Abstract
Prostate cancer is very common among men in the United States. The current literature on active surveillance (AS) suggests that it is a promising treatment option for men with low-risk prostate cancer. The purpose of this manuscript is to provide a thorough integrative review regarding the effects of AS on the quality of life (QoL) of men with prostate cancer. Utilizing a methodological strategy, electronic databases were reviewed for empirical articles during the time frame of January 2006 to December 2016. A total of 37 articles met the inclusion criteria wherein 20 focused on the QoL among men only receiving AS and 16 reported QoL among men undergoing AS and other forms of treatment for prostate cancer. The review highlights the purpose, common instruments, race and ethnicity, and strengths and limitations of each article. The majority of articles indicated low levels of anxiety and depression and decreased incidences of bladder, bowel and sexual functioning among men undergoing AS in comparison to men who received other treatment modalities. The results indicated that additional research is needed to determine the QoL among men receiving AS on a longitudinal basis. The results support previous literature that indicated the positive impact of AS on low-risk prostate cancer.
1. Introduction
Prostate cancer is the most common non-skin cancer found in American men [1,2]. Over the past three decades, prostate cancer diagnoses have risen dramatically [3]. The majority of men with prostate cancer remain clinically asymptomatic throughout their life [4]. Even though the data show that men diagnosed with prostate cancer typically die from reasons unassociated with their disease, most patients still opt for aggressive treatment [5]. Some of the common treatment options available for prostate cancer are brachytherapy, radiation, and radical prostatectomy. However, the common treatment options for prostate cancer bear specific risks that affect an individual′s quality of life (QoL) and/or health related quality of life (HRQoL) [6,7]. The invasive nature of some treatments leads to negative impacts on sexual, bowel, and urinary function, which in turn causes difficulties between those diagnosed with prostate cancer and their partners [6,7]. The one treatment option for prostate cancer that does not require chemotherapy, radiation, or surgery is active surveillance (AS) along with watchful waiting. At one time AS was underutilized, however, recent research indicates that it is increasingly used for prostate cancer in the United States [8,9,10,11]. Despite the benefits of AS as a treatment for prostate cancer, it remains an underutilized treatment modality in the United States (USA) [8].
1.1. Prostate Cancer
Prostate cancer is the sixth leading cause of cancer death worldwide [12]. In the USA, the estimated incidence of prostate cancer in 2016 was 180,890, which accounted for 21% of cancer diagnoses with regards to men [13]. The aggressive treatment of otherwise indolent prostate cancer tumors exposes individuals to potentially life altering side effects from the treatment [14]. Consequently, the potential for significant side effects from prostate cancer treatments led physicians to recommend AS as a treatment option [15].
In 2017, the American Cancer Society indicated that the 5-year relative survival rate for prostate cancer is 99%, which indicated that AS can be a promising treatment for nonaggressive forms of prostate cancer [2]. It is important to note that prostate cancer will progress. However, some tumors will progress at slower rates [3]. Therefore, in most cases, the tumor itself does not pose a threat to patients [5].
1.2. Active Surveillance
According to the American Cancer Society, AS is when the cancer is monitored carefully by a physician, which includes a prostate specific antigen test and a digital rectal exam every six months and prostate biopsies every year [2]. Active surveillance has been used interchangeably with the term “watchful waiting”. However, the literature indicated a separate distinction between the two terms. Watchful waiting, as a treatment for prostate cancer, is indicated for those with advanced prostate cancer, a limited life expectancy, and the goal of being palliative and not curative [8,16,17]. In contrast, AS, is individualized with a longer life expectancy and the goal of being curative if the cancer progresses [8,14,16,17,18].
During AS, the health care provider follows a protocol that does not involve surgery, chemotherapy, hormone treatment, or radiation to monitor the growth of the prostate cancer. The AS protocols vary among health care providers as there is no established protocol that is accepted by all health care providers. For example, research in Toronto Canada indicated an AS protocol which consisted of PSA testing every 3 months for 2 years, then every 6 months with a biopsy during the first year followed by every 3 to 4 years until age 80 [19]. The John′s Hopkins AS protocol included PSA testing and DRE every six months and a yearly prostate biopsy [19]. Despite the lack of treatments when AS is used, if signs of significant disease progression occur, the patient can undergo radical treatment at any time [20]. During AS, treatment is deferred until the tumor becomes clinically significant, which oftentimes never happens [3]. According to Surveillance, Epidemiology, and End Results and Medicare data, the use of AS rose from 9.7% in 2004 to 15.3% in 2007 [6]. In a study that examined the trends of prostate cancer treatment via Cancer of the Prostate Strategic Urologic Research Endeavor (CaPSURE) database, it was reported that AS use for low-risk disease increased from 6.7–14.3% from 1990–2009 to 40.4% from 2010–2013 [21]. Similarly, according to the American Urological Association Quality (AQUA) Registry, which included 47,288 prostate cancer patients from 2014–2016, AS rates for low-risk disease rose [22].
Research continues to examine whether AS is a safe treatment option with benefits for men with low-risk prostate cancer. Active surveillance was deemed as a safe alternative to radical treatment in a study that inquired whether anxiety and depression developed among men treated with AS2 [23]. Haymart and colleagues (2017) reported that the 5-year survival rate of nearly 100% for prostate cancer, along with the possible reduction in treatment side effects, indicated AS as a promising treatment for prostate cancer [24]. Similarly, in a comparison of radical prostatectomy, radiotherapy, and AS for prostate cancer, AS proved more beneficial for better sexual and urinary function in comparison to curative treatments [23]. Consequently, AS is a promising treatment option for those with low-risk prostate cancer which eliminates the need for radical treatments, which can cause anxiety and a decrease in QoL [25]. In the Prostate Cancer Intervention versus Observation Trial (PIVOT) study that followed patients for up to 20 years, radical prostatectomy all-cause mortality and prostate-cancer specific mortality were not significantly lower than observation in patients with localized prostate cancer (p = 0.06) [26]. It can be concluded that AS is a safe treatment option and that the risk of progression to metastatic disease and mortality is low. However, it is important to note that this depends on the low-risk classification protocol, which may vary slightly by institution. To date, the best treatment option for men with low-risk prostate cancer remains unclear [26]. Some of the ambiguity may arise from institutional differences in which patients meet the requirements for AS as a treatment option. The uncertainties regarding which treatment option is best strengthens the importance of this review, which further explores AS and its effects on QoL.
Active Surveillance among African Americans
It is important to note that while AS is a promising treatment option for patients with low-risk prostate cancer, African American men are affected at higher rates and have more aggressive forms of prostate cancer [27]. The mortality risk in African American men is reportedly 2.4 times that of White men [27]. Additionally, African Americans experience higher disease progression than their White counterparts [28]. This health disparity reduces the benefit of AS for African Americans living with prostate cancer because they are more likely to experience disease progression. While many studies have shown that AS has a decreased negative impact on QoL [6,29,30,31,32], most of them include less than 10% of African American men in their subject population [33]. Due to the disproportionately low numbers of African Americans in the studies, the results cannot be generalized to African American men [27]. Additionally, African Americans who chose to undergo AS were more likely to experience disease progression compared to White men [33]. It has been suggested that African Americans and other minority populations should have a more stringent criteria to qualify for AS [33].
1.3. Quality of Life
The mere diagnosis of cancer can significantly change the life of a patient and their family [34]. The thought of living with untreated cancer can possibly cause psychological distress and anxiety [35]. However, few studies have found significant negative psychological impacts for patients undergoing AS [34]. Quality of life and HRQoL are often used when comparing prostate cancer treatments [6]. Quality of life seemed to be the broad term that encompassed the physical and psychological aspects associated with treatment for prostate cancer, such as, urinary function and bother, sexual function and bother, bowel function and bother, and hormone function and bother [6,20,29]. The terms QoL and HRQoL are similar in that they are often used to gauge the psychosocial and physical outcomes of prostate cancer survivors. Follow up care for cancer survivors not only includes the treatment outcome, but also an overall improvement in their health in relation to their QoL [36]. For the purposes of the current review, QoL will be utilized as the overarching term for the physical and psychosocial outcomes associated with QoL and HRQoL prostate cancer survivors.
The concept of QoL is an essential aspect in the lives of prostate cancer survivors. Previous reviews regarding AS among prostate cancer survivors compared AS vs surgery and/or radiation, the psychosocial impact of AS on survivors and couples, and the under-utilization of AS [8,37,38,39]. However, there were a lack of integrative reviews, which is a methodology that allows for the inclusion of various types of studies as opposed to primarily only randomized clinical trials. Additional studies, which are long term in nature and consist of diverse patient samples, are needed for the continued examination of the impact of AS on the prostate cancer survivor′s QoL. The purpose of this paper is to provide an integrative review of the literature regarding the effects of AS as a treatment option for a prostate cancer survivor′s QoL.
2. Methods
2.1. Integrative Review Methodology
This study employed Whittemore and Knafl′s (2005) methodological strategies for conducting an integrative review [40]. The purpose of this integrative review was to synthesize the occurrence of literature regarding QoL among men receiving AS for prostate cancer between 2006 and 2016. Therefore, a quality appraisal was not implemented. The selected methodology of this review entailed a process of problem identification, literature search, data evaluation, data analysis, and presentation of the literature. This approach examined empirical, theoretical literature, and non-experimental studies related to the concept being researched. The inclusion of various types of literature, such as, theories, concepts, and pertinent issues within the healthcare arena is a benefit of integrative reviews. In addition, the method combined comprehensive searching with purposeful sampling to ensure all relevant literature was identified [40].
2.2. Search of the Databases
The electronic databases of Cinhal, Google Scholar, ProQuest, and PubMed were selected to examine the literature. The EMBASE database was not utilized in the review due to the University′s lack of subscription to the database. Each search of the databases utilized the key words “active surveillance”, “prostate cancer”, “cancer”, “quality of life”, and “health related quality of life”. The keywords were entered into each of the databases in different combinations that were established by the authors. The authors followed an identical format in searching the databases to ensure consistency with the data search. A search of the databases took place during January and April 2017 to capture relevant articles for the review. The inclusion criteria for this review were empirical or theoretical articles published between 2006 and 2016, written in the English language, and focused solely on the QoL factors of men undergoing AS as a treatment for prostate cancer. As indicated in the data abstraction process by Whittemore and Knafl (2005), the reference lists were also reviewed for inclusion. The study design was not a limitation of the review, which included quantitative, qualitative, mixed methods studies, and systematic reviews [40]. The exclusion criteria consisted of articles that were non-English, commentaries, dissertations, theses, editorials, letters to the editor, and books. Articles published outside of the time frame of 2006–2016 were excluded.
2.3. Data Analysis
The two authors independently evaluated the databases for articles that met the inclusion criteria. Each of the authors developed a table of their results and compared their findings. The results were used to determine which of the articles met the inclusion criteria and warranted further analysis to meet the objective of the review. Figure 1 represents a flow chart of the article selection process.
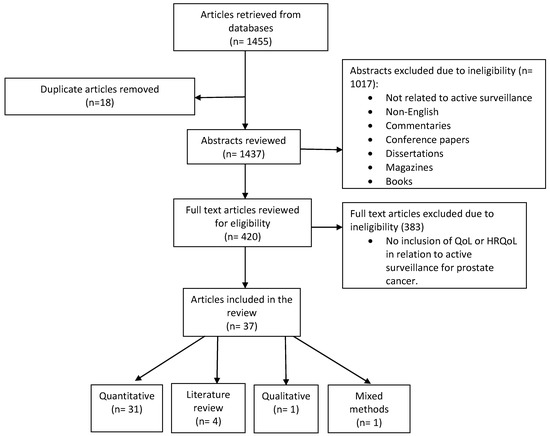
Figure 1.
Data flow chart of the article selection process.
3. Results
The current integrative review contained 37 peer reviewed empirical articles that examined the QoL among men undergoing AS for prostate cancer. A preliminary review of the abstracts from the selected electronic databases yielded 1455 articles. The authors compared and discussed their findings in each step of the data analysis in order to provide a thorough analysis. After the removal of duplicates (n = 18), the abstracts were screened (n = 1437) for inclusion in the review. Pertinent articles included studies that measured the physiological and psychological aspects of QoL among men receiving AS for prostate cancer. Upon review of the abstracts, 1017 were excluded (commentaries, books, non-English, etc.). Next, a review of the full text was implemented on the remaining articles (n = 420), in which four were identified from references and 383 did not meet the inclusion criteria (lack of AS in relation to QoL).
A thorough review of the remaining articles yielded a final count of 37 that met the inclusion criteria for the current review. An overview of the articles indicated that the majority were quantitative studies, i.e., a total of 31. Literature reviews were the next largest category (n = 4), followed by qualitative (n = 1), and mixed method (n = 1) articles. The selected articles were summarized in tables according to their theme (physiological and psychological). Each table included the author′s name, purpose, setting, design, race/ethnicity, methods, statistics, sample, response rate, reported instruments, key findings, strengths, and limitations. To minimize bias, two reviewers independently developed separate electronic spreadsheets of the articles that met the inclusion criteria for the integrative review. The reviewers discussed and compared their findings until a consensus was reached regarding the inclusion of the articles in the integrative review.
All the quantitative studies utilized validated surveys and questionnaires to gather information regarding QoL. The most commonly used questionnaires that measured QoL in the articles consisted of eight that measured QoL among prostate cancer survivors, the Expanded Prostate Cancer Index Composite (EPIC), five studies that used the Functional Assessment of Cancer Therapy-Prostate (FACT-P), and four that contained the European Organization for Research and Treatment of Cancer (EORTC) to name a few. Sexual function was a pertinent theme in the articles wherein six measured erectile dysfunctions with the International Index of Erectile Function (IIEF). Lastly, anxiety and depression were factors that influenced QoL among prostate cancer survivors receiving AS and six articles utilized the Hospital Anxiety and Depression Scale (HADS) to measure anxiety and depression. Overall, the questionnaires assessed various issues among the prostate cancer survivors such as anxiety, depression, physical strength, and their overall well-being as prostate cancer survivors.
A synopsis of the 37 articles reviewed indicated that 26 focused on the combination of the QoL factors of sexual, bladder, and bowel function, and anxiety and depression. The remaining 11 articles encompassed the QoL factors of anxiety and depression. Therefore, the data from the review was divided into two themes regarding QoL among AS articles: (1) combined physiological and psychological factors (sexual, bladder, bowel function, and anxiety and depression, and (2) only psychological factors (anxiety and depression).
The majority (86%; n = 32) of the articles in the review were non-experimental/cross-sectional, wherein there was only one randomized clinical trial (Lane, 2016). The sample size in the studies ranged from seven to 1643. The racial distribution of the studies consisted of mostly white men and revealed a significant lack of minority populations. For example, the racial distribution for the study conducted by Parker et al. (2016) was 86.1% White, 6.7% Black, 6.1% Hispanic, and 1.1% Asian [16]. Similar ratios regarding white and minority participants were found in other studies with less than 10% identified as minorities [41,42] or of a race that was not addressed in the studies [43,44,45,46,47,48].
The next sections of the integrative review will discuss the common QoL themes identified in the articles. Data from the two themes have been synthesized into two separate tables. The theme of combined physiological and psychological factors (sexual function, and bladder and bowel function, and anxiety and depression will be discussed first.
3.1. Sexual, Bladder, and Bowel Function and Anxiety and Depression Factors of QoL among Active Surveillance and Other Forms of Treatments
The current theme was comprised of articles that examined QoL through the factors of anxiety and depression, sexual function, and bladder and bowel functions of men who received AS and other forms of treatments for prostate cancer. A total of 26 articles were identified for the theme, which was comprised of 18 regarding sexual, bladder, and bowel function, six focused on a combination of anxiety, depression, sexual, bladder, and bowel function, one regarding only bladder and bowel function, and one focused on sexual function. Various studies examined the impact of non-AS treatment options on the prostate cancer survivors′ factors of sexual, bladder, and bowel function [6,29,31,32,45,46,49,50,51]. Common non-AS treatment options indicated in the articles consisted of, focal cryoablation, brachytherapy, external beam radiotherapy, and radical prostatectomy, which evaluated the effects of QoL on prostate cancer survivors [6,29,32,49,50,52]. The intimate topics of erectile dysfunction and sexual functioning were topics that surfaced and impacted the QoL of prostate cancer survivors.
3.1.1. Erectile and Sexual Function Factors of QoL among Active Surveillance and Other Forms of Treatments
When evaluating the sexual function of prostate cancer survivors, it would be remiss not to include erectile function. Erectile functioning emerged as a pertinent aspect of sexual functioning within the articles. For example, a study comparing focal cryoablation, brachytherapy, and AS reported men undergoing AS had lower mean scores on an erectile function questionnaire [46]. Donovan et al. (2015) compared AS to radical prostatectomy and radical radiotherapy and reported that erectile function decreased in all groups [31]. However, it decreased considerably more in the radical radiotherapy and radical prostatectomy groups. Similar results were found among a study that compared watchful waiting to brachytherapy and radiotherapy, primary hormonal therapy, and prostatectomy [32]. The study was comprised of participants that engaged in AS and watchful waiting. However, the researchers could not distinguish which of the treatments were used by the participants when treatment was deferred. Therefore, the researchers classified all the participants, whether they received AS or watchful waiting, as receiving watchful waiting. The results indicated that patients undergoing watchful waiting were less likely to report impotence, which was an indicator for measuring QoL [32].
In contrast, Pham et al. (2014) reported statistically significant (p < 0.05 at 1 year and 2 years) lower levels of erectile function among men receiving AS when compared to a control group which consisted of patients without prostate cancer [51]. Similarly, a study regarding the impact of prostate cancer biopsies among men receiving AS for prostate cancer indicated a small decrease in sexual function over time [53]. An additional study in the review that examined QoL among men only receiving AS also found a small decrease in sexual function which persisted every 6 months for 30 months [16]. A decrease in erectile and sexual function among prostate cancer survivors receiving AS was in the minority in the articles in the review.
The loss of sexual functioning has physiological and psychological implications on the QoL in the lives of men, as well as their partners. The decreased invasiveness of AS in the treatment of low-risk prostate cancer is a factor which promotes men maintaining erectile function. A comparison of AS to radical prostatectomy indicated men on AS had significantly better sexual functioning [6]. In a study that compared AS to brachytherapy and laparoscopic prostatectomy, sexual function decreased in 30% of patients on AS, 59% of patients who underwent brachytherapy, and 71% of patients who underwent laparoscopic prostatectomy [29]. Likewise, additional articles that examined QoL among men with localized prostate cancer reported sexual functioning as significantly better (p < 0.01) and there were higher scores for normal sexual functioning among those undergoing AS when compared to radical prostatectomy or radiation therapy [45,50]. However, the studies indicated that over an extended period, treatment modalities other than AS can offer the same degree of QoL among the issue of sexual functioning. Punnen et al. (2013) conducted a longitudinal study that compared AS to various treatment modalities, (radical prostatectomy, brachytherapy, external beam radiotherapy, and primary androgen deprivation therapy) to examine long term QoL [41]. The results suggested that QoL equalized over time. For example, despite an initial decreased QoL among the majority of the men in the study and decreased sexual function over the first two years among all forms of treatment, there was minimal change from three to ten years [41].
3.1.2. Bladder and Bowel Factors of QoL among Active Surveillance and Other Forms of Treatment
Bladder and bowel scores in relation to QoL were prevalent among many of the articles in the review that contained different modalities of treatment for prostate cancer. Concern regarding urinary functioning was a prevalent issue in the lives of prostate cancer survivors. Urinary function outweighed issues pertaining to sexual function for a cohort of men undergoing AS in Ireland [54]. In fact, uncertainty among urinary function showed no improvement after a five-week follow-up that occurred after an internet intervention to reduce uncertainty for men on AS [55]. In the study by Lokman et al. (2015), there was no decrease in the QoL regarding urinary function among men who received AS [56]. Similar results were found in one of the articles that reported no changes in urinary function or QoL among Finnish men receiving AS for prostate cancer [57]. A higher baseline score for urinary function among men receiving AS was reported in a study that compared QoL for men receiving AS and men who had negative biopsy results for prostate cancer [58]. However, using a model which estimated changes over time indicated a decrease in urinary function among the men who received AS [58]. A comparison of QoL among men receiving AS in Ireland and the USA revealed differences in urinary scores between the two populations [54]. The men from Ireland reported a higher mean (84.4) for urinary bother compared to (71.4) among men in the USA [54].
Along with concern regarding urinary function among prostate cancer survivors was the issue of bowel function within some of the articles in the review. Bowel and bladder function seemed to be inextricably linked as a factor for assessing QoL among men with prostate cancer. In a study that examined QoL among men receiving AS and radiation therapy, there were declines in QoL and worse bowel and urinary bother functions that yielded significant results, (p < 0.05) among men who received radiation therapy [59]. Quality of life regarding bowel and bladder function appeared to be maintained in a study among men who were treated with surgery, active monitoring, and radiotherapy [31]. Nevertheless, there were initial decreases in the QoL due to bladder and bowel issues during the first months of treatment that utilized surgery and radiotherapy [31]. In a comparison of QoL among men receiving AS for prostate cancer and men without prostate cancer, the results indicated a decline in bowel and urinary function for the men on AS [58]. However, the decline in men receiving AS was a comparison to men without cancer, which provided some insight into why bowel function scores may have been lower [58]. A five-year follow-up study among men undergoing AS revealed no changes among bowel function and other factors for QoL [60]. The study indicated that treatment may be linked to changes in bowel, urinary, and sexual function [60].
3.1.3. Combination of Physiological and Psychological Factors of QoL among Active Surveillance and Other Forms of Treatment
Lokman et al. (2013) examined the impact of AS on the QoL factors of erectile and urinary function among low-risk prostate cancer patients [56]. The results indicated there was no decrease in erectile or urinary function among the men after one or three years of follow-up [56]. A similar study also examined AS and QoL based on erectile and urinary function among low-risk prostate cancer survivors [57]. The study reported no significant changes in erectile and urinary function among prostate cancer survivors one year after following up. An additional article in the review found no significant difference in the QoL factors of sexual or urinary function among prostate cancer survivors, prior to and at the onset of receiving AS [61]. The findings from this review suggest that AS is positively related to the QoL factors of erectile and urinary function.
The combination of anxiety and decreased sexual functions were prevalent in the articles reviewed in the current review [16,57,58,60,61,62]. A study was conducted to examine the mental and physical QoL factors among Finnish men receiving AS for low-risk prostate cancer [57]. The QoL was not affected and anxiety did not cause the men to change their choice of treatment. In fact, the results were compared to the general population based on age, which indicated better overall mental and physical health among the men who received AS [57]. A first of its kind study in Australia examined QoL and anxiety among a cohort of men receiving AS for prostate cancer [61]. The QoL scores did not decrease and the men reported low levels of anxiety. Similar results were found in the review among the study by Seiler et al. (2012), which reported that men receiving AS exhibited low levels of anxiety and prostate cancer anxiety that were below the clinical levels. Additionally, the partners of the men receiving AS also experienced low distress and low levels of anxiety that were not significant [62]. Based on the results, one can surmise the prostate cancer patient′s QoL is impacted by the combination or separate factors of sexual function and anxiety.
Disease uncertainty, anxiety, and the fear of progress were also examined for a relationship among QoL and prostate cancer patients who received AS for prostate cancer. In the study, an inverse relationship existed among PSA scores and urinary and bowel QoL scores. Increased PSA scores were associated with decreased urinary and bowel scores. Similarly, as uncertainty scores increased, the QoL factors of urinary, bowel, sexual, hormonal, and satisfaction decreased. Lastly, increased anxiety predicted lower urinary, bowel, sexual, hormonal, and satisfaction QoL scores [16].
One of the recent largest studies in the United Kingdom examined patient reported outcomes (PROMS) from a randomized trial, Prostate Testing for Cancer Treatment (PROTEC T). The PROTEC T trial compared the use of AS, radical prostatectomy, and external beam radiotherapy with other segments of the population for the treatment of localized prostate cancer. Active surveillance was tied with radiotherapy as being the second largest category for treatment of prostate cancer, (n = 545), [30]. Obtaining the PROMS from patients with prostate cancer is essential for selecting the appropriate form of treatment and managing the impact of the treatment on their QoL [30]. Additionally, the PROMS provided an insight into the progression of the disease and the patient′s mortality from the disease [30]. The results from the PROTEC T indicated men on AS had the lowest scores for issues with sexual function (22.8%), lowest score for small overall sexuality problems (23%) and tied with all categories for big/moderate erectile problems (16%) [30]. However, results for anxiety, depression, health utility, mental, and physical health, were higher among the men receiving AS. The increased rates of anxiety and depression among receiving AS was also found in one of the articles included in the current review [42]. These findings indicated the negative impact that living with untreated prostate cancer can have on the QoL of men.
The results indicate the subjective nature of QoL among various populations of men along with the understanding that there is often a combination of factors, such as sexual, bladder, and bowel function and anxiety upon examining QoL among men with prostate cancer. Longitudinal research that assesses QoL among prostate cancer patients receiving AS will provide additional support for the benefits of receiving AS. The results of this section are presented in Table 1.

Table 1.
Sexual, bladder and bowel function and anxiety and depression among men utilizing active surveillance.
3.2. Anxiety and Depression Factors for QoL among Active Surveillance Treatment
The factors of anxiety and depression amongst patients receiving AS was a common theme throughout many of the articles. The psychological impact of living with prostate cancer has the potential to lead towards the development of anxiety and depression. There was a total of 11 studies that examined anxiety, prostate cancer specific anxiety, and depression among men who utilized AS. Additionally, all the studies were quantitative in methodology.
The most commonly used instruments to measure anxiety amongst the articles were the State-Trait Anxiety Inventory scale (STAI) and the Memorial Anxiety Scale for Prostate Cancer (MAX-PC). The STAI and MAX-PC were used in conjunction or separately in five studies. Depression was assessed most frequently with the Hospital and Anxiety Depression Scale (HADS) and/or Centre for Epidemiologic Studies Depression Scale (CES-D). Additionally, there were six studies that utilized the HADS and/or the CES-D in the studies.
3.2.1. Anxiety and Depression Factors for QoL among Men Only Receiving Active Surveillance
In an examination of anxiety among men on AS, a correlational study indicated that 86% of men on AS had low general anxiety and 87% reported low levels of prostate cancer-specific anxiety [66]. Similarly, van den Bergh et al. (2009) examined decisional conflict among those undergoing AS wherein 92% of the participants were below the reference values for clinical depression, and 83% were below the reference values for clinical anxiety [43]. Other studies pertaining to anxiety and AS in the review found their populations to have values below the reference values for prostate cancer-specific anxiety [43,61]. In the review, two studies also reported a correlation between anxiety, depression, and disease-specific anxiety [43,44]. The decreased psychological issues from AS provide promise for increased QoL among individuals undergoing AS instead of radical treatments [43].
Simpson (2014) conducted a review of the literature on AS and the impact of prostate cancer on the patient′s decision for treatment [65]. The results from the article indicated that prior to electing AS as a treatment for prostate cancer, patients must be psychologically prepared to monitor the cancer [65]. A series of studies that examined the impact of AS on individuals reported relatively low levels of anxiety, a decrease in anxiety over time, and the anxiety levels remained stable while on AS [16,44,47,67]. In a qualitative study, prostate cancer-specific anxiety decreased from the time of diagnosis to 18 months after diagnosis [47]. Van den Bergh et al. (2010) reported low levels of anxiety among patients receiving AS during the first nine months [44]. Despite depression remaining consistent for the patients on AS, there was no increase in depression after nine months. Low levels of anxiety and depression among individuals treated with AS provide promising results for individuals to maintain or improve their QoL. Similar results were found in the qualitative study by Frydenberg et al. (2013), which revealed 91% of men did not have anxiety and 87% had low levels of prostate cancer-specific anxiety [68]. Overall, the men reported high levels of QoL and low levels of anxiety for localized prostate cancer. It is important to note that the men in the study received a significant amount of patient education, which could have contributed to the low anxiety levels and increased QoL. However, there were two predictors which were significant for predicting QoL, younger age and an inherent anxiety trait.
There was an article that cited an increase in anxiety and depression among the men receiving AS as a treatment for prostate cancer. Watts et al. (2015) examined anxiety and depression in men undergoing AS for the treatment of prostate cancer. Clinical anxiety and depression were found to be 23% and 12.5%, respectively, among men receiving AS [42]. Previous data from men of the same age in the general population indicated rates of anxiety and depression to be 8% and 6%, respectively [42]. The results revealed rates of anxiety and depression that were twice as high among patients receiving AS compared to those without prostate cancer. For the most part, the articles in this review provided positive feedback for decreased rates of anxiety and depression among the men receiving AS for the treatment of prostate cancer.
3.2.2. Anxiety and Depression Factors for QoL among Active Surveillance and Other Forms of Treatments
Of the studies that compared the effects of AS to other forms of treatment for prostate cancer and the incidents of anxiety and depression, five examined anxiety and depression and one only examined anxiety. In addition, two studies found no significant differences in anxiety and depression levels between men who managed prostate cancer with only AS and those who underwent immediate radical treatment [35,41]. The articles within this integrative review examined the impact of AS and other forms of treatment for prostate cancer, such as, brachytherapy, radical prostatectomy, radical radiotherapy, and focal cryoablation [31,46] on QoL. Donovan et al. (2016) compared AS to radical prostatectomy and radical radiotherapy and found no significant differences in anxiety and depression between the groups [31]. Furthermore, Carter et al.′s (2015) systematic review regarding the psychological well-being and QoL among patients receiving AS and other forms of treatment for prostate cancer denoted no decrease in the psychological well-being of men receiving AS [69].
The results from the articles suggested that the majority of men on AS tended to report lower levels of anxiety and depression. However, the results were not inclusive of all the articles wherein some individuals on AS experienced higher levels of anxiety and depression compared with men receiving other forms of treatment for prostate cancer. The review cited articles that reported a contrast in results for higher levels of anxiety and depression [30,42,46]. De Cerqueira et al. (2015) conducted a study regarding anxiety and depression among prostate cancer survivors wherein participants on AS reported higher levels of anxiety and depression compared to participants that received brachytherapy and focal cryoablation [46]. Likewise, a large multisite study involving AS, QoL, and other forms of treatment in the United Kingdom indicated higher levels of anxiety and depression among the men who received AS [30].
The contrast in findings for higher levels of anxiety and depression among men receiving AS could be the result of psychological distress due to living with untreated cancer daily, which is one of possibly many reasons. The studies in the review highlight the need to examine the psychological issues encountered by men on AS. It is the examination of these issues which will provide additional data for identifying AS as a definitive, safe and beneficial treatment for prostate cancer. The results for this section in the review are presented in Table 2.
Table 2.
Anxiety and depression among men utilizing active surveillance.
4. Discussion
Research has shown that the determinants in the QoL of prostate cancer survivors were sexual, bladder, and bowel function [7,43,66]. It is not difficult to surmise that surgery and radiation treatments for prostate cancer have an adverse impact on sexual, bladder, and bowel function [7,46,49]. In essence, QoL is impacted by the treatment option for prostate cancer [46]. The findings from these articles address the sensitive issue of body image and the psychological impact it can have on men who encounter changes with their bladder function. An understanding of the impact of the various forms of treatment for prostate cancer can lead to interventions that meet the needs of men with decreased QoL. Interventions can also be developed that will maintain a sense of QoL among men receiving not only AS, but also other forms of treatment for prostate cancer. Furthermore, prostate cancer survivors must be aware of factors they will likely encounter if they choose curative treatments, such as radical prostatectomy, chemotherapy, and radiation treatment options.
An analysis of the articles included in the review indicated similar characteristics regarding the type of prostate cancer, use of questionnaires, and the study design. There was one stipulation that was consistent among the men who received AS for prostate cancer and it was the existence of low-risk prostate cancer. In essence, AS is not a curative form of treatment, which warrants its use only among localized low-risk prostate cancer. Despite some similarities in the characteristics among the articles, the varying types of studies caused difficulty in making comparisons. The concepts of QoL were similarly indicated by the factors of anxiety, depression, sexual, bladder, and bowel function. Within the articles in the current review, the concepts of QoL were predominately evaluated by questionnaires, such as, the EPIC, FACT-P, and the EORTC-QLQ-C30, except a qualitative study and one mixed methods study. The questionnaires were validated and were commonly found in the literature which evaluated QoL among individuals with prostate cancer. The disproportionately large number of quantitative articles in the current review did not allow for the evaluation of differences in QoL from questionnaires and interviews of prostate cancer patients receiving AS.
Sexual functioning of prostate cancer survivors is inextricably intertwined with the prostate cancer survivor′s QoL. In terms of sexual function, the majority of studies found men undergoing AS to experience fewer issues in sexual function when compared to other treatments [6,29,31,32,45,50]. However, a single study found that patients on AS presented with a higher rate for decreased erectile function when compared to patients who underwent focal cryoablation and brachytherapy [46]. A cause for the results may be attributed to age, in which older men may experience increased erectile dysfunction.
In the current literature regarding AS patients, the vast majority of the studies found low levels of anxiety, prostate cancer-specific anxiety, and depression [43,66]. Conversely, there were studies that found no significant differences in anxiety and depression when compared with other treatment modalities [31,35,41]. Overall, three studies found that men on AS presented with higher anxiety and depression levels [30,42,46]. Despite the studies reporting higher anxiety and depression levels among their low-risk prostate cancer survivors, it is difficult to compare the results from these very different studies. De Cerqueira et al. (2015), unlike Lane et al. (2016), had a small sample size (30 vs. 1438) and did not involve multiple sites [30,46]. Watts et al. (2015) had a medium sample size of 426 and was also multicenter with comparisons to the general population [42]. Furthermore, different questionnaires were used in the studies to assess anxiety, the Beck Anxiety Inventory [46] and the Hospital Anxiety and Depression Scale [30,42]. The types of treatments were also different, which included a combination of AS, focal cryoablation, and brachytherapy [46] and AS, radical prostatectomy and external-beam conformal radiotherapy [30]. These findings, while limited in number, indicate the need for continued research regarding the mental health of low-risk prostate cancer survivors. It cannot be assumed that a diagnosis of low-risk prostate cancer excludes the possibility of mental distress among these men.
The various themes identified in the review also included the comparison and evaluation of one or more factors associated with QoL and treatment for prostate cancer concurrently. It is apparent in a study published after the review (2017), which examined QoL among individuals with prostate cancer [70]. The results indicated that, after three years, the individuals who received a radical prostatectomy or external beam radiation had decreased sexual functioning and increased urinary incontinence compared to those who received AS. The invasive nature of surgery and the effects of radiation were far more detrimental, than AS, to the physiological functioning of men with prostate cancer. The decreased sexual functioning and increased urinary incontinence with the treatments other than AS matched the majority of results indicated in the current review. Similar results were reported in a two-year study, also published after the review that examined the impact of radical prostatectomy, radiation, brachytherapy, and AS on individuals with localized prostate cancer. In this study, radical prostatectomy had the highest rates of decreased sexual functioning and urinary incontinence compared to AS [71]. Additionally, radiation and brachytherapy treatment were commonly associated with urinary obstruction among the men in the study through two years. The large study in the United Kingdom, PROTEC T, also consisted of varying treatments and factors for QoL [30]. Symptoms from bowel and urinary issues were infrequent and older men had worse scores for urinary and sexual function. Only 1/5 of participants indicated problems with anxiety and depression.
Active surveillance is recommended as a treatment option for low-risk prostate cancer. However, based on the literature, African Americans and other minority populations are not well represented in the current research. Due to the lack of diversity in the research, it is difficult to generalize these findings to all populations [35]. One of the articles in the review focused solely on the utilization of AS among African American men with prostate cancer [64]. The results indicated an uncertainty for implementing AS among this population. This gap calls for more research on QoL among African American prostate cancer patients.
Overall, the results from the current review suggested that AS has a decreased negative impact on QoL when compared to other forms of treatment for prostate cancer. It could be that the decreased negative impact from AS on the QoL of prostate cancer survivors is due to the indications for the use of AS among low-risk prostate cancer. Men with low-risk prostate cancer may also perceive their health and diagnosis as less severe than an individual with advanced prostate cancer. A positive perception on health maybe a contributing factor into how they view their symptoms or even report the presence of symptoms. The thought of surgery, chemotherapy, and radiotherapy along with the recovery period and possible side effects can certainly be an area of concern and distress for any individual. Furthermore, men of older age tend to be diagnosed with prostate cancer and it is this older age that may lead to an improved outlook on life. The decreased side effects from AS indicate its use as an option for low-risk prostate cancer with a limited impact on QoL. There were only a few articles that indicated a negative impact on the QoL factors (sexual function, urinary continence, anxiety, and depression) [16,31,42,46,51,53] among men receiving AS while a limited number reported no change in the QoL factors for those that received AS [54,57]. Most of the articles reported declines in sexual functioning due to erectile dysfunction, bladder incontinence, bowel bother, anxiety, and depression among prostate cancer survivors who received a radical prostatectomy, radiation, or chemotherapy. The results corresponded with additional studies that evaluated the impact of various forms of treatment for prostate cancer on the individual′s QoL.
5. Clinical Implications
The results from the study build upon the platform of research in which healthcare providers can offer AS as a beneficial treatment among their low-risk prostate cancer patients. Despite many prostate cancer patients who acquire knowledge of AS from the internet [63], healthcare providers must also be a pertinent source for education regarding AS. Healthcare providers will benefit by engaging in open and clear conversations regarding the side effects and pros and cons of treatment modalities for low-risk prostate cancer. Transparent communication is needed for what may be considered a sensitive topic, prostate cancer, and healthcare providers are in a prime role to lead the conversations. The dissemination of this information can strengthen patient and healthcare provider relations along with the possibility of encouraging communication among family members and friends for support. Psychosocial support is known to be an essential component of comprehensive care of cancer patients and should consequently be examined [41]. Based on the articles listed in this review, knowledge seems to be increasing regarding the the benefits and effects of AS within the context of QoL, whereas prostate cancer research among minority populations is clearly lacking. Additional research is needed to establish the impact of living with untreated prostate cancer on the QoL of the men. Further investigation of the PROMs of men on AS is a promising avenue for identifying factors relevant to their QoL. Through continued research, interventions can be developed to provide support, education, and interventions for maintaining or improving the QoL for men of various ethnic and racial backgrounds who undergo AS.
6. Strengths and Limitations
The current integrative review strengthens the literature for studies focused on the impact of AS on the QoL for prostate cancer survivors. A focus on AS is a relevant topic in the field of prostate cancer given the increased exposure as a promising treatment for low-risk prostate cancer. The inclusion of various scholarly databases provided a diverse number of peer reviewed articles for inclusion in the review. Only empirical or theoretical articles were included in the review, which strengthened the acceptance of the credibility of the results from the articles included in the review. The use of two reviewers to collect, analyze, and organize the data allowed for a check and balance system for the inclusion of articles in the review. Overall, the review provides a breadth of knowledge on themes that many men find difficult to discuss. An awareness of the issues can ignite discussions and cause men to seek counseling or support for issues they once thought were taboo or too sensitive.
The limitations of the integrative review are centered on studies that were not listed in the databases used in this review. Two reviewers were used to assist with a thorough review. However, the use of keywords may have also been a limitation in the review. Articles may have been excluded from the review due to the arrangement of the keywords used to search the databases. Furthermore, the inclusion timeframe for the studies excluded studies from this review.
7. Conclusions
Through the use of a structured process, for conducting an integrative review, the factors of bladder, bowel, and sexual function, and anxiety and depression were identified as pertinent issues which impact the QoL among PCa survivors receiving AS. To date, there is not an integrative review focused solely on the concept of QoL among PCa survivors receiving AS. Within the 37 articles in the review, the majority used a quantitative design and mainly focused on QoL among the PCa survivors who received only AS as their form of treatment. A key attribute among the articles in the review was the commonality of low-risk PCa among the survivors that received AS. In general, there were higher levels of sexual, bladder, and bowel functioning and lower levels of anxiety and depression among those that received AS. Findings from the review were supported by similar studies regarding QoL among PCa survivors that received AS. However, there were a small number that indicated higher levels of anxiety and depression and lower levels of sexual, bladder, and bowel functioning. These findings could be attributed to the survivors knowingly living with PCa without receiving curative treatment. In essence, the review provided promising results for AS as a source of treatment that produced a positive impact on the PCa survivor’s QoL. The lack of racial and ethnic diversity among the participants in the studies and the variety of studies caused difficulty with making comparisons among the studies. However, the variety also provided insight into different methodologies to examine the concept of QoL among PCa survivors receiving AS as a form of treatment.
Funding
This research received no external funding.
Acknowledgments
We wish to acknowledge the University for the ease and access of the various databases utilized in the review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Daniyal, M.; Siddiqui, Z.A.; Akram, M.; Asir, H.M.; Sultana, S.; Khan, A. Epidemiology, etiology, diagnosis and treatment of prostate cancer. Asian Pac. J. Cancer Prev. 2014, 15, 9575–9578. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. American Cancer Society Medical and Content Team Survival rates for prostate cancer. American Cancer Society Statistics Center. 2016. Available online: https://www.cancer.org/cancer/prostate-cancer/detection-diagnosis-staging/survival-rates.html (accessed on 6 August 2017).
- Albertsen, P.C. When is active surveillance the appropriate treatment for prostate cancer? Acta Oncol. 2010, 50, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Bangma, C.H.; Bul, M.; van der Kwast, T.H.; Pickels, T.; Korfage, I.J.; Hoeks, C.M.; Steyerberg, E.W.; Jenster, G.; Kattan, M.W.; Bellardita, L.; et al. Active surveillance for low-risk prostate cancer. Crit. Rev. Oncol. Hematol. 2013, 85, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Dall′Era, M.A.; Albertsen, P.C.; Bangma, C.; Carroll, P.R.; Carter, H.B.; Cooperberg, M.R.; Freedland, S.J.; Klotz, L.H.; Parker, C.; Soloway, M.S. Active surveillance for prostate cancer: A systematic review of the literature. Eur. Urol. 2012, 62, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Jeldres, C.; Cullen, J.; Hurwitz, L.M.; Wolff, E.M.; Levie, K.E.; Odem-Davis, K.; Johnston, R.B.; Pham, K.N.; Rosner, I.L.; Brand, T.C.; et al. Prospective quality-of-life outcomes for low-risk prostate cancer: Active surveillance versus radical prostatectomy. Cancer 2015, 121, 2465–2473. [Google Scholar] [CrossRef] [PubMed]
- Sanda, M.G.; Dunn, R.L.; Michalski, J.; Sandler, H.M.; Northouse, L.; Hembroff, L.; Lin, X.; Greenfield, T.K.; Litwin, M.S.; Saigal, C.S.; et al. Quality of life and satisfaction with outcome among prostate-cancer survivors. N. Engl. J. Med. 2008, 358, 1250–1261. [Google Scholar] [CrossRef] [PubMed]
- Carter, H.B. Active surveillance for prostate cancer: An underutilized opportunity for reducing harm. J. Natl. Cancer Inst. Monogr. 2012, 175, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Drost, F.H.; Rannikko, A.; Valdagni, R.; Pickles, T.; Kakehi, Y.; Remmers, S.; van der Poel, H.G.; Bangma, C.H.; Roobol, M.J. Can active surveillance really reduce the harms of overdiagnosing prostate cancer? A reflection of real life clinical practice in the PRIAS study. Transl. Androl. Urol. 2018, 1, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Tosoian, J.J.; Carter, H.B.; Lepor, A.; Loeb, S. Active surveillance for prostate cancer: Current evidence and contemporary state of practice. Nat. Rev. Urol. 2016, 13, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L. Active surveillance for low-risk prostate cancer. Curr. Opin. Urol. 2017, 27, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Otero, J.R.; Gómez, B.G.; Ojeda, J.M.; Rodríguez-Antol, A.; Vilaseca, A.; Carlsson, S.V.; Touije, K.A. Active surveillance for prostate cancer. Int. J. Urol. 2016, 23, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA: A Cancer J. Clin. 2016, 66, 7–30. [Google Scholar]
- Klotz, L. Active surveillance for prostate cancer: A review. Curr. Urol. Rep. 2010, 11, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Davison, B.J.; Oliffe, J.L.; Pickles, T.; Mroz, L. Factors influencing men undertaking active surveillance for the management of low-risk prostate cancer. Oncol. Nurs. Forum 2009, 36, 89–96. [Google Scholar] [CrossRef]
- Parker, P.A.; Davis, J.W.; Latini, D.M.; Baum, G.; Wang, X.; Ward, J.F.; Kuban, D.; Frank, S.J.; Lee, A.K.; Logothetis, C.J. Relationship between illness uncertainty, anxiety, fear of progression and quality of life in men with favorable-risk prostate cancer undergoing active surveillance. Br. J. Urol. Int. 2016, 117, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Ganz, P.A. National Institutes of Health State-of-the-Science Conference: Role of active surveillance in the management of men with localized prostate cancer. Ann. Intern Med. 2012, 156, 591–595. [Google Scholar] [CrossRef]
- Morash, C. Active surveillance for the management of localized prostate cancer: Guideline recommendations. Can. Urol. Assoc. J. 2015, 9, 171–178. [Google Scholar] [CrossRef]
- Tosoian, J.J.; Loeb, S.; Epstein, J.I.; Turkbey, B.; Chokye, P.; Schaeffer, E.M. Active surveillance of prostate cancer: Use, outcomes, imaging, and diagnostic tools. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e235–e245. [Google Scholar] [CrossRef] [PubMed]
- Cooperberg, M.R.; Carroll, P.R.; Klotz, L. Active surveillance for prostate cancer: Progress and promise. J. Clin. Oncol. 2009, 29, 3669–3676. [Google Scholar] [CrossRef] [PubMed]
- Cooperberg, M.R.; Carroll, P.R. Trends in management for patients with localized prostate cancer, 1990-2013. J Am. Med. Assoc. 2015, 314, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Cooperberg, M.; Fang, R.; Wolf, J.S.; Hubbard, T.; Pendharkar, S.; Gupte, S.; Ross, K.; Nolin, M.; Schlossberg, S.; Clemens, J.Q. The current management of prostate cancer in the United States: Data from the AQUA registry. J. Urol. 2017, 197, e911–e912. [Google Scholar] [CrossRef]
- Venderbos, L.; Aluwini, S.; Roobol, M.; Bokhorst, L.P.; Oomens, E.H.; Bangma, C.H.; Korfage, I.J. Long-term follow-up after active surveillance or curative treatment: Quality-of-life outcomes of men with low-risk prostate cancer. Qual. Life Res. 2017, 26, 1635–1645. [Google Scholar] [CrossRef] [PubMed]
- Haymart, M.R.; Miller, D.C.; Hawley, S.T. Active surveillance for low-risk cancers—A viable solution to overtreatment? N. Engl. J. Med. 2017, 377, 203–206. [Google Scholar] [CrossRef]
- Tavlarides, A.M.; Ames, S.C.; Diehl, N.N.; Joseph, R.W.; Erik, P.; Castle, E.P.; David, D.; Thiel, D.D.; Broderick, G.A.; Parker, A.S. Evaluation of the association of prostate cancer-specific anxiety with sexual function, depression and cancer aggressiveness in men 1 year following surgical treatment for localized prostate cancer. Psycho-Oncology 2013, 22, 1328–1335. [Google Scholar] [CrossRef] [PubMed]
- Wilt, T.J.; Jones, K.M.; Barry, M.J.; Andriole, G.L.; Culkin, D.; Wheeler, T.; Aronson, W.J.; Brawer, M.K. Follow-up of prostatectomy versus observation for early prostate cancer. N. Engl. J. Med. 2017, 377, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.; Fan, Y.; Jarosek, S.; Adejoro, O.; Chamie, K.; Konety, B. Racial disparities in active surveillance for prostate cancer. J. Urol. 2017, 197, 342–3493. [Google Scholar] [CrossRef]
- Odom, B.D.; Mir, M.C.; Hughes, S.; Senechal, C.; Santy, A.; Eyraud, R.; Stephenson, A.J.; Ylitalo, K.; Miocinovic, R. Active surveillance for low-risk prostate cancer in African American men: A multi-institutional experience. Urology 2014, 83, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Acar, C.; Schoffelmeer, C.; Tillier, C.; de Blok, W.; van Muilekom, E.; van der Poel, H.G. Quality of life in patients with low-risk prostate cancer. A comparative retrospective study: Brachytherapy versus robot-assisted laparoscopic prostatectomy versus active surveillance. J. Endourol. 2014, 28, 117–124. [Google Scholar] [CrossRef]
- Lane, A.; Metcalfe, C.; Young, G.J.; Peters, T.J.; Blazeby, J.; Avery, K.N.; Dedman, D.; Down, L.; Mason, M.D.; Neal, D.E.; et al. Patient-reported outcomes in the ProtecT randomized trial of clinically localized prostate cancer treatments: Study design, and baseline urinary, bowel and sexual function and quality of life. BJU Int. 2016, 118, 869–879. [Google Scholar] [CrossRef]
- Donovan, J.L.; Hamdy, F.; Lane, M.; Mason, M.; Metcalfe, C.; Walsh, E.; Blazeby, J.M.; Peters, T.J.; Holding, P.; Bonnington, S.; et al. Patient-reported outcomes after monitoring, Surgery, or radiotherapy for prostate cancer. N. Engl. J. Med. 2016, 375, 1425–1437. [Google Scholar] [CrossRef]
- Kasperzyk, J.; Shappley, W.; Kenfield, S.; Mucci1, L.A.; Kurth, T.; Ma, J.; Stampfer, M.J.; Sanda, M.G. Watchful waiting and quality of life among prostate cancer survivors in the physicians′ health study. J. Urol. 2011, 186, 1862–1867. [Google Scholar] [CrossRef]
- Pietzak, E.J.; Van Arsdalen, K.; Patel, K.; Malkowicz, S.B.; Wein, A.J.; Guzzo, T.J. Impact of race on selecting appropriate patients for active surveillance with seemingly low-risk prostate cancer. Urology 2015, 85, 436–441. [Google Scholar] [CrossRef]
- Bastian, P.J.; Carter, H.B.; Bjartell, A.; Seitz, M.; Stanislaus, P.; Montorsi, F.; Stief, C.G.; Schröder, F. Insignificant prostate cancer and active surveillance: From definition to clinical implications. Eur. Urol. 2009, 55, 1321–1332. [Google Scholar] [CrossRef]
- Burnet, K.L.; Parker, C.; Dearnaley, D.; Brewin, C.R.; Watson, M. Does active surveillance for men with localized prostate cancer carry psychological morbidity? Br. J. Urol. Int. 2007, 100, 540–543. [Google Scholar] [CrossRef]
- Sægrov, S. Health, quality of life and cancer. Int. Nurs. Rev. 2005, 52, 233–240. [Google Scholar] [CrossRef]
- Simpkin, A.J.; Tilling, K.; Martin, R.M.; Lane, J.A.; Hamdy, F.C.; Holmberg, L.; Neal, D.E.; Metcalfe, C.; Donovan, J.L. Systematic review and meta-analysis of factors determining change to radical treatment in active surveillance for localized prostate cancer. Eur. Urol. 2015, 67, 993–1005. [Google Scholar] [CrossRef]
- Whiting, P.F.; Moore, T.H.M.; Jameson, C.M.; Davies, P.; Rowlands, M.; Burke, M.; Beynon, R.; Savovic, J.; Donovan, J.L. Symptomatic and quality-of-life outcomes after treatment for clinically localized prostate cancer: A systematic review. BJU Int. 2016, 118, 193–204. [Google Scholar] [CrossRef]
- Bellardita, L.; Valdagni, R.; van den Bergh, R.; Randsdorp, H.; Repetto, C.; Venderbos, L.D.F.; Lane, J.A.; Korfage, I.J. How Does Active Surveillance for Prostate Cancer Affect Quality of Life? A Systematic Review. Eur. Urol. 2015, 67, 637–645. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Punnen, S.; Cowan, J.; Dunn, L.B.; Carroll, P.R.; Cooperberg, M.R. A longitudinal study of anxiety, depression and distress as predictors of sexual and urinary quality of life in men with prostate cancer. BJU Int. 2015, 112, E67–E75. [Google Scholar] [CrossRef]
- Watts, S.; Leydon, G.; Eyles, C.; Moore, C.M.; Richardson, A.; Birch, B.; Prescott, P.; Powell, C.; Lewith, G. A quantitative analysis of the prevalence of clinical depression and anxiety in patients with prostate cancer undergoing active surveillance. Br. Med. J. Open 2015, 5, 1–7. [Google Scholar] [CrossRef]
- van den Bergh, R.C.; Essink-Bot, M.L.; Roobol, M.J.; Wolters, T.; Schröder, F.H.; Bangma, C.H.; Steyerberg, E.W. Anxiety and distress during active surveillance for early prostate cancer. Cancer 2009, 115, 3868–3878. [Google Scholar] [CrossRef]
- van den Bergh, R.C.; Essink-Bot, M.L.; Roobol, M.J.; Schröder, F.H.; Bangma, C.H.; Steyerberg, E.W. Do anxiety and distress increase during active surveillance for low risk prostate cancer? J. Urol. 2010, 183, 1786–1791. [Google Scholar] [CrossRef]
- van den Bergh, R.C.; Korfage, I.J.; Roobol, M.J.; Bangma, C.H.; de Koning, H.J.; Steyerberg, E.W.; Essink-Bot, M.L. Sexual function with localized prostate cancer: Active surveillance vs radical therapy. Br. J. Urol. Int. 2012, 110, 1032–1039. [Google Scholar] [CrossRef]
- de Cerqueira, M.A.; Laranja, W.W.; Sanches, B.C.; Monti, C.R.; Reis, L.O. Burden of focal cryoablation versus brachytherapy versus active surveillance in the treatment of very low-risk prostate cancer: A preliminary head-to-head comprehensive assessment. Eur. J. Cancer Care 2015, 24, 929–937. [Google Scholar] [CrossRef]
- Venderbos, L.D.; van den Bergh, R.C.; Roobol, M.J.; Schröder, F.H.; Essink-Bot, M.L.; Bangma, C.H.; Steyerberg, E.W.; Korfage, I.J. A longitudinal study on the impact of active surveillance for prostate cancer on anxiety and distress levels. Psycho-Oncology 2015, 24, 348–354. [Google Scholar] [CrossRef]
- Ruane-McAteer, E. An exploration of men′s experiences of undergoing active surveillance for favorable-risk prostate cancer: A mixed methods study protocol. BMC Cancer 2016, 16, 1–8. [Google Scholar] [CrossRef]
- Punnen, S.; Cowan, J.; Carroll, P.R.; Cooperberg, M.R. Long term health related quality of life after primary treatment for localized prostate cancer: Results from the CaPSURE registry. The Journal of Urology. 2013, 189, e411–e412. [Google Scholar] [CrossRef]
- Ercole, C.; Krebs, T.; Prots, D.; Berglund, R.; Ciezki, J.; Campbell, S.; Fergany, A.; Gong, M.; Haber, G.P.; Jones, S.; et al. Patient-reported health related quality-of-life (hrqol) outcomes of patients on active surveillance: Results of a prospective, longitudinal, single-center study. J. Urol. 2014, 191, e665. [Google Scholar] [CrossRef]
- Pham, K.; Jeldres, C.; Johnston, R.; Cullen, J.; Odem-Davis, K.; Wolff, E.; Levie, K.; Hurwitz, L.; Porter, C. Health-related quality of life for men with low risk prostate cancer managed with active surveillance compared to a cancer-screening cohort without prostate cancer. J. Urol. 2014, 191, e147. [Google Scholar] [CrossRef]
- Hayes, J.H.; Ollendorf, D.A.; Pearson, S.D.; Barry, M.J.; Kantoff, P.W.; Stewart, S.T.; Bhatnagar, V.; Sweeney, C.J.; Stahl, J.E.; McMahon, P.M. Active surveillance compared with initial treatment for men with low-risk prostate cancer: A decision analysis. JAMA 2010, 304, 2373–2380. [Google Scholar] [CrossRef] [PubMed]
- Braun, K.; Ahallal, Y.; Sjoberg, D.D.; Ghoneim, T.; Esteban, M.D.; Mulhall, J.; Vickers, A.; Eastham, J.; Scardino, P.T.; Touijer, K.A. Effect of repeated prostate biopsies on erectile function in men on active surveillance for prostate cancer. J. Urol. 2014, 191, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, J.M. Uncertainty and quality of life among men undergoing active surveillance for prostate cancer in the United States and Ireland. Am. J. Men′s Health 2008, 2, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Kazer, M.W. An internet intervention for management of uncertainty during active surveillance for prostate cancer. Oncol. Nurs. Forum 2011, 38, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Lokman, U.; Vasarainen, H.; Lahdensuo, K.; Erickson, A.M.; Taari, K.; Mirtti, T.K.; Rannikko, A. Prostate cancer active surveillance: Health-related quality of life in the Finnish arm of the prospective PRIAS-study. Three year update. Eur. Urol. Suppl. 2013, 12, e274–e275. [Google Scholar] [CrossRef]
- Vasarainen, H.; Lokman, U.; Ruutu, M.; Taari, K.; Rannikko, A. Prostate cancer active surveillance and health-related quality of life: Results of the Finnish arm of the prospective trial. Br. J. Urol. Int. 2011, 109, 1614–1619. [Google Scholar] [CrossRef] [PubMed]
- Pham, K.N.; Wolff, E.M.; Banerji, J.S.; Wolff, E.M.; Levie, K.E.; Odem-Davis, K.; Banerji, J.S.; Rosner, I.L.; Brand, T.C.; L′Esperance, J.O.; et al. Prospective quality of life in men choosing active surveillance compared to those biopsied but not diagnosed with prostate Cancer. J. Urol. 2016, 196, 392–398. [Google Scholar] [CrossRef]
- Banerji, J.S.; Hurwitz, L.M.; Cullen, J.; Odem-Davis, K.; Wolff, E.M.; Levie, K.; Pham, K.N.; Porter, C.R. A prospective study of health-related quality of life outcomes for low-risk prostate cancer patients managed by active surveillance or radiation therapy. J. Urol. 2015, 193, e513. [Google Scholar] [CrossRef]
- Bergman, J.; Litwin, M.S. Quality of life in men undergoing active surveillance for localized prostate cancer. J. Natl. Cancer Inst. Monogr. 2012, 45, 242–249. [Google Scholar] [CrossRef]
- Wilcox, C.B.; Gilbourd, D.; Louie-Johnsun, M. Anxiety and health-related quality of life (HRQL) in patients undergoing active surveillance of prostate cancer in an Australian centre. Br. J. Urol. Int. 2014, 113, 64–68. [Google Scholar] [CrossRef]
- Seiler, D.; Randazzo, M.; Leupold, U.; Zeh, N.; Isbarn, H.; Chun, F.K.; Ahyai, S.A.; Baumgartner, M.; Huber, A.; Recker, F.; et al. Health outcomes research: Protocol-based active surveillance for low-risk prostate cancer: Anxiety levels in both men and their partners. Urology 2012, 80, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Kazer, M.W.; Bailey, D.E.; Colberg, J.; Kelly, W.K.; Carroll, P. The needs for men undergoing active surveillance (AS) for prostate cancer: Results of a focus group study. J. Clin. Nurs. 2011, 20, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, J.L.; Feibus, A.H.; Maddox, M.M.; Abdel-Mageed, A.B.; Moparty, K.; Thomas, R.; Sartor, O. Active surveillance of prostate cancer in African American men. Urology 2014, 84, 1255–1266. [Google Scholar] [CrossRef] [PubMed]
- Simpson, P. Does active surveillance lead to anxiety and stress? Br. J. Nurs. 2014, 23, S4–S12. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; Burney, S.; Brooker, J.; Ricciardelli, L.A.; Fletcher, J.M.; Satasivam, P.; Frydenberg, M. Anxiety in the management of localized prostate cancer by active surveillance. Br. J. Urol. Int. 2014, 114, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Alvisi, M.F.; Bellardita, L.; Ricanti, T.; Villa, S.; Marenghi, C.; Bedini, N.; Villa, S.; Biasoni, D.; Nicolai, N.; Salvioni, R.; et al. Health related quality of life and coping in patients on active surveillance: Two-year follow-up. Eur. Urol. Suppl. 2013, 12, 159–160. [Google Scholar] [CrossRef]
- Frydenberg, M.; Anderson, J.; Ricciardelli, L.; Burney, S.; Brooker, J.; Fletcher, J. Psychological stress associated with active surveillance for localized low risk prostate cancer. J. Urol. 2013, 189, e548. [Google Scholar] [CrossRef]
- Carter, G.; Clover, K.; Britton, B.; Mitchell, A.J.; White, M.; McLeod, N.; Denham, J.; Lambert, S.D. Wellbeing during active surveillance for localized prostate cancer: A systematic review of psychological morbidity and quality of life. Ann. Fam. Med. 2015, 5, 112–119. [Google Scholar]
- Barocas, D.A.; Alvarez, J.; Resnick, M.J.; Koyama, T.; Hoffman, K.E.; Tyson, M.D.; Conwill, R.; McCollum, D.; Cooperberg, M.R.; Goodman, M.; et al. Association between radiation therapy, surgery or observation for localized prostate cancer and patient-reported outcomes after 3 years. JAMA 2017, 317, 1126–1140. [Google Scholar] [CrossRef]
- Chen, R.C.; Basak, R.; Meyer, A.; Kuo, T.M.; Carpenter, W.R.; Agans, R.P.; Broughman, J.R.; Reeve, B.B.; Nielsen, M.E.; Usinger, D.S.; et al. Association between choice of radical prostatectomy, external beam radiotherapy, brachytherapy, or active surveillance and patient-reported quality of life among men with localized prostate cancer. JAMA 2017, 317, 1141–1150. [Google Scholar] [CrossRef]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).