Social and Demographic Factors Associated with Postnatal Depression Symptoms among HIV-Positive Women in Primary Healthcare Facilities, South Africa



Abstract
1. Introduction
2. Research Methods and Design
2.1. Study Design
2.2. Study Setting
2.3. Study Population and Sampling Strategy
2.4. Data Collection
2.5. Ethical Considerations
2.6. Data Analysis
3. Results
3.1. Description of the Sample
3.2. HIV-Related Information
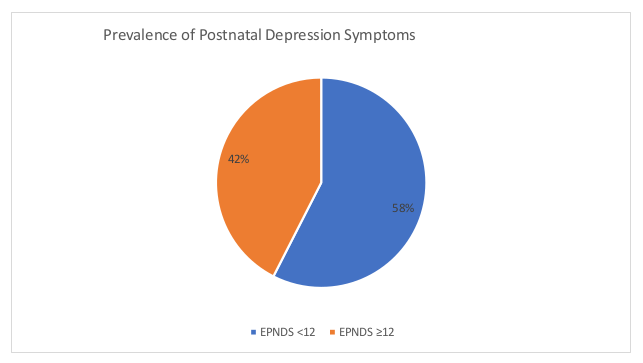
3.3. Prevalence of PND
3.4. Bivariate Analysis of Sociodemographic and Social Factors Associated with PND
3.5. Logistic Regression Analysis of the Factors Associated with PND
4. Discussion
5. Conclusions
Limitations
6. Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Essential Nutrition Actions Improving Maternal, Newborn, Infant and Young Child Health and Nutrition; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- UNAIDS. Global AIDS Update 2019; UNAIDS: Geneva, Switzerland, 2017. [Google Scholar]
- Kapetanovic, S.; Dass-Brailsford, P.; Nora, D.; Talisman, N. Mental health of HIV-seropositive women during pregnancy and postpartum period: A comprehensive literature review. AIDS Behav. 2014, 18, 1152–1173. [Google Scholar] [CrossRef] [PubMed]
- Kathree, T.; Selohilwe, O.M.; Bhana, A.; Petersen, I. Perceptions of postnatal depression and health care needs in a South African sample: The “mental” in maternal health care. BMC Women’s Health 2014, 14, 140. [Google Scholar] [CrossRef] [PubMed]
- Norhayati, M.; Hazlina, N.N.; Asrenee, A.; Emilin, W.W. Magnitude and risk factors for postpartum symptoms: A literature review. J. Affect. Disord. 2015, 175, 34–52. [Google Scholar] [CrossRef]
- Peltzer, K.; Shikwane, M. Prevalence of postnatal depression and associated factors among HIV-positive women in primary care in Nkangala district, South Africa. S. Afr. J. HIV Med. 2011, 12, 24–28. [Google Scholar] [CrossRef][Green Version]
- Kaida, A.; Matthews, L.T.; Ashaba, S.; Tsai, A.C.; Kanters, S.; Robak, M.; Psaros, C.; Kabakyenga, J.; Boum, Y.; Haberer, J.E.; et al. Depression during pregnancy and the postpartum among HIV-infected women on antiretroviral therapy in Uganda. J. Acquir. Immune Defic. Syndr. (1999) 2014, 67 (Suppl. 4), S179–S187. [Google Scholar] [CrossRef] [PubMed]
- Nesti, E.; Pearson, R.M.; Murray, L.; Cooper, P.; Craske, M.G.; Stein, A. Association of persistent and severe postnatal depression with child outcome. JAMA Psychiatry 2018, 75, 247–253. [Google Scholar]
- Verbeek, T.; Bockting, C.L.; van Pampus, M.G.; Ormel, J.; Meijer, J.L.; Hartman, C.A.; Burger, H. Postpartum depression predicts offspring mental health problems in adolescence independently of parental lifetime psychopathology. J. Affect. Disord. 2012, 136, 948–954. [Google Scholar] [CrossRef]
- Eastwood, J.G.; Jalaludin, B.B.; Kemp, L.A.; Phung, H.N.; Barnett, B.E. Relationship of postnatal depressive symptoms to infant temperament, maternal expectations, social support and other potential risk factors: Findings from a large Australian cross-sectional study. BMC Pregnancy Childbirth 2012, 12, 148. [Google Scholar] [CrossRef]
- Goker, A.; Yanikkerem, E.; Demet, M.M.; Dikayak, S.; Yildirim, Y.; Koyuncu, F.M. Postpartum depression: Is mode of delivery a risk factor? ISRN Obstet. Gynecol. 2012, 2012, 616759. [Google Scholar] [CrossRef]
- Parsons, C.E.; Young, K.S.; Rochat, T.J.; Kringelbach, M.L.; Stein, A. Postnatal depression and its effects on child development: A review of evidence from low-and middle-income countries. Br. Med. Bull. 2012, 101, 57–79. [Google Scholar] [CrossRef]
- Yator, O.; Mathai, M.; Vander Stoep, A.; Rao, D.; Kumar, M. Risk factors for postpartum depression in women living with HIV attending prevention of mother-to-child transmission clinic at Kenyatta National Hospital, Nairobi. AIDS Care 2016, 28, 884–889. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.; Chen, W.T.; Pearson, C.R.; Simoni, J.M.; Fredriksen-Goldsen, K.; Nelson, K.; Zhao, H.; Zhang, F. Social support mediates the relationship between HIV stigma and depression/quality of life among people living with HIV in Beijing, China. Int. J. STD AIDS 2012, 23, 481–484. [Google Scholar] [CrossRef] [PubMed]
- Munodawafa, M.; Mall, S.; Lund, C.; Schneider, M. Process evaluations of task sharing interventions for perinatal depression in low and middle income countries (LMIC): A systematic review and qualitative meta-synthesis. BMC Health Serv. Res. 2018, 18, 205. [Google Scholar] [CrossRef] [PubMed]
- Manikkam, L.; Burns, J.K. Antenatal depression and its risk factors: An urban prevalence study in KwaZulu-Natal. S. Afr. Med. J. 2012, 102, 940–944. [Google Scholar] [CrossRef]
- Katon, W.; Russo, J.; Gavin, A. Predictors of postpartum depression. J. Women’s Health 2014, 23, 753–759. [Google Scholar] [CrossRef]
- Sword, W.; Kurtz Landy, C.; Thabane, L.; Watt, S.; Krueger, P.; Farine, D.; Foster, G. Is mode of delivery associated with postpartum depression at 6 weeks: A prospective cohort study. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 966–977. [Google Scholar] [CrossRef]
- Evans, M.; Donelle, L.; Hume-Loveland, L. Social support and online postpartum depression discussion groups: A content analysis. Patient Educ. Couns. 2012, 87, 405–410. [Google Scholar] [CrossRef]
- Afolabi, O.; Bunce, L.; Lusher, J.; Banbury, S. Postnatal depression, maternal–infant bonding and social support: A cross-cultural comparison of Nigerian and British mothers. J. Ment. Health 2020, 29, 424–430. [Google Scholar] [CrossRef]
- Hartley, M.; Tomlinson, M.; Greco, E.; Comulada, W.S.; Stewart, J.; Le Roux, I.; Mbewu, N.; Rotheram-Borus, M.J. Depressed mood in pregnancy: Prevalence and correlates in two Cape Town peri-urban settlements. Reprod. Health 2011, 8, 9. [Google Scholar] [CrossRef]
- Agostini, F.; Neri, E.; Salvatori, P.; Dellabartola, S.; Bozicevic, L.; Monti, F. Antenatal depressive symptoms associated with specific life events and sources of social support among Italian women. Matern. Child Health J. 2015, 19, 1131–1141. [Google Scholar] [CrossRef]
- Bottino, M.N.; Nadanovsky, P.; Moraes, C.L.; Reichenheim, M.E.; Lobato, G. Reappraising the relationship between maternal age and postpartum depression according to the evolutionary theory: Empirical evidence from a survey in primary health services. J. Affect. Disord. 2012, 142, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, K.; Rodriguez, V.J.; Jones, D. Prevalence of prenatal depression and associated factors among HIV-positive women in primary care in Mpumalanga province, South Africa. SAHARA-J J. Soc. Asp. HIV/AIDS 2016, 13, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, W.; Brittain, K.; Mercer, G.; Peacock, D.; Stinson, K.; Janson, H.; Dubula, V. Improving men’s participation in preventing mother-to-child transmission of HIV as a maternal, neonatal, and child health priority in South Africa. PLoS Med. 2015, 12, e1001811. [Google Scholar]
- Groves, A.K.; Kagee, A.; Maman, S.; Moodley, D.; Rouse, P. Associations between intimate partner violence and emotional distress among pregnant women in Durban, South Africa. J. Interpers. Violence 2012, 27, 1341–1356. [Google Scholar] [CrossRef] [PubMed]
- Groves, A.K.; Moodley, D.; McNaughton-Reyes, L.; Martin, S.L.; Foshee, V.; Maman, S. Prevalence, rates and correlates of intimate partner violence among South African women during pregnancy and the postpartum period. Matern. Child Health J. 2015, 19, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Mokwena, K.; Shiba, D. Prevalence of postnatal depression symptoms in a primary health care clinic in Pretoria, South Africa: Management of health care services. Afr. J. Phys. Health Educ. Recreat. Dance 2014, 20 (Suppl. 1), 116–127. [Google Scholar]
- Bilszta, J.L.; Tang, M.; Meyer, D.; Milgrom, J.; Ericksen, J.; Buist, A.E. Single motherhood versus poor partner relationship: Outcomes for antenatal mental health. Aust. N. Z. J. Psychiatry 2008, 42, 56–65. [Google Scholar] [CrossRef]
- Bernstein, M.; Phillips, T.; Zerbe, A.; McIntyre, J.A.; Brittain, K.; Petro, G.; Abrams, E.J.; Myer, L. Intimate partner violence experienced by HIV-infected pregnant women in South Africa: A cross-sectional study. BMJ Open 2016, 6, e011999. [Google Scholar] [CrossRef]
- Tsai, A.C.; Tomlinson, M. Mental health spillovers and the Millennium Development Goals: The case of perinatal depression in Khayelitsha, South Africa. J. Glob. Health 2012, 2, 010302. [Google Scholar] [CrossRef]
- Vliegen, N.; Casalin, S.; Luyten, P. The course of postpartum depression: A review of longitudinal studies. Harv. Rev. Psychiatry 2014, 22, 1–22. [Google Scholar] [CrossRef]
- Qobadi, M.; Collier, C.; Zhang, L. The effect of stressful life events on postpartum depression: Findings from the 2009–2011 Mississippi pregnancy risk assessment monitoring system. Matern. Child Health J. 2016, 20, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Radoš, S.N.; Tadinac, M.; Herman, R. Validation study of the Croatian version of the Edinburgh Postnatal Depression Scale (EPDS). Suvrem. Psihol. 2013, 16, 203–218. [Google Scholar]
- Hartley, C.M.; Barroso, N.; Rey, Y.; Pettit, J.W.; Bagner, D.M. Factor structure and psychometric properties of English and Spanish versions of the Edinburgh Postnatal Depression Scale among Hispanic women in a primary care setting. J. Clin. Psychol. 2014, 70, 1240–1250. [Google Scholar] [CrossRef] [PubMed]
- Gibson, J.; McKenzie-McHarg, K.; Shakespeare, J.; Price, J.; Gray, R. A systematic review of studies validating the Edinburgh Postnatal Depression Scale in antepartum and postpartum women. Acta Psychiatr. Scand. 2009, 119, 350–364. [Google Scholar] [CrossRef] [PubMed]
- Stewart, R.C.; Umar, E.; Tomenson, B.; Creed, F. Validation of screening tools for antenatal depression in Malawi—A comparison of the Edinburgh Postnatal Depression Scale and Self Reporting Questionnaire. J. Affect. Disord. 2013, 150, 1041–1047. [Google Scholar] [CrossRef]
- Khalifa, D.S.; Glavin, K.; Bjertness, E.; Lien, L. Postnatal depression among Sudanese women: Prevalence and validation of the Edinburgh Postnatal Depression Scale at 3 months postpartum. Int. J. Women’s Health 2015, 7, 677. [Google Scholar] [CrossRef]
- Lawrie, T.; Hofmeyr, G.; De Jager, M.; Berk, M. Validation of the Edinburgh Postnatal Depression Scale on a cohort of South African women. S. Afr. Med. J. 1998, jnb88, 1340–1344. [Google Scholar]
- Usuda, K.; Nishi, D.; Okazaki, E.; Makino, M.; Sano, Y. Optimal cut-off score of the Edinburgh Postnatal Depression Scale for major depressive episode during pregnancy in Japan. Psychiatry Clin. Neurosci. 2017, 71, 836–842. [Google Scholar] [CrossRef]
- Stellenberg, E.L.; Abrahams, J.M. Prevalence of and factors influencing postnatal depression in a rural community in South Africa. Afr. J. Prim. Health Care Fam. Med. 2015, 7, 1–8. [Google Scholar] [CrossRef]
- Scheer, J.R.; Pachankis, J.E.; Bränström, R. Gender-based structural stigma and intimate partner violence across 28 countries: A population-based study of women across sexual orientation, immigration status, and socioeconomic status. J. Interpers. Violence 2020. [Google Scholar] [CrossRef]
- Shamu, S.; Zarowsky, C.; Roelens, K.; Temmerman, M.; Abrahams, N. High-frequency intimate partner violence during pregnancy, postnatal depression and suicidal tendencies in Harare, Zimbabwe. Gen. Hosp. Psychiatry 2016, 38, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Ramrakha, S.; Paul, C.; Bell, M.L.; Dickson, N.; Moffitt, T.E.; Caspi, A. The relationship between multiple sex partners and anxiety, depression, and substance dependence disorders: A cohort study. Arch. Sex. Behav. 2013, 42, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Guintivano, J.; Sullivan, P.F.; Stuebe, A.M.; Penders, T.; Thorp, J.; Rubinow, D.R.; Meltzer-Brody, S. Adverse life events, psychiatric history, and biological predictors of postpartum depression in an ethnically diverse sample of postpartum women. Psychol. Med. 2018, 48, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Meltzer-Brody, S.; Larsen, J.T.; Petersen, L.; Guintivano, J.; Florio, A.D.; Miller, W.C.; Sullivan, P.F.; Munk-Olsen, T. Adverse life events increase risk for postpartum psychiatric episodes: A population-based epidemiologic study. Depress. Anxiety 2018, 35, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Garman, E.C.; Schneider, M.; Lund, C. Perinatal depressive symptoms among low-income South African women at risk of depression: Trajectories and predictors. BMC Pregnancy Childbirth 2019, 19, 202. [Google Scholar] [CrossRef]
- Herba, C.M.; Glover, V.; Ramchandani, P.G.; Rondon, M.B. Maternal depression and mental health in early childhood: An examination of underlying mechanisms in low-income and middle-income countries. Lancet Psychiatry 2016, 3, 983–992. [Google Scholar] [CrossRef]
- Marsay, C.; Manderson, L.; Subramaney, U. Validation of the Whooley questions for antenatal depression and anxiety among low-income women in urban South Africa. S. Afr. J. Psychiatry 2017, 23, 1013. [Google Scholar] [CrossRef]
- January, J.; Burns, J.; Chimbari, M. Primary care screening and risk factors for postnatal depression in Zimbabwe: A scoping review of literature. J. Psychol. Afr. 2017, 27, 294–298. [Google Scholar] [CrossRef]
- Peltzer, K.; Rodriguez, V.J.; Lee, T.K.; Jones, D. Prevalence of prenatal and postpartum depression and associated factors among HIV-infected women in public primary care in rural South Africa: A longitudinal study. AIDS Care 2018, 30, 1372–1379. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Responses | Value n (%) |
|---|---|---|
| Maternal age | <25 years | 119 (30.9) |
| 26–35 years | 219 (56.7) | |
| >35 years | 48 (12.4) | |
| Marital status | Married | 56 (14.5) |
| Single/never married | 330 (85.5) | |
| Place of residence | Rural | 316 (81.9) |
| Urban | 70 (18.1) | |
| Religion | Christianity | 278 (72) |
| African traditional | 98 (25.4) | |
| Other | 10 (2.6) | |
| Education level | Matric | 276 (71.5) |
| No matric | 110(28.5) | |
| Employment | Not employed | 304 (78.8) |
| Employed | 82 (21.2) | |
| Household monthly income | <R 2000 | 122 (66) |
| R 2001–5000 | 40 (21.6) | |
| >R 5000 | 23 (12.4) | |
| Did not indicate | 201 (52.1) | |
| Source of income | Child support grant | 183 (47.4) |
| Partner and family support | 162 (42) | |
| Missing | 41 (10.6) |
| Variables | Responses | N (%) |
|---|---|---|
| In a relationship | Yes | 338 (87.6) |
| No | 48 (12.4) | |
| Living with | Alone | 29 (7.5) |
| Parents/other | 257 (66.6) | |
| Partner | 100 (25.9) | |
| Partner financial support | Yes | 338 (87.6) |
| No | 43 (11.1) | |
| Missing | 5 (1.3) | |
| Have other support | Yes | 348 (90.2) |
| No | 38 (9.8) | |
| Received most support from | Partner | 74 (19.2) |
| Family and friends | 251 (65) | |
| Other | 61 (15.8) | |
| Ever threatened by partner | No | 328 (85) |
| Yes | 39 (10.1) | |
| Missing | 19 (4.9) | |
| Male partner has other sexual partners | Yes | 109 (28.2) |
| No | 227 (58.8) | |
| Do not know | 28 (8) | |
| Missing | 22 (5) | |
| Partner drinks alcohol | Yes | 192 (49.8) |
| No | 173 (44.8) | |
| Missing | 21 (5.4) | |
| At least one adverse life event | Yes | 139 (36) |
| No | 244 (63.2) | |
| Missing | 3 (0.08) |
| Variable | Responses | N (%) |
|---|---|---|
| Period since HIV diagnosis | One year | 135 (35) |
| ≥2 years | 249 (64.5) | |
| Missing | 2 (0.5) | |
| Partner HIV+ | Yes | 188 (48.7) |
| No | 60 (15.5) | |
| Do not know | 125 (32.4) | |
| Missing | 13 (3.4) | |
| Disclosed HIV status to family member | Yes | 308 (79.8) |
| No | 76 (19.7) | |
| Missing | 2 (0.5) | |
| HIV diagnosed during latest pregnancy | Yes | 223 (57.8) |
| No | 158 (40.9) | |
| Missing | 5 (1.3) | |
| Difficulty taking Antiretroviral Therapy (ART) during pregnancy | Yes | 54 (14) |
| No | 301 (78) | |
| Missing | 31 (8%) | |
| Know baby’s HIV status | Yes | 217 (56.2) |
| No/awaiting results | 167 (43.3) | |
| Missing | 2 (0.5) |
| Variables | Response | Not Depressed n = 222 (%) | Depressed n = 164 (%) | p-Value | |
|---|---|---|---|---|---|
| Age | |||||
| <25 years | 67 (30.1) | 52 (31.7) | 0.98 | ||
| 26–35 years | 129 (58.1) | 90 (54.9) | |||
| >35 years | 26 (11.7) | 22 (13.4) | |||
| Marital status | |||||
| Married | 35 (15.8) | 21 (12.8) | 0.42 | ||
| Not married | 187 (84.2) | 143 (87.2) | |||
| Place of residence | |||||
| Rural | 187 (84.2) | 129 (78.7) | 0.16 | ||
| Urban | 35 (15.8) | 35 (21.3) | |||
| Religion | |||||
| Christianity | 152 (68.5) | 126 (76.8) | 0.1 | ||
| Traditional | 65 (29.3) | 33 (20.1) | |||
| Other | 5 (2.6) | 5 (3.1) | |||
| Education level | |||||
| Completed matric | 172 (77.5) | 104 (63.4) | 0.01 | ||
| Did not complete matric | 50 (22.5) | 60 (36.6) | |||
| Employment | |||||
| Unemployed | 174 (78.4) | 130 (79.3) | 0.83 | ||
| Employed | 48 (21.6) | 34 (20.7) | |||
| Monthly income | |||||
| <R 2000 | 100 (73) | 22 (45.8) | 0.01 | ||
| R 2001–5000 | 26 (19) | 14 (29.1) | |||
| >R 5000 | 11 (8) | 12 (25) | |||
| Source of income | |||||
| Child support grant | 114 (57.6) | 69 (47) | 0.05 | ||
| Partner and family support | 84 (42.4) | 78 (53) | |||
| HIV-related information | |||||
| Period since HIV diagnosis | |||||
| 1 year | 75 (33.9) | 60 (36.8) | 0.6 | ||
| ≥2 years | 146 (66.1) | 103 (63.2) | |||
| Partner HIV+ | |||||
| Yes | 106 (48.4) | 82 (53.3) | 0.15 | ||
| No | 42 (19.2) | 18 (11.7) | |||
| Disclosed to family member | |||||
| Yes | 179 (81) | 129 (79.1) | 0.6 | ||
| No | 42 (19) | 34 (20.9) | |||
| HIV diagnosis last pregnancy | |||||
| Yes | 133 (60.7) | 90 (55.6) | 0.31 | ||
| No | 86 (39.3) | 72 (44.4) | |||
| Difficulty taking ART during pregnancy | |||||
| Yes | 28 (13.3) | 26 (17.9) | 0.24 | ||
| No | 182 (86.7) | 119 (82.1) | |||
| Know baby HIV status | |||||
| Yes | 114 (52.5) | 103 (47.5) | 0.05 | ||
| No/awaiting results | 108 (64.7) | 59 (35.3) | |||
| Partner and social support information | |||||
| In a relationship | |||||
| Yes | 202 (91) | 136 (83) | |||
| No | 20 (9) | 28 (17) | 0.01 | ||
| Living with | |||||
| Alone | 20 (9) | 9 (5.5) | 0.30 | ||
| Parents/other | 142 (64) | 115 (70.1) | |||
| Partner | 60 (27) | 40 (40.4) | |||
| Partner financial support | |||||
| Yes | 203 (92.3) | 135 (83.9) | |||
| No | 17 (7.7) | 26 (16.1) | 0.01 | ||
| Other social support | |||||
| Yes | 207 (93.2) | 141 (86) | |||
| No | 15 (6.8) | 23 (14) | 0.01 | ||
| Source of most support | |||||
| Partner | 48 (22.9) | 26 (17.3) | 0.2 | ||
| Family | 135(64.3) | 95 (63.3) | |||
| Friends and other | 27 (12.8) | 29 (19.3) | |||
| Partner threats | |||||
| Never | 205 (95) | 123 (81.5) | 0.01 | ||
| Ever | 11 (5) | 28 (18.5) | |||
| Partner has other sex partners | |||||
| Yes | 160 (74) | 67 (45) | |||
| No | 43 (20) | 66 (44.3) | 0.01 | ||
| Do not know | 13 (6) | 16 (10.7) | |||
| Partner drinks alcohol | |||||
| Yes | 115 (53.7) | 77 (51) | 0.6 | ||
| No | 99 (46.3) | 74 (49) | |||
| Experienced adverse life events | |||||
| Yes | 48 (21.6) | 91 (56.5) | 0.01 | ||
| No | 174 (78.4) | 70 (43.5) | |||
| Variables | p-Value | Odds Ratio | 95% CI |
|---|---|---|---|
| Sociodemographic factors | |||
| Age | 0.8 | 0.9 | 0.22–3.75 |
| Marital status | 0.2 | 1.6 | 0.79–3.16 |
| Place of residence | 0.16 | 1.4 | 0.83–2.52 |
| Religion | 0.07 | 0.7 | 0.40–1.06 |
| Education level | 0.01 | 0.5 | 0.31–0.81 |
| Employment | 0.83 | 0.9 | 0.56–1.59 |
| Monthly income * | 0.05 | 2.8 | 0.91–11.68 |
| Income source * | 0.05 | 1.5 | 0.98–2.41 |
| HIV-Related Factors | |||
| Period since HIV diagnosis | 0.56 | 0.9 | 0.59–1.35 |
| Partner’s HIV status | 0.15 | 1.2 | 0.96–1.86 |
| Family knows HIV status | 0.7 | 1.1 | 0.65–1.92 |
| HIV diagnosis when pregnant | 0.31 | 0.8 | 0.52–1.25 |
| Experienced difficulty taking ART | 0.24 | 1.4 | 0.75–2.64 |
| Social Support Factors | |||
| Living with whom | 0.14 | 1.7 | 0.71–4.37 |
| Partner support * | 0.01 | 2.9 | 1.14–4.69 |
| Other support * | 0.01 | 2.3 | 1.08–4.80 |
| Most support | 0.2 | 1.4 | 0.80–2.51 |
| Have partner now * | 0.02 | 2.1 | 1.08–4.06 |
| Other sexual partners * | 0.01 | 3.5 | 2.19–5.59 |
| Ever threatened by partner * | 0.01 | 4.2 | 1.96–9.76 |
| Partner drinks | 0.61 | 0.9 | 0.58–1.39 |
| Experienced adverse life events * | 0.01 | 4.7 | 2.94–7.55 |
| PND Symptoms | Odds Ratio | p-Value | 95% Conf. Interval |
|---|---|---|---|
| Partner has other sexual partners | 4.81 | 0.007 | 1.55–14.97 |
| Adverse life event | 4.36 | 0.007 | 1.50–12.72 |
| HIV diagnosis (pregnant) | 0.26 | 0.013 | 0.09–0.75 |
| Level of education | 0.90 | 0.582 | 0.63–1.30 |
| Income | 2.25 | 0.015 | 1.17–4.35 |
| Source of income | 2.81 | 0.023 | 1.15–6.88 |
| Know baby HIV status | 0.47 | 0.065 | 0.21–1.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mokwena, K.E.; Mbatha, N.L. Social and Demographic Factors Associated with Postnatal Depression Symptoms among HIV-Positive Women in Primary Healthcare Facilities, South Africa. Healthcare 2021, 9, 65. https://doi.org/10.3390/healthcare9010065
Mokwena KE, Mbatha NL. Social and Demographic Factors Associated with Postnatal Depression Symptoms among HIV-Positive Women in Primary Healthcare Facilities, South Africa. Healthcare. 2021; 9(1):65. https://doi.org/10.3390/healthcare9010065
Chicago/Turabian StyleMokwena, Kebogile Elizabeth, and Nontokozo Lilian Mbatha. 2021. "Social and Demographic Factors Associated with Postnatal Depression Symptoms among HIV-Positive Women in Primary Healthcare Facilities, South Africa" Healthcare 9, no. 1: 65. https://doi.org/10.3390/healthcare9010065
APA StyleMokwena, K. E., & Mbatha, N. L. (2021). Social and Demographic Factors Associated with Postnatal Depression Symptoms among HIV-Positive Women in Primary Healthcare Facilities, South Africa. Healthcare, 9(1), 65. https://doi.org/10.3390/healthcare9010065