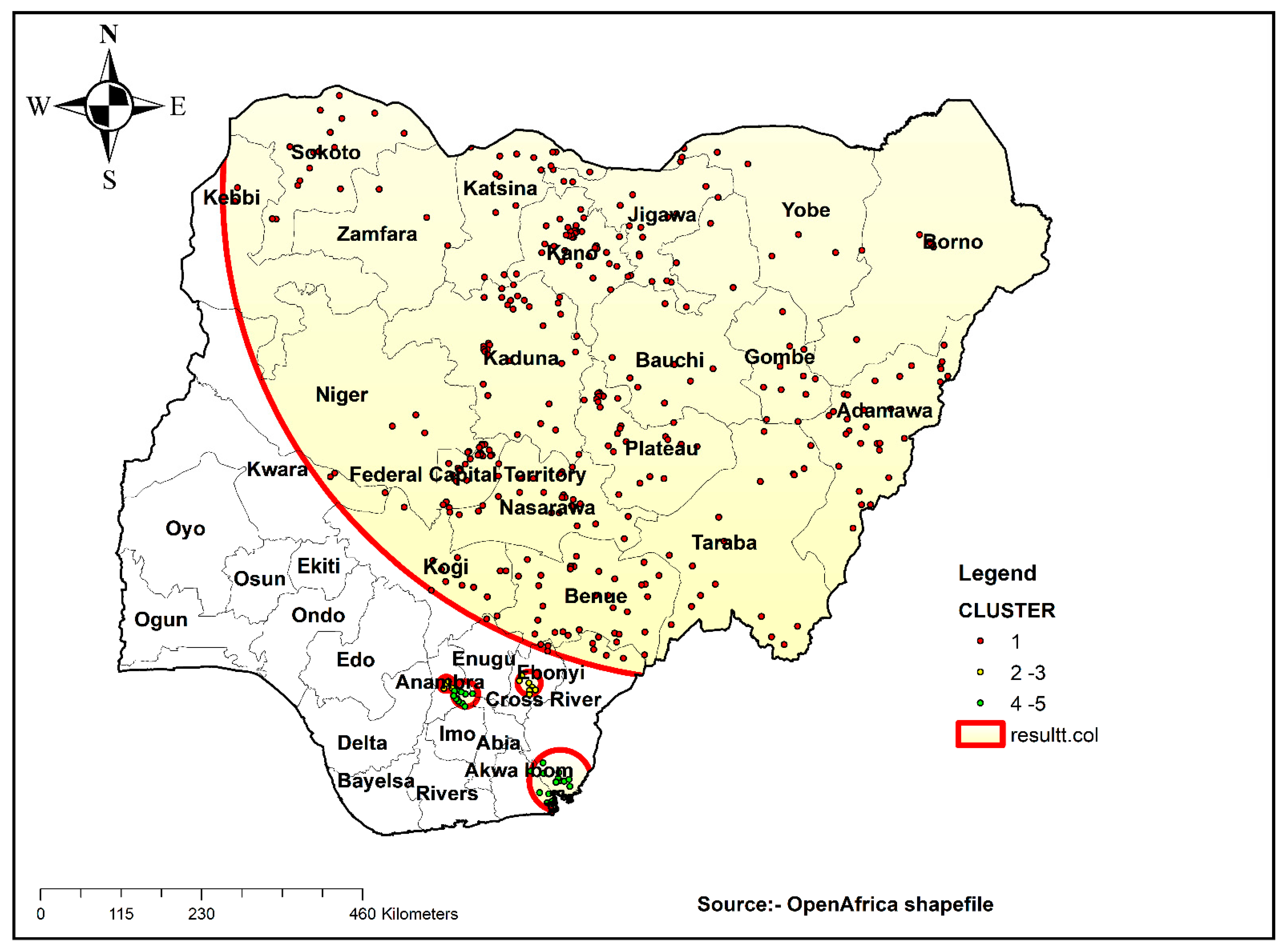
3.5. Spatial SaTScan Analysis of Stillbirth Bernoulli-Based Model
3.6. Multi-Level Fixed Effects (Measures of Associations) Results
3.7. Random Effects (Measures of Variations) Results
4. Discussion
4.1. Strengths and Limitations
4.2. Policy and Public Health Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Approval
Abbreviations
References
- World Health Organization. WHO Guideline Development Group Meeting on WHO Antenatal Care Guidelines: Update on Early Ultrasound Scan Recommendation. 2021. Available online: https://www.who.int/news/item/07-06-2021-who-antenatal-care-guidelines-update-on-early-ultrasound-scan-recommendation (accessed on 25 June 2021).
- Lincetto, O.; Mothebesoane-Anoh, S.; Gomez, P.; Munjanja, S. Antenatal Care, Opportunities for Africa’s Newborns: Practical Data, Policy and Programmatic Support for Newborn Care in Africa; WHO: Geneva, Switzerland, 2006; pp. 55–62. [Google Scholar]
- World Health Organization. Maternal Mortality. Fact Sheets. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (accessed on 25 June 2021).
- Fagbamigbe, A.F.; Idemudia, E.S. Barriers to antenatal care use in Nigeria: Evidences from non-users and implications for maternal health programming. BMC Pregnancy Childbirth 2015, 15, 95. [Google Scholar] [CrossRef] [PubMed]
- Tessema, Z.T.; Teshale, A.B.; Tesema, G.A.; Tamirat, K.S. Determinants of completing recommended antenatal care utilization in sub-Saharan from 2006 to 2018: Evidence from 36 countries using Demographic and Health Surveys. BMC Pregnancy Childbirth 2021, 21, 192. [Google Scholar] [CrossRef]
- World Health Organization. Maternal Health in Nigeria: Generating Information for Action. 2019. Available online: https://www.who.int/reproductivehealth/maternal-health-nigeria/en (accessed on 25 June 2021).
- Ajayi, I.; Osakinle, D. Socio Demographic Factors Determining the Adequacy of Antenatal Care among Pregnant Women Visiting Ekiti State Primary Health Centers. Online J. Health Allied Sci. 2013, 12, 9152. [Google Scholar]
- World Health Organization. World Health Statistics 2016: Monitoring Health for the SDGs Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Fagbamigbe, A.F.; Idemudia, E.S. Wealth and antenatal care utilization in Nigeria: Policy implications. Health Care Women Int. 2017, 38, 17–37. [Google Scholar] [CrossRef]
- Nwosu, C.O.; Ataguba, J.E. Socioeconomic inequalities in maternal health service utilisation: A case of antenatal care in Nigeria using a decomposition approach. BMC Public Health 2019, 19, 1493. [Google Scholar] [CrossRef]
- Tegegne, T.K.; Chojenta, C.; Getachew, T.; Smith, R.; Loxton, D. Antenatal care use in Ethiopia: A spatial and multilevel analysis. BMC Pregnancy Childbirth 2019, 19, 399. [Google Scholar] [CrossRef] [PubMed]
- Tessema, Z.T.; Akalu, T.Y. Spatial pattern and associated factors of ANC visits in Ethiopia: Spatial and multilevel modeling of Ethiopian demographic health survey data. Adv. Prev. Med. 2020, 2020, 4676591. [Google Scholar] [CrossRef]
- Chandhiok, N.; Dhillon, B.S.; Kambo, I.; Saxena, N.C. Determinants of antenatal care utilization in rural areas of India: A cross-sectional study from 28 districts (An ICMR task force study). J. Obstet. Gynecol. India 2006, 56, 47–52. [Google Scholar]
- Omo-Aghoja, L.; Aisien, O.; Akuse, J.; Bergstrom, S.; Okonofua, F.E. Maternal mortality and emergency obstetric care in Benin City, South-south Nigeria. J. Clin. Med. Res. 2010, 2, 55–60. [Google Scholar]
- Dairo, M.; Owoyokun, K. Factors affecting the utilization of antenatal care services in Ibadan, Nigeria. Benin J. Postgrad. Med. 2010, 12, 1. [Google Scholar] [CrossRef]
- Indicator, W.B. Physicians (Per 1000 People)—Nigeria. Available online: https://data.worldbank.org/indicator/SH.MED.PHYS.ZS?locations=NG-GN (accessed on 16 September 2021).
- Awogbami, P.A.; Opele, J.K.; Awe, T.P. Health Records Management Practices and Patients’ Satisfaction in Selected University Medical Centres in South-West, Nigeria. Glob. J. Soc. Sci. Stud. 2020, 6, 106–114. [Google Scholar] [CrossRef]
- Corsi, D.J.; Neuman, M.; Finlay, J.E.; Subramanian, S. Demographic and health surveys: A profile. Int. J. Epidemiol. 2012, 41, 1602–1613. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Ahinkorah, B.O.; Ameyaw, E.K.; Seidu, A.-A.; Odusina, E.K.; Keetile, M.; Yaya, S. Examining barriers to healthcare access and utilization of antenatal care services: Evidence from demographic health surveys in sub-Saharan Africa. BMC Health Serv. Res. 2021, 21, 125. [Google Scholar] [CrossRef]
- Kareem, Y.O.; Morhason-Bello, I.O.; OlaOlorun, F.M.; Yaya, S. Temporal relationship between Women’s empowerment and utilization of antenatal care services: Lessons from four National Surveys in sub-Saharan Africa. BMC Pregnancy Childbirth 2021, 21, 198. [Google Scholar] [CrossRef]
- Ekholuenetale, M.; Benebo, F.O.; Idebolo, A.F. Individual-, household-, and community-level factors associated with eight or more antenatal care contacts in Nigeria: Evidence from Demographic and Health Survey. PLoS ONE 2020, 15, e0239855. [Google Scholar] [CrossRef]
- Goldstein, H. Multilevel Statistical Models; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Adewuyi, E.O.; Auta, A.; Khanal, V.; Bamidele, O.D.; Akuoko, C.P.; Adefemi, K.; Tapshak, S.J.; Zhao, Y. Prevalence and factors associated with underutilization of antenatal care services in Nigeria: A comparative study of rural and urban residences based on the 2013 Nigeria demographic and health survey. PLoS ONE 2018, 13, e0197324. [Google Scholar] [CrossRef]
- Abegunde, D.; Kabo, I.A.; Sambisa, W.; Akomolafe, T.; Orobaton, N.; Abdulkarim, M.; Sadauki, H. Availability, utilization, and quality of emergency obstetric care services in Bauchi State, Nigeria. Int. J. Gynecol. Obstet. 2015, 128, 251–255. [Google Scholar] [CrossRef]
- Sinai, I.; Anyanti, J.; Khan, M.; Daroda, R.; Oguntunde, O. Demand for women’s health services in northern Nigeria: A review of the literature. Afr. J. Reprod. Health 2017, 21, 96–108. [Google Scholar] [CrossRef]
- Onyejose, K.N.; Ndep, A.O.; Offiong, D.A.; Omang, J.A.; Otu, F.T. Sociocultural factors influencing maternal health outcomes in Nigeria. Sci. Res. J. 2019, VII, 86–96. [Google Scholar]
- Okedo-Alex, I.N.; Akamike, I.C.; Ezeanosike, O.B.; Uneke, C.J. Determinants of antenatal care utilisation in sub-Saharan Africa: A systematic review. BMJ Open 2019, 9, e031890. [Google Scholar] [CrossRef]
- Zhao, Q.; Huang, Z.J.; Yang, S.; Pan, J.; Smith, B.; Xu, B. The utilization of antenatal care among rural-to-urban migrant women in Shanghai: A hospital-based cross-sectional study. BMC Public Health 2012, 12, 1012. [Google Scholar] [CrossRef]
- Tran, T.K.; Gottvall, K.; Nguyen, H.D.; Ascher, H.; Petzold, M. Factors associated with antenatal care adequacy in rural and urban contexts-results from two health and demographic surveillance sites in Vietnam. BMC Health Serv. Res. 2012, 12, 40. [Google Scholar] [CrossRef] [PubMed]
- Paredes, I.; Hidalgo, L.; Chedraui, P.; Palma, J.; Eugenio, J. Factors associated with inadequate prenatal care in Ecuadorian women. Int. J. Gynecol. Obstet. 2005, 88, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Simkhada, B.; Teijlingen, E.R.V.; Porter, M.; Simkhada, P. Factors affecting the utilization of antenatal care in developing countries: Systematic review of the literature. J. Adv. Nurs. 2008, 61, 244–260. [Google Scholar] [CrossRef] [PubMed]
- Fagbamigbe, A.F.; Abel, C.; Mashabe, B.; Adebowale, A.S. Survival analysis and prognostic factors of the timing of first antenatal care visit in Nigeria. Adv. Integr. Med. 2019, 6, 110–119. [Google Scholar] [CrossRef]
- Onyeajam, D.J.; Xirasagar, S.; Khan, M.M.; Hardin, J.W.; Odutolu, O. Antenatal care satisfaction in a developing country: A cross-sectional study from Nigeria. BMC Public Health 2018, 18, 368. [Google Scholar] [CrossRef]
- Basha, G.W. Factors affecting the utilization of a minimum of four antenatal care services in Ethiopia. Obstet. Gynecol. Int. 2019, 2019, 5036783. [Google Scholar] [CrossRef]
- Odesanya, A.; Hassan, S.; Olaluwoye, D. Mass media and maternal healthcare: A critical discourse. New Media Mass Commun. 2015, 34, 63–71. [Google Scholar]
- Akanbiemu, F.A.; Manuwa-Olumide, A.; Fagbamigbe, A.F.; Adebowale, A.S. Effect of perception and free maternal health services on antenatal care facilities utilization in selected rural and semi-urban communities of Ondo State, Nigeria. J. Adv. Med. Med Res. 2013, 3, 681–697. [Google Scholar] [CrossRef][Green Version]
- Islam, M.M.; Masud, M.S. Determinants of frequency and contents of antenatal care visits in Bangladesh: Assessing the extent of compliance with the WHO recommendations. PLoS ONE 2018, 13, e0204752. [Google Scholar] [CrossRef]
- Babalola, B.I. Determinants of urban-rural differentials of antenatal care utilization in Nigeria. Afr. Popul. Stud. 2014, 28, 1263–1273. [Google Scholar] [CrossRef][Green Version]
- Chima, V. Women autonomy and maternal healthcare services utilization among young ever-married women in Nigeria. Int. J. Nurs. Midwifery 2018, 10, 62–73. [Google Scholar]
- Banke-Thomas, O.E.; Banke-Thomas, A.O.; Ameh, C.A. Factors influencing utilisation of maternal health services by adolescent mothers in Low-and middle-income countries: A systematic review. BMC Pregnancy Childbirth 2017, 17, 65. [Google Scholar] [CrossRef]
- Mustafa, M.H.; Mukhtar, A.M. Factors associated with antenatal and delivery care in Sudan: Analysis of the 2010 Sudan household survey. BMC Health Serv. Res. 2015, 15, 452. [Google Scholar] [CrossRef]
- Mumtaz, S.; Bahk, J.; Khang, Y.-H. Current status and determinants of maternal healthcare utilization in Afghanistan: Analysis from Afghanistan demographic and health survey 2015. PLoS ONE 2019, 14, e0217827. [Google Scholar] [CrossRef] [PubMed]
- Dimbuene, Z.T.; Amo-Adjei, J.; Amugsi, D.; Mumah, J.; Izugbara, C.O.; Beguy, D. Women’s education and utilization of maternal health services in Africa: A multi-country and socioeconomic status analysis. J. Biosoc. Sci. 2018, 50, 725–748. [Google Scholar] [CrossRef] [PubMed]
- Weitzman, A. The effects of women’s education on maternal health: Evidence from Peru. Soc. Sci. Med. 2017, 180, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Tiruneh, F.N.; Chuang, K.-Y.; Chuang, Y.-C. Women’s autonomy and maternal healthcare service utilization in Ethiopia. BMC Health Serv. Res. 2017, 17, 718. [Google Scholar] [CrossRef] [PubMed]
- Tekelab, T.; Chojenta, C.; Smith, R.; Loxton, D. Factors affecting utilization of antenatal care in Ethiopia: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0214848. [Google Scholar] [CrossRef] [PubMed]
- Goli, S.; Nawal, D.; Rammohan, A.; Sekher, T.; Singh, D. Decomposing the socioeconomic inequality in utilization of maternal health care services in selected countries of South Asia and sub-Saharan Africa. J. Biosoc. Sci. 2018, 50, 749–769. [Google Scholar] [CrossRef]
- Mekonnen, T.; Dune, T.; Perz, J. Maternal health service utilisation of adolescent women in sub-Saharan Africa: A systematic scoping review. BMC Pregnancy Childbirth 2019, 19, 366. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable (20,003) | Weighted Frequency | Weighted Percentage | Number of ANC Visits | p-Value (χ2) | |
|---|---|---|---|---|---|
| Individual Level Factors | Complete | Incomplete | |||
| Maternal current age | p < 0.001 | ||||
| 15–24 | 4793 | 23.96 | 12.59 | 87.41 | |
| 25–34 | 9665 | 48.32 | 22.67 | 77.33 | |
| 35 and above | 5545 | 27.72 | 22.53 | 77.47 | |
| Maternal education | p < 0.001 | ||||
| No education | 9245 | 46.22 | 4.19 | 95.81 | |
| Primary education | 2913 | 14.56 | 19.17 | 80.83 | |
| Secondary and above | 7846 | 39.22 | 39.48 | 60.52 | |
| Partner’s level of education | p < 0.001 | ||||
| No education | 7322 | 36.60 | 4.35 | 95.65 | |
| Primary education | 2795 | 13.97 | 17.77 | 82.23 | |
| Secondary and above | 9886 | 49.42 | 32.66 | 67.34 | |
| Marital status | p < 0.001 | ||||
| Currently married | 19,387 | 96.92 | 19.51 | 80.49 | |
| Cohabitating | 617 | 3.08 | 42.25 | 57.75 | |
| Working status | p < 0.001 | ||||
| Not working | 6393 | 31.96 | 10.68 | 89.32 | |
| Working | 13,610 | 68.04 | 24.69 | 75.31 | |
| Ethnicity | p < 0.001 | ||||
| Hausa | 9125 | 45.62 | 4.40 | 95.60 | |
| Yoruba | 2428 | 12.14 | 61.55 | 38.45 | |
| Igbo | 2424 | 12.12 | 44.77 | 55.23 | |
| Others | 6027 | 30.13 | 17.63 | 82.37 | |
| Parity | p < 0.001 | ||||
| 1 | 3123 | 15.61 | 26.36 | 73.64 | |
| 2 | 3618 | 18.09 | 27.47 | 72.53 | |
| 3 | 3082 | 15.41 | 25.39 | 74.61 | |
| 4 and above | 10,180 | 50.89 | 14.18 | 85.82 | |
| Distance to health facility | p < 0.001 | ||||
| Big problem | 5685 | 28.42 | 15.67 | 84.33 | |
| Not a big problem | 14,319 | 71.58 | 22.02 | 77.98 | |
| Religion | |||||
| Christianity | 7255 | 36.27 | 37.93 | 62.07 | |
| Islam | 12,647 | 63.22 | 10.16 | 89.84 | |
| Traditionalist and others | 102 | 0.51 | 5.83 | 94.17 | |
| Exposure to media | p < 0.001 | ||||
| No | 7677 | 38.38 | 5.60 | 94.40 | |
| Yes | 12,326 | 61.62 | 29.31 | 70.69 | |
| Household-level factors | |||||
| Place of residence | p < 0.001 | ||||
| Urban | 7737 | 38.68 | 35.97 | 64.03 | |
| Rural | 12,266 | 61.32 | 10.27 | 89.73 | |
| Wealth index | p < 0.001 | ||||
| Poorest | 4464 | 22.32 | 3.95 | 96.05 | |
| Poorer | 4451 | 22.25 | 7.34 | 92.66 | |
| Middle | 4003 | 20.01 | 16.85 | 83.15 | |
| Richer | 3671 | 18.35 | 31.08 | 68.92 | |
| Richest | 3414 | 17.07 | 50.54 | 49.46 | |
| Region | p < 0.001 | ||||
| North Central | 2806 | 14.03 | 14.47 | 85.53 | |
| North East | 3581 | 17.90 | 3.78 | 96.22 | |
| North West | 7269 | 36.34 | 4.15 | 95.84 | |
| South East | 1874 | 9.37 | 38.97 | 61.03 | |
| South-South | 1675 | 8.38 | 41.35 | 58.65 | |
| South West | 2798 | 13.99 | 63.49 | 36.51 | |
| Sex of household head | |||||
| Male | 18,595 | 92.96 | 19.40 | 80.60 | |
| Female | 1409 | 7.04 | 31.00 | 69.00 | |
| Community literacy level | p < 0.001 | ||||
| Low | 6705 | 33.52 | 4.51 | 95.49 | |
| Medium | 6512 | 32.55 | 13.97 | 86.03 | |
| High | 6786 | 33.93 | 41.73 | 58.27 | |
| Community socioeconomic status | p < 0.001 | ||||
| Low | 11,957 | 59.77 | 8.55 | 91.45 | |
| Medium | 861 | 4.30 | 17.10 | 82.90 | |
| High | 7186 | 35.92 | 40.00 | 60.00 | |
| Cluster | Enumeration Area (Cluster) Identified | Coordinate/Radius | Population | Case | RR | LLR | p-Value |
|---|---|---|---|---|---|---|---|
| 1 | 336 | (12.458115 N, 10.398881 E)/690.22 km | 6670 | 5952 | 1.79 | 1307.55 | <0.001 |
| 2 | 8 | (6.224563 N, 7.971626 E)/16.54 km | 109 | 97 | 1.28 | 11.90 | 0.0062 |
| Variable Individual-Level Variables | Model 0 | Model I | Model II | Model III |
|---|---|---|---|---|
| aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | ||
| Maternal current age | ||||
| 15–24 | 1 | 1 | ||
| 25–34 | 0.72 *** [0.62–0.83] | 0.82 ** [0.71–0.95] | ||
| 35 and above | 0.58 *** [0.48–0.69] | 0.69 *** [0.58–0.83] | ||
| Maternal education | ||||
| No education | 1 | 1 | ||
| Primary education | 0.58 *** [0.48–0.70] | 0.73 ** [0.60–0.89] | ||
| Secondary and above | 0.44 *** [0.36–0.53] | 0.62 *** [0.51–0.76] | ||
| Partner’s level of education | ||||
| No education | 1 | 1 | ||
| Primary education | 0.91 [0.74–1.12] | 1.04 [0.84–1.29] | ||
| Secondary and above | 0.63 *** [0.52–0.76] | 0.76 ** [0.62–0.93] | ||
| Marital status | ||||
| Currently married | 1 | 1 | ||
| Cohabitating | 0.84 [0.67–1.05] | 0.99 [0.79–1.23] | ||
| Working status | ||||
| Not working | 1 | 1 | ||
| Working | 0.75 *** [0.66–0.85] | 0.76 *** [0.67–0.87] | ||
| Ethnicity | ||||
| Hausa | 1 | 1 | ||
| Yoruba | 0.12 *** [0.09–0.15] | 0.59 ** [0.43–0.80] | ||
| Igbo | 0.22 *** [0.17–0.29] | 0.56 ** [0.40–0.78] | ||
| Others | 0.56 *** [0.45–0.69] | 0.97 [0.76–1.24] | ||
| Parity | ||||
| 1 | 1 | 1 | ||
| 2 | 1.14 [0.97–1.33] | 1.13 [0.96–1.32] | ||
| 3 | 1.28 ** [1.08–1.52] | 1.23 * [1.03–1.45] | ||
| 4 and above | 1.65 *** [1.39–1.95] | 1.50 *** [1.27–1.77] | ||
| Distance to health facility | ||||
| Big problem | 1 | 1 | ||
| Not a big problem | 0.99 [0.87–1.12] | 1.03 [0.91–1.18] | ||
| Religion | ||||
| Christianity | 1 | 1 | ||
| Islam | 1.38 *** [1.17–1.62] | 0.98 [0.83–1.16] | ||
| Traditionalist and others | 5.01 *** [2.12–11.81] | 5.79 *** [2.45–13.58] | ||
| Exposure to Media | ||||
| No | 1 | 1 | ||
| Yes | 0.51 *** [0.44–0.59] | 0.65 *** [0.56–0.75] | ||
| Household-level factors | ||||
| Place of residence | ||||
| Urban | 1 | 1 | ||
| Rural | 1.36 ** [1.14–1.64] | 1.32 ** [1.10–1.58] | ||
| Wealth index | ||||
| Poorest | 1 | 1 | ||
| Poorer | 0.70 ** [0.56–0.88] | 0.80 * [0.63–1.01] | ||
| Middle | 0.51 *** [0.40–0.65] | 0.66 ** [0.52–0.84] | ||
| Richer | 0.42 *** [0.33–0.54] | 0.62 *** [0.47–0.80] | ||
| Richest | 0.27 *** [0.20–0.35] | 0.45 *** [0.33–0.59] | ||
| Region | ||||
| North Central | 1 | 1 | ||
| North East | 4.03 *** [2.97–5.46] | 3.00 *** [2.21–4.07] | ||
| North West | 4.17 *** [3.15–5.52] | 3.02 *** [2.19–4.18] | ||
| South East | 0.37 *** [0.29–0.49] | 0.60 ** [0.42–0.84] | ||
| South-South | 0.45 *** [0.35–0.59] | 0.47 *** [0.36–0.61] | ||
| South West | 0.13 *** [0.10–0.16] | 0.19 *** [0.14–0.26] | ||
| Sex of household head | ||||
| Male | 1 | 1 | ||
| Female | 0.95 [0.82–1.11] | 1.00 [0.86–1.17] | ||
| Community literacy level | ||||
| Low | 1 | 1 | ||
| Medium | 0.71 * [0.55–0.93] | 0.92 [0.70–1.19] | ||
| High | 0.46 *** [0.34–0.62] | 0.72 * [0.53–0.98] | ||
| Community socioeconomic status | ||||
| Low | 1 | 1 | ||
| Medium | 1.06 [0.69–1.64] | 1.04 [0.68–1.58] | ||
| High | 1.11 [0.89–1.38] | 1.08 [0.87–1.34] | ||
| Random effects results | ||||
| PSU Variance (95% CI) | 5.33 [4.73–6.02] | 1.32 [1.13–1.54] | 1.17 [1.00–1.37] | 1.05 [0.90–1.24] |
| ICC | 0.62 | 0.29 | 0.26 | 0.24 |
| LR Test | χ2 = 4953.88, p < 0.001 | χ2 = 840.39, p < 0.001 | χ2 = 769.82, p < 0.001 | χ2 = 636.64, p < 0.001 |
| Wald χ2 | Reference | 1420.84 *** | 1601.48 *** | 1818.00 *** |
| Model fitness | ||||
| Log-likelihood | −7161.20 | −6617.80 | −6499.20 | −6379.96 |
| AIC | 14,326.39 | 13,275.60 | 13,032.40 | 12,829.91 |
| BIC | 14,342.18 | 13,433.51 | 13,166.63 | 13,106.26 |
| Number of clusters | 1387 | 1387 | 1387 | 1387 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolarinwa, O.A.; Sakyi, B.; Ahinkorah, B.O.; Ajayi, K.V.; Seidu, A.-A.; Hagan, J.E., Jr.; Tessema, Z.T. Spatial Patterns and Multilevel Analysis of Factors Associated with Antenatal Care Visits in Nigeria: Insight from the 2018 Nigeria Demographic Health Survey. Healthcare 2021, 9, 1389. https://doi.org/10.3390/healthcare9101389
Bolarinwa OA, Sakyi B, Ahinkorah BO, Ajayi KV, Seidu A-A, Hagan JE Jr., Tessema ZT. Spatial Patterns and Multilevel Analysis of Factors Associated with Antenatal Care Visits in Nigeria: Insight from the 2018 Nigeria Demographic Health Survey. Healthcare. 2021; 9(10):1389. https://doi.org/10.3390/healthcare9101389
Chicago/Turabian StyleBolarinwa, Obasanjo Afolabi, Barbara Sakyi, Bright Opoku Ahinkorah, Kobi V. Ajayi, Abdul-Aziz Seidu, John Elvis Hagan, Jr., and Zemenu Tadesse Tessema. 2021. "Spatial Patterns and Multilevel Analysis of Factors Associated with Antenatal Care Visits in Nigeria: Insight from the 2018 Nigeria Demographic Health Survey" Healthcare 9, no. 10: 1389. https://doi.org/10.3390/healthcare9101389
APA StyleBolarinwa, O. A., Sakyi, B., Ahinkorah, B. O., Ajayi, K. V., Seidu, A.-A., Hagan, J. E., Jr., & Tessema, Z. T. (2021). Spatial Patterns and Multilevel Analysis of Factors Associated with Antenatal Care Visits in Nigeria: Insight from the 2018 Nigeria Demographic Health Survey. Healthcare, 9(10), 1389. https://doi.org/10.3390/healthcare9101389