
Oral Health Behavior and Lifestyle Factors among Overweight and Non-Overweight Young Adults in Europe: A Cross-Sectional Questionnaire Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethics
2.3. Body Mass Index (BMI) Measurement and Classification
2.4. Questionnaire
2.5. Statistical Analyses
3. Results
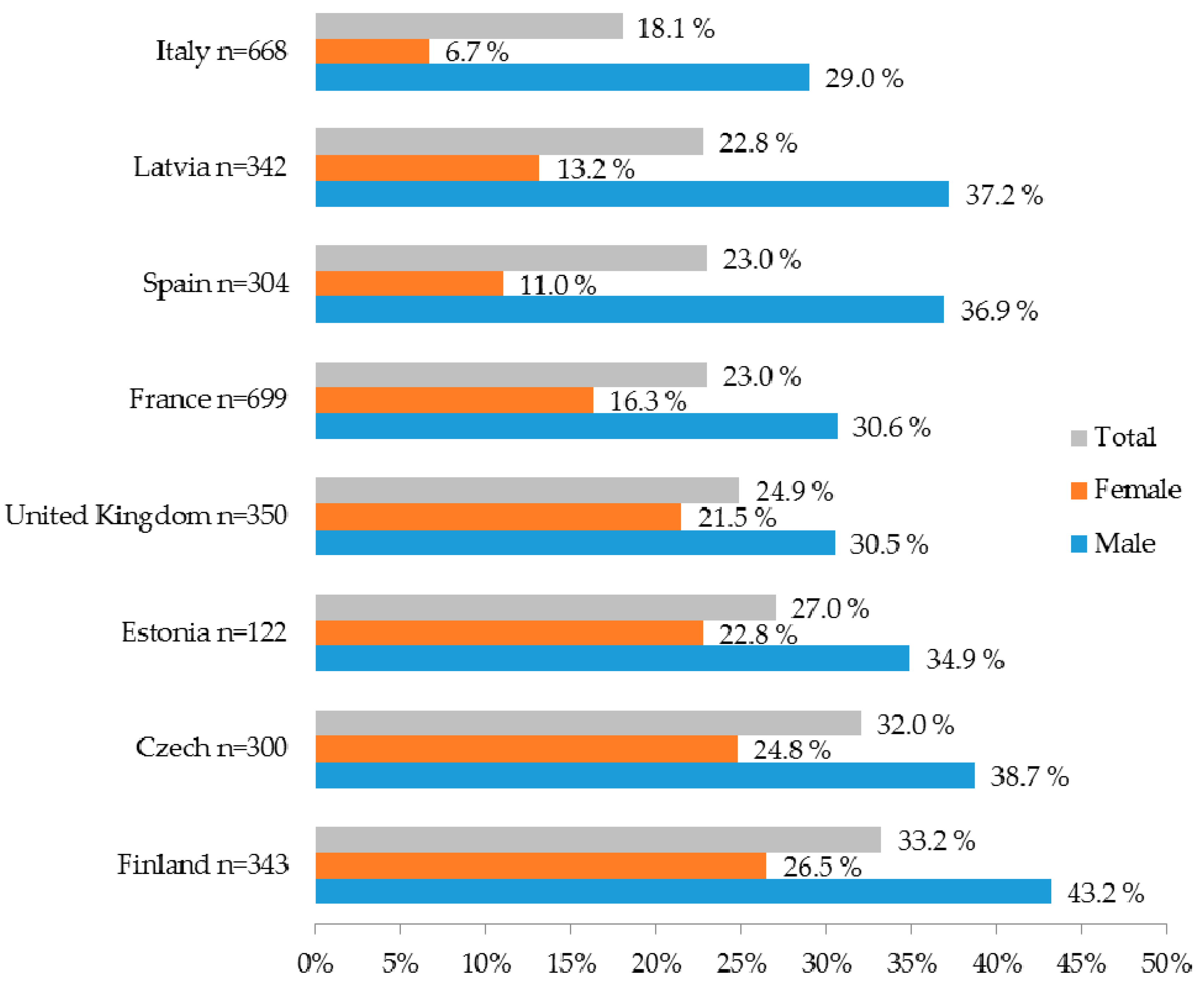
3.1. Prevalence of Being Overweight
3.2. Oral Health Behavior and Being Overweight
3.3. Lifestyle Factors and Being Overweight
3.4. Relationship of Being Overweight to Demographic, Oral Hygiene, Smoking and Dietary Factors
4. Discussion
4.1. Oral Health Behavior and Being Overweight
4.2. The Use of Sugar-Sweetened Beverages
4.3. The Role of Oral Health Professionals in Reducing Overweight Individuals
4.4. Limitations and Strengths
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Brown, W.V.; Fujioka, K.; Wilson, P.W.; Woodworth, K.A. Obesity: Why be concerned? Am. J. Med. 2009, 122, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Östberg, A.L.; Bengtsson, C.; Lissner, L.; Hakeberg, M. Oral health and obesity indicators. BMC Oral Health 2012. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Ogawa, H. The global burden of periodontal disease: Towards integration with chronic disease prevention and control. Periodontol 2000 2012, 60, 15–39. [Google Scholar] [CrossRef] [PubMed]
- Rugg-Gunn, A. Dental caries: Strategies to control this preventable disease. Acta Med. Acad. 2013, 42, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Marcenes, W.; Kassebaum, N.J.; Bernabe, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J. Global burden of oral conditions in 1990–2010: A systematic analysis. J. Dent. Res. 2013, 92, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol 2000 2013, 62, 59–94. [Google Scholar] [CrossRef] [PubMed]
- Huttunen, R.; Syrjänen, J. Obesity and the risk and outcome of infection. Int. J. Obes. 2013, 37, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; Watt, R.G. The common risk factor approach: A rational basis for promoting oral health. Community Dent. Oral Epidemiol. 2000, 28, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Watt, R.; Sheiham, A. Integrating the common risk factor approach into a social determinants framework. Community Dent. Oral Epidemiol. 2012, 40, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Koskinen, J.; Magnussen, C.G.; Sabin, M.A.; Kähönen, M.; Hutri-Kähönen, N.; Laitinen, T.; Taittonen, L.; Jokinen, E.; Lehtimäki, T.; Viikari, J.S.; et al. Youth overweight and metabolic disturbances in predicting carotid intima-media thickness, type 2 diabetes, and metabolic syndrome in adulthood: The Cardiovascular Risk in Young Finns study. Diabetes Care 2014, 37, 1870–1877. [Google Scholar] [CrossRef] [PubMed]
- Suliburska, J.; Bogdanski, P.; Pupek-Musialik, D.; Glod-Nawrocka, M.; Krauss, H.; Piatek, J. Analysis of lifestyle of young adults in the rural and urban areas. Ann. Agric. Environ. Med. 2012, 19, 135–139. [Google Scholar] [PubMed]
- Capewell, S. Sugar sweetened drinks should carry obesity warnings. BMJ 2014. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Diet, nutrition and the prevention of chronic diseases. World Health Organ Tech Rep Ser. 2003, 916, 1–149. [Google Scholar]
- Anonymous. Position paper: Tobacco use and the periodontal patient. Research, Science and Therapy Committee of the American Academy of Periodontology. J. Periodontol. 1999, 70, 1419–1427. [Google Scholar]
- Tunick, M.H.; Van Hekken, D.L. Dairy products and health: Recent insights. J. Agric. Food Chem. 2015, 63, 9381–9388. [Google Scholar] [CrossRef] [PubMed]
- Merritt, J.; Qi, F.; Shi, W. Milk helps build strong teeth and promotes oral health. J. Calif. Dent. Assoc. 2006, 34, 361–366. [Google Scholar] [PubMed]
- Kravitz, A.S.; Bulloc, A. EU Manual of Dental Practice 2015. Edition 5.1. The Council of European Dentists 2015. Available online: https://www.omd.pt/europa/cedmanual/2015/ced-manual-2015-completo.pdf (accessed on 2 April 2016).
- Oral Health. Available online: http://ec.europa.eu/public_opinion/archives/ebs/ebs_330_en.pdf (accessed on 15 February 2016).
- West, N.X.; Sanz, M.; Lussi, A.; Bartlett, D.; Bouchard, P.; Bourgeois, D. Prevalence of dentine hypersensitivity and study of associated factors: A European population-based cross-sectional study. J. Dent. 2013, 41, 841–885. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, D.W.; Lussi, A.; West, N.X.; Bouchard, P.; Sanz, M.; Bourgeois, D. Prevalence of tooth wear on buccal and lingual surfaces and possible risk factors in young European adults. J. Dent. 2013, 41, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- HTTP Status. Available online: http://apps.who.int/bmi/index.jsp (accessed on 15 February 2016).
- Beikler, T.; Flemmig, T.F. Oral biofilm-associated diseases: Trends and implications for quality of life, systemic health and expenditures. Periodontol 2000 2011, 55, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Chaffee, B.W.; Weston, S.J. Association between chronic periodontal disease and obesity: A systematic review and meta-analysis. J. Periodontol. 2010, 81, 1708–1724. [Google Scholar] [CrossRef] [PubMed]
- Levine, R.S. Obesity, diabetes and periodontitis––A triangular relationship? Br. Dent. J. 2013, 215, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabe, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global Burden of Severe Periodontitis in 1990–2010: A Systematic Review and Meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Kay, E.J. How often should we go to the dentist? BMJ 1999, 319, 204–205. [Google Scholar] [CrossRef] [PubMed]
- Crocombe, L.A.; Broadbent, J.M.; Thomson, W.M.; Brennan, D.S.; Poulton, R. Impact of dental visiting trajectory patterns on clinical oral health and oral health-related quality of life. J. Public Health Dent. 2012, 72, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Kandelman, D. Sugar, alternative sweeteners and meal frequency in relation to caries prevention: New perspectives. Br. J. Nutr. 1997, 77, 121–128. [Google Scholar] [CrossRef]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Zhang, Z.; Gregg, E.W.; Flanders, W.D.; Merritt, R.; Hu, F.B. Added sugar intake and cardiovascular diseases mortality among US adults. JAMA Intern. Med. 2014, 174, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Zucconi, S.; Volpato, C.; Adinolfi, F.; Gandini, E.; Gentile, E.; Loi, A.; Fioriti, L. Gathering Consumption Data on Specific Consumer Groups of Energy Drinks; Supporting Publications: Parma, Italy, 2013. [Google Scholar]
- Breda, J.J.; Whiting, S.H.; Encarnacao, R.; Norberg, S.; Jones, R.; Reinap, M.; Jewell, J. Energy drink consumption in Europe: A review of the risks, adverse health effects, and policy options to respond. Front. Public Health 2014. [Google Scholar] [CrossRef] [PubMed]
- Rosseel, J.P.; Jacobs, J.E.; Plasschaert, A.J.; Grol, R.P. A review of strategies to stimulate dental professionals to integrate smoking cessation interventions into primary care. Community Dent. Health 2012, 29, 154–161. [Google Scholar] [PubMed]
- Franki, J.; Hayes, M.J.; Taylor, J.A. The provision of dietary advice by dental practitioners: A review of the literature. Community Dent. Health 2014, 31, 9–14. [Google Scholar] [PubMed]
- Visscher, T.L.; Viet, A.L.; Kroesbergen, I.H.; Seidell, J.C. Underreporting of BMI in adults and its effect on obesity prevalence estimations in the period 1998 to 2001. Obesity 2006, 14, 2054–2063. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Statistics Explained. Available online: http://ec.europa.eu/eurostat/statistics-explained/index.php/Overweight_and_obesity_-_BMI_statistics (accessed on 15 February 2016).


{kind=link}
| Variables | Normal or Underweight BMI < 25 (n = 2369) % | Overweight BMI ≥ 25 (n = 759) % | p-Value |
|---|---|---|---|
| Age | <0.001 | ||
| 18–25 | 44.2 | 30.6 | |
| 26–35 | 55.8 | 69.4 | |
| Sex | <0.001 | ||
| Male | 39.7 | 62.8 | |
| Female | 60.3 | 37.2 | |
| Education | 0.001 | ||
| To age 15 | 4.9 | 6.3 | |
| To age 16–19 | 24.9 | 26.4 | |
| To age 20+ | 43.9 | 48.2 | |
| Still studying | 26.3 | 19.1 | |
| Brushing frequency | <0.001 | ||
| 1 per day | 13.1 | 22.2 | |
| ≥2 per day | 86.9 | 77.8 | |
| Toothbrush used | 0.750 | ||
| Manual | 77.2 | 78.3 | |
| Electric | 19.7 | 19.0 | |
| Fluoride toothpaste | 0.311 | ||
| Yes | 71.6 | 71.9 | |
| No | 9.1 | 7.1 | |
| Do not know | 19.3 | 20.8 | |
| Last dental visit | 0.016 | ||
| 0–2 years ago | 86.8 | 81.6 | |
| More than 2 years ago | 13.2 | 18.4 | |
| Reason for last dental visit | <0.001 | ||
| Examination | 61.5 | 52.6 | |
| Routine dental treatment | 24.6 | 26.2 | |
| Emergency treatment | 13.9 | 21.3 |
| Variables | Normal or Underweight (n = 2369) % | Overweight (n = 759) % | p-Value |
|---|---|---|---|
| Smoking | 0.021 | ||
| Often or occasionally | 30.1 | 34.2 | |
| Rarely or never | 69.9 | 65.8 | |
| Exercise | 0.005 | ||
| ≥3 times a week | 31.4 | 28.6 | |
| 1 to 2 times a week | 34.0 | 30.2 | |
| Less often | 34.6 | 41.1 | |
| Consumption of soft drinks | 0.005 | ||
| Often or occasionally | 55.8 | 61.3 | |
| Rarely or never | 44.2 | 38.7 | |
| Consumption of energy drinks | 0.006 | ||
| Often or occasionally | 19.0 | 23.4 | |
| Rarely or never | 81.0 | 76.6 | |
| Consumption of fruit | 0.246 | ||
| Often or occasionally | 82.4 | 81.2 | |
| Rarely or never | 17.6 | 18.8 | |
| Consumption of dairy products | 0.279 | ||
| Often or occasionally | 90.7 | 89.9 | |
| Rarely or never | 9.3 | 10.1 | |
| Eating or drinking occasions | <0.001 | ||
| 0–6 per day | 81.9 | 76.3 | |
| 7 or more | 18.1 | 23.7 |
| Independent Variables | OR (95% CI) | p-value |
|---|---|---|
| Age | ||
| 26–35 | 1.8 (1.5,2.1) | <0.001 |
| 18–25 | Reference | |
| Sex | ||
| Male | 2.6 (2.2,3.0) | <0.001 |
| Female | Reference | |
| Education | ||
| Stopped studying before age of 20 | 1.0 (0.9,1.3) | 0.640 |
| Studied until age of 20 or is still studying | Reference | |
| Brushing frequency | ||
| 1 per day | 1.6(1.3,2.0) | <0.001 |
| ≥2 per day | Reference | |
| Last dental visit | ||
| More than 2 years ago | 1.3 (1.1,1.7) | 0.012 |
| 0–2 years ago | Reference | |
| Reason for last dental visit | ||
| Emergency | 1.6 (1.3,1.9) | <0.001 |
| Other | Reference | |
| Eating or drinking occasions | ||
| 7 or more | 1.4(1.1,1.7) | 0.002 |
| 0–6 per day | Reference | |
| Smoking | ||
| Often or occasionally | 1.0 (0.9,1.0) | 0.947 |
| Rarely or never | Reference | |
| Consumption of soft drinks | ||
| Often or occasionally | 1.1 (0.9,1.3) | 0.149 |
| Rarely or never | Reference | |
| Consumption of energy drinks | ||
| Often or occasionally | 1.1(0.9,1.4) | 0.224 |
| Rarely or never | Reference | |
| Exercise | ||
| <3 times a week | 1.3(1.1,1.5) | 0.014 |
| ≥3 times a week | Reference |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nihtila, A.; West, N.; Lussi, A.; Bouchard, P.; Ottolenghi, L.; Senekola, E.; Llodra, J.C.; Viennot, S.; Bourgeois, D. Oral Health Behavior and Lifestyle Factors among Overweight and Non-Overweight Young Adults in Europe: A Cross-Sectional Questionnaire Study. Healthcare 2016, 4, 21. https://doi.org/10.3390/healthcare4020021
Nihtila A, West N, Lussi A, Bouchard P, Ottolenghi L, Senekola E, Llodra JC, Viennot S, Bourgeois D. Oral Health Behavior and Lifestyle Factors among Overweight and Non-Overweight Young Adults in Europe: A Cross-Sectional Questionnaire Study. Healthcare. 2016; 4(2):21. https://doi.org/10.3390/healthcare4020021
Chicago/Turabian StyleNihtila, Annamari, Nicola West, Adrian Lussi, Philippe Bouchard, Livia Ottolenghi, Egita Senekola, Juan Carlos Llodra, Stephane Viennot, and Denis Bourgeois. 2016. "Oral Health Behavior and Lifestyle Factors among Overweight and Non-Overweight Young Adults in Europe: A Cross-Sectional Questionnaire Study" Healthcare 4, no. 2: 21. https://doi.org/10.3390/healthcare4020021
APA StyleNihtila, A., West, N., Lussi, A., Bouchard, P., Ottolenghi, L., Senekola, E., Llodra, J. C., Viennot, S., & Bourgeois, D. (2016). Oral Health Behavior and Lifestyle Factors among Overweight and Non-Overweight Young Adults in Europe: A Cross-Sectional Questionnaire Study. Healthcare, 4(2), 21. https://doi.org/10.3390/healthcare4020021