Effects of Attitude, Barriers/Facilitators, and Visual Differentiation on Oral Mucosa Pressure Ulcer Prevention Performance Intention

Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants and Data Collection
2.3. Instrument
2.3.1. General Characteristics
2.3.2. Intention to Perform Oral Mucosa PU Prevention
2.3.3. Attitude
2.3.4. Barriers and Facilitators of Oral Mucosa PU Prevention
2.3.5. Visual Differentiation Ability
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
3.1. General Characteristics of the Participants
3.2. Characteristics of the Variables
3.3. Correlation between Variables
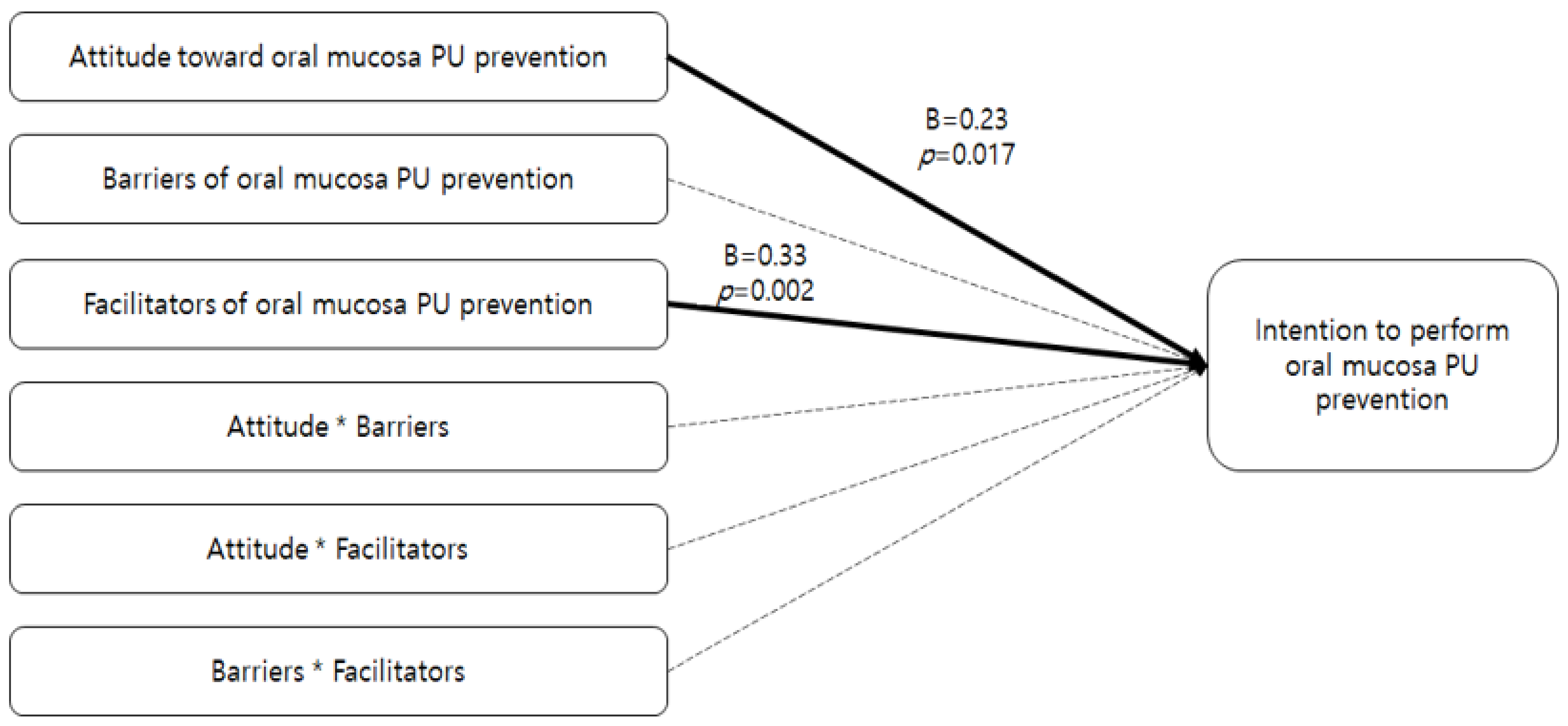
3.4. Factors Affecting Intention to Perform Oral Mucosa PU Prevention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schank, J.E. The NPUAP Meeting—This was no consensus conference. J. Am. Coll. Clin. Wound Spec. 2015, 7, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Barakat-Johnson, M.; Lai, M.; Wand, T.; Li, M.; White, K.; Coyer, F. The incidence and prevalence of medical device-related pressure ulcers in intensive care: A systematic review. J. Wound Care 2019, 28, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Karadag, A.; Hanönü, S.C.; Eyikara, E. A prospective, descriptive study to assess nursing staff perceptions of and interventions to prevent medical device-related pressure injury. Ostomy Wound Manag. 2017, 63, 34–41. [Google Scholar]
- Hanonu, S.; Karadag, A. A prospective, descriptive study to determine the rate and characteristics of and risk factors for the development of medical device-related pressure ulcers in intensive care units. Ostomy Wound Manag. 2016, 62, 12–22. [Google Scholar]
- Kim, C.H.; Kim, M.S.; Kang, M.J.; Kim, H.H.; Park, N.J.; Jung, H.K. Oral mucosa pressure ulcers in intensive care unit patients: A preliminary observational study of incidence and risk factors. J. Tissue Viability 2019, 28, 27–34. [Google Scholar] [CrossRef]
- Kayser, S.A.; VanGilder, C.A.; Ayello, E.A.; Lachenbruch, C. Prevalence and analysis of medical device-related pressure injuries: Results from the International pressure ulcer prevalence survey. Adv. Skin Wound Care 2018, 31, 276–285. [Google Scholar] [CrossRef]
- Kim, S. Relationships between Oral-Mucosal Pressure Ulcers, Mechanical Conditions, and Individual Susceptibility in Intubated Patients Under Intensive Care: A PCU-Based Observational Study. Master’s Thesis, Pukyong National University, Busan, South Korea, 2020. [Google Scholar]
- Dyer, A. Ten top tips: Preventing device-related pressure ulcers. Wounds Int. 2015, 6, 9–13. [Google Scholar]
- Coke, L.; Otten, K.; Staffileno, B.; Minarich, L.; Nowiszewski, C. The impact of an oral hygiene education module on patient practices and nursing documentation. Clin. J. Oncol. Nurs. 2015, 19, 75–80. [Google Scholar] [CrossRef]
- Kim, A.; Jeong, I. Performance of evidence-based pressure ulcer prevention practices among hospital nurses. Glob. Health Nurs. 2018, 8, 8–16. [Google Scholar]
- Hrisos, S.; Eccles, M.P.; Francis, J.J.; Dickinson, H.O.; Kaner, E.F.; Beyer, F.; Johnston, M. Are there valid proxy measures of clinical behaviour? A systematic review. Implement Sci. 2009, 4, 37. [Google Scholar] [CrossRef]
- Rollon, R. Using the theory of planned behavior to improve perioperative practice. AORN J. 2020, 111, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ Behav. Human Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Gollwitzer, P.M. Implementation intentions: Strong effects of simple plans. Am. Psychol. 1999, 54, 493. [Google Scholar] [CrossRef]
- Choi, E.J.; Kang, S.W. The relationship between acceptance intention toward a smartphone healthcare application and health-promoting behaviors among nursing students. Comput. Inform. Nurs. 2018, 36, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Park, O.K.; Park, M.Y. A structural equation model of pressure ulcer prevention action in clinical nurses. J. Korean Acad. Nurs. 2016, 46, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior: Frequently asked questions. Human Behav. Emerg. Technol. 2020, 2, 314–324. [Google Scholar] [CrossRef]
- Baker, D.P.; Amodeo, A.M.; Krokos, K.J.; Slonim, A.; Herrera, H. Assessing teamwork attitudes in healthcare: Development of the Team STEPPS teamwork attitudes questionnaire. Qual. Saf. Health Care 2010, 19, 49. [Google Scholar] [CrossRef]
- Park, S.; Yang, N.Y.; Choi, J.S. Factors affecting attitudes and preventive practice of pressure ulcer among nurses. J. Muscle Joint Health 2013, 20, 43–51. [Google Scholar] [CrossRef][Green Version]
- Simonetti, V.; Comparcini, D.; Flacco, M.E.; Di Giovanni, P.; Cicolini, G. Nursing students’ knowledge and attitude on pressure ulcer prevention evidence-based guidelines: A multicenter cross-sectional study. Nurse Educ. Today 2015, 35, 573–579. [Google Scholar] [CrossRef]
- Kim, M.S.; Ryu, J.M. Canonical correlation between knowledge-barriers/facilitators for pressure ulcer prevention nursing variables and attitude-performance variables. J. Health Info. Stat. 2019, 44, 227–236. [Google Scholar] [CrossRef]
- Tubaishat, A.; Aljezawi, M.; Al Qadire, M. Nurses’ attitudes and perceived barriers to pressure ulcer prevention in Jordan. J. Wound Care 2013, 22, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Lavallée, J.F.; Gray, T.A.; Dumville, J.; Cullum, N. Barriers and facilitators to preventing pressure ulcers in nursing home residents: A qualitative analysis informed by the Theoretical Domains Framework. Int. J. Nurs. Stud. 2018, 82, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, C.W.; Solomon, J.; Palmer, J.A.; Lukas, C.V. Contextual facilitators of and barriers to nursing home pressure ulcer prevention. Adv. Skin Wound Care 2016, 29, 226–238. [Google Scholar] [CrossRef] [PubMed]
- Moore, Z.; Price, P. Nurses’ attitudes, behaviours and perceived barriers towards pressure ulcer prevention. J. Clin. Nurs. 2004, 13, 942–951. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Park, S.; Kim, J.Y.; Kim, C.G.; Cha, S.K. Clinical nurses’ knowledge and visual differentiation ability in pressure ulcer classification system and incontinence-associated dermatitis. J. Korean Acad. Nurs. 2013, 43, 526–535. [Google Scholar] [CrossRef]
- Earle, A.M.; Napper, L.E.; LaBrie, J.W.; Brooks-Russell, A.; Smith, D.J.; Rutte, J. Examining interactions within the theory of planned behavior in the prediction of intentions to engage in cannabis-related driving behaviors. J. Am. Coll. Health 2020, 68, 374–380. [Google Scholar] [CrossRef]
- Hukkelberg, S.S.; Hagtvet, K.A.; Kovac, V.B. Latent interaction effects in the theory of planned behaviour applied to quitting smoking. Br. J. Health Psychol. 2014, 19, 83–100. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Pearson: Boston, MA, USA, 2007. [Google Scholar]
- Park, I.J.; Kweon, S.S. Performance of preventive actions for hospital falls and factors related to university hospital nurses. Nurs. Health Issues 2018, 23, 19–27. [Google Scholar]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef]
- Seo, K.S. Nurses’ Knowledge, Attitudes, and Preventive Care for Pressure Ulcers in Nursing Homes. Master’s Thesis, Ewha Womans University, Seoul, Korea, 2010. [Google Scholar]
- Reaper, S.; Green, C.; Gupta, S.; Tiruvoipati, R. Inter-rater reliability of the reaper oral mucosa pressure injury scale (ROMPIS): A novel scale for the assessment of the severity of pressure injuries to the mouth and oral mucosa. Aust. Crit. Care 2017, 30, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Neter, J.; Wasserman, W.; Kutner, M.H. Applied Linear Regression Models; CRC Press: Boca Raton, FL, USA, 1989. [Google Scholar]
- Etafa, W.; Argaw, Z.; Gemechu, E.; Melese, B. Nurses’ attitude and perceived barriers to pressure ulcer prevention. BMC Nurs. 2018, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Worsley, P.R.; Clarkson, P.; Bader, D.L.; Schoonhoven, L. Identifying barriers and facilitators to participation in pressure ulcer prevention in allied healthcare professionals: A mixed methods evaluation. Physiotherapy 2017, 103, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Jun, S.S.; Kim, H.J.; Jang, Y.J. Pressure ulcers caused by equipment and supplies in intensive care unit. J. Korean Acad. Soc. Home Health Care Nurs. 2017, 24, 255–263. [Google Scholar]
- Park, J.H.; Son, J.T. Structural analysis of variables related to fall prevention behavior of registered nurses in small-to-medium sized hospitals. J. Korean Acad. Fund. Nurs. 2018, 25, 269–281. [Google Scholar] [CrossRef][Green Version]
- Edsberg, L.E.; Black, J.M.; Goldberg, M.; McNichol, L.; Moore, L.; Sieggreen, M. Revised national pressure ulcer advisory panel pressure injury staging system: Revised pressure injury staging system. J. Wound Ostomy Cont. Nurs. 2016, 43, 585–597. [Google Scholar] [CrossRef]
- Lee, Y.J.; Kim, J.Y. Effects of pressure ulcer classification system education programme on knowledge and visual differential diagnostic ability of pressure ulcer classification and incontinence-associated dermatitis for clinical nurses in Korea. Int. Wound J. 2016, 13, 26–32. [Google Scholar] [CrossRef]
- Junqueira, L.C.; Carneiro, J. Basic Histology: Text and Atlas, 7th ed.; McGraw-Hill: New York, NY, USA, 2005. [Google Scholar]
- Kim, Y.H.; Jang, J.N.; Song, M.J.; Oh, M.K. Effect of integrative pressure ulcers nursing program for the prevention and management of pressure ulcers. J. Korean Data Anal. Soc. 2015, 17, 1015–1029. [Google Scholar]
- Kaddourah, B.; Abu-Shaheen, A.K.; Al-Tannir, M. Knowledge and attitudes of health professionals towards pressure ulcers at a rehabilitation hospital: A cross-sectional study. BMC Nurs. 2016, 15, 17. [Google Scholar] [CrossRef]
- Kim, J.; Lee, J.Y.; Lee, E. Risk factors for newly acquired pressure ulcer and the impact of nurse staffing on pressure ulcer incidence. J. Nurs. Manag. 2019, 00, 1–9. [Google Scholar] [CrossRef]
- Berry, T.R.; Jones, K.E.; McLeod, N.C.; Spence, J.C. The relationship between implicit and explicit believability of exercise-related messages and intentions. Health Psychol. 2011, 30, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, M.; Ajzen, I. Prediction and Change of Behavior: The Reasoned Action Approach; Psychology Press: East Sussex, UK, 2010. [Google Scholar]
- Kim, J.K.; Yoo, S.H.; Nho, J.H.; Ju, J.K. Performance and influencing factors of evidence-based pressure ulcer care among acute care hospital nurses. Worldviews Evid. Based Nurs. 2019, 16, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Dellefield, M.E.; Magnabosco, J.L. Pressure ulcer prevention in nursing homes: Nurse descriptions of individual and organization level factors. Geriatr. Nurs. 2014, 35, 97–104. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Categories | n (%) | Intention to Perform Oral Mucosa Pressure Ulcer (PU) Prevention | |
|---|---|---|---|---|
| M ± SD | t/F (p) | |||
| Gender | Male | 5 (4.5) | 4.20 ± 0.89 | 1.85 (0.068) |
| Female | 107 (95.5) | 3.65 ± 0.65 | ||
| Age (in years) | <30 | 60 (53.6) | 3.65 ± 0.67 | 1.08 (0.362) |
| (M ± SD = 31.16 ± 6.06) | 30∼39 | 40 (35.7) | 3.69 ± 0.66 | |
| 40∼49 | 9 (8.0) | 3.61 ± 0.49 | ||
| 50 ≦ | 3 (2.7) | 4.33 ± 0.58 | ||
| Marital | Married | 25 (22.3) | 3.86 ± 0.55 | 1.59 (0.116) |
| status | Single | 87 (77.7) | 3.63 ± 0.67 | |
| Educational | College | 9 (8.0) | 3.61 ± 0.49 | 0.67 (0.935) |
| level | University | 94 (84.0) | 3.68 ± 0.68 | |
| Master ≦ | 9 (8.0) | 3.72 ± 0.57 | ||
| Working | ICU | 55 (49.1) | 3.82 ± 0.64ⓐ | 3.66 (0.029) |
| department | Medical-surgical ward | 51 (45.5) | 3.50 ± 0.62ⓑ | ⓐ > ⓑ |
| Anesthesiology | 6 (5.4) | 3.83 ± 0.75 | ||
| Total clinical | 1∼5 | 57 (50.9) | 3.60 ± 0.67 | 0.48 (0.753) |
| experience | 6∼10 | 39 (34.8) | 3.73 ± 0.63 | |
| (in years) | 11∼15 | 5 (4.5) | 3.80 ± 0.84 | |
| (M ± SD = 7.11 ± 5.52) | 16∼20 | 5 (4.5) | 3.70 ± 0.67 | |
| 20 ≦ | 6 (5.3) | 3.91 ± 0.66 | ||
| Clinical experience | ≦1 | 33 (29.5) | 3.65 ± 0.63 | 1.02 (0.388) |
| in the current | 2∼4 | 45 (40.2) | 3.62 ± 0.71 | |
| department (in years) | 5∼9 | 23 (20.5) | 3.67 ± 0.56 | |
| (M ± SD = 4.25 ± 4.70) | 10 ≦ | 11 (9.8) | 4.00 ± 0.67 | |
| Number of beds | <500 | 18 (16.1) | 3.69 ± 0.67 | 0.01 (1.000) |
| 500∼<1000 | 46 (41.1) | 3.68 ± 0.73 | ||
| 1000∼<1500 | 33 (29.4) | 3.67 ± 0.52 | ||
| 1500 ≦ | 15 (13.4) | 3.67 ± 0.70 | ||
| Variables | M ± SD | Actual Range | Potential Range |
|---|---|---|---|
| Intention to perform oral mucosa PU prevention | 3.68 ± 0.65 | 2.00–5.00 | 1.00–5.00 |
| Attitude toward oral mucosa PU prevention | 3.74 ± 0.39 | 2.90–4.70 | 1.00–5.00 |
| Barriers of oral mucosa PU prevention | 5.65 ± 1.66 | 0.57–9.43 | 0.00–10.00 |
| Facilitators of oral mucosa PU prevention | 5.35 ± 1.34 | 1.50–10.00 | 0.00–10.00 |
| Visual differentiation ability for oral mucosa PU | 0.13 ± 0.13 | 0.00–0.64 | 0.00–1.00 |
| Category | Items | M ± SD |
|---|---|---|
| Barriers | My knowledge for of oral mucosa PU prevention is insufficient | 5.42 ± 2.15 |
| My competence in oral mucosa PUs prevention is insufficient | 4.72 ± 2.07 | |
| There is not enough time to perform oral mucosa PU prevention | 5.68 ± 2.21 | |
| There is insufficient expert provision for preventing oral mucosa PUs | 6.49 ± 2.27 | |
| Priority given to preventing oral mucosa PUs is low | 5.49 ± 2.06 | |
| There are insufficient resources or tools to provide oral mucosa PU prevention | 5.87 ± 2.18 | |
| There are insufficient current record forms for oral mucosa PU risk factors or nursing interventions | 5.85 ± 2.21 | |
| Facilitators | Education opportunities for oral mucosa PU prevention are sufficient | 3.88 ± 1.87 |
| There is sufficient communication among staff about oral mucosa PU prevention performance | 4.48 ± 1.97 | |
| Preventing oral mucosa PUs can also prevent most PUs | 6.41 ± 1.74 | |
| The role of nurses in preventing oral mucosa PUs is clear | 5.71 ± 1.88 | |
| The organization is collaborative in performing oral mucosa PU prevention | 5.67 ± 1.88 | |
| My manager supports the implementation of oral mucosa PU prevention | 5.93 ± 1.88 |
| Variables | 1 r (p) | 2 r (p) | 3 r (p) | 4 r (p) |
|---|---|---|---|---|
| 1. Intention to perform oral mucosa PU prevention | 1 | |||
| 2. Attitude toward oral mucosa PU prevention | 0.38(<0.001) | 1 | ||
| 3. Barriers of oral mucosa PU prevention | −0.33(<0.001) | −0.36(<0.001) | 1 | |
| 4. Facilitators of oral mucosa PU prevention | 0.43(<0.001) | 0.39(<0.001) | −0.47(<0.001) | 1 |
| 5. Visual differentiation ability for oral mucosa PU | −0.10(0.273) | −0.02(0.828) | 0.10(0.308) | −0.17(0.079) |
| Variables | B | SE | β | t | p | Tolerance | VIF |
|---|---|---|---|---|---|---|---|
| Attitude toward oral mucosa PU prevention (Attitude) | 0.77 | 0.32 | 0.23 | 2.43 | 0.017 | 0.78 | 1.29 |
| Barriers of oral mucosa PU prevention (Barriers) | −0.08 | 0.08 | −0.10 | −0.99 | 0.326 | 0.68 | 1.47 |
| Facilitators of oral mucosa PU prevention (Facilitators) | 0.32 | 0.10 | 0.33 | 3.12 | 0.002 | 0.64 | 1.57 |
| Attitude*Barriers | 0.17 | 0.21 | 0.11 | 0.80 | 0.425 | 0.35 | 2.83 |
| Attitude*Facilitators | −0.07 | 0.06 | −0.19 | −1.09 | 0.277 | 0.23 | 4.27 |
| Barriers*Facilitators | −0.24 | 0.27 | −0.15 | −0.15 | 0.367 | 0.25 | 3.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.K.; Kim, M.S. Effects of Attitude, Barriers/Facilitators, and Visual Differentiation on Oral Mucosa Pressure Ulcer Prevention Performance Intention. Healthcare 2021, 9, 76. https://doi.org/10.3390/healthcare9010076
Kang MK, Kim MS. Effects of Attitude, Barriers/Facilitators, and Visual Differentiation on Oral Mucosa Pressure Ulcer Prevention Performance Intention. Healthcare. 2021; 9(1):76. https://doi.org/10.3390/healthcare9010076
Chicago/Turabian StyleKang, Min Kyeong, and Myoung Soo Kim. 2021. "Effects of Attitude, Barriers/Facilitators, and Visual Differentiation on Oral Mucosa Pressure Ulcer Prevention Performance Intention" Healthcare 9, no. 1: 76. https://doi.org/10.3390/healthcare9010076
APA StyleKang, M. K., & Kim, M. S. (2021). Effects of Attitude, Barriers/Facilitators, and Visual Differentiation on Oral Mucosa Pressure Ulcer Prevention Performance Intention. Healthcare, 9(1), 76. https://doi.org/10.3390/healthcare9010076