
Artificial Intelligence in Digital Pathology: What Is the Future? Part 2: An Investigation on the Insiders


Abstract
:1. Introduction
- The development of the DP, due to the introduction of whole-slide scanners and the progress of computer vision algorithms, have significantly grown the usage of AI. It can perform tumor diagnosis, subtyping, grading, staging, and prognostic prediction
- The pathological diagnosis of the future could merge proteomics and genomics in the BIG-DATA.
- Delay of digital cytology.
- Greater complexity in the introduction of AI in digital cytology.
- Focus on the DICOM WSI standard.
- Attention to both eHealth and mHealth.
- New training models must adapt to AI in DP.
- Need for standardization actions.
- Extensive acceptance surveys on professionals.
- Need to focus on all the professionals involved.
- ▪
- ▪
- Submit it electronically to a first sample of insiders.
- ▪
- Analyze the outcome.
2. Materials and Methods
3. Results
4. Discussion and Conclusions
shows 2290 results as of 23 August 2021 (907 in 2021).(artificial intelligence [Title/Abstract]) AND (image [Title/Abstract])
This justifies the need of focusing on studies of acceptance, in consideration of both the interest of the scholars and the possible opportunities in the clinical routine.
The three illustrated potentials [25,26,27] are also important in DP. In fact, in DP, the need for categorizing images merges with the need to make decisions and/or deduce approaches through actions on large databases and data sets or with other needs not based on medical images [1,19,20]. The implications are multifaceted. It is necessary to carry out direct studies on the opinion of insiders in view of the introduction of the clinical routine of AI.
we found as of 23 August 2021 only two studies based on non-validated and non-standardized questionnaires.((digital pathology [Title/Abstract]) AND (artificial intelligence [Title/Abstract])) AND (survey [Title/Abstract])-even with alternative terms to the survey-
5. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giovagnoli, M.; Giansanti, D. Artificial Intelligence in Digital Pathology: What Is the Future? Part 1: From the Digital Slide Onwards. Healthcare 2021, 9, 858. [Google Scholar] [CrossRef] [PubMed]
- Giansanti, D.; Pochini, M.; Giovagnoli, M.R. Integration of Tablet Technologies in the e-Laboratory of Cytology: A Health Technology Assessment. Telemed. e-Health 2014, 20, 909–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giansanti, D.; Castrichella, L.; Giovagnoli, M.R. The Design of a Health Technology Assessment System in Telepathology. Telemed. e-Health 2008, 14, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Latonen, L.; Ruusuvuori, P. Building a central repository landmarks a new era for artificial intelligence–assisted digital pathology development in Europe. Eur. J. Cancer 2021, 150, 31–32. [Google Scholar] [CrossRef] [PubMed]
- Aeffner, F.; Sing, T.; Turner, O.C. Special Issue on Digital Pathology, Tissue Image Analysis, Artificial Intelligence, and Machine Learning: Approximation of the Effect of Novel Technologies on Toxicologic Pathology. Toxicol. Pathol. 2021, 49, 705–708. [Google Scholar] [CrossRef]
- Sobhani, F.; Robinson, R.; Hamidinekoo, A.; Roxanis, I.; Somaiah, N.; Yuan, Y. Artificial intelligence and digital pathology: Opportunities and implications for immuno-oncology. Biochim. Biophys. Acta (BBA) Bioenerg. 2021, 1875, 188520. [Google Scholar] [CrossRef]
- Abdolahi, M.; Salehi, M.; Shokatian, I.; Reiazi, R. Artificial intelligence in automatic classification of invasive ductal carcinoma breast cancer in digital pathology images. Med. J. Islam. Repub. Iran 2020, 34, 965–973. [Google Scholar] [CrossRef]
- Sakamoto, T.; Furukawa, T.; Lami, K.; Pham, H.H.N.; Uegami, W.; Kuroda, K.; Kawai, M.; Sakanashi, H.; Cooper, L.A.D.; Bychkov, A.; et al. A narrative review of digital pathology and artificial intelligence: Focusing on lung cancer. Transl. Lung Cancer Res. 2020, 9, 2255–2276. [Google Scholar] [CrossRef]
- Bera, K.; Katz, I.; Madabhushi, A. Reimagining T Staging Through Artificial Intelligence and Machine Learning Image Processing Approaches in Digital Pathology. JCO Clin. Cancer Inform. 2020, 4, 1039–1050. [Google Scholar] [CrossRef] [PubMed]
- Salama, M.E.; Macon, W.R.; Pantanowitz, L. Is the time right to start using digital pathology and artificial intelligence for the diagnosis of lymphoma? J. Pathol. Inform. 2020, 11, 16. [Google Scholar] [CrossRef]
- Browning, L.; Colling, R.; Rakha, E.; Rajpoot, N.; Rittscher, J.; James, J.A.; Salto-Tellez, M.; Snead, D.R.J.; Verrill, C. Digital pathology and artificial intelligence will be key to supporting clinical and academic cellular pathology through COVID-19 and future crises: The PathLAKE consortium perspective. J. Clin. Pathol. 2020, 74, 443–447. [Google Scholar] [CrossRef]
- Parwani, A.V.; Amin, M.B. Convergence of Digital Pathology and Artificial Intelligence Tools in Anatomic Pathology Practice: Current Landscape and Future Directions. Adv. Anat. Pathol. 2020, 27, 221–226. [Google Scholar] [CrossRef]
- Harmon, S.A.; Sanford, T.H.; Brown, G.T.; Yang, C.; Mehralivand, S.; Jacob, J.M.; Valera, V.A.; Shih, J.H.; Agarwal, P.K.; Choyke, P.L.; et al. Multiresolution Application of Artificial Intelligence in Digital Pathology for Prediction of Positive Lymph Nodes From Primary Tumors in Bladder Cancer. JCO Clin. Cancer Inform. 2020, 4, 367–382. [Google Scholar] [CrossRef] [PubMed]
- Parwani, A.V. Next generation diagnostic pathology: Use of digital pathology and artificial intelligence tools to augment a pathological diagnosis. Diagn. Pathol. 2019, 14, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Turner, O.C.; Aeffner, F.; Bangari, D.S.; High, W.; Knight, B.; Forest, T.; Cossic, B.; Himmel, L.E.; Rudmann, D.G.; Bawa, B.; et al. Society of Toxicologic Pathology Digital Pathology and Image Analysis Special Interest Group Article*: Opinion on the Application of Artificial Intelligence and Machine Learning to Digital Toxicologic Pathology. Toxicol. Pathol. 2019, 48, 277–294. [Google Scholar] [CrossRef]
- Bera, K.; Schalper, K.A.; Rimm, D.L.; Velcheti, V.; Madabhushi, A. Artificial intelligence in digital pathology—New tools for diagnosis and precision oncology. Nat. Rev. Clin. Oncol. 2019, 16, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Colling, R.; Pitman, H.; Oien, K.; Rajpoot, N.; Macklin, P.; CM-Path AI in Histopathology Working Group; Snead, D.; Sackville, T.; Verrill, C. Artificial intelligence in digital pathology: A roadmap to routine use in clinical practice. J. Pathol. 2019, 249, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Niazi, M.K.K.; Parwani, A.V.; Gurcan, M.N. Digital pathology and artificial intelligence. Lancet Oncol. 2019, 20, e253–e261. [Google Scholar] [CrossRef]
- Tizhoosh, H.R.; Pantanowitz, L. Artificial intelligence and digital pathology: Challenges and opportunities. J. Pathol. Inform. 2018, 9, 38. [Google Scholar] [CrossRef]
- Avanzo, M.; Trianni, A.; Botta, F.; Talamonti, C.; Stasi, M.; Iori, M. Artificial Intelligence and the Medical Physicist: Welcome to the Machine. Appl. Sci. 2021, 11, 1691. [Google Scholar] [CrossRef]
- Sarwar, S.; Dent, A.; Faust, K.; Richer, M.; Djuric, U.; Van Ommeren, R.; Diamandis, P. Physician perspectives on integration of artificial intelligence into diagnostic pathology. NPJ Digit. Med. 2019, 2, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Grimshaw, J. SURGE (The SUrvey Reporting GuidelinE). In Guidelines for Reporting Health Research: A User’s Manual; John Wiley & Sons, Ltd.: Oxford, UK, 2014; pp. 206–213. [Google Scholar] [CrossRef]
- Available online: https://forms.office.com/Pages/ResponsePage.aspx?id=_ccwzxZmYkutg7V0sn1ZEvPNtNci4kVMpoVUounzQ3tUNjNSVENQU01DRTVVWUkxMVg5V0tBQUhKMy4u (accessed on 9 October 2021).
- Available online: https://drive.google.com/file/d/1Av6cNrjkOi-00VNT7vtqBEZeDWpKnZXP/view?usp=sharing (accessed on 9 October 2021).
- Barbieri, D.; Chawla, N.; Zaccagni, L.; Grgurinović, T.; Šarac, J.; Čoklo, M.; Missoni, S. Predicting Cardiovascular Risk in Athletes: Resampling Improves Classification Performance. Int. J. Environ. Res. Public Health 2020, 17, 7923. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, D.; Giuliani, E.; Del Prete, A.; Losi, A.; Villani, M.; Barbieri, A. How Artificial Intelligence and New Technologies Can Help the Management of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 7648. [Google Scholar] [CrossRef] [PubMed]
- Halasz, G.; Sperti, M.; Villani, M.; Michelucci, U.; Agostoni, P.; Biagi, A.; Rossi, L.; Botti, A.; Mari, C.; Maccarini, M.; et al. A Machine Learning Approach for Mortality Prediction in COVID-19 Pneumonia: Development and Evaluation of the Piacenza Score. J. Med. Internet Res. 2021, 23, e29058. [Google Scholar] [CrossRef] [PubMed]
- Farris, A.B.; Moghe, I.; Wu, S.; Hogan, J.; Cornell, L.D.; Alexander, M.P.; Kers, J.; Demetris, A.J.; Levenson, R.M.; Tomaszewski, J.; et al. Banff Digital Pathology Working Group: Going digital in transplant pathology. Am. J. Transplant. 2020, 20, 2392–2399. [Google Scholar] [CrossRef] [Green Version]
- Tsuchihashi, Y. Expanding application of digital pathology in Japan—From education, telepathology to autodiagnosis. Diagn. Pathol. 2011, 6, S19. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
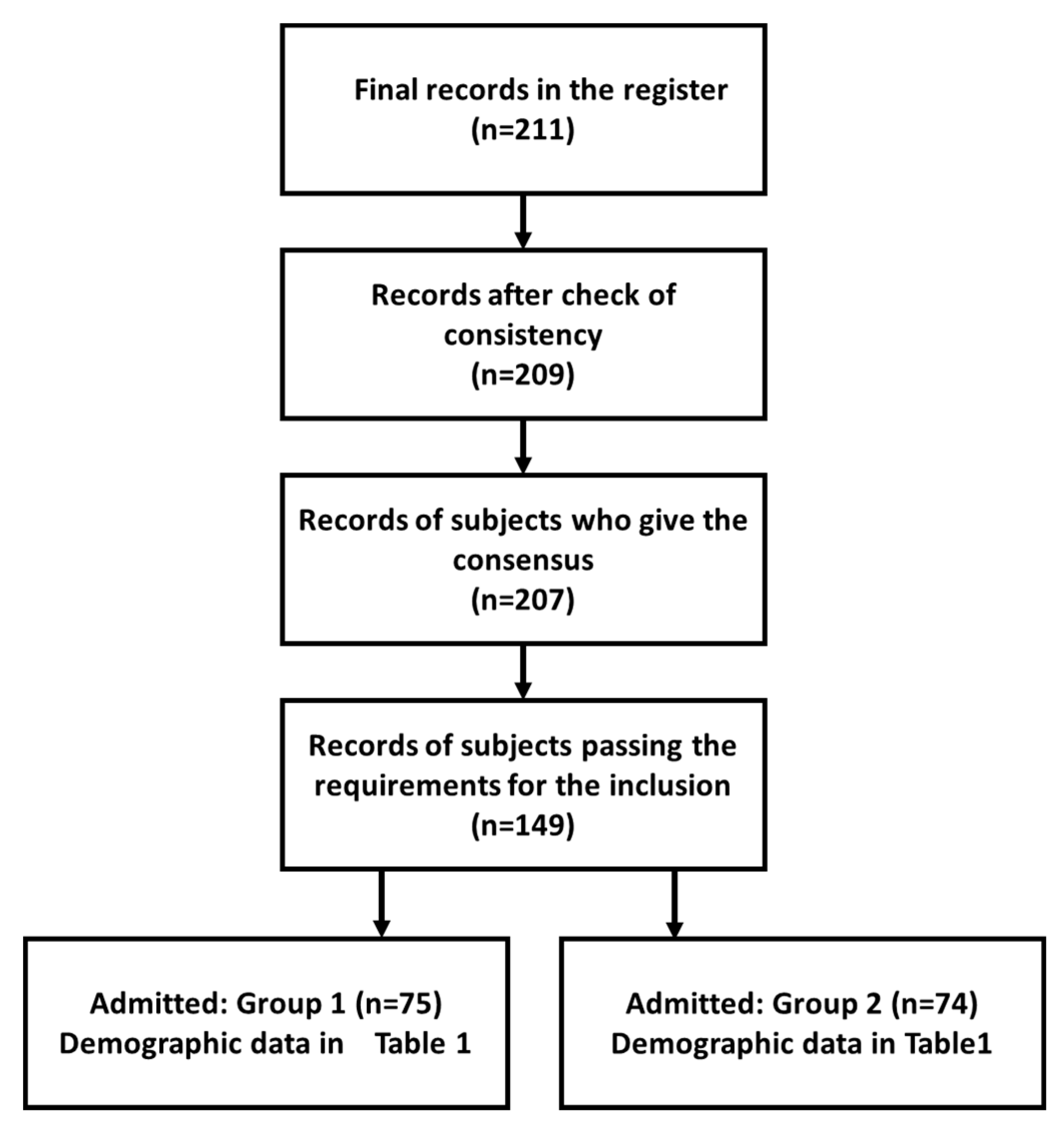
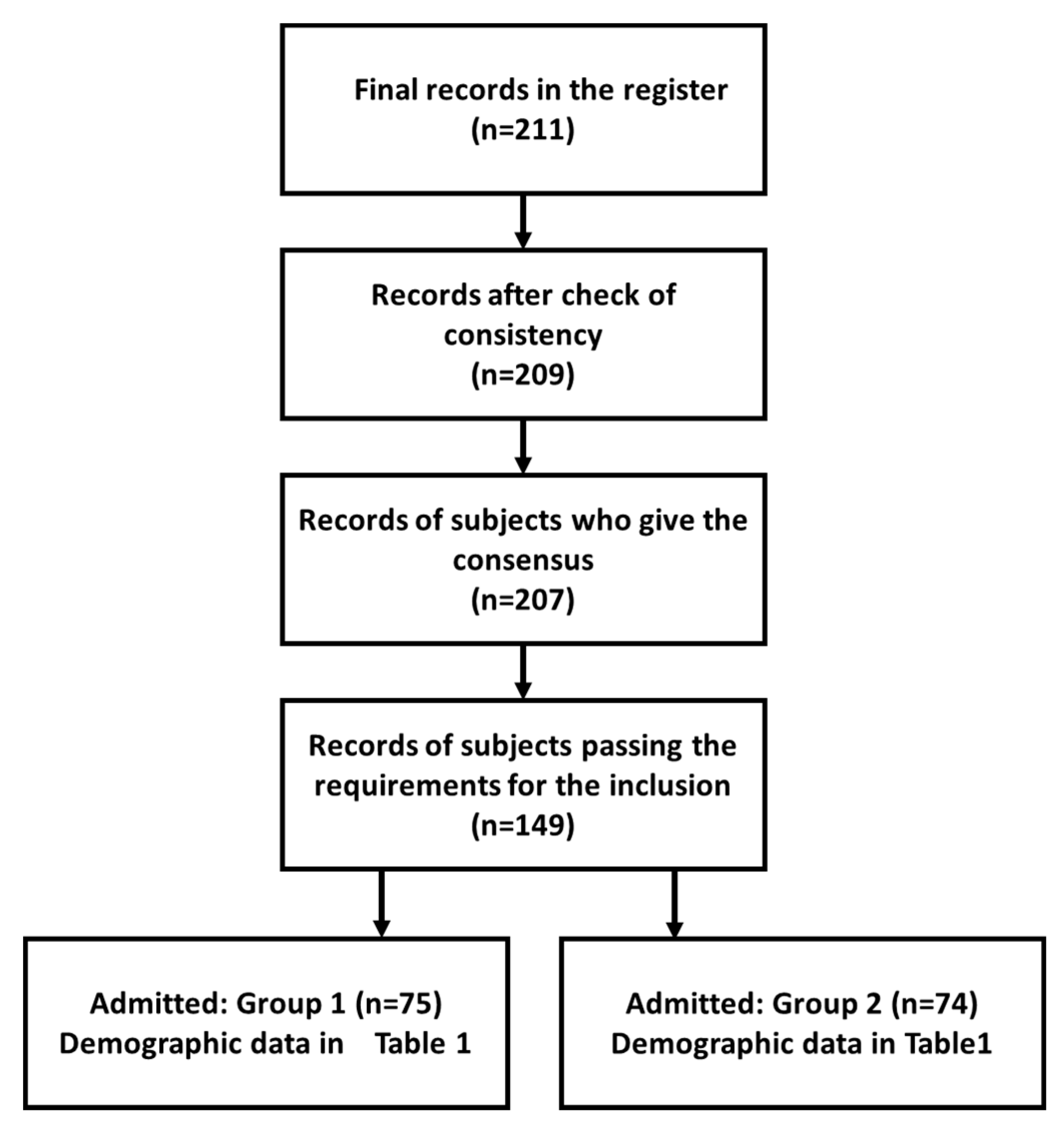
| Submission | Participants | Males/Females | Min Age/Max Age | Mean Age |
|---|---|---|---|---|
| Biomedical laboratory technicians under the course of the study (BLT-DCS) | 75 | 39/36 | 21/36 | 25.3 |
| Biomedical laboratory technicians after the course of the study (BLT-ACS) | 74 | 37/37 | 25/59 | 41.8 |
| Feature | Rating DCS | Rating ACS | p-Value |
|---|---|---|---|
| Q6: Degree of knowledge in computer science | 4.8 | 4.9 | 0.009 |
| Q7: Degree of knowledge of biomedical technologies | 4.7 | 4.7 | 0.134 |
| Q9: Degree of knowledge of AI (in general) | 3.3 | 3.1 | 0.009 |
| Q10: Degree of knowledge of AI (in biomedical sector) | 3.4 | 3.2 | 0.009 |
| Q11: Degree of direct knowledge of technologies and applications of AI (in biomedical sector) | 1.8 | 1.3 | 0.008 |
| Feature | Rating DCS | Rating ACS | p-Value |
|---|---|---|---|
| Digital cytology | 4.9 | 4.5 | 0.008 |
| Digital histology | 4.8 | 4.4 | 0.009 |
| Omics (e.g., genomics and proteomics) | 4.6 | 4.3 | 0.008 |
| Integration with BIG-DATA | 3.9 | 3.7 | 0.008 |
| Integration with historical and clinical data of the patient | 4.1 | 3.8 | 0.009 |
| Search for slide labeling | 3.9 | 3.6 | 0.009 |
| Quality control | 4.1 | 3.8 | 0.009 |
| Integration of DP with digital radiology | 4.2 | 3.9 | 0.009 |
| Quality control | 4.5 | 4.2 | 0.008 |
| Integration with the virtual medical record | 3.9 | 3.7 | 0.008 |
| Training | 3.9 | 3.6 | 0.008 |
| Feature | Rating DCS | Rating ACS | p-Value |
|---|---|---|---|
| Risk analysis | 4.3 | 3.7 | 0.008 |
| Therapy | 4.4 | 3.8 | 0.008 |
| Prevention | 3.9 | 3.6 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giovagnoli, M.R.; Ciucciarelli, S.; Castrichella, L.; Giansanti, D. Artificial Intelligence in Digital Pathology: What Is the Future? Part 2: An Investigation on the Insiders. Healthcare 2021, 9, 1347. https://doi.org/10.3390/healthcare9101347
Giovagnoli MR, Ciucciarelli S, Castrichella L, Giansanti D. Artificial Intelligence in Digital Pathology: What Is the Future? Part 2: An Investigation on the Insiders. Healthcare. 2021; 9(10):1347. https://doi.org/10.3390/healthcare9101347
Chicago/Turabian StyleGiovagnoli, Maria Rosaria, Sara Ciucciarelli, Livia Castrichella, and Daniele Giansanti. 2021. "Artificial Intelligence in Digital Pathology: What Is the Future? Part 2: An Investigation on the Insiders" Healthcare 9, no. 10: 1347. https://doi.org/10.3390/healthcare9101347
APA StyleGiovagnoli, M. R., Ciucciarelli, S., Castrichella, L., & Giansanti, D. (2021). Artificial Intelligence in Digital Pathology: What Is the Future? Part 2: An Investigation on the Insiders. Healthcare, 9(10), 1347. https://doi.org/10.3390/healthcare9101347