
Current Novel Caries Diagnostic Technologies: Restorative Dentists’ Attitude and Use Preferences


Abstract
1. Introduction
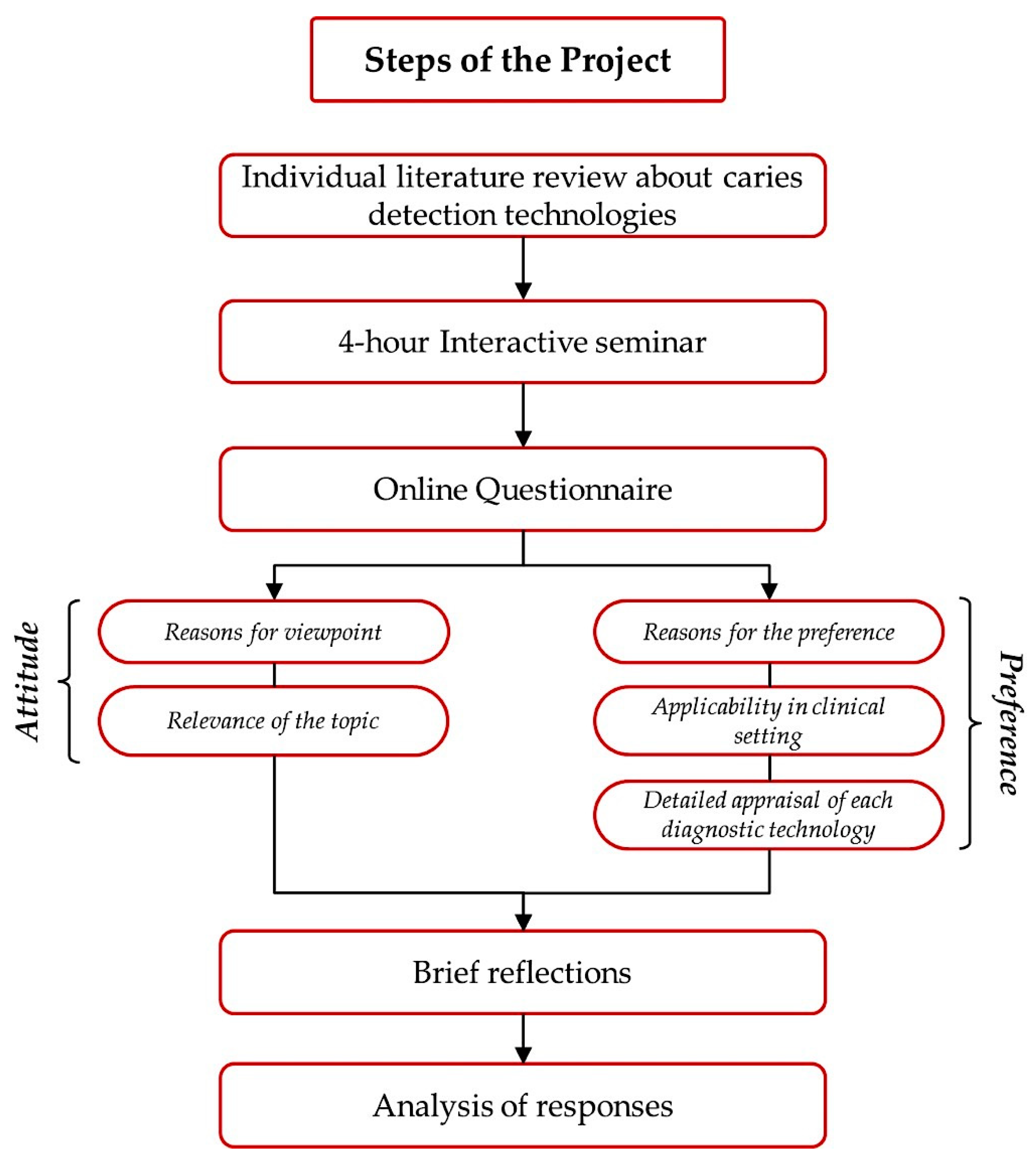
2. Materials and Methods
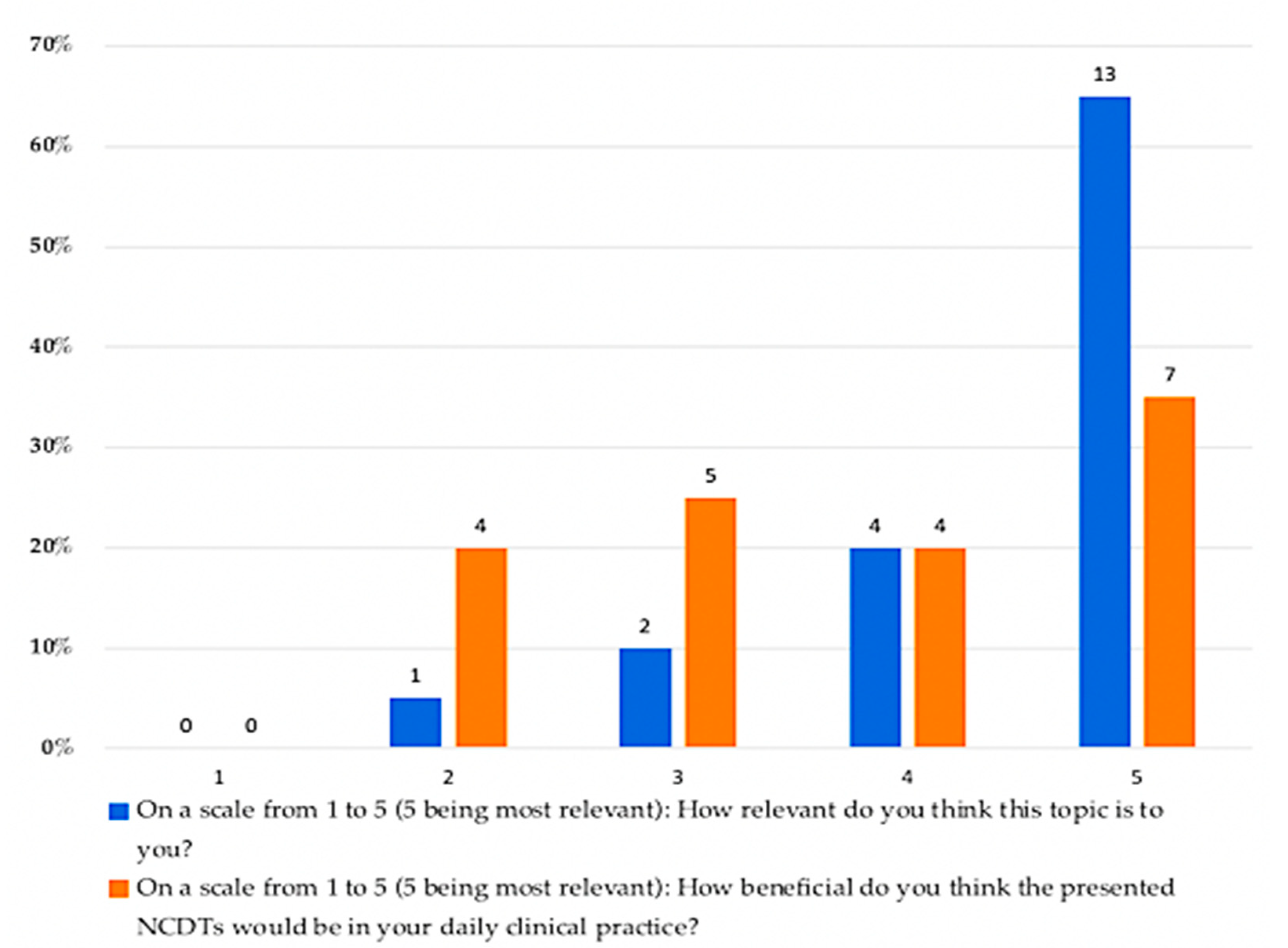
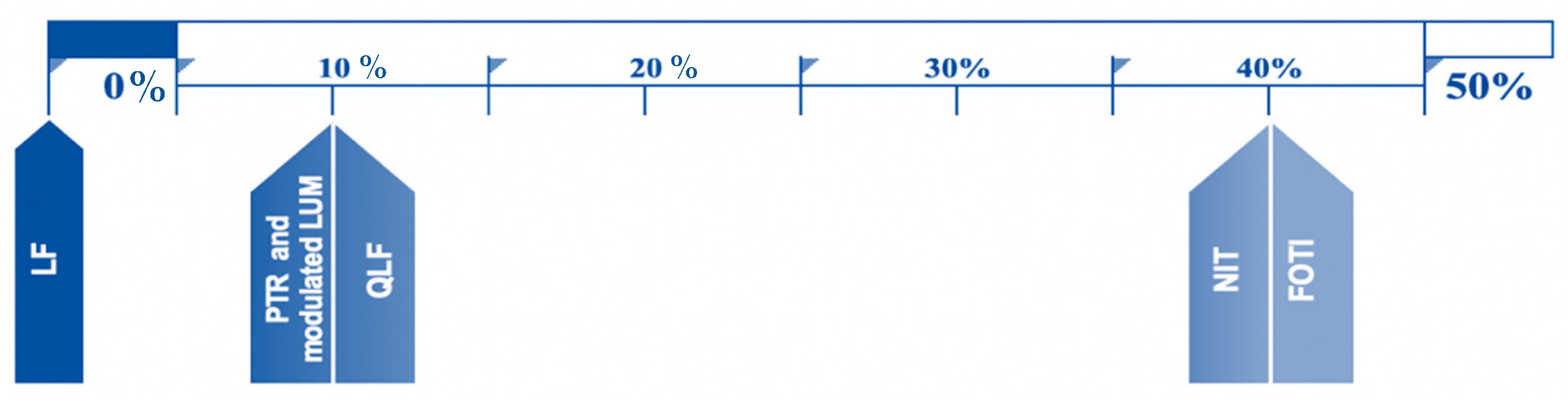
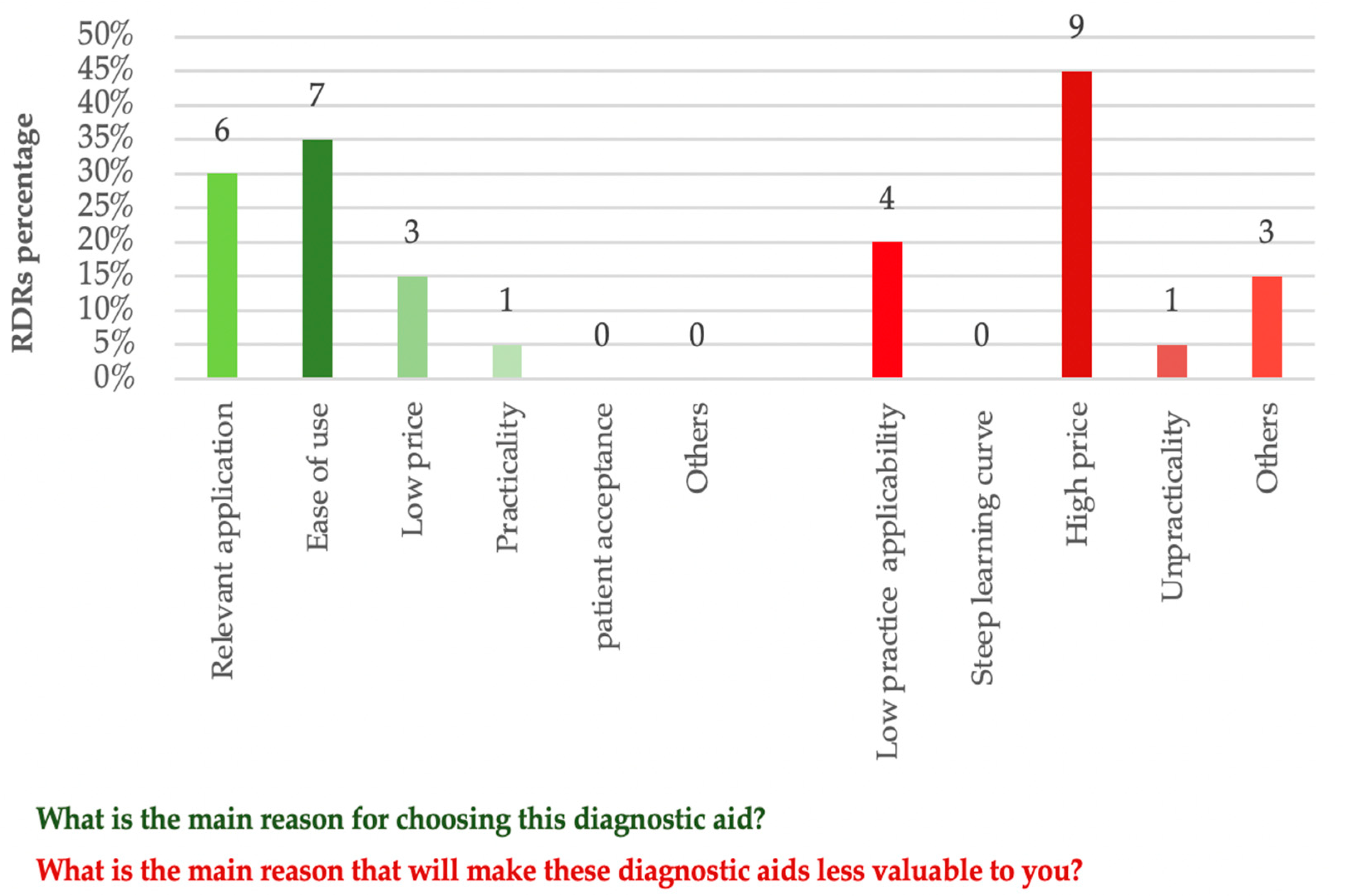
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Featherstone, J.D. Dental caries: A dynamic disease process. Aust. Dent. J. 2008, 53, 286–291. [Google Scholar] [CrossRef]
- Fontana, M.; Gonzalez-Cabezas, C. Evidence-based dentistry caries risk assessment and disease management. Dent. Clin. North. Am. 2019, 63, 119–128. [Google Scholar] [CrossRef]
- World Health Organization. Sugar and Dental Caries. 2017. Contract No.: WHO/NMH/NHD/17.12; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef]
- Featherstone, J.D. The continuum of dental caries—Evidence for a dynamic disease process. J. Dent. Res. 2004, 83, 39–42. [Google Scholar] [CrossRef]
- Featherstone, J.D. The science and practice of caries prevention. J. Am. Dent. Assoc. 2000, 131, 887–899. [Google Scholar] [CrossRef] [PubMed]
- Araujo, G.S.; Naufel, F.S.; Alonso, R.C.; Lima, D.A.; Puppin-Rontani, R.M. Influence of staining solution and bleaching on color stability of resin used for caries infiltration. Oper. Dent. 2015, 40, E250–E256. [Google Scholar] [CrossRef] [PubMed]
- Nassar, H.M.; Neel, E.A.A. Awareness and utilization of bulk-fill composites among dental practitioners in Saudi Arabia. Open Dent. J. 2021, 15, 160–169. [Google Scholar] [CrossRef]
- Aswani, R.; Chandrappa, V.; Uloopi, K.S.; Chandrasekhar, R.; RojaRamya, K.S. Resin infiltration of artificial enamel lesions: Evaluation of penetration depth, surface roughness and color stability. Int. J. Clin. Pediatr. Dent. 2019, 12, 520–523. [Google Scholar] [PubMed]
- Nassar, H.M. Dental caries preventive considerations: Awareness of undergraduate dental students. Dent. J. 2020, 8, 31. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D. Microbiology of dental plaque biofilms and their role in oral health and caries. Dent. Clin. North. Am. 2010, 54, 441–454. [Google Scholar] [CrossRef]
- Marghalani, A.A.; Alsahafi, Y.A.; Alshouibi, E.N. The cost of dental caries in Saudi Arabia. Putting numbers into context. Saudi Med. J. 2014, 35, 93–94. [Google Scholar]
- Banerjee, A.; Frencken, J.E.; Schwendicke, F.; Innes, N.P.T. Contemporary operative caries management: Consensus recommendations on minimally invasive caries removal. Br. Dent. J. 2017, 223, 215–222. [Google Scholar] [CrossRef]
- Slimani, A.; Terrer, E.; Manton, D.J.; Tassery, H. Carious lesion detection technologies: Factual clinical approaches. Br. Dent. J. 2020, 229, 432–442. [Google Scholar] [CrossRef]
- Radwan, W.; AlNasser, A.A.; Aloqab, H.; Al-Saggaf, K.; Almuhtab, N.A.; Alnasyan, B. Knowledge and use of caries detection methods among dental students and dental practitioners in Riyadh, Saudi Arabia. Int. J. Dent. 2020, 2020, 8825890. [Google Scholar] [CrossRef]
- Zandona, A.F.; Zero, D.T. Diagnostic tools for early caries detection. J. Am. Dent. Assoc. 2006, 137, 1675–1684. [Google Scholar] [CrossRef] [PubMed]
- Vural, U.K.; Gokalp, S. Diagnostic methods for dental caries used by private dental practitioners in Ankara. Niger. J. Clin. Pract. 2017, 20, 382–387. [Google Scholar] [CrossRef]
- Pretty, I.A.; Ekstrand, K.R. Detection and monitoring of early caries lesions: A review. Eur. Arch. Paediatr. Dent. 2016, 17, 13–25. [Google Scholar] [CrossRef]
- Pitts, N.B.; Stamm, J.W. International Consensus Workshop on Caries Clinical Trials (ICW-CCT)—Final consensus statements: Agreeing where the evidence leads. J. Dent. Res. 2004, 83, 125–128. [Google Scholar] [CrossRef]
- Neuhaus, K.W.; Rodrigues, J.A.; Hug, I.; Stich, H.; Lussi, A. Performance of laser fluorescence devices, visual and radiographic examination for the detection of occlusal caries in primary molars. Clin. Oral. Investig. 2011, 15, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Longbottom, C.L.; Huysmans, M.C.; Pitts, N.B.; Fontana, M. Glossary of key terms. Monogr. Oral. Sci. 2009, 21, 209–216. [Google Scholar] [PubMed]
- Schwendicke, F.; Göstemeyer, G. Conventional bitewing radiography. Clin. Dent. Rev. 2020, 4, 22. [Google Scholar] [CrossRef]
- Stookey, G. Should a dental explorer be used to probe suspected carious lesions? No—Use of an explorer can lead to misdiagnosis and disrupt remineralization. J. Am. Dent. Assoc. 2005, 136, 1527, 1529, 1531. [Google Scholar] [PubMed]
- Lennon, A.M.; Wiegand, A.; Buchalla, W.; Wahl, B.; Werner, C.; Betke, H.; Hannig, C.; Rödig, T.; Attin, T. Subjectivity and examiner experience in diagnosis of residual caries—An in vitro study. Schweiz Mon. Zahnmed 2007, 117, 123–127. [Google Scholar]
- Ntovas, P.; Loubrinis, N.; Maniatakos, P.; Rahiotis, C. Evaluation of dental explorer and visual inspection for the detection of residual caries among Greek dentists. J. Conserv. Dent. JCD 2018, 21, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Pretty, I.A. Caries detection and diagnosis: Novel technologies. J. Dent. 2006, 34, 727–739. [Google Scholar] [CrossRef]
- Machiulskiene, V.; Nyvad, B.; Baelum, V. A comparison of clinical and radiographic caries diagnoses in posterior teeth of 12-year-old Lithuanian children. Caries Res. 1999, 33, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Machiulskiene, V.; Nyvad, B.; Baelum, V. Comparison of diagnostic yields of clinical and radiographic caries examinations in children of different age. Eur. J. Paediatr. Dent. 2004, 5, 157–162. [Google Scholar] [PubMed]
- Carvalho, J.C. Caries process on occlusal surfaces: Evolving evidence and understanding. Caries Res. 2014, 48, 339–346. [Google Scholar] [CrossRef]
- Banerjee, A.; Splieth, C.; Breschi, L.; Fontana, M.; Paris, S.; Burrow, M.; Crombie, F.; Foster Page, L.; Gaton-Hernandez, P.; Giacaman, R.A.; et al. When to intervene in the caries process? A Delphi consensus statement. Br. Dent. J. 2020, 229, 474–482. [Google Scholar] [CrossRef]
- Schwendicke, F.; Splieth, C.; Breschi, L.; Banerjee, A.; Fontana, M.; Paris, S.; Burrow, M.F.; Crombie, F.; Page, L.F.; Gaton-Hernandez, P.; et al. When to intervene in the caries process? An expert Delphi consensus statement. Clin. Oral. Investig. 2019, 23, 3691–3703. [Google Scholar] [CrossRef]
- Gomez, J. Detection and diagnosis of the early caries lesion. BMC Oral Health 2015, 15, 1–7. [Google Scholar] [CrossRef]
- Foros, P.; Oikonomou, E.; Koletsi, D.; Rahiotis, C. Detection methods for early caries diagnosis: A systematic review and meta-analysis. Caries Res. 2021, 55, 247–259. [Google Scholar] [CrossRef]
- Tagliaferro, E.; Junior, A.V.; Rosell, F.L.; Silva, S.; Riley, J.L.; Gilbert, G.H.; Gordan, V.V. Caries diagnosis in dental practices: Results from dentists in a Brazilian community. Oper. Dent. 2019, 44, E23–E31. [Google Scholar] [CrossRef]
- Fontana, M.; Zero, D. Bridging the gap in caries management between research and practice through education: The Indiana University experience. J. Dent. Educ. 2007, 71, 579–591. [Google Scholar] [CrossRef]
- Frencken, J.E.; Sharma, P.; Stenhouse, L.; Green, D.; Laverty, D.; Dietrich, T. Global epidemiology of dental caries and severe periodontitis—A comprehensive review. J. Clin. Periodontol. 2017, 44, S94–S105. [Google Scholar] [CrossRef]
- Dye, B.A.; Mitnik, G.L.; Iafolla, T.J.; Vargas, C.M. Trends in dental caries in children and adolescents according to poverty status in the United States from 1999 through 2004 and from 2011 through 2014. J. Am. Dent. Assoc. 2017, 148, 550–565. [Google Scholar] [CrossRef]
- Ferreira Zandona, A.; Santiago, E.; Eckert, G.J.; Katz, B.P.; Pereira de Oliveira, S.; Capin, O.R.; Mau, M.; Zero, D.T. The natural history of dental caries lesions: A 4-year observational study. J. Dent. Res. 2012, 91, 841–846. [Google Scholar] [CrossRef]
- Nyvad, B.; Baelum, V. Nyvad criteria for caries lesion activity and severity assessment: A validated approach for clinical management and research. Caries Res. 2018, 52, 397–405. [Google Scholar] [CrossRef]
- Deery, C. The concept of hidden caries. In Detection and Assessment of Dental Caries: A Clinical Guide; Ferreira Zandona, A., Longbottom, C., Eds.; Springer: Cham, Switzerland, 2019; pp. 27–32. [Google Scholar]
- Fontana, M.; Guzman-Armstrong, S.; Schenkel, A.B.; Allen, K.L.; Featherstone, J.; Goolsby, S.; Kanjirath, P.; Kolker, J.; Martignon, S.; Pitts, N.; et al. Development of a core curriculum framework in cariology for U.S. dental schools. J. Dent. Educ. 2016, 80, 705–720. [Google Scholar] [CrossRef] [PubMed]
- Martignon, S.; Gomez, J.; Tellez, M.; Ruiz, J.A.; Marin, L.M.; Rangel, M.C. Current cariology education in dental schools in Spanish-speaking Latin American countries. J. Dent. Educ. 2013, 77, 1330–1337. [Google Scholar] [CrossRef]
- Silvertown, J.D.; Wong, B.P.Y.; Abrams, S.H.; Sivagurunathan, K.S.; Mathews, S.M.; Amaechi, B.T. Comparison of The Canary System and DIAGNO dent for the in vitro detection of caries under opaque dental sealants. J. Investig. Clin. Dent. 2017, 8, 12239. [Google Scholar] [CrossRef] [PubMed]
- Mialhe, F.L.; Pereira, A.C.; Meneghim Mde, C.; Ambrosano, G.M.; Pardi, V. The relative diagnostic yields of clinical, FOTI and radiographic examinations for the detection of approximal caries in youngsters. Indian J. Dent. Res. 2009, 20, 136–140. [Google Scholar] [CrossRef]
- Kim, B., II. Quantitative light-induced fluorescence. In Detection and Assessment of Dental Caries: A Clinical Guide; Ferreira Zandona, A., Longbottom, C., Eds.; Springer: Cham, Switzerland, 2019; pp. 159–170. [Google Scholar]
- van der Veen, M.H.; de Josselin de Jong, E. Application of quantitative light-induced fluorescence for assessing early caries lesions. Monogr. Oral. Sci. 2000, 17, 144–162. [Google Scholar]
- Kuhnisch, J.; Sochtig, F.; Pitchika, V.; Laubender, R.; Neuhaus, K.W.; Lussi, A.; Hickel, R. In vivo validation of near-infrared light transillumination for interproximal dentin caries detection. Clin. Oral. Investig. 2016, 20, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Huynh, G.; Jones, G.; Fried, D. Near-infrared transillumination at 1310-nm for the imaging of early dental decay. Opt. Express 2003, 11, 2259–2265. [Google Scholar] [CrossRef]
- Amaechi, B.T. Photothermal radiometry and modulated luminescence: The Canary System. In Detection and Assessment of Dental Caries: A Clinical Guide; Ferreira Zandona, A., Longbottom, C., Eds.; Springer: Cham, Switzerland, 2019; pp. 177–186. [Google Scholar]
- Kühnisch, J. Near-infrared light transillumination. In Detection and Assessment of Dental Caries: A Clinical Guide; Ferreira Zandona, A., Longbottom, C., Eds.; Springer: Cham, Switzerland, 2019; pp. 151–158. [Google Scholar]
- Mady, S.; Alzayyat, N. Chapter 2—Nanotechnology in targeting and detection of microcavities. In Nanotechnology in Conservative Dentistry; Riad, M.I., Ibrahim, S.H., Eds.; Woodhead: Cambridge, UK, 2021; pp. 29–47. [Google Scholar]
- Hogan, R.; Pretty, I.A.; Ellwood, R.P. Fibre-optic transillumination: FOTI. In Detection and Assessment of Dental Caries: A Clinical Guide; Ferreira Zandona, A., Longbottom, C., Eds.; Springer: Cham, Switzerland, 2019; pp. 139–150. [Google Scholar]
- Abogazalah, N.; Ando, M. Alternative methods to visual and radiographic examinations for approximal caries detection. J. Oral. Sci. 2017, 59, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, K.W.; Lussi, A. DIAGNO dent. In Detection and Assessment of Dental Caries: A Clinical Guide; Ferreira Zandona, A., Longbottom, C., Eds.; Springer: Cham, Switzerland, 2019; pp. 171–175. [Google Scholar]
- Almaz, E.C.; Simon, J.C.; Fried, D.; Darling, C.L. Influence of stains on lesion contrast in the pits and fissures of tooth occlusal surfaces from 800–1600-nm. Proc. SPIE Int. Soc. Opt. Eng. 2016, 9692, 96920X. [Google Scholar]
- Schwendicke, F.; Tzschoppe, M.; Paris, S. Radiographic caries detection: A systematic review and meta-analysis. J. Dent. 2015, 43, 924–933. [Google Scholar] [CrossRef]
- Silvertown, J.D.; Wong, B.P.Y.; Sivagurunathan, K.S.; Abrams, S.H.; Kirkham, J.; Amaechi, B.T. Remineralization of natural early caries lesions in vitro by P11-4 monitored with photothermal radiometry and luminescence. J. Investig. Clin. Dent. 2017, 8, 12257. [Google Scholar] [CrossRef]
- Vaarkamp, J.; ten Bosch, J.J.; Verdonschot, E.H.; Bronkhoorst, E.M. The real performance of bitewing radiography and fiber-optic transillumination in approximal caries diagnosis. J. Dent. Res. 2000, 79, 1747–1751. [Google Scholar] [CrossRef] [PubMed]
- Bussaneli, D.G.; Restrepo, M.; Boldieri, T.; Pretel, H.; Mancini, M.W.; Santos-Pinto, L.; Cordeiro, R.C.L. Assessment of a new infrared laser transillumination technology (808 nm) for the detection of occlusal caries—an in vitro study. Lasers Med Sci. 2015, 30, 1873–1879. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.C.; Lucas, S.A.; Staninec, M.; Tom, H.; Chan, K.H.; Darling, C.L.; Cozin, M.J.; Lee, R.C.; Fried, D. Near-IR transillumination and reflectance imaging at 1300 nm and 1500–1700 nm for in vivo caries detection. Lasers Surg. Med. 2016, 48, 828–836. [Google Scholar] [CrossRef] [PubMed]
- Kishore, M.; Panat, S.R.; Aggarwal, A.; Agarwal, N.; Upadhyay, N.; Alok, A. Evidence based dental care: Integrating clinical expertise with systematic research. J. Clin. Diagn. Res. 2014, 8, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Bahammam, M.A.; Linjawi, A.I. Knowledge, attitude, and barriers towards the use of evidence based practice among senior dental and medical students in western Saudi Arabia. Saudi Med. J. 2014, 35, 1250–1256. [Google Scholar] [PubMed]
- Afshar, M.K.; Torabi, M.; Khalafi, E.; Shamsadini, Z.; Afshar, M.K.; Mohammadzadeh, I. Knowledge, attitude and practice regarding caries risk assessment and management in general dentists—A cross sectional survey. J. Evol. Med Dent. Sci. 2019, 8, 3499–3504. [Google Scholar] [CrossRef]
- Ismail, A.I.; Tellez, M.; Pitts, N.B.; Ekstrand, K.R.; Ricketts, D.; Longbottom, C.; Eggertsson, H.; Deery, C.; Fisher, J.; Young, D.A.; et al. Caries management pathways preserve dental tissues and promote oral health. Community Dent. Oral. Epidemiol. 2013, 41, 12–40M. [Google Scholar] [CrossRef]
- Tranaeus, S.; Shi, X.Q.; Angmar-Mansson, B. Caries risk assessment: Methods available to clinicians for caries detection. Community Dent. Oral. Epidemiol. 2005, 33, 265–273. [Google Scholar] [CrossRef]
- Spaveras, A.; Karkazi, F.; Antoniadou, M. Caries detection with laser fluorescence devices. Limitations of their use. Stoma. Edu. J. 2017, 4, 46–53. [Google Scholar] [CrossRef]
- Gordan, V.V.; Riley, J.L., III; Carvalho, R.M.; Snyder, J.; Sanderson, J.L., Jr.; Anderson, M.; Gilbert, G.H. Methods used by dental practice-based research network (DPBRN) dentists to diagnose dental caries. Oper. Dent. 2011, 36, 2–11. [Google Scholar] [CrossRef][Green Version]
- Bader, J.D.; Shugars, D.A.; Bonito, A.J. Systematic reviews of selected dental caries diagnostic and management methods. J. Dent. Educ. 2001, 65, 960–968. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, M.I.G.; de Melo Alencar, C.; de Paula, B.L.F.; Magno, M.B.; Maia, L.C.; Silva, C.M. Accuracy of near-infrared light transillumination (NILT) compared to bitewing radiograph for detection of interproximal caries in the permanent dentition: A systematic review and meta-analysis. J. Dent. 2020, 98, 103351. [Google Scholar] [CrossRef] [PubMed]
- Marwa, A.; Ivo, K. Longitudinal caries detection and monitoring with near infrared transillumination. In Proceedings of the SPIE BIOS Conference, San Francisco, CA, USA, 2−7 February 2019. [Google Scholar]
- Bounds, A.D.; Girkin, J.M. Early stage dental caries detection using near infrared spatial frequency domain imaging. Sci. Rep. 2021, 11, 2433. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Gallardo, I.; Martin-Gonzalez, J.; Jimenez-Sanchez, M.C.; Cabanillas-Balsera, D.; Sanchez-Dominguez, B.; Segura-Egea, J.J. Dentist s knowledge, attitudes and determining factors of the conservative approach in teeth with reversible pulpitis and deep caries lesions. J. Clin. Exp. Dent. 2018, 10, 1205–1215. [Google Scholar] [CrossRef] [PubMed]
- Makhija, S.K.; Robinson, M.E.; Bader, J.D.; Shugars, D.A.; Litaker, M.S.; Im, H.R.; Rindal, D.B.; Pihlstrom, D.J.; Meyerowitz, C.; Gordan, V.V.; et al. Dentists’ decision strategies for suspicious occlusal caries lesions in a National Dental PBRN study. J. Dent. 2018, 69, 83–87. [Google Scholar] [CrossRef]
- Didier, H.; Assandri, F.; Gaffuri, F.; Cavagnetto, D.; Abate, A.; Villanova, M.; Maiorana, C. The role of dental occlusion and neuromuscular behavior in professional ballet dancers’ performance: A pilot study. Healthcare 2021, 9, 251. [Google Scholar] [CrossRef]
- Jeganath, J.; Wong, A.; Chandler, N.; Murray, C. New Zealand general dentists’ usage and views on caries detection methods. New Zealand Dent. J. 2016, 112, 73–79. [Google Scholar]
- Strassler, H.E.; Pitel, M.L. Using fiber-optic transillumination as a diagnostic aid in dental practice. Compend. Contin. Educ. Dent. 2014, 35, 80–88. [Google Scholar]
- Stookey, G.K. (Ed.) Early Detection of Dental Caries: Early detection of dental caries: Proceedings of the 1st annual Indiana Conference; Indiana University: Indianapolis, IN, USA, 1996. [Google Scholar]
- Davies, G.M.; Worthington, H.V.; Clarkson, J.E.; Thomas, P.; Davies, R.M. The use of fibre-optic transillumination in general dental practice. Br. Dent. J. 2001, 191, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, K.W.; Rodrigues, J.A.; Seemann, R.; Lussi, A. Detection of proximal secondary caries at cervical class II-amalgam restoration margins in vitro. J. Dent. 2012, 40, 493–499. [Google Scholar] [CrossRef]
- Rodrigues, J.A.; Neuhaus, K.W.; Hug, I.; Stich, H.; Seemann, R.; Lussi, A. In vitro detection of secondary caries associated with composite restorations on approximal surfaces using laser fluorescence. Oper. Dent. 2010, 35, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Kim, S.K.; Lee, H.S.; Lee, E.S.; de Josselin de Jong, E.; Kim, B.I. Comparison of fluorescence parameters between three generations of QLF devices for detecting enamel caries in vitro and on smooth surfaces. Photodiagnosis Photodyn. Ther. 2019, 25, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Abrams, S.H.; Sivagurunathan, K.S.; Silvertown, J.D.; Wong, B.; Hellen, A.; Mandelis, A.; Hellen, W.M.P.; Elman, G.I.; Mathew, S.M.; Mensinkai, P.K.; et al. Correlation with caries lesion depth of the Canary System, DIAGNO dent and ICDAS II. Open Dent. J. 2017, 11, 679–689. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Assessment of NCDTs Using ANOVA | ||||||||
|---|---|---|---|---|---|---|---|---|
| 95% Confidence Interval for Mean | ||||||||
| N | Mean | SD * | SEM ** | Lower Bound | Upper Bound | Minimum | Maximum | |
| PTR and modulated LUM | 20 | 48.00 | 16.65 | 3.72 | 40.21 | 55.79 | 20.00 | 80.00 |
| FOTI | 20 | 78.50 | 19.06 | 4.26 | 69.58 | 87.42 | 25.00 | 100.00 |
| QLF | 20 | 46.00 | 18.54 | 4.15 | 37.32 | 54.68 | 15.00 | 95.00 |
| LF | 20 | 60.75 | 15.92 | 3.56 | 53.30 | 68.20 | 25.00 | 85.00 |
| NIT | 20 | 53.00 | 21.11 | 4.72 | 43.12 | 62.88 | 20.00 | 85.00 |
| One way Analysis of variance Table ANOVA | ||||||||
| Sum of Squares | Df *** | Mean Square | F | P value | ||||
| Between Groups | 13880.00 | 4 | 3470.00 | 10.31 | 0.000001 | |||
| Within Groups | 31988.75 | 95 | 336.72 | |||||
| Total | 45868.75 | 99 | ||||||
| 95% Confidence Interval | ||||||
|---|---|---|---|---|---|---|
| Mean Difference | Std. Error | P Value | Lower Bound | Upper Bound | ||
| PTR and modulated LUM a | FOTI | −30.5 | 5.8 | 0.000009 * | −47.18 | −13.82 |
| PTR and modulated LUM a | QLF a | 2 | 5.8 | 1 | −14.68 | 18.68 |
| PTR and modulated LUM a | LF a | −12.75 | 5.8 | 0.304361 | −29.43 | 3.93 |
| PTR and modulated LUM a | NIT a | −5 | 5.8 | 1 | −21.68 | 11.68 |
| FOTI | QLF a | 32.5 | 5.8 | 0.000002 * | 15.82 | 49.18 |
| FOTI | LF a | 17.75 | 5.8 | 0.028869 * | 1.07 | 34.43 |
| FOTI | NIT a | 25.5 | 5.8 | 0.000289 * | 8.82 | 42.18 |
| QLF a | LF a | −14.75 | 5.8 | 0.126437 | −31.43 | 1.93 |
| QLF a | NIT a | −7 | 5.8 | 1 | −23.68 | 9.68 |
| LF a | NIT a | 7.75 | 5.8 | 1 | −8.93 | 24.43 |
| Parameter | Photothermal Radiometry and Modulated Luminescence (PTR/LUM) | Fiberoptic and Digital Fiberoptic Transillumination (FOTI and DIFOTI) | Quantitative Light-Induced Fluorescence (QLF) | Laser Fluorescence (LF) | Near infrared Light transillumination (NIT) and Near-Infrared Reflectance (NIR) |
|---|---|---|---|---|---|
| Commercial product examples | Canary System (Quantum Dental Technologies, Toronto, Canada) | Phatelus Optic Transillumination Light (NSK, Tochigi, Japan) Microlux (AdDent Inc., CT, USA) DiaLUX probe (KaVo Dental GmBH, Biberach, Germany) | * The Inspektor™ Pro QLF, * The Inspektor™ QLF-D Biluminator™ 2+ * Qscan™ (* Inspektor Research Systems BV, Bussum, The Netherlands) | DiagnoDent pen (KaVo Dental GmBH, Biberach, Germany) | DIAGNOcam (KaVo Dental GmBH, Biberach, Germany) CariVu (DEXIS, LLC, Hatfield, PA, USA) |
| Year of introduction * | 2010 | From 1990s | first generation Inspektor: 2004 | Early 2000s | 2012 (Europe) 2013 (USA) |
| Concept | Conversion of optical energy produced from a laser source into irradiation leading to temperature changes detected by an infrared detector [43] | White light scattering [14,34,44] (wavelength = 450–700 nm) | Green and red fluorescence of EDJ after exposure to visible blue light [45,46] (wavelength~400–488 nm) | Fluorescence due to bacterial protoporphyrin after the application of red light [14,26,43] (wavelength = 655 nm) | Transillumination of near- infrared light (wavelength ~780 nm) using two light emission windows [26,47] (NIR wavelength = 1310 nm) [48] |
| Main indication | Proximal caries lesions and cracks [49] | Detection of proximal caries lesions [14] | Smooth (facial) surface lesions [45] | Occlusal caries lesions [14] | Detection of proximal caries lesions in posterior teeth [50] |
| Caries lesion quantification ** | Yes | No | Yes | Partial (0–99 scale depending on fluorescence of bacterial protoporphyrin) [51] | Partial (Grey scale) |
| Caries lesion activity determination [18,26] | No | No | Yes | No | No |
| Main shortcoming | It is often not possible to correlate the Canary Number to results of visual examination or bitewing (BW) radiographs [49] | No lesion quantification, Subjective [14,52], Potential higher false positive due to difficulty to differentiate between caries lesions and developmental defects and stains, False negative due to large restoration FOTI unsuitable for longitudinal lesion monitoring [53] | Not indicated for proximal lesions Sensitive to the ambient light, difficult accurate repositioning of intraoral camera type devices to take the next image [45] | High values for false positive, no detection of cavitation, no imaging [43], requires clean teeth and calibration on a sound surface before use [20,54] | Not indicated for smooth surface on the facial surfaces, No imaging of the caries extension relative to the pulp [50] |
| Main Advantage | Doesn’t require a dry field [51],detection of secondary caries around composite and below resin infiltrants, high repeatability. Canary Software connects with compatible practice management software, so that it can be easily moved around a dental office [49] | Affordability, short learning curve, Ease of use, applicability in other dental situations [52] | nondestructive quantification (numerical values) of the physical characteristics of caries lesions, QLF-D advanced device was able to analyze the entire oral cavity extraorally [26,45,46] | Caries monitoring possible [20,53] | NIR with longer wavelengths have no interference from occlusal surface stains [55], possible to detect caries lesions close to restoration margins, relative ease of use, crack detection, repeatability [50] |
| Set-up | Laser-emitting box with a handpiece containing an intraoral camera | Light-emitting electrode attached to a hand-held box (DiaLUXattached to the dental unit) (DIFOTI contains CCD sensor producing grey scale image) | Light box attached to a handpiece containing a light source and an intraoral camera | Red Laser producing box attached to a handpiece with different tips | Handpiece with near infrared light source and CCD sensor connected to a computer |
| Radiation/ Hazards * | Needs eye protection | None | Needs eye protection | Needs eye protection | None |
| Sensitivity (vs. X-ray ~0.41) [56] | range in 97% [49,57] | 0.70 ± 0.01 to 0.50 ± 0.02 [58] | ~0.69 [59] | 0.76 to 1.00 [43] | 99% for dentin caries detection on proximal surfaces under in vivo conditions [47] NIR:0.53 proximal and 0.49 occlusal [60] |
| Specificity (vs. X-ray ~0.78) [56] | range in 97% [49,57] | DIFOTI = 0.76 | ~0.83 [59] | 0.47 to 0.94 [43] | NIR: 0.86 proximal and 0.70 occlusal [60] |
| Occlusal Caries ** | Yes | No (error possibility) | Yes | Yes | Yes |
| Proximal caries ** | Yes | Yes | No (detect bacterial porphyrins using 3rd generation QLF) [45] | Yes | Yes |
| Facial surface caries ** | Yes | No | Yes | No | No |
| Price * | $$$$$ | $ | $$$$$ | $$ | $$$ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nassar, H.M.; Yeslam, H.E. Current Novel Caries Diagnostic Technologies: Restorative Dentists’ Attitude and Use Preferences. Healthcare 2021, 9, 1387. https://doi.org/10.3390/healthcare9101387
Nassar HM, Yeslam HE. Current Novel Caries Diagnostic Technologies: Restorative Dentists’ Attitude and Use Preferences. Healthcare. 2021; 9(10):1387. https://doi.org/10.3390/healthcare9101387
Chicago/Turabian StyleNassar, Hani M., and Hanin E. Yeslam. 2021. "Current Novel Caries Diagnostic Technologies: Restorative Dentists’ Attitude and Use Preferences" Healthcare 9, no. 10: 1387. https://doi.org/10.3390/healthcare9101387
APA StyleNassar, H. M., & Yeslam, H. E. (2021). Current Novel Caries Diagnostic Technologies: Restorative Dentists’ Attitude and Use Preferences. Healthcare, 9(10), 1387. https://doi.org/10.3390/healthcare9101387