Cross-Country Differences and Similarities in Undernutrition Prevalence and Risk as Measured by SCREEN II in Community-Dwelling Older Adults

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.2.1. Canadian Derived International Dataset
2.2.2. Dutch Dataset
2.2.3. New Zealand Dataset
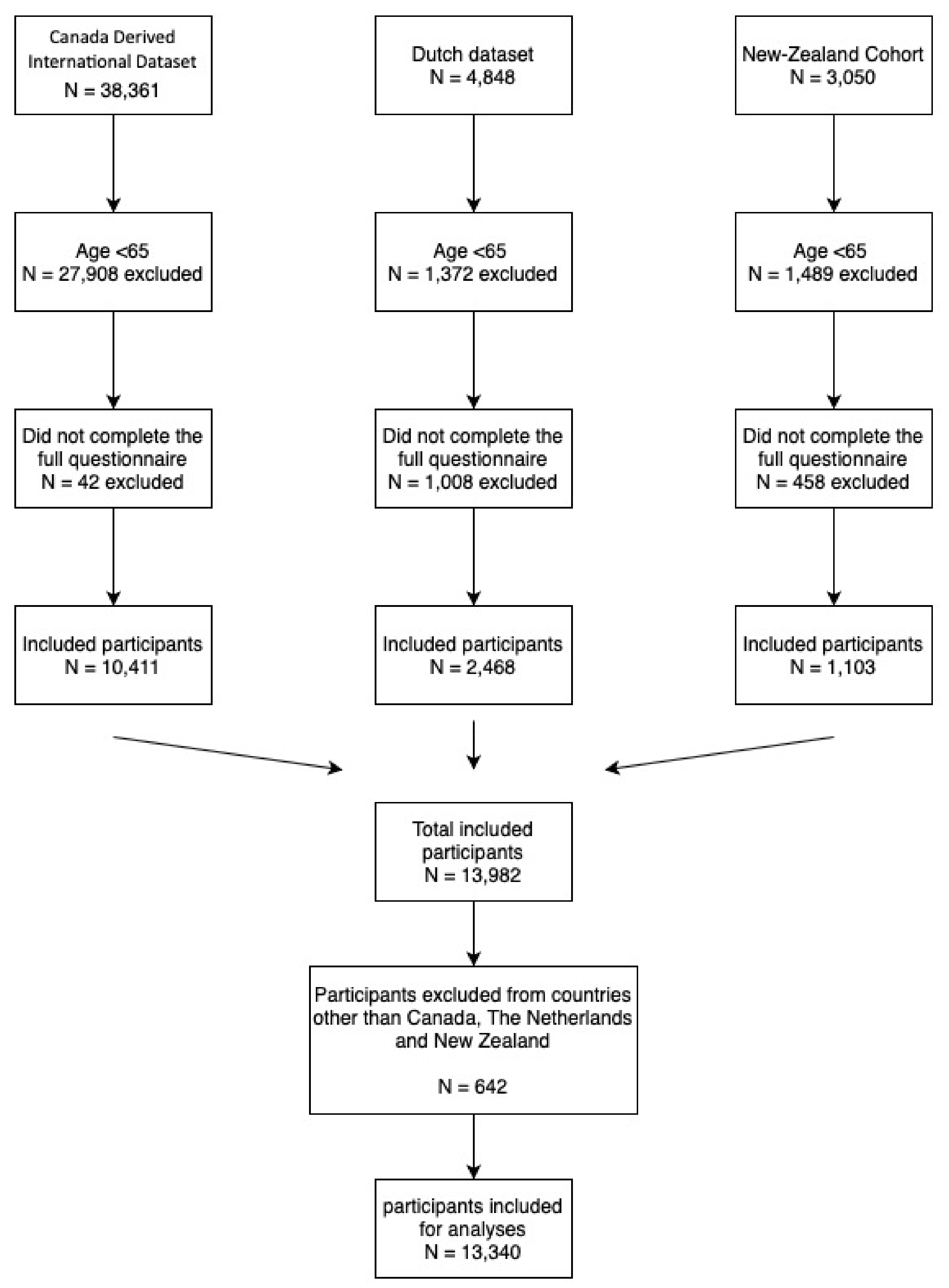
2.2.4. Participants Current Study
2.3. Measurements
2.4. Data Analysis
Sensitivity Analysis
3. Results
3.1. Total Score with All Included Datasets
3.2. Sensitivity Analyses: Total Score with only Datasets from Online Websites
3.3. Nutritional Risk Items
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Total | The Netherlands | New Zealand | Canada | |
|---|---|---|---|---|
| n = 13,416 | n = 2482 | n = 1396 | n = 9538 | |
| Change in weight last six months (Gained or lost ≥ 2.5 kg) | 6377 (47.5%) | 964 (38.8%) | 420 (31.8%) | 4940 (51.8%) |
| OR | ref | 0.74 (0.61–0.89) | 1.69 (1.50–1.91) | |
| adjusted OR * | 0.79 (0.66–0.96) | 1.72 (1.53–1.94) | ||
| Unintentional weight change last six months | 1804 (13.4%) | 245 (9.9%) | 122 (9.2%) | 1413 (14.8%) |
| OR | ref | 0.93 (0.69–1.26) | 1.59 (1.32–1.92) | |
| adjusted OR * | 1.22 (0.90–1.67) | 1.73 (1.43–2.10) | ||
| Perception bodyweight (More or less than it should be) | 9536 (71.1%) | 1554 (62.6%) | 771 (58.4%) | 7165 (75.1%) |
| OR | ref | 0.84 (0.70–1.00) | 1.80 (1.59–2.04) | |
| adjusted OR * | 0.84 (0.67–1.05) | 1.75 (1.54–1.98) | ||
| Skipping meals (Sometimes or more frequent) | 4842 (36.1%) | 536 (21.6%) | 229 (17.3%) | 4032 (42.3%) |
| OR | ref | 0.76 (0.61–0.96) | 2.66 (2.32–3.05) | |
| adjusted OR * | 0.97 (0.78–1.21) | 2.76 (2.40–3.16) | ||
| Limitation or avoiding certain products | 6634 (49.8%) | 1011 (40.7%) | 550 (41.7%) | 5037 (52.8%) |
| OR | ref | 1.04 (0.87–1.24) | 1.63 (1.45–1.83) | |
| adjusted OR * | 1.08 (0.90–1.30) | 1.63 (1.45–1.84) | ||
| Fair/poor Appetite | 2659 (19.8%) | 597 (24.1%) | 85 (6.4%) | 1943 (20.4%) |
| OR | ref | 0.22 (0.16–0.30) | 0.81 (0.70–0.93) | |
| adjusted OR * | 0.30 (0.22–0.42) | 0.88 (0.76–1.02) | ||
| Low intake fruit or vegetables per day (Three or less Portions) | 6932 (51.7%) | 1674 (67.4%) | 518 (39.2%) | 4696 (49.2%) |
| OR | ref | 0.31 (0.26–0.37) | 0.47 (0.41–0.53) | |
| adjusted OR * | 0.31 (0.26–0.38) | 0.48 (0.42–0.54) | ||
| Low intake of meat, eggs, fish or meat substitute (Once a day or less) | 5581 (41.6%) | 1376 (55.4%) | 557 (42.2%) | 3613 (37.9%) |
| OR | ref | 0.59 (0.49–0.70) | 0.49 (0.44–0.55) | |
| adjusted OR * | 0.61 (0.51–0.73) | 0.50 (0.45–0.56) | ||
| Low dairy intake (One portion a day or less) | 8141 (60.7%) | 1373 (55.3%) | 806 (61.1%) | 5919 (62.1%) |
| OR | ref | 1.27 (1.06–1.51) | 1.32 (1.18–1.49) | |
| adjusted OR * | 1.23 (1.02–1.47) | 1.32 (1.17–1.49) | ||
| Low fluid intake (≤four glasses) | 4904 (36.6%) | 622 (25.1%) | 415 (31.4%) | 3827 (40.1%) |
| OR | ref | 1.37 (1.13–1.66) | 2.00 (1.76–2.28) | |
| adjusted OR * | 1.54 (1.26–1.88) | 2.15 (1.88–2.45) | ||
| Problems with coughing, choking or pain when swallowing (Sometimes or often) | 2372 (17.7%) | 437 (17.6%) | 142 (10.8%) | 1771 (18.6%) |
| OR | ref | 0.56 (0.43–0.74) | 1.07 (0.92–1.24) | |
| adjusted OR * | 0.69 (0.53–0.91) | 1.12 (0.96–1.31) | ||
| Problems with biting or chewing (Sometimes or often) | 2344 (17.5%) | 369 (14.9%) | 175 (13.3%) | 1774 (18.6%) |
| OR | ref | 0.88 (0.68–1.13) | 1.31 (1.12–1.54) | |
| adjusted OR * | 1.19 (0.91–1.54) | 1.44 (1.22–1.70) | ||
| Use of meal replacements/supplements (Sometimes or more frequent) | 2495 (18.6%) | 236 (9.5%) | 142 (10.8%) | 2095 (22.0%) |
| OR | ref | 1.15 (0.86–1.53) | 2.68 (2.22–3.23) | |
| adjusted OR * | 1.35 (1.01–1.81) | 2.89 (2.49–3.33) | ||
| Eating meals together (Sometimes or fewer) | 5483 (40.9%) | 1014 (40.9%) | 414 (31.4%) | 4004 (42.0%) |
| OR | 0.66 (0.55–0.80) | 1.05 (0.93–1.18) | ||
| adjusted OR * | ref | 0.84 (0.69–1.01) | 1.11 (0.99–1.26) | |
| Meal preparation (Meal preparation is hard/I do not enjoy the meals that were prepared for me) | 6442 (48.0%) | 984 (39.6%) | 405 (30.7%) | 5004 (52.5%) |
| OR | ref | 0.67 (0.56–0.81) | 1.68 (1.49–1.89) | |
| adjusted OR * | 0.85 (0.70–1.03) | 1.78 (1.57–2.00) | ||
| Problems with doing groceries (Sometimes or more often) | 10,285 (76.7%) | 433 (17.4%) | 350 (26.5%) | 2300 (24.1%) |
| OR | 3131 (23.3%) | ref | 1.71 (1.38–2.11) | 1.50 (1.30–1.75) |
| adjusted OR * | 2.60 (2.09–3.25) | 1.72 (1.48–2.01) |
References
- WHO. Global Health and Aging; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Agarwal, E.; Miller, M.D.; Yaxley, A.; Isenring, E. Malnutrition in the elderly: A narrative review. Maturitas 2013, 76, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Kiesswetter, E.; Cederholm, T.; Donini, L.M.; Eglseer, D.; Norman, K.; Schneider, S.M.; Ströbele-Benschop, N.; Torbahn, G.; Wirth, R.; et al. Development of a Model on Determinants of Malnutrition in Aged Persons: A MaNuEL Project. Gerontol. Geriatr. Med. 2019, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.B.; Foley, A.L.; Barnard, R.; Isenring, E.A.; Miller, M.D. Nutritional screening in community-dwelling older adults: A systematic literature review. Asia Pac. J. Clin. Nutr. 2010, 19, 440–449. [Google Scholar] [PubMed]
- Power, L.; Mullaly, D.; Gibney, E.; Clarke, M.; Visser, M.; Dorothee, V.; Bardon, L.; de van der Schueren, M.A.E.; Corish, C. A review of the validity of malnutrition screening tools used in older adults in community and healthcare settings—A MaNuEL study. Clin. Nutr. 2018, 24, 1–13. [Google Scholar] [CrossRef]
- Keller, H.H. Promoting food intake in older adults living in the community: A review. Appl. Physiol. Nutr. Metab. 2007, 32, 991–1000. [Google Scholar] [CrossRef]
- Keller, H.H.; Goy, R.; Kane, S.-L. Validity and reliability of SCREEN II (Seniors in the Community: Risk evaluation for eating and nutrition, Version II). Eur. J. Clin. Nutr. 2005, 59, 1149–1157. [Google Scholar] [CrossRef]
- Haakma, T.A.; Wham, C. High prevalence of Nutrition risk among community living older people in Woerden, The Netherlands. J. Aging Res. Clin. Pract. 2015, 4, 230–234. [Google Scholar]
- Borkent, J.; Beelen, J.; Linschooten, J.O.; Roodenburg, A.J.C.; De Van Der Schueren, M.A. The ConsuMEER study: A randomised trial towards the effectiveness of protein-rich ready-made meals and protein-rich dairy products in increasing protein intake of community-dwelling older adults after switching from self-prepared meals towards ready-made meals. J. Nutr. Sci. 2019, 8, e30. [Google Scholar] [CrossRef]
- Wham, C.; Teh, R.; Robinson, M.; Kerse, N.M. What is associated with nutrition risk in very old age? J. Nutr. Health Aging 2011, 15, 247–251. [Google Scholar] [CrossRef]
- Ramage-Morin, P.L.; Garriguet, D. Nutritional risk among older Canadians. Health Rep. 2013, 24, 3–13. [Google Scholar]
- Dietitians of Canada. Nutri-eSCREEN. Available online: http://www.nutritionscreen.ca/escreen/default.aspx (accessed on 1 June 2020).
- Stuurgroep Ondervoeding. Goed Gevoed Ouderworden. Available online: https://www.goedgevoedouderworden.nl (accessed on 1 June 2020).
- Borkent, J.W.; Naumann, E.; Vasse, E.; van der Heijden, E.; de van der Schueren, M.A.E. Prevalence and determinants of undernutrition in a sample of dutch community-dwelling older adults: Results from two online screening tools. Int. J. Environ. Res. Public Health 2019, 16, 1562. [Google Scholar] [CrossRef] [PubMed]
- Dulin, P.L.; Stephens, C.; Alpass, F.; Hill, R.D.; Stevenson, B. The impact of socio-contextual, physical and lifestyle variables on measures of physical and psychological wellbeing among Māori and non-Māori: The New Zealand Health, Work and Retirement Study. Ageing Soc. 2011, 31, 1406–1424. [Google Scholar] [CrossRef]
- Wham, C.; Teh, R.; Moyes, S.A.; Dyall, L.; Kepa, M.; Hayman, K.; Kerse, N. Health and social factors associated with nutrition risk: Results from life and living in advanced age: A cohort study in New Zealand (LILACS NZ). J. Nutr. Health Aging 2015, 19, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Gallacher, J.E.J.; Hatch, E.E. Why representativeness should be avoided. Int. J. Epidemiol. 2013, 42, 1012–1014. [Google Scholar] [CrossRef] [PubMed]
- Hatch, E.; Hahn, K.A.; Wise, L.A.; Mikkelsen, E.M.; Kumar, R.; Fox, M.P.; Brooks, D.; Riis, A.H.; Sørensen, H.T.; Rothman, K.J. Evaluation of Selection Bias in an Internet-based Study of Pregnancy Planners. Epidemiology 2016, 27, 98–104. [Google Scholar] [CrossRef]
- Pizzi, C.; De Stavola, B.; Merletti, F.; Bellocco, R.; dos Santos Silva, I.; Pearce, N.; Richiardi, L. Sample selection and validity of exposureedisease association estimates in cohort studies. J. Epidemiol. Community Health 2011, 65, 407–411. [Google Scholar] [CrossRef]
- Borkent, J.; Schuurman, L.; Beelen, J.; Linschooten, J.; Keller, H.; Roodenburg, A.; de van der SChueren, M. What do screening tools measure? lessons learned from SCREEN II and SNAQ65+. Clin. Nutr. ESPEN 2020. accepted for publication. [Google Scholar]
- Ministry of Health. Eating and Activity Guidelines for New Zealand Adults; Ministry of Health: Wellington, New Zealand, 2015.
- Department of Health and Human Services. Dietary Guidelines for Americans 2015–2020 Eighth Edition; Department of Health and Human Services: Washington, DC, USA, 2015.
- RIVM. Dutch National Food Consumption Survey Older Adults 2010–2012; RIVM: Bilthoven, The Netherlands, 2013. [Google Scholar]
- Garriguet, D. Overview of Canadians’ Eating Habits. Stat. Canada 2004, 2004, 82–620. [Google Scholar]
- Ministry of Health. Food and Nutrition Guidelines for Healthy Older People: A Background Paper; Ministry of Health: Wellington, New Zealand, 2013.
- Bauer, J.M.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.M.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper From the PROT-AGE Study Group. J. Am. Med Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Hooper, L.; Bunn, D.; Jimoh, F.O.; Fairweather-Tait, S. Water-loss dehydration and aging. Mech. Ageing Dev. 2014, 136, 50–58. [Google Scholar] [CrossRef]
- Luckey, A.E.; Parsa, C.J. Fluid and Electrolytes in the Aged. Arch. Surg. 2003, 138, 1055. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Bunn, D.K.; Downing, A.; Jimoh, F.O.; Groves, J.; Free, C.; Cowap, V.; Potter, J.F.; Hunter, P.R.; Shepstone, L. Which Frail Older People Are Dehydrated? The UK DRIE Study. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2015, 71, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Liperoti, R.; Soldato, M.; Cipriani, M.C.; Bernabei, R.; Landi, F. Chewing Problems and Mortality in Older Adults in Home Care: Results from the Aged in Home Care Study. J. Am. Geriatr. Soc. 2007, 55, 1961–1966. [Google Scholar] [CrossRef] [PubMed]
- Furuta, M.; Yamashita, Y. Oral Health and Swallowing Problems. Curr. Phys. Med. Rehabil. Rep. 2013, 1, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Kandelman, D.; Arpin, S.; Ogawa, H. Global oral health of older people--call for public health action. Community Dent Health 2010, 27, 257–267. [Google Scholar]
- Tada, A.; Miura, H. Systematic review of the association of mastication with food and nutrient intake in the independent elderly. Arch. Gerontol. Geriatr. 2014, 59, 497–505. [Google Scholar] [CrossRef]
- Quandt, S.A.; Chen, H.; Bell, R.A.; Savoca, M.R.; Anderson, A.M.; Leng, X.; Kohrman, T.; Gilbert, G.H.; Arcury, T.A. Food Avoidance and Food Modification Practices of Older Rural Adults: Association With Oral Health Status and Implications for Service Provision. Gerontologist 2009, 50, 100–111. [Google Scholar] [CrossRef]
- Vandenberghe-Descamps, M.; Sulmont-Rossé, C.; Septier, C.; Follot, C.; Feron, G.; Labouré, H. Impact of blade tenderization, marinade and cooking temperature on oral comfort when eating meat in an elderly population. Meat Sci. 2018, 145, 86–93. [Google Scholar] [CrossRef]
- Host, A.; McMahon, A.-T.; Walton, K.; Charlton, K. Factors Influencing Food Choice for Independently Living Older People—A Systematic Literature Review. J. Nutr. Gerontol. Geriatr. 2016, 35, 67–94. [Google Scholar] [CrossRef]
- Wylie, C.; Copeman, J.; Kirk, S.F. Health and social factors affecting the food choice and nutritional intake of elderly people with restricted mobility. J. Hum. Nutr. Diet. 1999, 12, 375–380. [Google Scholar] [CrossRef]
- Canada Statistics Location of Internet access by Age Group and Household Income Quartile. Available online: https://doi.org/10.25318/2210008101-eng (accessed on 18 May 2020).
- CBS Internet; Toegang, Gebruik en Faciliteiten. Available online: https://statline.cbs.nl/Statweb/publication/?DM=SLNL&PA=83429ned&D1=0-69&D2=3-19&D3=0&D4=a&VW=T (accessed on 22 May 2020).
- Ministery of social Development. The Social Report 2016; Ministery of Social Development: Wellington, New Zealand, 2016.
- Yoon, H.; Jang, Y.; Vaughan, P.W.; Garcia, M. Older Adults’ Internet Use for Health Information: Digital Divide by Race/Ethnicity and Socioeconomic Status. J. Appl. Gerontol. 2018, 39, 105–110. [Google Scholar] [CrossRef] [PubMed]

| Total | The Netherlands | New Zealand | Canada | |
|---|---|---|---|---|
| n = 13,340 | n = 2482 | n = 1320 | n = 9538 | |
| Gender | ||||
| Men | 3544 (26.6%) | 607 (24.5%) | 589 (42.2%) | 2368 (24.8%) |
| Women | 9796 (73.4%) | 1875 (75.5%) | 807 (57.8%) | 7170 (75.2%) |
| Age | ||||
| 65–74 | 8773 (65.8%) | 1437(57.9%) | 1025 (77.7%) | 6311 (66.2%) |
| 75–84 | 3569 (26.8%) | 805 (32.4%) | 283 (21.4%) | 2481 (26.0%) |
| ≥85 | 998 (7.5%) | 240 (9.7%) | 12 (0.9%) | 746 (7.8%) |
| SCREEN II | ||||
| ≥54 | 1909 (14.3%) | 394 (15.9%) | 343 (26.0%) | 1172 (12.3%) |
| ≤53 * | 11,431 (85.7%) | 2088 (84.1%) | 977 (74.0%) | 8366 (87.7%) |
| OR | ref | 0.54 (0.43–0.67) | 1.35 (1.15–1.59) | |
| Adjusted OR *** | 0.60 (0.48–0.75) | 1.39 (1.18–1.64) | ||
| SCREEN II | ||||
| ≥50 | 4499 (33.7%) | 956 (38.5%) | 690 (52.3%) | 2853 (29.9%) |
| ≤49 ** | 8841 (66.3%) | 1526 (61.5%) | 630 (47.7%) | 6685 (70.1%) |
| OR | ref | 0.57 (0.48–0.68) | 1.47 (1.30–1.66) | |
| Adjusted OR *** | 0.66 (0.55–0.79) | 1.53 (1.36–1.73) | ||
| SCREEN II | ||||
| total score | 44.6 (9.3) | 46.1 (8.3) | 48.7 (7.4) | 43.7 (9.5) |
| Regression coefficient | ref | 2.6 (1.9; 3.5) | −2.4 (−2.9; −1.8) | |
| Adjusted Regression coefficient *** | 1.4 (0.6; 2.2) | −2.7 (−3.2; −2.2) | ||
| Total | The Netherlands | New Zealand | Canada | |
|---|---|---|---|---|
| n = 12,237 | n = 2482 | n = 217 | n = 9538 | |
| Gender | ||||
| Men | 3044 (24.9%) | 607 (24.5%) | 69 (31.8%) | 2368 (24.8%) |
| Women | 9193 (75.1%) | 1875 (75.5%) | 148 (68.2%) | 7170 (75.2%) |
| Age | ||||
| 65–74 | 7902 (64.6%) | 1437 (57.9%) | 154 (71.0%) | 6311 (66.2%) |
| 75–84 | 3340 (27.3%) | 805 (32.4%) | 54 (24.9%) | 2481 (26.0%) |
| ≥85 | 995 (8.1%) | 240 (9.7%) | 9 (4.1%) | 746 (7.8%) |
| SCREEN II | ||||
| ≥54 | 1598(13.1%) | 394 (15.9%) | 32 (14.7%) | 1172 (12.3%) |
| ≤53 * | 10,639 (86.9%) | 2088 (84.1%) | 185 (85.3%) | 8366 (87.7%) |
| OR | ref | 1.09 (0.65; 1.82) | 1.35 (1.15; 1.59) | |
| Adjusted OR *** | 1.17 (0.70; 1.96) | 1.39 (1.18; 1.64) | ||
| SCREEN II | ||||
| ≥50 | 3878 (31.7%) | 956 (38.5%) | 69 (31.8%) | 2853 (29.9%) |
| ≤49 ** | 8359 (68.3%) | 1526 (61.5%) | 148 (68.2%) | 6685 (70.1%) |
| OR | ref | 1.34 (0.91; 1.99) | 1.47 (1.30; 1.66) | |
| Adjusted OR *** | 1.47 (1.00; 2.18) | 1.54 (1.36; 1.74) | ||
| SCREEN II | ||||
| total score | 44.2 (9.3) | 46.1 (8.3) | 43.0 (10.3) | 43.7 (9.5) |
| Regression coefficient | ref | −3.1 (−4.8; −1.4) | −2.4 (−2.9; −1.8) | |
| Adjusted Regression coefficient *** | −3.8 (−5.5; −2.2) | −2.7 (−3.2; −2.2) | ||
| Total | The Netherlands | New Zealand | Canada | |
|---|---|---|---|---|
| n = 12,237 | n = 2482 | n = 293 | n = 9538 | |
| Change in weight in last six months (gained or lost ≥ 2.5 kg) | 6023 (49.2%) | 964 (38.8%) | 119 (54.8%) | 4940 (51.8%) |
| OR | ref | 1.91 (1.33–2.76) | 1.59 (1.31–1.92) | |
| adjusted OR * | 2.00 (1.38–2.89) | 1.73 (1.43–2.10) | ||
| Unintentional weight change last six months | 1703 (13.9%) | 245 (9.9%) | 45 (20.7%) | 1413 (14.8%) |
| OR | ref | 2.39 (1.50–3.80) | 1.48 (1.24–1.76) | |
| adjusted OR * | 2.87 (1.79–4.61) | 1.62 (1.35–1.93) | ||
| Perception bodyweight (more or less than it should be) | 8864 (72.4%) | 1554 (62.6%) | 145 (66.8%) | 7165 (75.1%) |
| OR | ref | 1.20 (0.82–1.77) | 1.80 (1.59–2.04) | |
| adjusted OR ** | 1.13 (0.77–1.67) | 1.74 (1.54–1.97) | ||
| Skipping meals (sometimes or more frequent) | 4632 (37.9%) | 536 (21.6%) | 64 (29.5%) | 4032 (42.3%) |
| OR | ref | 1.52 (1.01–2.27) | 2.66 (2.32–3.05) | |
| adjusted OR * | 1.62 (1.08–2.42) | 2.76 (2.40–3.16) | ||
| Limitation or avoiding certain products | 6148 (50.2%) | 1011 (40.7%) | 100 (46.1%) | 5037 (52.8%) |
| OR | ref | 1.24 (0.86–1.79) | 1.63 (1.45–1.83) | |
| adjusted OR * | 1.27 (0.88– 1.83) | 1.63 (1.45–1.84) | ||
| Fair/poor Appetite | 2595 (21.2%) | 597 (24.1%) | 55 (25.3%) | 1943 (20.4%) |
| OR | ref | 1.07 (0.70–1.63) | 0.81 (0.70–0.93) | |
| adjusted OR * | 1.35 (0.87–2.08) | 0.88 (0.76–1.02) | ||
| Low intake fruit or vegetables per day (three or less portions) | 6455 (52.7%) | 1674 (67.4%) | 85 (39.2%) | 4696 (49.2%) |
| OR | ref | 0.31 (0.21–0.45) | 0.38 (0.28–0.52) | |
| adjusted OR * | 0.32 (0.22–0.46) | 0.48 (0.42–0.54) | ||
| Low intake of meat, eggs, fish or meat substitute (once a day or less) | 5113 (41.8%) | 1376 (55.4%) | 124 (57.1%) | 3613 (37.9%) |
| OR | ref | 1.07 (0.74–1.55) | 0.49 (0.44–0.55) | |
| adjusted OR * | 1.12 (0.77–1.62) | 0.50 (0.45–0.56) | ||
| Low dairy intake (one portion a day or less) | 7434 (60.8%) | 1373 (55.3%) | 142 (65.4%) | 5919 (62.1%) |
| OR | ref | 1.53 (1.04–2.24) | 1.32 (1.18–1.49) | |
| adjusted OR * | 1.51 (1.03–2.22) | 1.32 (1.17–1.48) | ||
| Low fluid intake (≤four glasses) | 4514 (36.9%) | 622 (25.1%) | 65 (30.0%) | 3827 (40.1%) |
| OR | ref | 1.28 (0.86–1.91) | 2.00 (1.76–2.28) | |
| adjusted OR * | 1.41 (0.94–2.11) | 2.16 (1.89–2.46) | ||
| Problems with coughing, choking or pain when swallowing (sometimes or often) | 2245 (18.3%) | 437 (17.6%) | 37 (17.1%) | 1771 (18.6%) |
| OR | ref | 0.96 (0.59–1.56) | 1.07 (0.92–1.24) | |
| adjusted OR * | 1.08 (0.66–1.77) | 1.12 (0.96–1.31) | ||
| Problems with biting or chewing (sometimes or often) | 2187 (17.9%) | 369 (14.9%) | 44 (20.3%) | 1774 (18.6%) |
| OR | ref | 1.46 (0.92–2.30) | 1.31 (1.12–1.54) | |
| adjusted OR * | 1.78 (1.12–2.85) | 1.44 (1.22–1.70) | ||
| Use of meal replacements/supplements (sometimes or more frequent) | 2362 (19.3%) | 236 (9.5%) | 31 (14.3%) | 2095 (22.0%) |
| OR | ref | 1.59 (0.93–2.69) | 2.68 (2.22–3.23) | |
| adjusted OR * | 1.78 (1.04– 3.03) | 2.89 (2.39–3.49) | ||
| Eating meals with others (sometimes or fewer) | 5143 (42.0%) | 1014 (40.9%) | 125 (57.6%) | 4004 (42.0%) |
| OR | ref | 1.97 (1.36– 2.85) | 1.05 (0.93–1.18) | |
| adjusted OR * | 2.31 (1.58–3.35) | 1.12 (0.99–1.26) | ||
| Meal preparation (meal preparation is hard/I do not enjoy the meals that were prepared for me) | 6123 (50.0%) | 984 (39.6%) | 135 (62.2%) | 5004 (52.5%) |
| OR | ref | 2.51 (1.72–3.65) | 1.68 (1.49–1.89) | |
| adjusted OR * | 2.94 (2.00–4.33) | 1.77 (1.57–2.00) | ||
| Problems with doing groceries (sometimes or more often) | 2794 (22.8%) | 433 (17.4%) | 61 (28.1%) | 2300 (24.1%) |
| OR | ref | 1.85 (1.22–2.79) | 1.50 (1.30–1.75) | |
| adjusted OR * | 2.42 (1.58–3.71) | 1.72 (1.48–2.01) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borkent, J.W.; Keller, H.; Wham, C.; Wijers, F.; de van der Schueren, M.A.E. Cross-Country Differences and Similarities in Undernutrition Prevalence and Risk as Measured by SCREEN II in Community-Dwelling Older Adults. Healthcare 2020, 8, 151. https://doi.org/10.3390/healthcare8020151
Borkent JW, Keller H, Wham C, Wijers F, de van der Schueren MAE. Cross-Country Differences and Similarities in Undernutrition Prevalence and Risk as Measured by SCREEN II in Community-Dwelling Older Adults. Healthcare. 2020; 8(2):151. https://doi.org/10.3390/healthcare8020151
Chicago/Turabian StyleBorkent, Jos W., Heather Keller, Carol Wham, Fleur Wijers, and Marian A. E. de van der Schueren. 2020. "Cross-Country Differences and Similarities in Undernutrition Prevalence and Risk as Measured by SCREEN II in Community-Dwelling Older Adults" Healthcare 8, no. 2: 151. https://doi.org/10.3390/healthcare8020151
APA StyleBorkent, J. W., Keller, H., Wham, C., Wijers, F., & de van der Schueren, M. A. E. (2020). Cross-Country Differences and Similarities in Undernutrition Prevalence and Risk as Measured by SCREEN II in Community-Dwelling Older Adults. Healthcare, 8(2), 151. https://doi.org/10.3390/healthcare8020151