Strategies for the Prevention of the Intra-Hospital Transmission of COVID-19: A Retrospective Cohort Study



Abstract
1. Introduction
2. Methods
3. Results
3.1. Strategies for Preventing Intra-Hospital Spread of COVID-19
3.2. Actual Situation in Our Hospital during the COVID-19 Outbreak
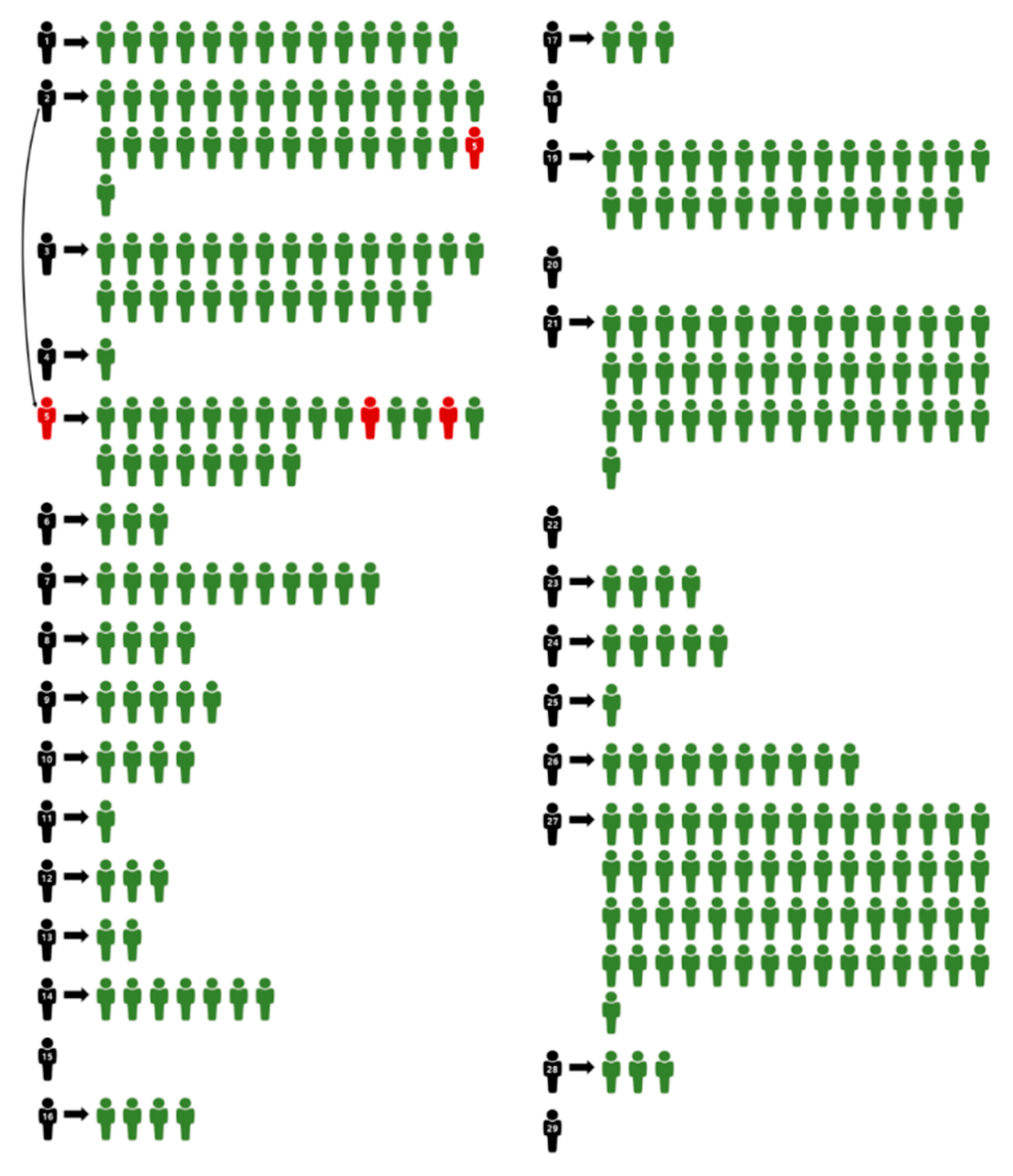
3.3. Transmission Path of COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Chang, M.C.; Park, D. How should rehabilitative departments of hospitals prepare for coronavirus disease 2019? Am. J. Phys. Med. Rehabil. 2020, 99, 475–476. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Park, D. How can blockchain help people in the event of pandemics such as the COVID-19? J. Med. Syst. 2020, 44, 102. [Google Scholar] [CrossRef] [PubMed]
- Korean Society of Infectious Diseases; Korean Society of Pediatric Infectious Diseases; Korean Society of Epidemiology; Korean Society for Antimicrobial Therapy; Korean Society for Healthcare-associated Infection Control and Prevention; Korea Centers for Disease Control and Prevention. Report on the epidemiological features of coronavirus disease 2019 (COVID-19) outbreak in the Republic of Korea from January 19 to March 2, 2020. J. Korean Med. Sci. 2020, 35, e112. [Google Scholar] [CrossRef] [PubMed]
- Park, H.W.; Park, S.; Chong, M. Conversations and medical news frames on Twitter: Infodemiological study on novel coronavirus (COVID-19) in South Korea. J. Med. Internet. Res. 2020, 22, e18897. [Google Scholar] [CrossRef] [PubMed]
- COVID-19. Available online: www.ncov.mohw.go.kr (accessed on 23 April 2020).
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Song, R.; Han, B.; Song, M.; Wang, L.; Conlon, C.P.; Dong, T.; Tian, D.; Zhang, W.; Chen, Z.; Zhang, F.; et al. Clinical and epidemiological features of COVID-19 family clusters in Beijing, China. J. Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cheng, V.C.C.; Wong, S.C.; Chuang, V.W.M.; So, S.Y.C.; Chen, J.H.K.; Sridhar, S.; To, K.K.W.; Chan, J.F.W.; Hung, I.F.N.; Ho, P.L.; et al. The role of community-wide wearing of face mask for control of coronavirus disease 2019 (COVID-19) epidemic due to SARS-CoV-2. J. Infect. 2020, 81, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A.; Grinshpun, S.A.; Reponen, T. Respiratory performance offered by N95 respirators and surgical masks: Human subject evaluation with NaCl aerosol representing bacterial and viral particle size range. Ann. Occup. Hyg. 2008, 52, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Fehr, A.R.; Perlman, S. Coronaviruses: An overview of their replication and pathogenesis. Methods Mol. Biol. 2015, 1282, 1–23. [Google Scholar] [PubMed]
- Eninger, R.M.; Honda, T.; Adhikari, A.; Heinonen-Tanski, H.; Reponen, T.; Grinshpun, S.A. Filter performance of N99 and N95 facepiece respirators against viruses and ultrafine particles. Ann. Occup. Hyg. 2008, 52, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Oberg, T.; Brosseau, L.M. Surgical mask filter and fit performance. Am. J. Infect. Control 2008, 36, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Grinshpun, S.A.; Haruta, H.; Eninger, R.M.; Reponen, T.; McKay, R.T.; Lee, S.A. Performance of an N95 filtering facepiece particulate respirator and a surgical mask during human breathing: Two pathways for particle penetration. J. Occup. Environ. Hyg. 2009, 6, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.B.; Duling, M.G.; Calvert, C.A.; Coffey, C.C. Comparison of performance of three different types of respiratory protection devices. J. Occup. Environ. Hyg. 2006, 3, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
|
|
|
|
|
|
|
|
|
|
|
| A. Rules for inpatient care and nursing: |
| (1) Check whether patients and guardians have fever and/or respiratory symptoms on admission. (2) Do not share manometers, thermometers, and BST devices with other teams. (3) Use separate manometers, thermometers, and BST devices for patients with fever and those in isolation. (4) Monitor for fever and respiratory symptoms and notify the doctor about any such symptoms, if present. (5) Check the travel history of patients as well as whether they are Shincheonji * members or have visited Cheongdo Daenam Hospital *. If yes, then report this to the manager. (6) If there is a high likelihood that a patient has COVID-19 on a ward, then the manager must report this to the COVID-19 Situation Room authority. (7) When patients or guardians notify staff that they were ordered to isolate during the hospitalization period, this must be reported to the COVID-19 Situation Room. (8) Generally, the transfer of a patient to another ward is prohibited. If necessary, follow the rules regarding the transfer of patients to another ward. (9) During the hospitalization period, inpatients are not allowed to go outside. If it is necessary to go outside, then the patient must be readmitted after discharge. |
| B. Care rules for patients and guardians: |
| (1) Patients and guardians must wear a mask. (2) The number of guardians is limited to 1 per patient. (3) Shincheonji members and those who have visited Cheongdo Daenam Hospital * must be removed from the list of approved caregivers. (4) Patients and guardians must limit their movement and not leave the ward, except for undergoing tests. (5) Visitors are not allowed. |
| Criteria | Exposure Risk | Response |
|---|---|---|
| Performing a procedure on a patient with confirmed COVID-19 or staying in the same room during the procedure without wearing personal protective equipment (all 4 kinds *). Procedures: cardiopulmonary resuscitation, intubation, bronchoscopy, nebulizer therapy, and aspiration. | High -Medium | Not allowed to work for 2 weeks after the last exposure |
| Close contact with a patient without wearing personal protective equipment (N95 mask and goggles). This is regardless of whether the patient wore a mask. | Medium | |
| Medical staff who did not wear gloves and came into direct contact with infected excreta/feces without hand hygiene. | Medium | |
| Medical staff who wore a mask →Close contact with patients who wore a mask. | Low | Allowed to work but must self-monitor |
| Medical staff wore personal protective equipment (all 4 kinds *) →Handled or touched excreta/feces. | Low | |
| Medical staff did not wear personal protective equipment (all 4 kinds *) → movement between wards without contact. | Low |
|
1. Transfer of patients with confirmed COVID-19 to another ward: (1) Preparations: a negative air-pressure cart, vinyl. (2) Transfer staff: -The medical staff of the corresponding wards (2 people). -Security team (1 person): securing the elevator control and a patient transport path. (3) Gear of transfer staff: | ||
| Medical staff in the ward | Security team | Infection control team |
| (when required) | ||
| N95 mask, AP gown, gloves, and goggles | N95 mask, AP gown, and gloves | N95 mask, AP gown, and gloves |
| (4) * If the patient has severe symptoms such as coughing, it is recommended that medical staff in the ward should wear level D gowns. | ||
| 2. Transport method: | ||
| (1) Once a room is assigned for the patient to be transferred to, the transfer needs to be arranged with the destination ward when the least patient traffic is expected. (2) Notify the security team (6651) of the respiratory ward on the 1st floor of the transport. (3) The security team goes to the ward with a negative air-pressure cart and a remote control for the elevator. (4) Medical staff in the ward should wear protective equipment (at least an N95 mask, AP gown, gloves, and goggles) and transfer the patient to the negative air-pressure cart. (5) Clean the surface of the negative air-pressure cart with a disinfectant. (6) Once out of the ward, the AP gown and gloves need to be replaced with new ones. (7) The security team secures the transport path for the patient, and the medical staff of the ward moves the cart. (8) After arriving at the destination ward, the patient is handed over in the clean zone. | ||
| 3. Transport path: | ||
| (1) Departments | Moving path | |
| (2) Ward in the Main (3) Building | Elevator No. 2 of the West Building (1st floor in the basement) → Elevator No. 1 of the Respiratory Ward → the corresponding ward | |
| (4) Intensive Care Unit in the Main Building | Elevator No. 2 for the outpatient department in the Main Building (1st floor in the basement) → Elevator No. 1 of the Respiratory Ward → the corresponding ward | |
| (5) Wards 130 and 132 | Patient elevator in the Main Building (1st floor in the basement) → Elevator No. 1 of the Respiratory Ward → the corresponding ward | |
| (6) Regional Emergency Medical center & critical care unit | Elevator No. 2 of the West Building (1st floor in the basement) → Elevator No. 1 of the Respiratory Ward → the corresponding ward | |
| * While the elevator is in use, others are not allowed in. | ||
| 4. Measures after transport: | ||
| (1) Take off the protective equipment used during patient transport in the designated dressing room and return to the ward. | ||
| 5. Quarantine/disinfection: | ||
| (1) After all patients with confirmed COVID-19 have been moved, the general affairs team needs to be contacted for quarantine. (2) After quarantine, the sanitation team cleans the ward. (3) Clean all medical devices used for testing the patient using a disinfectant (medical disinfectant and disinfecting tissues). | ||
| 6. Management of those who came into contact with the confirmed case: | ||
| (1) Investigation period for those who came into contact with the confirmed case: those who came into contact with the confirmed case from the day before the onset of symptoms in the confirmed case: -The investigation can be expanded depending on the movement range of the confirmed case, for example, patients who shared the same space with the confirmed patient. | ||
| (After the investigation of the individuals who were in close contact, the infection control team is informed.) | ||
| 7. Management of the close contacts: | ||
| (1) Movement between wards: Generally, patients should be isolated in a single occupancy room. If no single occupancy room is available, cohort isolation in the isolated ward will be used. (2) Filling in the application form for isolation by a doctor. | ||
| 8. Management of the close contacts (staff): | ||
| (1) Make a list of the close contacts and consider whether they were wearing protective equipment and the contact time, after the infection control team and the nursing headquarters have checked the CCTV recordings. (2) The infection control team decides whether staff needs to self-isolate or self-monitor. | ||
| 9. Rules for preventing contacts. | ||
| (1) Comply with the standards, including wearing a mask and hand hygiene. (2) Those subject to isolation: Xomply with the isolation rule and submit the required paperwork after being informed by the infection control team (isolation notice), monitor symptoms, and undergo a test for COVID-19. (3) Those subject to self-monitoring: Continuously monitor symptoms. Report to the manager or infection control team during symptoms onset. This should be followed by a test or time off work according to the instructions given. | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, M.C.; Hur, J.; Park, D. Strategies for the Prevention of the Intra-Hospital Transmission of COVID-19: A Retrospective Cohort Study. Healthcare 2020, 8, 195. https://doi.org/10.3390/healthcare8030195
Chang MC, Hur J, Park D. Strategies for the Prevention of the Intra-Hospital Transmission of COVID-19: A Retrospective Cohort Study. Healthcare. 2020; 8(3):195. https://doi.org/10.3390/healthcare8030195
Chicago/Turabian StyleChang, Min Cheol, Jian Hur, and Donghwi Park. 2020. "Strategies for the Prevention of the Intra-Hospital Transmission of COVID-19: A Retrospective Cohort Study" Healthcare 8, no. 3: 195. https://doi.org/10.3390/healthcare8030195
APA StyleChang, M. C., Hur, J., & Park, D. (2020). Strategies for the Prevention of the Intra-Hospital Transmission of COVID-19: A Retrospective Cohort Study. Healthcare, 8(3), 195. https://doi.org/10.3390/healthcare8030195