Technology to Support Aging in Place: Older Adults’ Perspectives

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Data Collection
2.2.1. Focus Group Semi-Structured Interview Guide
2.2.2. Survey
Westin Privacy Segmentation Index
Westin Privacy Concern Index
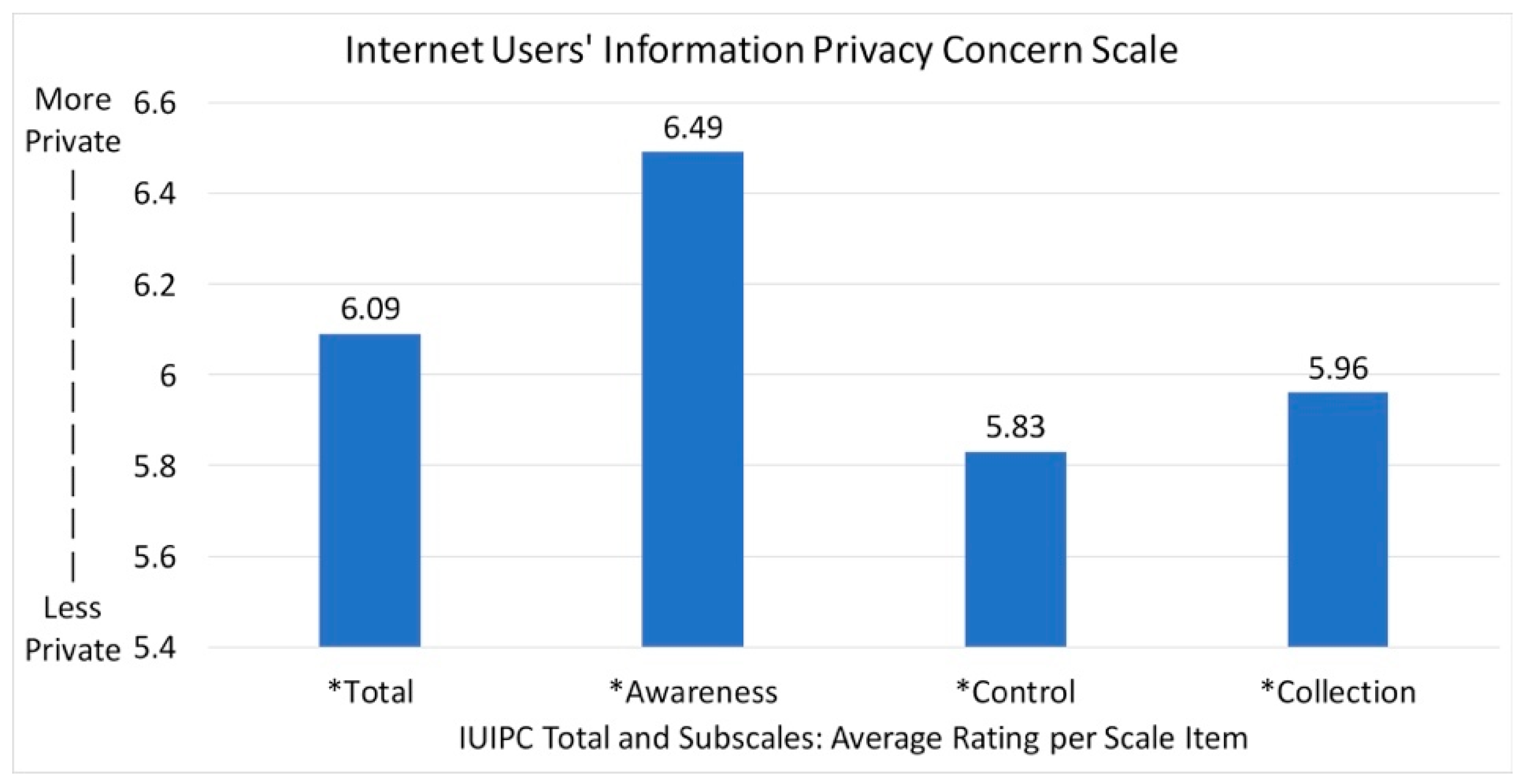
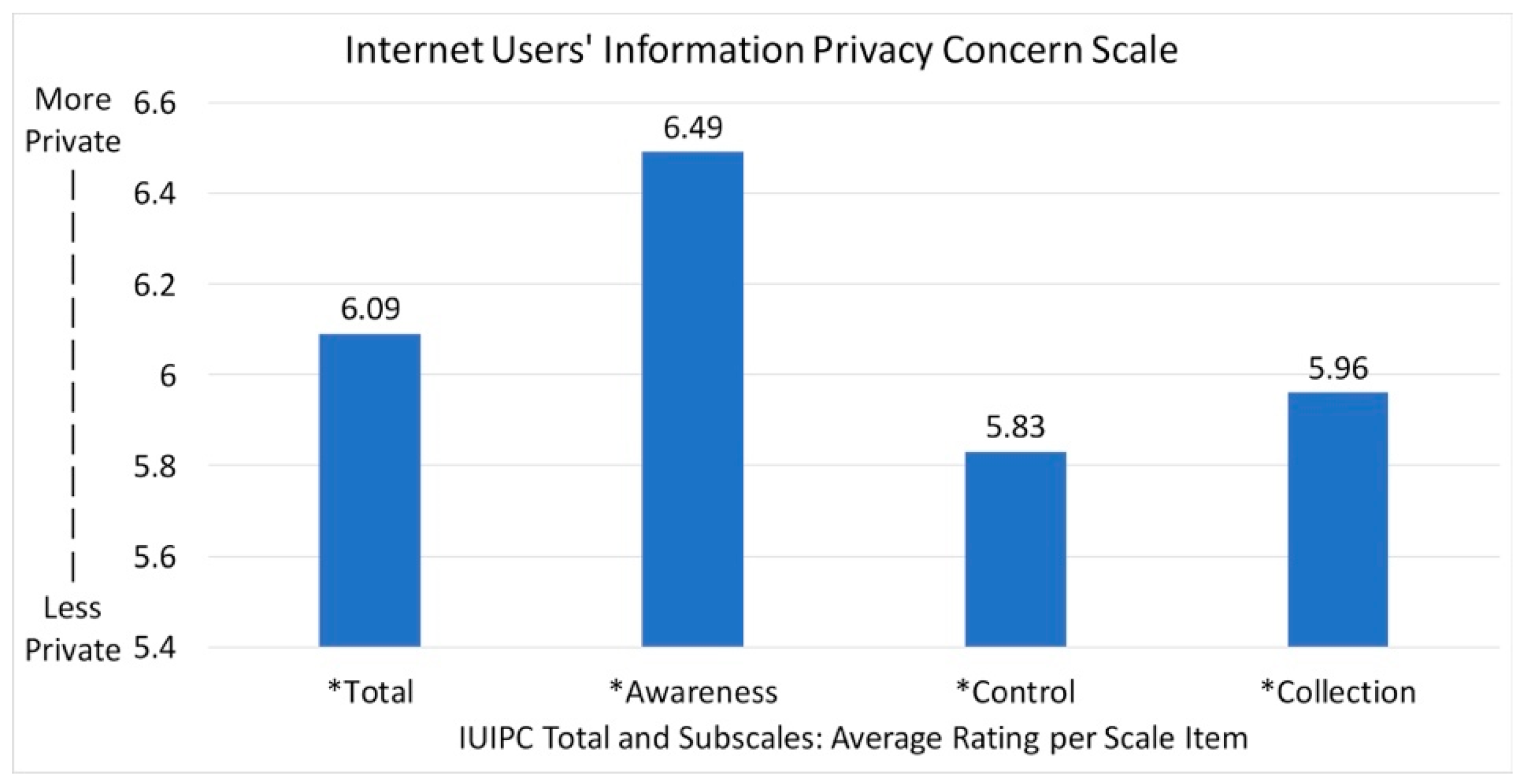
Internet Users’ Information Privacy Concerns (IUIPC)
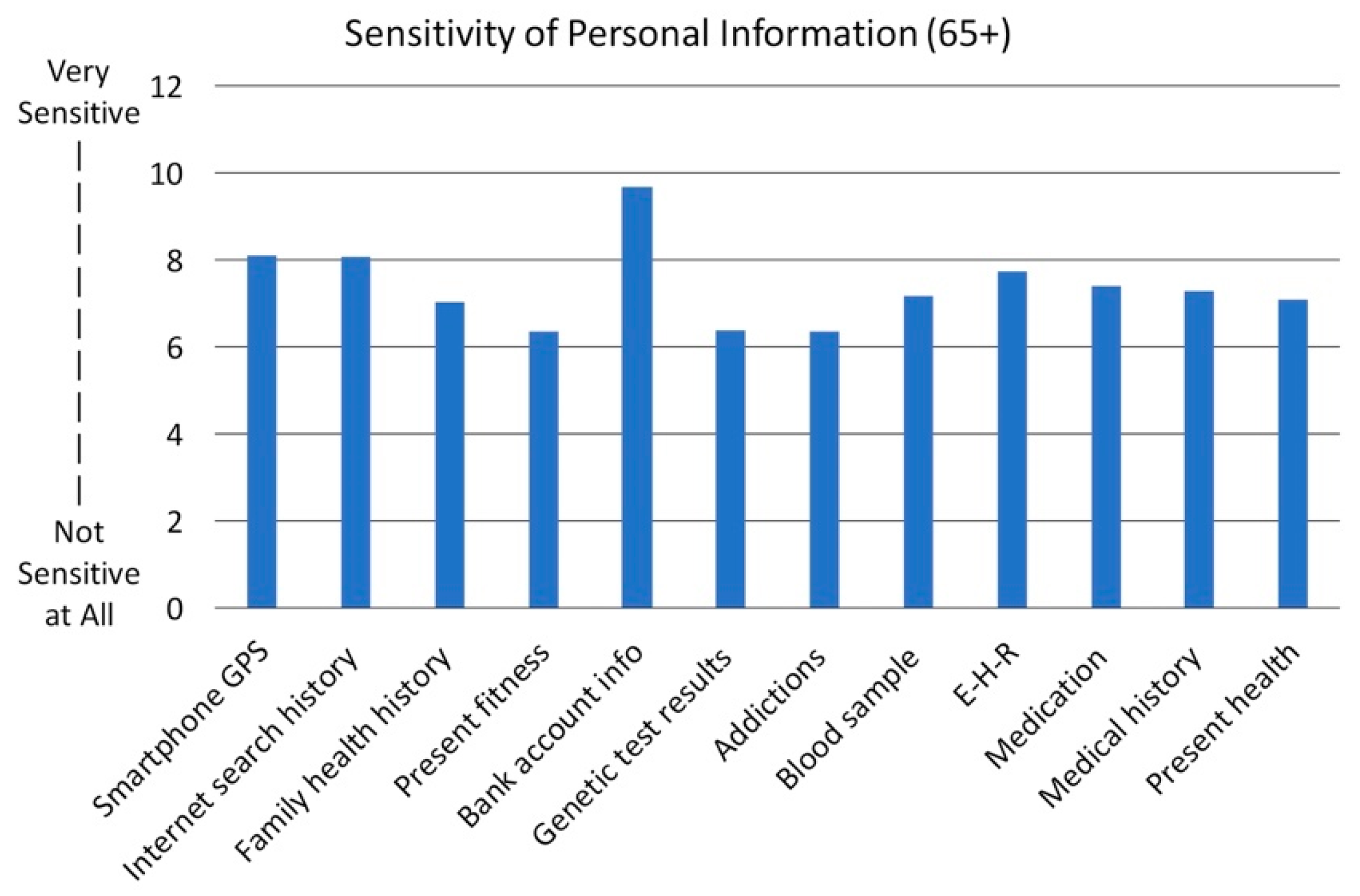
Data Sensitivity
2.3. Data Analysis
3. Results
3.1. Technology Usability
3.1.1. Lack of Unified Frameworks and User Interfaces
“To get email hooked up, to get this done, to get the keyboard… all that stuff, and a lot of folks just give up.”
“I’m going 160 days without backup because even the geek group that we have here can’t answer my question in order for me to get it set up.”
“I think technology can, for some people, get to the point where life is more difficult than it was before we had that technology.”“I have a smart phone. My kids think I can use this, but I don’t really know how to use this, and they bought it for me thinking it would be a great tool, but I don’t really know what to do with it.”
3.1.2. Increased Mobility and Visual Challenges When Using Technologies
“One of the biggest frustrations that I’ve seen was folks with power carts and a lot of them, to charge the battery, the plug is way down underneath your seat…. Couldn’t bend over to put it in, can’t see it…”
“I have had more calls from people who say, “I just put a brand-new battery and it doesn’t work.” They put the battery in backwards (laughter) and, at times, it burns out the unit.”
3.1.3. Recommendations for Improving Technology Usability
“Why don’t they have a senior version or an app that can get to on, off, volume up/down, channel, and make it kind of simple?”
3.2. Technology Literacy
3.2.1. Knowledge Barriers
“I know I’m looking for this connection, but I don’t know what it’s called, I don’t know what the things are, and so there is no … terminology, you know … um.”
“…I retired 20-something years ago, so I didn’t have the opportunity to work with them [technology] at work. So we got less work-based training on them and I don’t understand the language of it. Trying to hook a printer up to my laptop—they said to put in the IPP [sic IP] address. Uhh, I can’t find it… you know, and things like that, I don’t know what they are talking about.”
3.2.2. Recommendations for Improving Technology Literacy: Need for Resources
“Show me, slow down, and it’s hard to get ‘em to slow down. And you know, and I feel like I’m being a burden or they just don’t think Nana is smart enough. Maybe I’m not, but I could try to be if they were a little more patient.”
3.3. Data Management and Privacy
3.3.1. Data Collection and Use
“If they’re [the technology] so sensitive, they know three weeks before we know what’s going wrong with our bodies. It seems to me that that kind of information could really be compromised, and seniors could, uh, who are very vulnerable, could really be hoodwinked more easily.”
3.3.2. Return of Value
“You need to talk to your doctor about X, Y and Z. Um, but if you just keep gathering data and nothing happens to that data … um … except that you can look at it and … and you can’t really interpret it…”
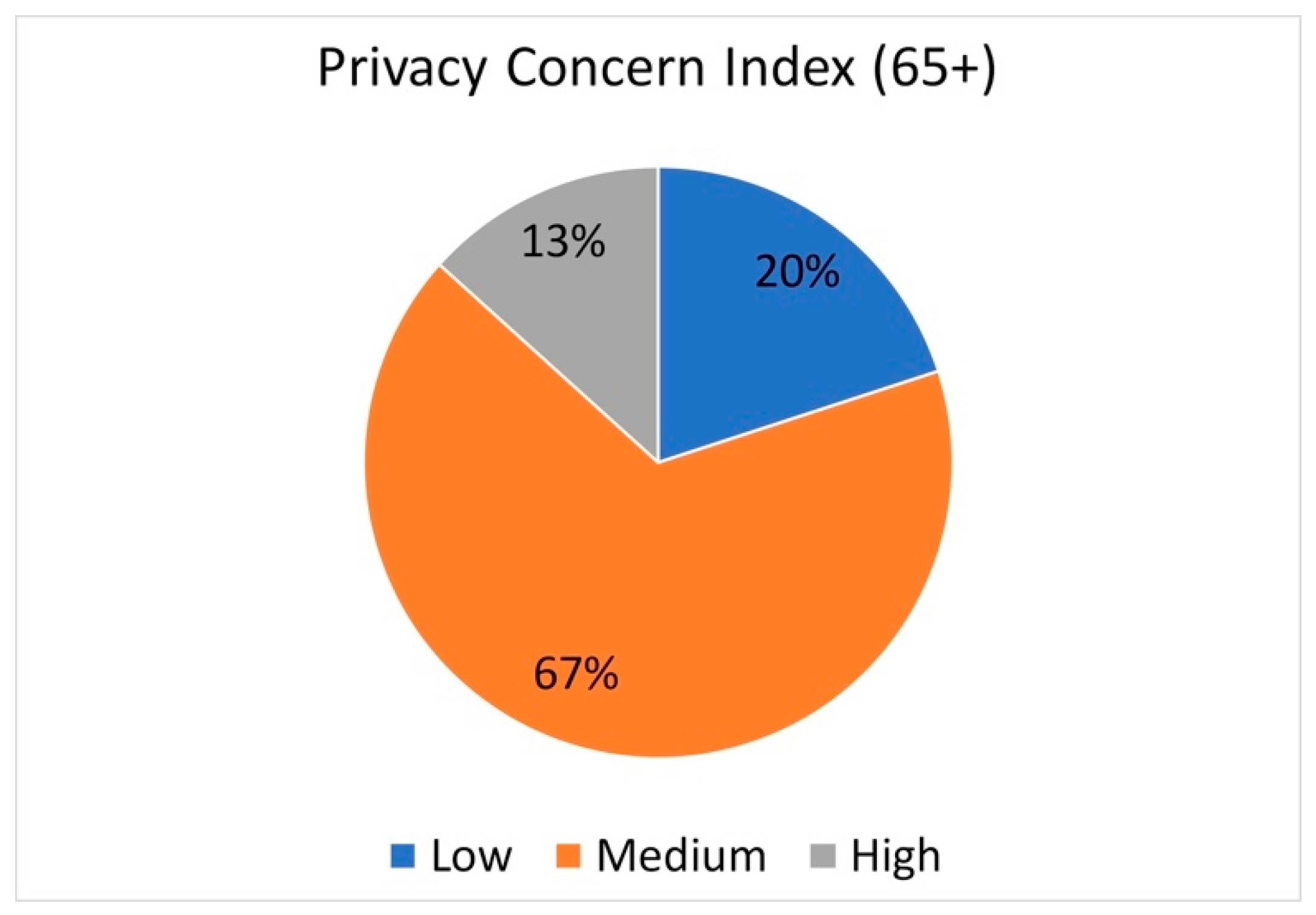
3.3.3. Privacy
Westin Privacy Concern Index
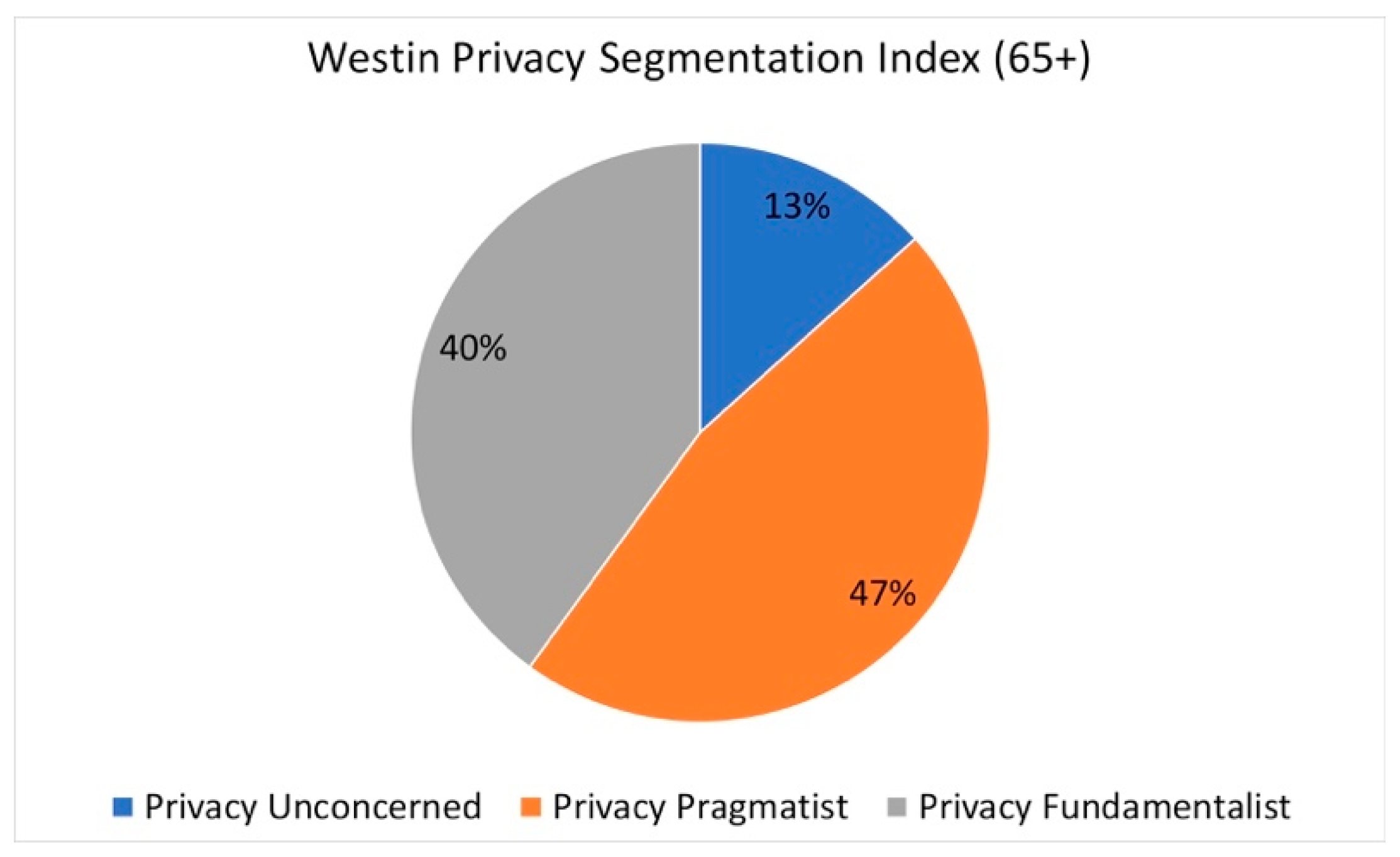
Westin Privacy Segmentation Index
“That’s fine, you can take all the data you want, I mean … but is it gonna be of benefit to me?”
“Well, I think if you can get some sort of readout that is, you know, available from the unit in your apartment, the status of where you are today, to be interactive in a sense, broadcasting the information that is … is collected about you and be analyzed by the artificial intelligence obviously to give you some kind of status, you know, you … you’re doing okay today or … or you ate too much yesterday.”
Internet Users’ Information Privacy Concerns (IUIPC):
Sensitivity to Personal Information
3.4. Co-Design of Technology
“… ethics and morality and seeing further from having lived longer that I think collective wisdom of the elderly might be extremely important in the checks and balances put in place.”“I think it’s a deal of bioethics. Sometimes the 85 and above have more human knowledge than the people working in the industry.”
“Why can’t there be a feature on the TV that I can get the sound to come straight to my hearing aid electronically?”“If they would come up with a universal remote that worked for the TV, for the iPhone … for everything so that you could program into it that you could remotely operate… I think that would solve some of the problems we all have.”
4. Discussion
4.1. Technology Usability
4.2. Software Interface
4.3. Data Control and Privacy
4.4. Implications for Creating Age-Friendly Communities
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
INTRODUCTION
- Welcome: Hello everyone! I’d like to thank you for accepting our invitation to participate in this focus group.
- Confidentiality: Your contributions to our discussion are important and Shengzhi will be taking notes to help us remember what we discuss today. To make sure we don’t forget anything, we are audio recording each session. In our transcript of the recording, we will not identify you by name and your responses will be confidential. Only members of our research team will have access to the recording, transcripts and our notes.
- Purpose: We are conducting this research as part of a UC San Diego Health Sciences project on technology-enabled health research. We’ve asked you here today to talk about how technology might be used to facilitate living independently. We are also interested in knowing how your think about your health information and privacy. In addition to asking you to respond to questions, I will also ask that you complete a survey which will take about 10 min.
- Consent: As with any research, you are free to ask questions at any time and your involvement is completely voluntary. If you have any concerns about being recorded or decide you don’t want to participate in this focus group, please know that you can leave at any time and there will be no hard feelings. To acknowledge your time and contributions, we will give you a $30.00 script that can be exchanged for cash at a local bank.
- So, to get started, I would like mention some basic instructions for how this works…This session will last about 90-min. Near the end of our time we will ask you to complete a survey. After that, we will give you a check that’s called “script” that you can take to the bank to exchange for cash.We are interested in your thoughts and opinions—there are no right or wrong answers here. We expect that there will be some areas where most people agree but, there will also be times when there is disagreement. That’s not a problem—we want to be respectful of each other’s opinions. Differences of opinion are expected so feel free to share yours even if it’s different.Please make sure everyone has a chance to chime in and please don’t interrupt each other!
- A.
- Curiosity about technology and connection to personal health
- 1.
- Digital technologies you currently useThere is growing interest in how digital technologies can be used to support healthy living and aging-in-place. To get started, I would like you to think about what “digital technologies” you use in your daily life.Feel free to use the 3 × 5 cards in front of you to jot down any thoughts you have.<Give 1-2 min to think>Okay, what are some of the technologies that you’re using?<Write key words identified by participants on butcher paper>Think back to a time when you felt that you’d like to use a technology like a smart phone app or Facebook and were not quite sure how to do it? Can you tell us about that?Think back to a time when you felt that using a technology or a smart phone app has made you feel great. Can you tell us about that?
- 2.
- Technology use over timeWe’ve talked a little about how we think about technology—we’re also curious about how your thoughts about technology has change over time.Is the way you think about using technology different than how your family might think about it?Why did you start using the technologies on your list? Why have you continued using them?
- 3.
- Health Practices and ToolsNow, we want to talk about how you keep yourself healthy.Think about the kinds of tools you use daily to track your health and to keep yourself healthy.Write those down on the index card.(Examples: hearing aids, blood sugar or blood pressure monitor, scale, exercise machines, fitness trackers, pill trackers (whether a box or a digital device), medication reminders, mail-order prescription delivery services, safe-alert buttons, diet/nutrition aids, electronic health record monitoring, canes, wheelchairs, etc.)Why do you use these tools or adopt these practices? How did you come to acquire them?Why do you keep using them?Think of a time that using your health practice or tool was frustrating, or when you struggled to use it correctly. Can you tell us about that?Think of a time that your health practices or tools has made you feel reassured, or safer. Can you tell us about that?How could keeping track of your health and keeping yourself healthy be made easier?What would make you feel confident transitioning adopting a new health practice or tool?
- 4.
- Health Data and PrivacyWith technology, there have been problems with handling of personal information and people are worried about their privacy.How would you describe the characteristics of a very private person?How about a not at all private person? Make notes on your 3 × 5 cardsDo you think privacy means something different today than say 30 years ago?Is the way you think about privacy different than how your family might think about it?Most people think about their health information being located in their electronic health record but, nowadays, our information is found on Facebook, Twitter as well as in sensor technologies and apps that we download onto our phones.There are now fitness devices and apps that can track your steps, diet and sleep as well as mood.Do you currently use any apps or wearable devices?What are you using and what do you like or dislike about it?These devices capture information that could be personal and health related.Would you want to control who has access to this information? Why or Why Not?Would you want to share information from your personal devices or apps with your doctor?What about with researchers like me?We are interested in using wearable sensors to learn about how people live in their everyday lives.Show a variety of devices (lumo, empatica, sensecam, authographer, garmin, fitbit)Wearable Sensors
- What do you think about the wearable camera? Would you wear it for a day or a week? What concerns would you have? What would motivate you to wear it?
- What do you think about the wrist worn devices? Would you wear it for a day or a week? What concerns would you have? What would motivate you to wear it?
- What do you think about the waist worn devices? Would you wear it for a day or a week? What concerns would you have? What would motivate you to wear it?
- What do you think of the overall design of these devices? Can you get it on/off easily? Is the information that is collected useful to you?
Home Sensors- What do you think about having sensors placed in your apartment that could alert you or a friend about how you’re doing?
Show examples of data produced. - B.
- Preferences for involvement in participatory design of intelligent assistive technologies
- 1.
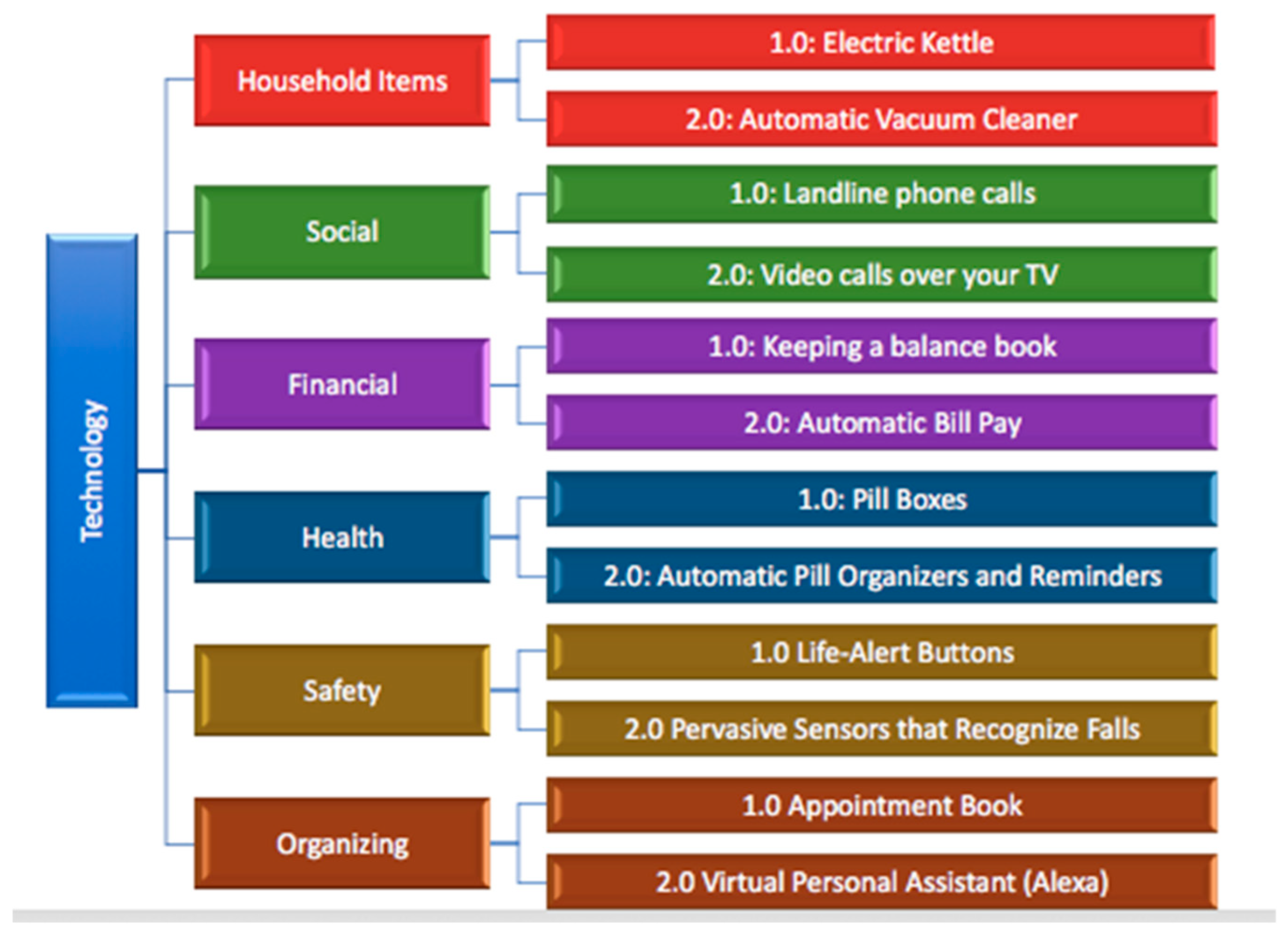
- Interest in co-designSome researchers are trying to make activities such as tracking your health, keeping you safe, taking care of your home, communicating with your family even easier with new technologies and tools. < Show figure of technologies >Figure A1. Technology by Domains.
![Healthcare 07 00060 g0a1]() Now, researchers, and especially engineers and technology developers, might think they know how to best help you, but they also need your input to make sure that they create products that actually fulfill your goals and are easy for you to use.Would you be interested in having conversations with technology makers to guide the design process of products that are specifically geared toward people in retirement communities?If you could develop technology to improve your life in any way, what would you develop?Do you have an idea of what it would look like? Could you draw a picture of it?
Now, researchers, and especially engineers and technology developers, might think they know how to best help you, but they also need your input to make sure that they create products that actually fulfill your goals and are easy for you to use.Would you be interested in having conversations with technology makers to guide the design process of products that are specifically geared toward people in retirement communities?If you could develop technology to improve your life in any way, what would you develop?Do you have an idea of what it would look like? Could you draw a picture of it? - 2.
- Familiarity with terms, concepts, and processes associated with the design of assistive technologies for aging in placeTerm 1: Aging in Place
- What does “aging in place” mean to you?
- What kinds of technologies do you think could support aging in place?
- What would “success” mean for the design of aids for aging in place?
Term 2: Participatory Design- Participatory design means that stakeholders are involved in the design of new products and devices. What do you think this means in practice?
- What can you contribute?
- How would you think of your role on the design team?
- What type of process would you want to feel like you a part of it?
Term 3: Assistive Technologies/Intelligent Assistive Technologies- <Show videos or prototypes, such as: https://www.smithsonianmag.com/innovation/how-will-artificial-intelligence-help-aging-180962682/>
- 3.
- Advice and preferences for how technology development experts should most effectively communicate such information to enable an authentic and informed participatory design processWe want to know how we could maximize your involvement in a participatory design process.How much time would you want to spend?Do you want to do it at your home, or do you want to meet elsewhere?How often can you fit this in?Would you be willing to test out devices while they are still in development? Why or why not?That’s the end of our session. Thank you for participating!
References
- Woolhead, G.; Calnan, M.; Dieppe, P.; Tadd, W. Dignity in older age: What do older people in the United Kingdom think? Age Ageing 2004, 33, 165–170. [Google Scholar] [CrossRef]
- Eckert, J.K.; Morgan, L.A.; Swamy, N. Preferences for receipt of care among community-dwelling adults. J. Aging Soc. Policy 2004, 16, 49–65. [Google Scholar] [PubMed]
- Matsumoto, H.; Naruse, T.; Sakai, M.; Nagata, S. Who prefers to age in place? Cross-sectional survey of middle-aged people in Japan. Geriatr. Gerontol. Int. 2016, 16, 631–637. [Google Scholar] [CrossRef]
- Boldy, D.; Grenade, L.; Lewin, G.; Karol, E.; Burton, E. Older people’s decisions regarding “ageing in place”: A Western Australian case study. Australas J. Ageing 2011, 30, 136–142. [Google Scholar] [CrossRef]
- Ball, M.M.; Perkins, M.M.; Whittington, F.J.; Connell, B.R.; Hollingsworth, C.; King, S.V.; Elrod, C.L.; Combs, B.L. Managing Decline in Assisted Living: The Key to Aging in Place. J. Gerontol. B Psychol. Sci. Soc. Sci. 2004, 59, S202–S212. [Google Scholar] [PubMed]
- Diehr, P.H.; Thielke, S.M.; Newman, A.B.; Hirsch, C.; Tracy, R. Decline in health for older adults: Five-year change in 13 key measures of standardized health. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1059–1067. [Google Scholar]
- González-Colaço Harmand, M.; Meillon, C.; Rullier, L.; Avila-Funes, J.-A.; Bergua, V.; Dartigues, J.-F.; Amieva, H. Cognitive decline after entering a nursing home: A 22-year follow-up study of institutionalized and noninstitutionalized elderly people. J. Am. Med. Dir. Assoc. 2014, 15, 504–508. [Google Scholar] [CrossRef]
- Task Force on Research and Development for Technology to Support Aging Adults. Emerging Technologies to Support an Aging Population; Committee on Technology of the National Science & Technology Council: Washington, DC, USA, 2019.
- Mihailidis, A.; Carmichael, B.; Boger, J. The use of computer vision in an intelligent environment to support aging-in-place, safety, and independence in the home. IEEE Trans. Inf. Technol. Biomed. 2004, 8, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Cody, M.J.; Dunn, D.; Hoppin, S.; Wendt, P. Silver surfers: Training and evaluating internet use among older adult learners. Commun. Educ. 1999, 48, 269–286. [Google Scholar] [CrossRef]
- Chiu, C.-J.; Hu, Y.-H.; Lin, D.-C.; Chang, F.-Y.; Chang, C.-S.; Lai, C.-F. The attitudes, impact, and learning needs of older adults using apps on touchscreen mobile devices: Results from a pilot study. Comput. Hum. Behav. 2016, 63, 189–197. [Google Scholar] [CrossRef]
- Wang, J.; Carroll, D.; Peck, M.; Myneni, S.; Gong, Y. Mobile and Wearable Technology Needs for Aging in Place: Perspectives from Older Adults and Their Caregivers and Providers. Stud. Health Technol. Inf. 2016, 225, 486–490. [Google Scholar]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inf. 2017, 101, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Aging Well in the 21st Century: Strategic Directions for Research on Aging. Available online: https://www.nia.nih.gov/about/aging-well-21st-century-strategic-directions-research-aging (accessed on 2 April 2019).
- Khosravi, P.; Ghapanchi, A.H. Investigating the effectiveness of technologies applied to assist seniors: A systematic literature review. Int. J. Med. Inform. 2016, 85, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Peek, S.T.M.; Wouters, E.J.M.; Luijkx, K.G.; Vrijhoef, H.J.M. What it Takes to Successfully Implement Technology for Aging in Place: Focus Groups with Stakeholders. J. Med. Internet Res. 2016, 18, e98. [Google Scholar] [CrossRef]
- Renaud, K.; Karen, B.J. Judy Predicting technology acceptance and adoption by the elderly: A qualitative study. In Proceedings of the ACM International Conference Proceeding Series, Wilderness, South Africa, 6–8 October 2008; Volume 338. [Google Scholar]
- Lorenz, A.; Oppermann, R. Mobile health monitoring for the elderly: Designing for diversity. Pervasive Mob. Comput. 2009, 5, 478–495. [Google Scholar] [CrossRef]
- Iwaya, L.H.; Gomes, M.A.L.; Simplício, M.A.; Carvalho, T.C.M.B.; Dominicini, C.K.; Sakuragui, R.R.M.; Rebelo, M.S.; Gutierrez, M.A.; Näslund, M.; Håkansson, P. Mobile health in emerging countries: A survey of research initiatives in Brazil. Int. J. Med. Inform. 2013, 82, 283–298. [Google Scholar] [CrossRef] [PubMed]
- Designing for Older Adults: Principles and Creative Human Factors Approaches, Second Edition. Available online: https://www.crcpress.com/Designing-for-Older-Adults-Principles-and-Creative-Human-Factors-Approaches/Fisk-Czaja-Rogers-Charness-Czaja-Sharit/p/book/9781420080551 (accessed on 23 March 2019).
- Scandurra, I.; Sjölinder, M. Participatory Design with Seniors: Design of Future Services and Iterative Refinements of Interactive eHealth Services for Old Citizens. Med. 2.0 2013, 2, e12. [Google Scholar] [CrossRef]
- Ritter, F.E.; Baxter, G.D.; Churchill, E.F. Foundations for Designing User-Centered Systems: What System Designers Need to Know about People; Springer: London, UK, 2014; ISBN 978-1-4471-5133-3. [Google Scholar]
- Zarem, J.E. Today’s Continuing Care Retirement Community (CCRC); LeadingAge: Washington, DC, USA; American Seniors Housing Association: Washington, DC, USA; National Investment Center: Annapolis, MD, USA, 2010. [Google Scholar]
- Kumaraguru, P.; Cranor, L.F. Privacy Indexes: A Survey of Westin’s Studies; Carnegie Mellon University: Pittsburgh, PA, USA, 2005. [Google Scholar]
- Malhotra, N.K.; Kim, S.S.; Agarwal, J. Internet users’ information privacy concerns (IUIPC): The construct, the scale, and a causal model. Inf. Syst. Res. 2004, 15, 336–355. [Google Scholar] [CrossRef]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine de Gruyter: Hawthorne, NY, USA, 1967; ISBN 978-0-202-30260-7. [Google Scholar]
- Willms, D.G.; Best, J.A.; Taylor, D.W.; Gilbert, J.R.; Wilson, D.M.C.; Lindsay, E.A.; Singer, J. A Systematic Approach for Using Qualitative Methods in Primary Prevention Research. Med. Anthropol. Q. 1990, 4, 391–409. [Google Scholar] [CrossRef]
- Golko, A.; Jol, E.; Schmidt, M.; Terlizzi, J. Dual Orientation Connector with Exteral Contacts and Conductive Frame. U.S. Patent US20130115821, 9 May 2013. [Google Scholar]
- Elueze, I.; Quan-Haase, A. Privacy Attitudes and Concerns in the Digital Lives of Older Adults: Westin’s Privacy Attitude Typology Revisited. Am. Behav. Sci. 2018, 62, 1372–1391. [Google Scholar]
- Westin, A.F. Intrusions Privacy tradeoffs in a free society. Public Perspect. 2000, 11, 8. [Google Scholar]
- Melenhorst, A.-S.; Rogers, W.A.; Caylor, E.C. The Use of Communication Technologies by Older Adults: Exploring the Benefits from the User’s Perspective. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2001, 45, 221–225. [Google Scholar] [CrossRef]
- Jeste, D.V.; Blazer, D.G.; Buckwalter, K.C.; Cassidy, K.-L.K.; Fishman, L.; Gwyther, L.P.; Levin, S.M.; Phillipson, C.; Rao, R.R.; Schmeding, E.; et al. Age-Friendly Communities Initiative: Public Health Approach to Promoting Successful Aging. Am. J. Geriatr. Psychiatry 2016, 24, 1158–1170. [Google Scholar] [PubMed]
- Davidson, J.L.; Jensen, C. What Health Topics Older Adults Want to Track: A Participatory Design Study. In Proceedings of the 15th International ACM SIGACCESS Conference on Computers and Accessibility, Bellevue, WA, USA, 21–23 October 2013; ACM: New York, NY, USA, 2013; pp. 26:1–26:8. [Google Scholar]
- Spinuzzi, C. The Methodology of Participatory Design. Tech. Commun. 2005, 52, 163–174. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (mean, SD) | 80.0 (6.2) |
| Gender (n, % female) | 20 (64.5%) |
| Highest education (n, %) | |
| Graduated from high school or GED completed | 4 (13.3%) |
| Graduated from 2-year college | 5 (16.7%) |
| Graduated from 4-year college | 6 (20.0%) |
| Completed some post-college education | 6 (20.0%) |
| Completed Master’s degree | 6 (20.0%) |
| Completed professional degree or Ph.D. | 3 (10.0%) |
| Ethnicity (n, %) | |
| Hispanic or Latino | 2 (6.5%) |
| Not Hispanic or Latino | 28 (90.3%) |
| NA | 1 (3.2%) |
| Race (n, %) | |
| Caucasian/White | 30 (96.8%) |
| Asian | 1 (3.2%) |
| Approximate annual household income (n, %) | |
| $50,000–$99,999 | 12 (40.0%) |
| $100,000–$149,999 | 14 (46.7%) |
| $150,000–$199,999 | 3 (10.0%) |
| $300,000 or more | 1 (3.3%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, S.; Bolling, K.; Mao, W.; Reichstadt, J.; Jeste, D.; Kim, H.-C.; Nebeker, C. Technology to Support Aging in Place: Older Adults’ Perspectives. Healthcare 2019, 7, 60. https://doi.org/10.3390/healthcare7020060
Wang S, Bolling K, Mao W, Reichstadt J, Jeste D, Kim H-C, Nebeker C. Technology to Support Aging in Place: Older Adults’ Perspectives. Healthcare. 2019; 7(2):60. https://doi.org/10.3390/healthcare7020060
Chicago/Turabian StyleWang, Shengzhi, Khalisa Bolling, Wenlin Mao, Jennifer Reichstadt, Dilip Jeste, Ho-Cheol Kim, and Camille Nebeker. 2019. "Technology to Support Aging in Place: Older Adults’ Perspectives" Healthcare 7, no. 2: 60. https://doi.org/10.3390/healthcare7020060
APA StyleWang, S., Bolling, K., Mao, W., Reichstadt, J., Jeste, D., Kim, H.-C., & Nebeker, C. (2019). Technology to Support Aging in Place: Older Adults’ Perspectives. Healthcare, 7(2), 60. https://doi.org/10.3390/healthcare7020060