The Monetary Value of Human Lives Lost to Suicide in the African Continent: Beating the African War Drums

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area and Population
2.2. Analytical Framework
“Such a definition (of society) leads to the proposition that the value of a person to others is measured by any excess of his contribution to production over what he consumes from production—this difference being the amount by which everyone else benefits from his productivity. … The present value of a man at any given age may be defined operationally as his discounted expected future earnings stream (net of his consumption if the net concept is used)”(pp. 426–427)
2.3. Data Sources
2.4. Data Analysis
2.5. Ethics Approval
3. Results
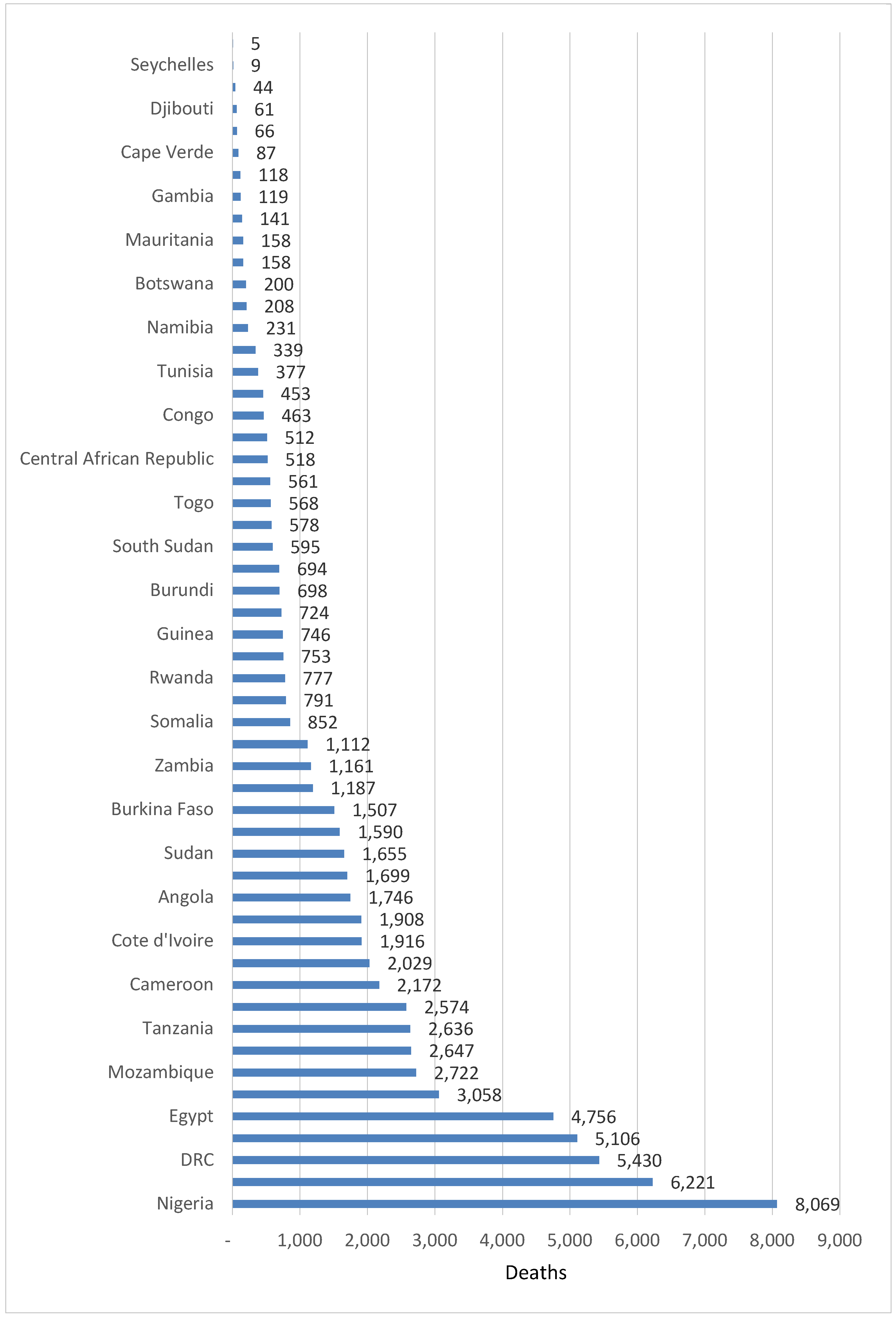
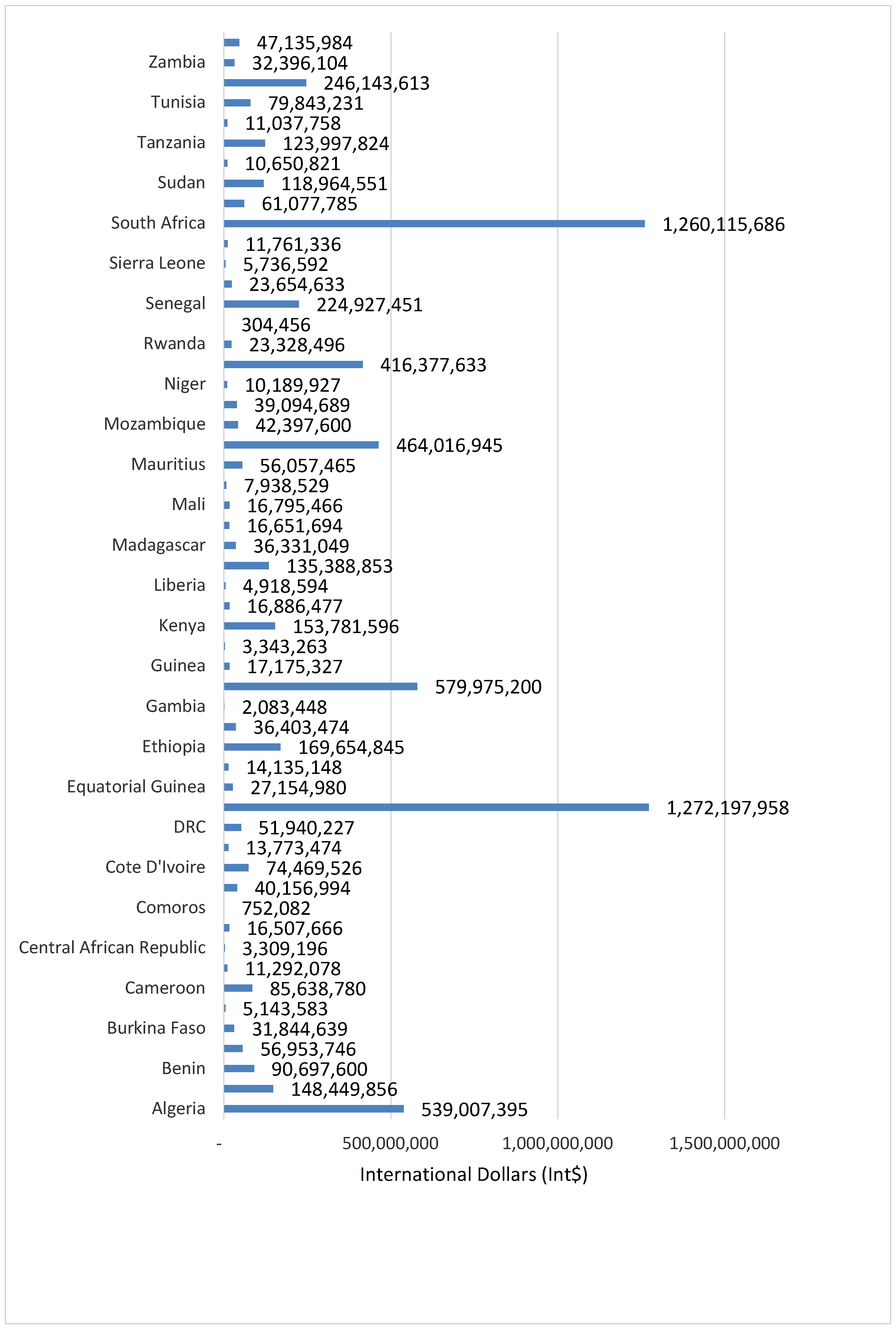
3.1. Value of Human Life Loss Attributable to Suicide
3.2. Money Value of Human Life Lost Among Group 1 Countries
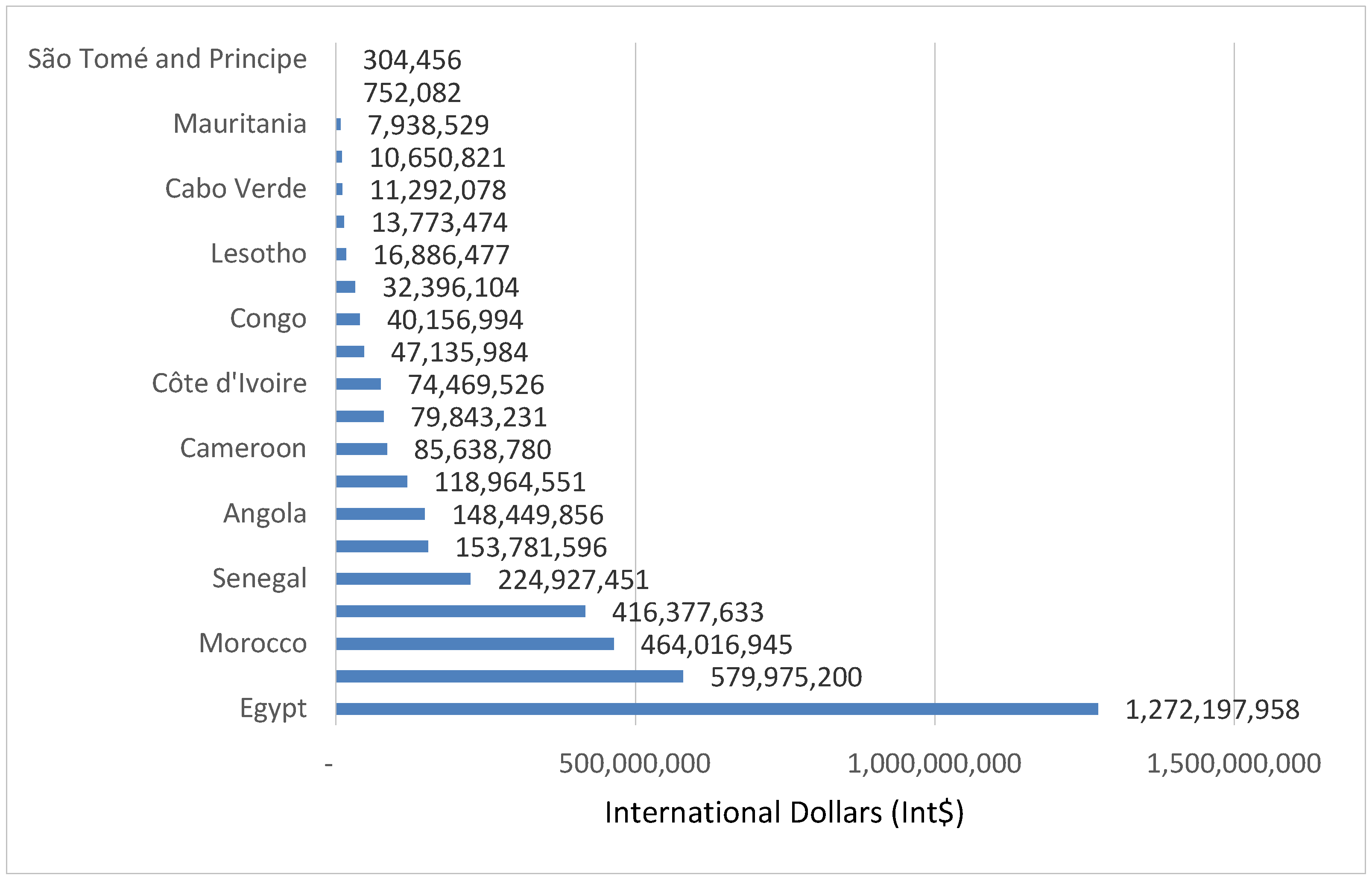
3.3. Money Value of Human Life Lost Among Group 2 Countries
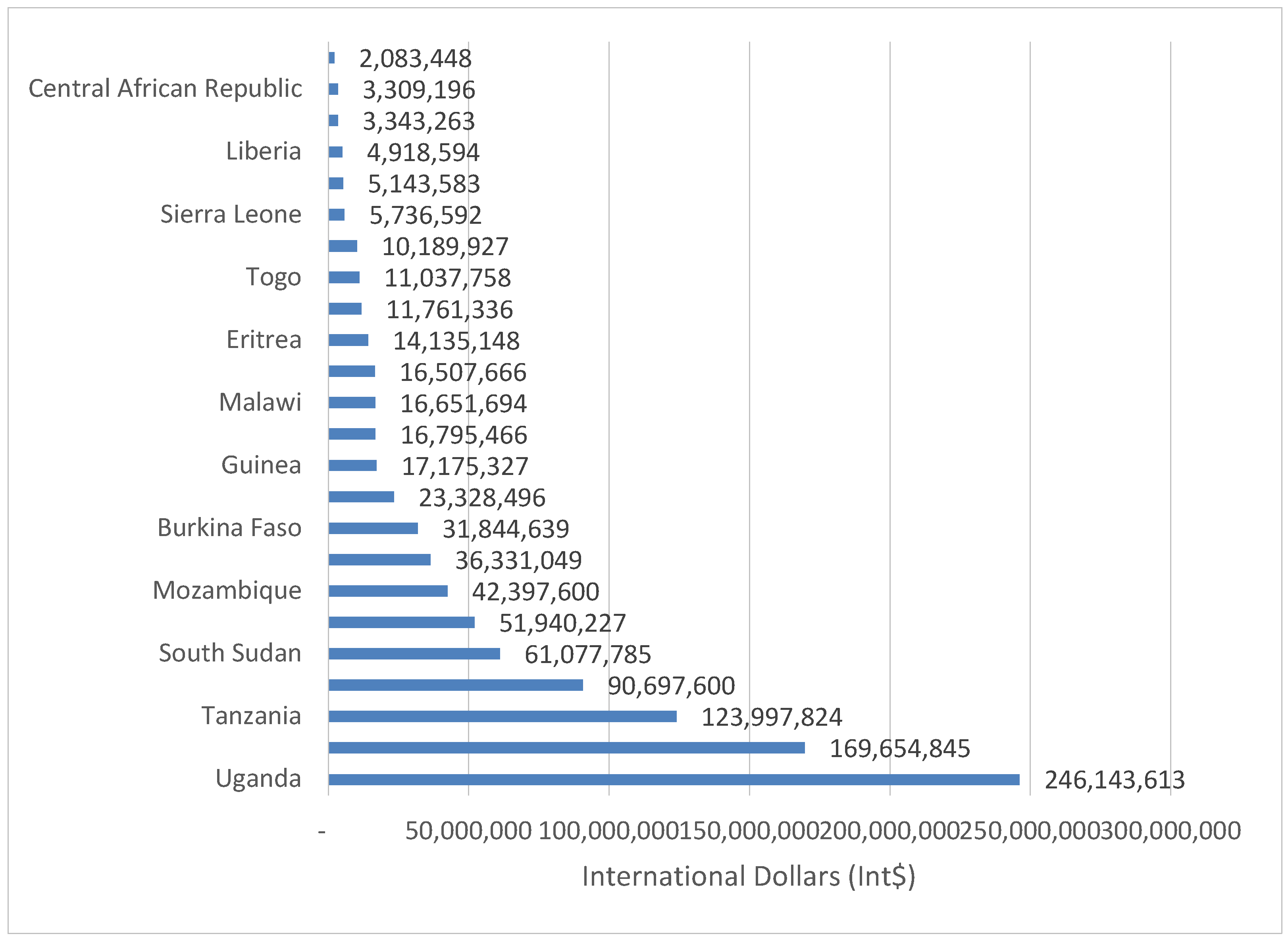
3.4. Money Value of Human Life Lost Among Group 3 Countries
3.5. Average Value of Human Lives
3.6. Sensitivity Analysis Results
4. Discussion
4.1. Potential Use of the Evidence
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Bank. New Country Classifications by Income Level: 2019–2020; World Bank: Washington, DC, USA, 2019; Available online: http://blogs.worldbank.org/opendata/new-country-classifications-income-level-2019-2020 (accessed on 1 October 2019).
- International Monetary Fund (IMF). World Economic Outlook Database; IMF: Washington, DC, USA, 2019; Available online: https://www.imf.org/external/pubs/ft/weo/2018/02/weodata/index.aspx. (accessed on 23 September 2019).
- Crosby, A.E.; Ortega, L.; Melanson, C. Self-directed Violence Surveillance: Uniform Definitions and Recommended Data Elements, Version 1.0; National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA, 2011.
- U.S. Department of Health and Human Services (HHS) Office of the Surgeon General and National Action Alliance for Suicide Prevention. 2012 National Strategy for Suicide Prevention: Goals and Objectives for Action; HHS: Washington, DC, USA, 2012.
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2017 (GBD 2017) Results; Institute for Health Metrics and Evaluation (IHME): Seattle, WA, USA, 2018; Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 15 August 2019).
- CDC. Understanding Suicide; CDC: Atlanta, GA, USA, 2015.
- Khang, Y.H.; Lynch, J.W.; Kaplan, G.A. Impact of economic crisis on cause-specific mortality in South Korea. Int. J. Epidemiol. 2005, 34, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Oyesanya, M.; Lopez-Morinigo, J.; Dutta, R. Systematic review of suicide in economic recession. World J. Psychiatry 2015, 5, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Stuckler, D.; Yip, P.; Gunnell, D. Impact of 2008 global economic crisis on suicide: Time trend study in 54 countries. BMJ 2013, 347. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Gunnell, D.; Sterne, J.A.C.; Lu, T.H.; Cheng, A.T.A. Was the economic crisis 1997–1998 responsible for rising suicide rates in East/Southeast Asia? A time-trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Soc. Sci. Med. 2009, 68, 1322–1331. [Google Scholar] [CrossRef]
- Stuckler, D.; Basu, S.; Suhrcke, M.; Coutts, A.; McKee, M. Effects of the 2008 recession on health: A first look at European data. Lancet 2011, 378, 124–125. [Google Scholar] [CrossRef]
- Qin, P.; Agerbo, E.; Mortensen, P.B. Suicide risk in relation to socio- economic, demographic, psychiatric, and familial factors: A national register-based study of all suicides in Denmark, 1981–1997. Am. J. Psychiatry 2003, 160, 765–772. [Google Scholar] [CrossRef]
- Rajkumar, A.P.; Senthilkumar, P.; Gayathri, K.; Shyamsundar, G.; Jacob, K.S. Associations between the macroeconomic indicators and suicide rates in India: Two ecological studies. Indian J. Psychol. Med. 2015, 37, 277–281. [Google Scholar] [CrossRef]
- Stuckler, D.; Basu, S.; Suhrcke, M.; Coutts, A.; McKee, M. The public health effect of economic crises and alternative policy responses in Europe: An empirical analysis. Lancet 2009, 374, 315–323. [Google Scholar] [CrossRef]
- Wong, P.W.C.; Chan, W.S.C.; Chen, E.Y.H.; Chan, S.S.M.; Law, Y.W.; Yip, P.S.F. Suicide among adults aged 30–49: A psychological autopsy study in Hong Kong. BMC Public Health 2008, 8, 147. [Google Scholar] [CrossRef]
- United Nations (UN). Transforming Our World: The 2030 Agenda for Sustainable Development; UN General Assembly Resolution; UN: New York, NY, USA, 2015. [Google Scholar]
- World Health Organization (WHO); The World Bank. Tracking Universal Health Coverage: 2017 Global Monitoring Report; WHO: Geneva, Switzerland; The World Bank: Washington, DC, USA, 2017. [Google Scholar]
- WHO World Health Statistics Overview 2019: Monitoring Health for the SDGs, Sustainable Development Goals; WHO: Geneva, Switzerland, 2019.
- Stenberg, K.; Hanssen, O.; Edejer, T.T.; Bertram, M.; Brindley, C.; Meshreky, A.; Rosen, J.E.; Stover, J.; Verboom, P.; Sanders, R.; et al. Financing transformative health systems towards achievement of the health sustainable development goals: A model for projected resource needs in 67 low-income and middle-income countries. Lancet Glob. Health 2017, 5, e875–e887. [Google Scholar] [CrossRef]
- WHO. Global Health Expenditure Database; WHO: Geneva, Switzerland, 2019; Available online: http://apps.who.int/nha/database/Select/Indicators/en (accessed on 18 August 2019).
- Mars, B.; Burrows, S.; Hjelmeland, H.; Gunnell, G. Suicidal behaviour across the African continent: A review of the literature. BMC Public Health 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- CDC. Cost of Injury Reports 2010; CDC: Atlanta, GA, USA, 2014.
- Shepard, D.S.; Gurewich, D.; Lwin, A.K.; Reed, G.A.; Silverman, M.M. Suicide and suicidal attempts in the United States: Costs and policy implications. Suicide Life-Threat. Behav. 2016, 46, 352–362. [Google Scholar] [CrossRef] [PubMed]
- SmartRisk. The Economic Burden of Injury in Canada; SmartRisk: Toronto, ON, Canada, 2009. [Google Scholar]
- Yang, B.; Lester, D. Recalculating the economic cost of suicide. Death Stud. 2007, 31, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Corso, P.S.; Mercy, J.A.; Simon, T.R.; Finkelstein, E.A.; Miller, T.R. Medical Costs and Productivity Losses Due to Interpersonal and Self-Directed Violence in the United States. Am. J. Prev. Med. 2007, 32, 474–482. [Google Scholar] [CrossRef]
- Greenberg, P.E.; Kessler, R.C.; Birnbaum, H.G.; Leong, S.A.; Lowe, S.W.; Berglund, P.A.; Corey-Lisle, P.K. The economic burden of depression in the United States: How did it change between 1990 and 2000? J. Clin. Psychiatry 2003, 64, 1465–1475. [Google Scholar] [CrossRef]
- Clayton, D.; Barcelo, A. The cost of suicide mortality in New Brunswick, 1996. Chronic Dis. Can. 1999, 20, 89–95. [Google Scholar]
- Orlewska, K.; Orlewska, E. Burden of suicide in Poland in 2012: How could it be measured and how big is it? Eur. J. Health Econ. 2018, 19, 409–417. [Google Scholar] [CrossRef]
- Rivera, B.; Casal, B.; Currais, L. Crisis, suicide and labour productivity losses in Spain. Eur. J. Health Econ. 2017, 18, 83–96. [Google Scholar] [CrossRef]
- Salvador-Carulla, L.; Bendeck, M.; Fernández, A.; Alberti, C.; Sabes-Figuera, R.; Molina, C.; Knapp, M. Costs of depression in Catalonia (Spain). J. Affect. Disord. 2011, 132, 130–138. [Google Scholar] [CrossRef]
- Knapp, M.; McDaid, D.; Parsonage, M. (Eds.) Mental Health Promotion and Mental Illness Prevention: The Economic Case; Department of Health: London, UK, 2011.
- OECD/EU. Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2018. [Google Scholar]
- Kennelly, B. Economic cost of suicide in Ireland. Crisis 2007, 28, 89–94. [Google Scholar] [CrossRef]
- Platt, S.; McLean, J.; Blamey, A.; MacKenzie, M.; McDaid, D.; Maxwell, M.; Halliday, E.; Woodhouse, A. Evaluation of the First Phase of Choose Life: The National Strategy and Action Plan to Prevent Suicide in Scotland; Scotland Executive: Edinburg, Scotland, UK, 2006.
- Cameron, S. Economics of suicide. In Economics Uncut: A Complete Guide to Life, Death and Misadventure; Bowmaker, S.W., Ed.; Edward Elgar Publishing: Northampton, MA, USA, 2006; pp. 229–263. [Google Scholar]
- Sobocki, P.; Jönsson, B.; Angst, J.; Rehnberg, C. Cost of Depression in Europe. J. Ment. Health Policy Econ. 2006, 9, 87–98. [Google Scholar] [PubMed]
- Thomas, C.M.; Morris, S. Cost of depression among adults in England in 2000. Br. J. Psychiatry 2003, 183, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, B.; Bebbington, P. What Price Depression? The Cost of Depression and the Cost-Effectiveness of Pharmacological Treatment. Br. J. Psychiatry 1994, 164, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Kinchin, I.; Doran, C.M. The Cost of Youth Suicide in Australia. Int. J. Environ. Res. Public Health 2018, 15, 672. [Google Scholar] [CrossRef]
- Kinchin, I.; Doran, C.M. The Economic Cost of Suicide and Non-Fatal Suicide Behavior in the Australian Workforce and the Potential Impact of a Workplace Suicide Prevention Strategy. Int. J. Environ. Res. Public Health 2017, 14, 347. [Google Scholar] [CrossRef]
- Doran, C.M.; Ling, R.; Milner, A.; Kinchin, I. The Economic Cost of Suicide and Non-fatal Suicidal Behaviour in the Australian Construction Industry. Int. J. Ment. Health Psychiatry 2016, 2. [Google Scholar] [CrossRef]
- KPMG International. Economic Cost of Suicide in Australia; KPMG: Amstelveen, The Netherlands, 2013. [Google Scholar]
- ConNetica Consulting. The Estimation of the Economic Cost of Suicide to Australia; ConNetica Consulting: Stamford, CT, USA, 2009. [Google Scholar]
- O’Dea, D.; Tucker, S. The Cost of Suicide to Society; Ministry of Health: Wellington, New Zealand, 2005.
- Chang, S.M.; Hong, J.; Cho, M.J. Economic burden of depression in South Korea. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 683–689. [Google Scholar] [CrossRef]
- Choi, Y.; Kim, Y.; Ko, Y.; Cha, E.S.; Kim, J.; Lee, W.J. Economic burden of acute pesticide poisoning in South Korea. Trop. Med. Int. Health 2012, 17, 1534–1543. [Google Scholar] [CrossRef]
- Hu, T.W.; He, Y.; Zhang, M.; Chen, N. Economic costs of depression in China. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 110–116. [Google Scholar] [CrossRef]
- Law, C.K.; Yip, P.S.; Chen, Y.Y. The economic and potential years of life lost from suicide in Taiwan, 1997–2007. Crisis 2011, 32, 152–159. [Google Scholar] [CrossRef]
- Okumura, Y.; Higuchi, T. Cost of depression among adults in Japan. Prim. Care Companion CNS Disord. 2011, 13, PCC.10m01082. [Google Scholar] [CrossRef] [PubMed]
- Yip, P.S.F.; Liu, K.Y.; Law, C.K.; Law, Y.W. Social and economic burden of suicides in Hong Kong SAR: A year of life lost perspective. Crisis 2005, 26, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Bundhamcharoen, K.; Odton, P.; Mugem, S.; Phulkerd, S.; Dhisayathikom, K.; Brown, D.W.; Tangcharoensathien, V. Costs of injuries due to interpersonal and self-directed violence in Thailand, 2005. J. Med. Assoc. Thail. 2008, 91 (Suppl. 2), S110–S118. [Google Scholar]
- Organisation for Economic Co-operation and Development (OECD). The Well-Being of Nations: The Role of Human and Social Capital; OECD: Paris, France, 2001.
- Petty, W. Political Arithmetick, or a Discourse: Concerning, the Extent and Value of Lands, People, Buildings; Husbandry, Manufacture, Commerce, Fishery, Artizans, Seamen, Soldiers; Publick Revenues, Interest, Taxes, Superlucration, Registries, Banks; Robert Caluel: London, UK, 1699. [Google Scholar]
- Farr, W. The Income and Property Tax. J. R. Stat. Soc. 1853, 16, 1–44. [Google Scholar] [CrossRef]
- Kiker, B.F. The Historical Roots of the Concept of Human Capital. J. Polit. Econ. 1966, 74, 481–499. [Google Scholar] [CrossRef]
- Fein, R. Economics of Mental Illness; Basic Books: New York, NY, USA, 1958. [Google Scholar]
- Mushkin, S.J.; Collings, F.A. Economic costs of disease and injury. Public Health Rep. 1959, 74, 795–809. [Google Scholar] [CrossRef]
- Weisbrod, B. Costs and benefits of medical research: A case study of poliomyelitis. J. Polit. Econ. 1971, 79, 527–544. [Google Scholar] [CrossRef]
- Landefeld, J.S.; Seskin, E.P. The economic value of life: Linking theory to practice. Am. J. Public Health 1982, 72, 555–566. [Google Scholar] [CrossRef]
- Linnerooth, J. The value of human life: A review of the models. Econ. Inq. 1979, 17, 52–74. [Google Scholar] [CrossRef]
- Mooney, G.H. The Valuation of Human Life; Macmillan: London, UK, 1977. [Google Scholar]
- Kirigia, J.M.; Sambo, H.B.; Sambo, L.G.; Barry, S.P. Economic burden of diabetes mellitus in the WHO African region. BMC Int. Health Hum. Rights 2009, 9, 6. [Google Scholar] [CrossRef]
- Kirigia, J.M.; Sambo, L.G.; Yokouide, A.; Soumbey-Alley, E.; Muthuri, L.K.; Kirigia, D.G. Economic burden of cholera in the WHO African region. BMC Int. Health Hum. Rights 2009, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Kirigia, J.M.; Mwabu, G.M.; Orem, J.N.; Muthuri, R.D.K. Indirect cost of maternal deaths in the WHO African Region in 2010. BMC Pregnancy Childbirth 2014, 14, 299. [Google Scholar] [CrossRef] [PubMed]
- Kirigia, J.M.; Mwabu, G.M.; Orem, J.N.; Muthuri, R.D.K. Indirect cost of maternal deaths in the WHO African Region, 2013. Int. J. Soc. Econ. 2016, 43, 532–548. [Google Scholar] [CrossRef]
- Kirigia, J.M.; Muthuri, R.D.K.; Nabyonga-Orem, J.; Kirigia, D.W. Counting the cost of child mortality in the World Health Organization African region. BMC Public Health 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- Kirigia, J.M.; Masiye, F.; Kirigia, D.W.; Akweongo, P. Indirect costs associated with deaths from the Ebola virus disease in West Africa. Infect. Dis. Poverty 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Kirigia, J.M.; Muthuri, R.N.D.K.; Muthuri, N.G. The monetary value of human lives lost through Ebola Virus Disease in the Democratic Republic of Congo in 2019. BMC Public Health 2019, 19. [Google Scholar] [CrossRef] [PubMed]
- Kirigia, J.M.; Muthuri, R.D.K. Productivity losses associated with tuberculosis deaths in the World Health Organization African Region. Infect. Dis. Poverty 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Kirigia, J.M.; Mwabu, G.M.; M’Imunya, J.M.; Muthuri, R.D.K.M.; Nkanata, L.H.K.; Gitonga, E.B. Indirect cost of non-communicable diseases deaths in the World Health Organization African Region. Int. Arch. Med. 2017, 10. [Google Scholar] [CrossRef]
- Kirigia, J.M.; Mburugu, G.N. The monetary value of human lives lost due to neglected tropical diseases in Africa. Infect. Dis. Poverty 2017, 6. [Google Scholar] [CrossRef]
- Pass, C.; Lowes, B.; Davies, L. Collins Dictionary of Economics; HarperCollins Publishers: Glasgow, UK, 2005. [Google Scholar]
- Fourie, F.C.N. How to Think and Reason in Macroeconomics; Juta & Co. Ltd.: Cape Town, South Africa, 1999. [Google Scholar]
- Weisbrod, B.A. The valuation of human capital. J. Polit. Econ. 1961, 69, 425–436. [Google Scholar] [CrossRef]
- WHO. WHO Guide to Identifying the Economic Consequences of Disease and Injury; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Chisholm, D.; Stanciole, A.E.; Edejer, T.T.T.; Evans, D.B. Economic Impact of Disease and Injury: Counting What Matters. BMJ 2010, 340, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.L. Quantifying the burden of disease: The technical basis for disability-adjusted life years. Bull. World Health Organ. 1994, 72, 429–445. [Google Scholar] [PubMed]
- WHO The World Health Report 2000—Health Systems: Improving Performance; WHO: Geneva, Switzerland, 2000.
- Kirigia, J.M. Economic Evaluation of Public Health Problems in Sub-Saharan Africa; University of Nairobi Press: Nairobi, Kenya, 2009. [Google Scholar]
- Poduri, G.S. Short-term Cost of Suicides in India. Indian J. Psychol. Med. 2016, 38, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Tsiachristas, A.; McDaid, D.; Casey, D.; Brand, F.; Leal, J.; Park, A.L.; Geulayov, G.; Hawton, K. General hospital costs in England of medical and psychiatric care for patients who self-harm: A retrospective analysis. Lancet Psychiatry 2017, 4, 759–767. [Google Scholar] [CrossRef]
- Sgobin, S.M.T.; Traballi, A.L.M.; Botega, N.J.; Coelho, O.R. Direct and indirect cost of attempted suicide in a general hospital: Cost-of-illness study. Sao Paulo Med. J. 2015, 133, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Marcotte, D.E. The economics of suicide, revisited. South. Econ. J. 2003, 69, 628–643. [Google Scholar] [CrossRef]
- Jordan, J. Is suicide bereavement different? A reassessment of the literature. Suicide Life-Threat. Behav. 2001, 31, 91–102. [Google Scholar] [CrossRef]
- Hamermesh, D.S.; Soss, N.M. An economic theory of suicide. J. Polit. Econ. 1974, 82, 83–98. [Google Scholar] [CrossRef]
- Chuang, H.L.; Huang, W.C. Economic and social correlates of regional suicide rates: A pooled cross-section and time-series analysis. J. Socio Econ. 1997, 26, 277–289. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Income Group | Countries |
|---|---|
| Group 1: High income (US$ 12,375 or more) and Upper middle income (US$ 3996–12,375) | Seychelles, Algeria, Botswana, Equatorial Guinea, Gabon, Libya, Mauritius, Namibia, South Africa (n = 9) |
| Group 2: Lower middle income (U$ 1026–3995) | Angola, Cabo Verde, Cameroon, Comoros, Congo, Côte d’Ivoire, Djibouti, Egypt, Eswatini (Swaziland), Ghana, Kenya, Lesotho, Mauritania, Morocco, Nigeria, São Tomé and Principe, Senegal, Sudan, Tunisia, Zambia, Zimbabwe (n = 21) |
| Group 3: Low income (US$ 1025 or less) | Benin, Burkina Faso, Burundi, Central African Republic, Chad, Democratic Republic of Congo, Eritrea, Ethiopia, The Gambia, Guinea, Guinea-Bissau, Liberia, Madagascar, Malawi, Mali, Mozambique, Niger, Rwanda, Sierra Leone, Somalia, South Sudan, Tanzania, Togo, Uganda (n = 24) |
| Age Group | Monetary Value (Int$) | Percent (%) |
|---|---|---|
| 10–14 | 165,278,172 | 2.36 |
| 15–19 | 629,799,693 | 9.01 |
| 20–24 | 1,014,518,001 | 14.51 |
| 25–29 | 1,023,659,026 | 14.64 |
| 30–34 | 1,857,591,488 | 26.58 |
| 35–39 | 784,496,461 | 11.22 |
| 40–44 | 559,357,213 | 8.00 |
| 45–49 | 411,995,125 | 5.89 |
| 50–54 | 287,655,819 | 4.12 |
| 55–59 | 161,681,640 | 2.31 |
| 60–64 | 69,517,406 | 0.99 |
| 65–69 | 20,064,418 | 0.29 |
| 70–74 | 4,348,864 | 0.06 |
| Total | 6,989,963,325 | 100.00 |
| Country | (A) Population | (B) SD | (C)Total Value of Human Lives Lost Due to SD (Int$) | (D) Value of Human Life Lost per SD (Int$) [D = (C/B)] | (E) Value of Human Life Lost Per Person in Population (Int$) [E = (C/A)] |
|---|---|---|---|---|---|
| Algeria | 43,088,000 | 1699 | 539,007,395 | 317,312 | 12.51 |
| Angola | 30,053,000 | 1746 | 148,449,856 | 85,023 | 4.94 |
| Benin | 11,722,000 | 694 | 90,697,600 | 130,742 | 7.74 |
| Botswana | 2,378,000 | 200 | 56,953,746 | 284,592 | 23.95 |
| Burkina Faso | 19,996,000 | 1507 | 31,844,639 | 21,126 | 1.59 |
| Burundi | 11,529,000 | 698 | 5,143,583 | 7374 | 0.45 |
| Cameroon | 25,506,000 | 2172 | 85,638,780 | 39,433 | 3.36 |
| Cape Verde | 551,000 | 87 | 11,292,078 | 129,637 | 20.49 |
| Central African Republic | 5,181,000 | 518 | 3,309,196 | 6389 | 0.64 |
| Chad | 12,802,000 | 791 | 16,507,666 | 20,863 | 1.29 |
| Comoros | 872,000 | 44 | 752,082 | 17,266 | 0.86 |
| Republic of Congo | 4,568,000 | 463 | 40,156,994 | 86,805 | 8.79 |
| Cote d’Ivoire | 26,275,000 | 1916 | 74,469,526 | 38,870 | 2.83 |
| Democratic Republic of Congo | 91,931,000 | 5430 | 51,940,227 | 9566 | 0.56 |
| Equatorial Guinea | 887,000 | 66 | 27,154,980 | 410,550 | 30.61 |
| Eritrea | 6,159,000 | 561 | 14,135,148 | 25,213 | 2.30 |
| Ethiopia | 95,644,000 | 5106 | 169,654,845 | 33,226 | 1.77 |
| Gabon | 2,080,000 | 158 | 36,403,474 | 230,189 | 17.50 |
| Gambia, The | 2,238,000 | 119 | 2,083,448 | 17,473 | 0.93 |
| Ghana | 29,742,000 | 1908 | 579,975,200 | 304,007 | 19.50 |
| Guinea | 13,627,000 | 746 | 17,175,327 | 23,015 | 1.26 |
| Guinea-Bissau | 1,776,000 | 141 | 3,343,263 | 23,777 | 1.88 |
| Kenya | 49,364,000 | 3058 | 153,781,596 | 50,282 | 3.12 |
| Lesotho | 2,048,000 | 512 | 16,886,477 | 33,003 | 8.25 |
| Liberia | 4,978,000 | 339 | 4,918,594 | 14,492 | 0.99 |
| Madagascar | 27,055,000 | 1590 | 36,331,049 | 22,846 | 1.34 |
| Malawi | 20,289,000 | 1187 | 16,651,694 | 14,023 | 0.82 |
| Mali | 20,161,000 | 724 | 16,795,466 | 23,192 | 0.83 |
| Mauritania | 4,058,000 | 158 | 7,938,529 | 50,349 | 1.96 |
| Mauritius | 1,279,000 | 118 | 56,057,465 | 476,497 | 43.83 |
| Mozambique | 31,157,000 | 2722 | 42,397,600 | 15,577 | 1.36 |
| Namibia | 2,408,000 | 231 | 39,094,689 | 169,130 | 16.24 |
| Niger | 19,939,000 | 753 | 10,189,927 | 13,539 | 0.51 |
| Nigeria | 199,206,000 | 8069 | 416,377,633 | 51,599 | 2.09 |
| Rwanda | 12,432,000 | 777 | 23,328,496 | 30,036 | 1.88 |
| Sao Tome and Principe | 222,000 | 5 | 304,456 | 57,046 | 1.37 |
| Senegal | 16,793,000 | 1112 | 224,927,451 | 202,362 | 13.39 |
| Seychelles | 96,000 | 9 | 23,654,633 | 2,659,224 | 246.40 |
| Sierra Leone | 7,737,000 | 453 | 5,736,592 | 12,654 | 0.74 |
| South Africa | 58,333,000 | 6221 | 1,260,115,686 | 202,558 | 21.60 |
| South Sudan | 13,378,000 | 595 | 61,077,785 | 102,569 | 4.57 |
| Swaziland | 1,177,000 | 208 | 10,650,821 | 51,284 | 9.05 |
| Tanzania | 52,067,000 | 2636 | 123,997,824 | 47,044 | 2.38 |
| Togo | 8,205,000 | 568 | 11,037,758 | 19,431 | 1.35 |
| Uganda | 40,007,000 | 2029 | 246,143,613 | 121,334 | 6.15 |
| Zambia | 18,321,000 | 1161 | 32,396,104 | 27,908 | 1.77 |
| Zimbabwe | 15,658,000 | 2647 | 47,135,984 | 17,804 | 3.01 |
| Djibouti | 1,078,000 | 61 | 13,773,474 | 226,015 | 12.78 |
| Egypt | 99,211,000 | 4756 | 1,272,197,958 | 267,508 | 12.82 |
| Libya | 6,578,000 | 578 | 135,388,853 | 234,068 | 20.58 |
| Morocco | 35,587,000 | 2574 | 464,016,945 | 180,238 | 13.04 |
| Somalia | 15,540,481 | 852 | 11,761,336 | 13,797 | 0.76 |
| Sudan | 43,222,000 | 1655 | 118,964,551 | 71,863 | 2.75 |
| Tunisia | 11,783,000 | 377 | 79,843,231 | 211,807 | 6.78 |
| Summary of Indirect Costs | Group 1: High-Income and Upper-Middle-Income Countries Sub-Total Cost (Int$) | Group 2: Lower-Middle-Income Countries Sub-Total Cost (Int$) | Group 3: Low-Income Countries Sub-Total Cost (Int$) | Grand total Cost (Int$) |
|---|---|---|---|---|
| (1) Total present value of SDs | 2,173,830,922 | 3,799,929,726 | 1,016,202,676 | 6,989,963,325 |
| (2) Average present value per SD | 234,244 | 109,545 | 32,223 | 92,576 |
| (3) Average present value per person in population | 18.56 | 6.18 | 1.86 | 5.5 |
| % of grand total | 31.0 | 54.5 | 14.5 | 100 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kirigia, J.M.; Muthuri, R.D.K.; Muthuri, N.G. The Monetary Value of Human Lives Lost to Suicide in the African Continent: Beating the African War Drums. Healthcare 2020, 8, 84. https://doi.org/10.3390/healthcare8020084
Kirigia JM, Muthuri RDK, Muthuri NG. The Monetary Value of Human Lives Lost to Suicide in the African Continent: Beating the African War Drums. Healthcare. 2020; 8(2):84. https://doi.org/10.3390/healthcare8020084
Chicago/Turabian StyleKirigia, Joses M., Rosenabi D.K. Muthuri, and Newton G. Muthuri. 2020. "The Monetary Value of Human Lives Lost to Suicide in the African Continent: Beating the African War Drums" Healthcare 8, no. 2: 84. https://doi.org/10.3390/healthcare8020084
APA StyleKirigia, J. M., Muthuri, R. D. K., & Muthuri, N. G. (2020). The Monetary Value of Human Lives Lost to Suicide in the African Continent: Beating the African War Drums. Healthcare, 8(2), 84. https://doi.org/10.3390/healthcare8020084