Development and Validation of a Chinese Version of a Professional Identity Scale for Healthcare Students and Professionals



Abstract
1. Introduction
2. Methodology
2.1. Procedure and Participants
2.2. Statistical Analysis
3. Results
3.1. Participants’ Demographic Characteristics
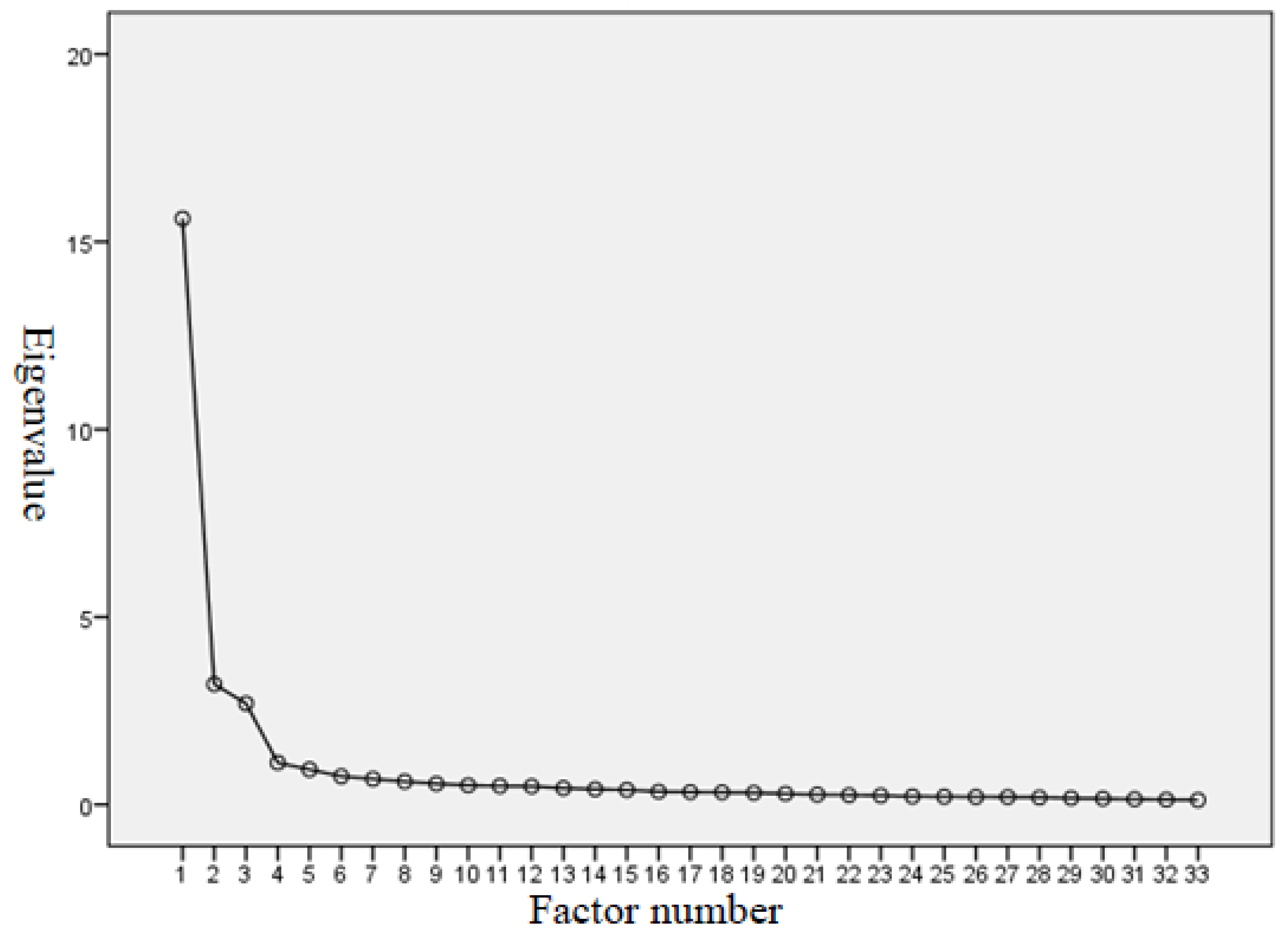
3.2. Exploratory Factor Analysis (EFA)
3.2.1. KMO Test and Bartlett’s Test of Sphericity
3.2.2. EFA Model for the PIS-HSP Scale
3.2.3. Reliability of the EFA Model for the PIS-HSP Scale
3.2.4. Descriptive Item Statistics and Standard Deviations of the EFA Model for the PIS-HSP Scale
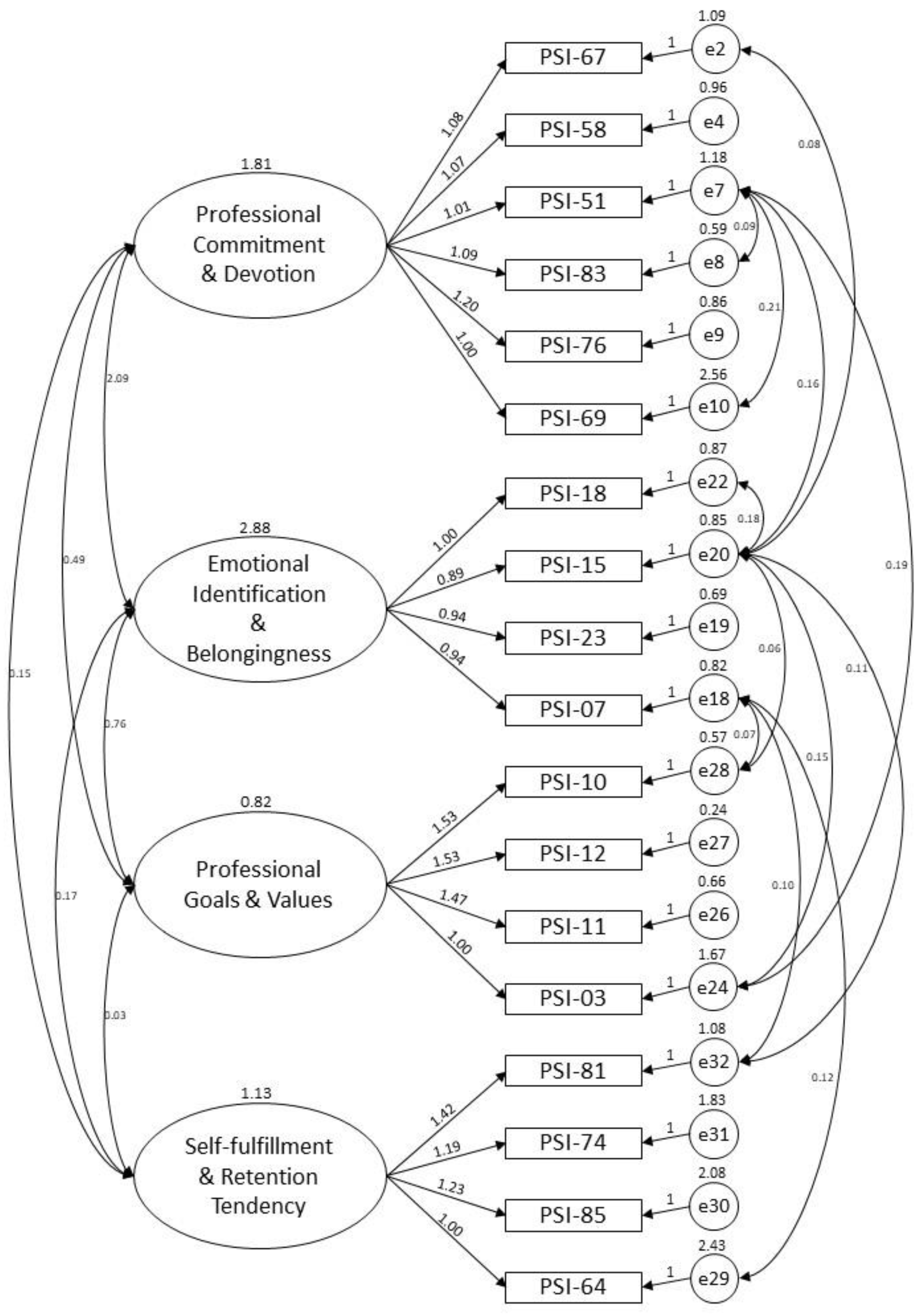
3.3. Confirmatory Factor Analysis (CFA)
3.3.1. Goodness of Fit of the CFA Model for the PIS-HSP Scale
3.3.2. Reliability
3.3.3. Convergent Validity
3.3.4. Discriminant Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. The Factors and Items of CFA Model for the PIS-HSP Scale
- 67. Even if I am married, I (will) remain in healthcare work.
- 58. I would regret it if I have to leave healthcare work.
- 51. No matter how many setbacks I may receive in healthcare work, I will never give it up.
- 83. I like my healthcare specialties and am actively preparing myself for the profession.
- 76. My personal goals are highly relevant to my healthcare work.
- 69. I often read journals and books related to healthcare work to enrich my professional knowledge.
- 18. I am proud of being a healthcare professional.
- 15. It is important for me to devote myself to healthcare work.
- 23. I have a strong interest in healthcare and always enjoy working in this field.
- 7. I am happy with choosing healthcare as my profession.
- 10. I think that healthcare is a professional job.
- 12. I agree with the value of healthcare work.
- 11. I think that healthcare is a respected profession.
- 3. I believe that healthcare is a profession that can bring certain contributions to the country and society.
- 81. I often want to change my current job. (-)
- 74. If I have the chance to choose, under the same working conditions, I will choose a job that is not related to healthcare. (-)
- 85. I have a negative perception of self-worth in response to the current healthcare situation. (-)
- 64. Healthcare is only one of the many jobs I can do; I cannot put my whole heart into it. (-)
References
- Gee, J.P. Identity as an analytic lens for research in education. Rev. Res. Educ. 2001, 25, 99–125. [Google Scholar] [CrossRef]
- Tajfel, H. Human Groups and Social Categories: Studies in Social Psychology; CUP Archive: Cambridge, UK, 1981. [Google Scholar]
- Fagermoen, M.S. Professional identity: Values embedded in meaningful nursing practice. J. Adv. Nurs. 1997, 25, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Ibarra, H. Provisional selves: Experimenting with image and identity in professional adaptation. Adm. Sci. Q. 1999, 44, 764. [Google Scholar] [CrossRef]
- Adams, K.; Hean, S.; Sturgis, P.; Clark, J.M. Investigating the factors influencing professional identity of first-year health and social care students. Learn. Health Soc. Care 2006, 5, 55–68. [Google Scholar] [CrossRef]
- Reisetter, M.; Korcuska, J.S.; Yexley, M.; Bonds, D.; Nikels, H.; McHenry, W. Counselor educators and qualitative research: Affirming a research identity. Couns. Educ. Superv. 2004, 44, 2–16. [Google Scholar] [CrossRef]
- Crossley, J.; Vivekananda-Schmidt, P. The development and evaluation of a Professional Self Identity Questionnaire to measure evolving professional self-identity in health and social care students. Med. Teach. 2009, 31, e603–e607. [Google Scholar] [CrossRef]
- Van Dick, R.; Haslam, S.A. Stress and well-being in the workplace: Support for key propositions from the social identity approach. In The Social Cure: Identity, Health and Well-being; Jetten, J., Haslam, C., Haslam, S.A., Eds.; Psychology Press: New York, NY, USA, 2012; pp. 175–194. [Google Scholar]
- Crocetti, E.; Rubini, M.; Meeus, W. Capturing the dynamics of identity formation in various ethnic groups: Development and validation of a three-dimensional model. J. Adolesc. 2008, 31, 207–222. [Google Scholar] [CrossRef]
- Ashmore, R.D.; Deaux, K.; McLaughlin-Volpe, T. An Organizing framework for collective identity: Articulation and significance of multidimensionality. Psychol. Bull. 2004, 130, 80–114. [Google Scholar] [CrossRef]
- Kroger, J.; Marcia, J.E. The Identity Statuses: Origins, Meanings, and Interpretations. In Handbook of Identity Theory and Research; Springer Science and Business Media LLC: New York, NY, USA, 2011; pp. 31–53. [Google Scholar]
- Schwartz, S.J.; Luyckx, K.; Vignoles, V.L. Handbook of Identity Theory and Research; Springer: New York, NY, USA, 2011. [Google Scholar]
- Stringer, K.J.; Kerpelman, J.L. Career Identity Development in College Students: Decision Making, Parental Support, and Work Experience. Identity 2010, 10, 181–200. [Google Scholar] [CrossRef]
- Lingard, L.; Reznick, R.; DeVito, I.; Espin, S. Forming professional identities on the health care team: Discursive constructions of the ‘other’ in the operating room. Med. Educ. 2002, 36, 728–734. [Google Scholar] [CrossRef]
- Korkmaz, H.; Şenol, Y. Exploring first grade medical students’ professional identity using metaphors: Implications for medical curricula. Med. Educ. Online 2014, 19, 7. [Google Scholar] [CrossRef] [PubMed]
- Jahanbin, I.; Badiyepeyma, Z.; Ghodsbin, F.; Sharif, F.; Keshavarzi, S. The impact of teaching professional self-concept on clinical performance perception in nursing students. Life Sci. 2012, 9, 653–659. [Google Scholar] [CrossRef]
- Wade, G.H. Professional nurse autonomy: Concept analysis and application to nursing education. J. Adv. Nurs. 1999, 30, 310–318. [Google Scholar] [CrossRef]
- Thorne, M.L. Colonizing the new world of NHS management: The shifting power of professionals. Health Serv. Manag. Res. 2002, 15, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, A.; Devlin, A. Struggling to maintain professional identities when engaging in inter-professional teamwork to deliver integrated care. Int. J. Integr. Care 2017, 17, 76. [Google Scholar] [CrossRef]
- Divall, M.V.; Kolbig, L.; Carney, M.; Kirwin, J.; Letzeiser, C.; Mohammed, S. Interprofessional socialization as a way to introduce collaborative competencies to first-year health science students. J. Interprof. Care 2014, 28, 576–578. [Google Scholar] [CrossRef] [PubMed]
- Khalili, H.; Orchard, C.; Laschinger, H.K.S.; Farah, R. An interprofessional socialization framework for developing an interprofessional identity among health professions students. J. Interprof. Care 2013, 27, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Hutz, C.S.; Bandeira, D.R. Psicometria; Trentini, C.M., Ed.; Artmed: Porto Alegre, Brazil, 2015. [Google Scholar]
- Arias, M.R.M.; Lloreda, M.J.H.; Lloreda, M.V.H. Psicometría; Alianza Editorial: Madrid, Spain, 2014. [Google Scholar]
- Uzunboylu, H.; Ozdamli, F. Teacher perception for m-learning: Scale development and teachers’ perceptions. J. Comput. Assist. Learn. 2011, 27, 544–556. [Google Scholar] [CrossRef]
- World Medical Association World Medical Association Declaration of Helsinki. JAMA 2013, 310, 2191–2194. [CrossRef]
- DeVellis, R.F. Scale Development: Theory and Applications, 3rd ed; Sage publications: California, CA, USA, 2012. [Google Scholar]
- Kaiser, H.F. A second generation little jiffy. Psychometrika 1970, 35, 401–415. [Google Scholar] [CrossRef]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Forina, M.; Armanino, C.; Lanteri, S.; Leardi, R. Methods of varimax rotation in factor analysis with applications in clinical and food chemistry. J. Chemom. 2005, 3, 115–125. [Google Scholar] [CrossRef]
- Churchill, G.A., Jr. A paradigm for developing better measures of marketing constructs. J. Mark. Res. 1979, 16, 64–73. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modeling With AMOS, EQS, and LISREL: Comparative Approaches to Testing for the Factorial Validity of a Measuring Instrument. Int. J. Test. 2001, 1, 55–86. [Google Scholar] [CrossRef]
- Ma, Z. Application of structural equation modeling to evaluate customer satisfaction in the China internet bank sector. In Proceedings of the International Conference on Instrumentation, Measurement, Circuits and Systems (ICIMCS 2011), Hong Kong, China, 12–13 December 2011; ASME International, 2011; pp. 975–978. [Google Scholar]
- Tucker, L.R.; Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika 1973, 38, 1–10. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Hair, J.; Black, W.; Babin, B.; Anderson, R. Multivariate data analysis, 7th ed.; Prentice-Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Malhotra, N.K. Pesquisa de Marketing: Uma Orientação Aplicada, 6th ed.; Bookman: São Paulo, Brazil, 2011. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39. [Google Scholar] [CrossRef]
- Houston, W. The analysis of errors in orthodontic measurements. Am. J. Orthod. 1983, 83, 382–390. [Google Scholar] [CrossRef]
- Cunha, C.M.; Almeida Neto, O.P.; Stackfleth, R. Main psychometric evaluation methods of measuring instruments reliability. Rev. Atenção Saúde 2016, 14, 98–103. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Categories | Number | Percentage | |
|---|---|---|---|---|
| Gender | Male | 170 | 33.40% | |
| Female | 339 | 66.60% | ||
| Source | Healthcare professionals | 133 | 26.13% | |
| Students | College of Medicine | 129 | 25.34% | |
| College of Medical Science and Technology | 182 | 35.76% | ||
| College of Health Care and Management | 65 | 12.77% | ||
| Age | 19 + to 22 years old | 320 | 62.87% | |
| 22 + to 30 years old | 111 | 21.81% | ||
| 30 + years old | 78 | 15.32% | ||
| Educational background | High school | 34 | 6.68% | |
| University | 367 | 72.10% | ||
| Graduated school | 108 | 21.22% | ||
| Ever married | No | 389 | 76.42% | |
| Yes | 120 | 23.58% | ||
| Item | Factor 1: Professional Commitment & Devotion | Factor 2: Emotional Identification & Belongingness | Factor 3: Professional Goals & Values | Factor 4: Self-Fulfillment & Retention Tendency |
|---|---|---|---|---|
| Factor 1: α = 0.96 | ||||
| 66 | 0.82 | |||
| 67 | 0.76 | |||
| 84 | 0.75 | |||
| 58 | 0.73 | |||
| 61 | 0.72 | |||
| 63 | 0.71 | |||
| 51 | 0.70 | |||
| 83 | 0.70 | |||
| 76 | 0.68 | |||
| 69 | 0.68 | |||
| 43 | 0.67 | |||
| 48 | 0.66 | |||
| 79 | 0.65 | |||
| 37 | 0.64 | |||
| 50 | 0.61 | |||
| 33 | 0.61 | |||
| Factor 2: α = 0.96 | ||||
| 16 | 0.79 | |||
| 18 | 0.75 | |||
| 14 | 0.74 | |||
| 15 | 0.73 | |||
| 23 | 0.67 | |||
| 7. | 0.64 | |||
| 21 | 0.64 | |||
| Factor 3: α = 0.88 | ||||
| 10 | 0.89 | |||
| 12 | 0.89 | |||
| 11 | 0.84 | |||
| 19 | 0.68 | |||
| 3 | 0.65 | |||
| Factor 4: α = 0.84 | ||||
| 73 | 0.88 | |||
| 81 | 0.83 | |||
| 74 | 0.78 | |||
| 85 | 0.78 | |||
| 64 | 0.64 | |||
| Eigen value | 15.62 | 3.21 | 2.70 | 1.12 |
| % of variance | 47.33 | 9.72 | 8.17 | 3.38 |
| Item | Mean | S.D. |
|---|---|---|
| Factor 1: Professional Commitment & Devotion | 87.40 | 23.11 |
| 66. Even if the salary is not satisfactory, I (will) remain in healthcare work. | 4.78 | 1.79 |
| 67. Even if I am married, I (will) remain in healthcare work. | 5.46 | 1.80 |
| 84. I like healthcare work. Even if there are other job opportunities with higher pay, I will not consider them. | 5.00 | 1.97 |
| 58. I would regret it if I have to leave healthcare work. | 5.41 | 1.75 |
| 61. If I could choose my career again, I would still choose to work in healthcare. | 5.49 | 1.87 |
| 63. I (will) devote all my time to healthcare work, even if I have to sacrifice time with my family. | 4.26 | 2.09 |
| 51. No matter how many setbacks I may receive in healthcare work, I will never give it up. | 5.53 | 1.75 |
| 83. I like my healthcare specialties and am actively preparing myself for the profession. | 5.69 | 1.66 |
| 76. My personal goals are highly relevant to my healthcare work. | 5.62 | 1.86 |
| 69. I often read journals and books related to healthcare work to enrich my professional knowledge. | 5.65 | 2.09 |
| 43. I often think of my healthcare work that I am responsible for right now, as well as the work that I have not yet finished and completed. | 5.46 | 1.83 |
| 48. My personality and personal beliefs are consistent with the characteristics and values of healthcare work. | 5.65 | 1.77 |
| 79. I think healthcare work itself is challenging and stimulating. | 6.10 | 1.72 |
| 37. I am always thinking about how to do better in healthcare. | 5.68 | 1.70 |
| 50. I believe I can succeed in a healthcare career. | 5.87 | 1.78 |
| 33. Engaging in healthcare work gives me psychological satisfaction. | 5.74 | 1.85 |
| Factor 2: Emotional Identification & Belongingness | 40.54 | 11.58 |
| 16. For me, healthcare is the best career that I can do. | 5.49 | 1.95 |
| 18. I am proud of being a healthcare professional. | 5.74 | 1.94 |
| 14. Even if there are job opportunities other than healthcare, I (will) persist in being a healthcare professional. | 5.52 | 1.93 |
| 15. It is important for me to devote myself to healthcare work. | 5.91 | 1.79 |
| 23. I have a strong interest in healthcare and always enjoy working in this field. | 5.73 | 1.81 |
| 7. I am happy with choosing healthcare as my profession. | 6.17 | 1.83 |
| 21. I feel that I am a member of the healthcare profession. | 5.98 | 1.79 |
| Factor 3: Professional Goals & Values | 35.97 | 6.53 |
| 10. I think that healthcare is a professional job. | 7.43 | 1.58 |
| 12. I agree with the value of healthcare work. | 7.39 | 1.46 |
| 11. I think that healthcare is a respected profession. | 7.30 | 1.56 |
| 19. I am sure that the healthcare workers are interested in helping people. | 6.94 | 1.72 |
| 3. I believe that healthcare is a profession that can bring certain contributions to the country and society. | 6.91 | 1.58 |
| Factor 4: Self-Fulfillment & Retention Tendency | 24.92 | 7.41 |
| 73. I regret choosing healthcare as my career. (-) | 5.05 | 1.93 |
| 81. I often want to change my current job. (-) | 4.99 | 1.84 |
| 74. If I have the chance to choose, under the same working conditions, I will choose a job that is not related to healthcare. (-) | 4.89 | 1.86 |
| 85. I have a negative perception of self-worth in response to the current healthcare situation. (-) | 5.08 | 1.95 |
| 64. Healthcare is only one of the many jobs I can do; I cannot put my whole heart into it. (-) | 4.91 | 1.88 |
| p | TLI | CFI | RMSEA | ||||
|---|---|---|---|---|---|---|---|
| Baseline EFA Model | 1649.885 | 489 | 3.374 | 0.000 | 0.912 | 0.918 | 0.068 |
| CFA Model | 133.157 | 117 | 1.138 | 0.146 | 0.997 | 0.997 | 0.016 |
| Reliability Factor | Cronbach’s Alpha PIS-HSP: Baseline EFA Model and Long-Version Scale | Cronbach’s Alpha PIS-HSP: CFA Model and Short-Version Scale | Composite Reliability PIS-HSP: CFA Model and Short-Version Scale |
|---|---|---|---|
| Professional commitment & Devotion | 0.96 | 0.91 | 0.92 |
| Emotional Identification & Belongingness | 0.96 | 0.93 | 0.93 |
| Professional Goals & Values | 0.88 | 0.88 | 0.89 |
| Self-fulfillment & Retention Tendency | 0.84 | 0.78 | 0.78 |
| Overall | 0.95 | 0.89 | 0.97 |
| Factor | AVE | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|
| 1. Professional Commitment & Devotion | 0.651 | 0.806 | |||
| 2. Emotional Identification & Belongingness | 0.760 | 0.832 ** | 0.871 | ||
| 3. Professional Goals & Values | 0.679 | 0.398 ** | 0.477 ** | 0.824 | |
| 4. Self-Fulfillment & Retention Tendency | 0.477 | −0.089 * | −0.092 * | 0.019 | 0.690 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, H.-C.; Wang, Y.-h. Development and Validation of a Chinese Version of a Professional Identity Scale for Healthcare Students and Professionals. Healthcare 2020, 8, 451. https://doi.org/10.3390/healthcare8040451
Liao H-C, Wang Y-h. Development and Validation of a Chinese Version of a Professional Identity Scale for Healthcare Students and Professionals. Healthcare. 2020; 8(4):451. https://doi.org/10.3390/healthcare8040451
Chicago/Turabian StyleLiao, Hung-Chang, and Ya-huei Wang. 2020. "Development and Validation of a Chinese Version of a Professional Identity Scale for Healthcare Students and Professionals" Healthcare 8, no. 4: 451. https://doi.org/10.3390/healthcare8040451
APA StyleLiao, H.-C., & Wang, Y.-h. (2020). Development and Validation of a Chinese Version of a Professional Identity Scale for Healthcare Students and Professionals. Healthcare, 8(4), 451. https://doi.org/10.3390/healthcare8040451