

Differentiating Nontuberculous Mycobacterial Pulmonary Disease from Pulmonary Tuberculosis in Resource-Limited Settings: A Pragmatic Model for Reducing Misguided Antitubercular Treatment
Abstract
1. Introduction
2. Materials and Methods
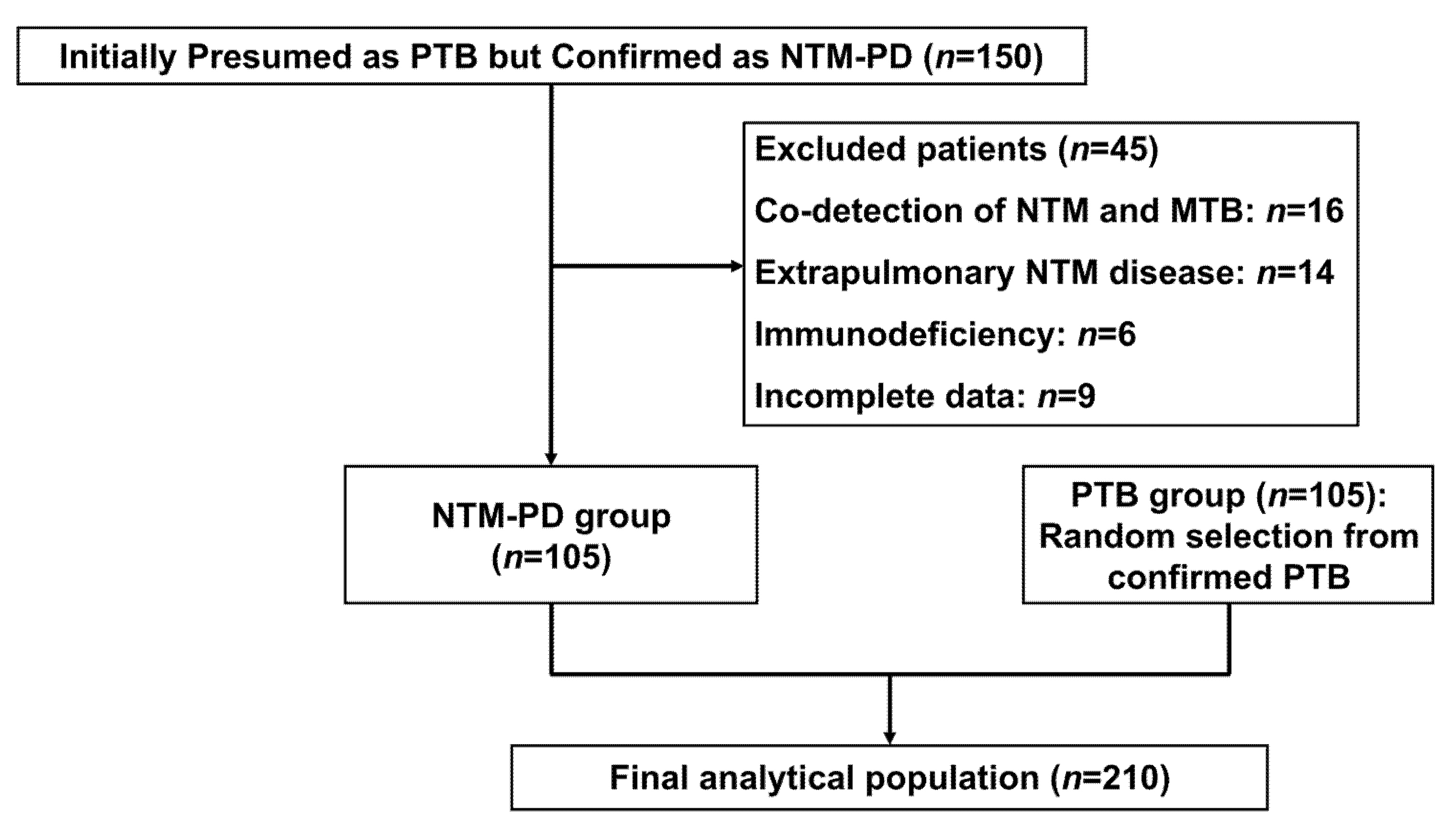
2.1. Patients
2.2. Collection of Clinical Data
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of NTM-PD and PTB Patients
3.2. Laboratory and Microbiological Characteristics
3.3. Comparative Analysis of Thoracic CT Features
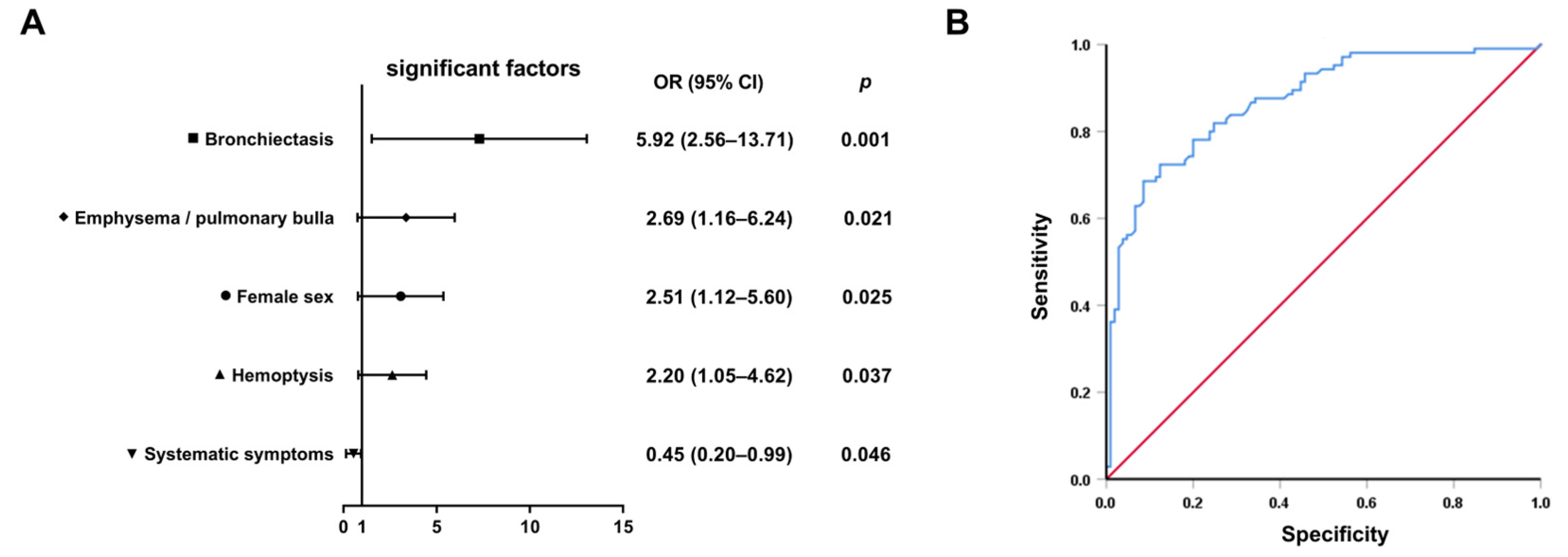
3.4. Multivariable Predictors and Diagnostic Model Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harding, E. WHO global progress report on tuberculosis elimination. Lancet Respir. Med. 2020, 8, 19. [Google Scholar] [CrossRef]
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 2007, 175, 367–416. [Google Scholar] [CrossRef]
- Tan, Y.; Deng, Y.; Yan, X.; Liu, F.; Tan, Y.; Wang, Q.; Bao, X.; Pan, J.; Luo, X.; Yu, Y.; et al. Nontuberculous mycobacterial pulmonary disease and associated risk factors in China: A prospective surveillance study. J. Infect. 2021, 83, 46–53. [Google Scholar] [CrossRef]
- Liu, C.F.; Song, Y.M.; He, W.C.; Liu, D.X.; He, P.; Bao, J.J.; Wang, X.Y.; Li, Y.M.; Zhao, Y.L. Nontuberculous mycobacteria in China: Incidence and antimicrobial resistance spectrum from a nationwide survey. Infect. Dis. Poverty 2021, 10, 59. [Google Scholar] [CrossRef]
- Winthrop, K.L.; Marras, T.K.; Adjemian, J.; Zhang, H.; Wang, P.; Zhang, Q. Incidence and Prevalence of Nontuberculous Mycobacterial Lung Disease in a Large U.S. Managed Care Health Plan, 2008–2015. Ann. Am. Thorac. Soc. 2020, 17, 178–185. [Google Scholar] [CrossRef]
- Diel, R.; Jacob, J.; Lampenius, N.; Loebinger, M.; Nienhaus, A.; Rabe, K.F.; Ringshausen, F.C. Burden of non-tuberculous mycobacterial pulmonary disease in Germany. Eur. Respir. J. 2017, 49, 1602109. [Google Scholar] [CrossRef]
- Ojo, O.T.; Odeyemi, A.O. Non-Mycobacteria Tuberculosis in Africa: A Literature Review. Ethiop. J. Health Sci. 2023, 33, 913–918. [Google Scholar] [CrossRef]
- Esteban, J.; García-Coca, M. Mycobacterium Biofilms. Front. Microbiol. 2017, 8, 2651. [Google Scholar] [CrossRef]
- Loebinger, M.R.; Quint, J.K.; van der Laan, R.; Obradovic, M.; Chawla, R.; Kishore, A.; van Ingen, J. Risk Factors for Nontuberculous Mycobacterial Pulmonary Disease: A Systematic Literature Review and Meta-Analysis. Chest 2023, 164, 1115–1124. [Google Scholar] [CrossRef]
- Varley, C.D.; Streifel, A.C.; Bair, A.M.; Winthrop, K.L. Nontuberculous Mycobacterial Pulmonary Disease in the Immunocompromised Host. Clin. Chest Med. 2023, 44, 829–838. [Google Scholar] [CrossRef]
- Renna, M.; Schaffner, C.; Brown, K.; Shang, S.; Tamayo, M.H.; Hegyi, K.; Grimsey, N.J.; Cusens, D.; Coulter, S.; Cooper, J.; et al. Azithromycin blocks autophagy and may predispose cystic fibrosis patients to mycobacterial infection. J. Clin. Investig. 2011, 121, 3554–3563. [Google Scholar] [CrossRef]
- Yu, G.; Shen, Y.; Xu, X.; Lin, L. Nucleic acid amplification techniques for rapid diagnosis of nontuberculous mycobacteria: A protocol of systematic review and meta-analysis. PLoS ONE 2021, 16, e0250470. [Google Scholar] [CrossRef]
- Zhu, Y.; Liu, Z.; Peng, L.; Liu, B.; Wu, K.; Zhang, M.; Wang, X.; Pan, J. Evaluation of nucleotide MALDI-TOF-MS for the identification of Mycobacterium species. Front. Cell. Infect. Microbiol. 2024, 14, 1335104. [Google Scholar] [CrossRef]
- Liu, Q.; Pan, X.; An, H.; Du, J.; Li, X.; Sun, W.; Gao, Y.; Li, Y.; Niu, H.; Gong, W.; et al. Building a model for the differential diagnosis of non-tuberculous mycobacterial lung disease and pulmonary tuberculosis: A case-control study based on immunological and radiological features. Int. Immunopharmacol. 2023, 124, 111064. [Google Scholar] [CrossRef]
- Jia, H.; Pan, L.; Wang, G.; Duan, H.; Song, Z.; Sun, Q.; Wei, R.; Du, B.; Xing, A.; Zhang, Z. Assessment of Interferon-Gamma Release Assay in Patients with Non-Tuberculous Mycobacteria Pulmonary Disease. Clin. Lab. 2019, 65, 1813. [Google Scholar] [CrossRef]
- Khare, R.; Brown-Elliott, B.A. Culture, Identification, and Antimicrobial Susceptibility Testing of Pulmonary Nontuberculous Mycobacteria. Clin. Chest Med. 2023, 44, 743–755. [Google Scholar] [CrossRef]
- Gopalaswamy, R.; Shanmugam, S.; Mondal, R.; Subbian, S. Of tuberculosis and non-tuberculous mycobacterial infections—A comparative analysis of epidemiology, diagnosis and treatment. J. Biomed. Sci. 2020, 27, 74. [Google Scholar] [CrossRef]
- Kendall, B.A.; Varley, C.D.; Choi, D.; Cassidy, P.M.; Hedberg, K.; Ware, M.A.; Winthrop, K.L. Distinguishing tuberculosis from nontuberculous mycobacteria lung disease, Oregon, USA. Emerg. Infect. Dis. 2011, 17, 506–509. [Google Scholar] [CrossRef]
- Daley, C.L.; Iaccarino, J.M.; Lange, C.; Cambau, E.; Wallace, R.J., Jr.; Andrejak, C.; Böttger, E.C.; Brozek, J.; Griffith, D.E.; Guglielmetti, L.; et al. Treatment of nontuberculous mycobacterial pulmonary disease: An official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur. Respir. J. 2020, 56, 2000535. [Google Scholar] [CrossRef]
- NHFPC. Diagnosis for pulmonary tuberculosis (WS 288-2017). Electr. J. Emerg. Infect. Dis. 2018, 3, 59–61. [Google Scholar] [CrossRef]
- Kim, T.S.; Koh, W.J.; Han, J.; Chung, M.J.; Lee, J.H.; Lee, K.S.; Kwon, O.J. Hypothesis on the evolution of cavitary lesions in nontuberculous mycobacterial pulmonary infection: Thin-section CT and histopathologic correlation. AJR Am. J. Roentgenol. 2005, 184, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Retuerto-Guerrero, M.; López-Medrano, R.; de Freitas-González, E.; Rivero-Lezcano, O.M. Nontuberculous Mycobacteria, Mucociliary Clearance, and Bronchiectasis. Microorganisms 2024, 12, 665. [Google Scholar] [CrossRef]
- Muñoz-Egea, M.C.; Akir, A.; Esteban, J. Mycobacterium biofilms. Biofilm 2023, 5, 100107. [Google Scholar] [CrossRef]
- Kim, B.G.; Choi, Y.S.; Shin, S.H.; Lee, K.; Um, S.W.; Kim, H.; Cho, J.H.; Kim, H.K.; Kim, J.; Shim, Y.M.; et al. Risk Factors for the Development of Nontuberculous Mycobacteria Pulmonary Disease during Long-Term Follow-Up after Lung Cancer Surgery. Diagnostics 2022, 12, 1086. [Google Scholar] [CrossRef]
- Park, Y.; Kim, N.E.; Kwak, S.H.; Park, M.S.; Jeong, S.J.; Lee, J.G.; Paik, H.C.; Kim, S.Y.; Kang, Y.A. Nontuberculous mycobacterial infection after lung transplantation: A single-center experience in South Korea. J. Microbiol. Immunol. Infect. 2022, 55, 123–129. [Google Scholar] [CrossRef]
- Nishimura, T.; Fujita-Suzuki, Y.; Mori, M.; Carpenter, S.M.; Fujiwara, H.; Uwamino, Y.; Tamizu, E.; Yano, I.; Kawabe, H.; Hasegawa, N. Middle-aged to elderly women have a higher asymptomatic infection rate with Mycobacterium avium complex, regardless of body habitus. Respirology 2016, 21, 553–555. [Google Scholar] [CrossRef]
- Kartalija, M.; Ovrutsky, A.R.; Bryan, C.L.; Pott, G.B.; Fantuzzi, G.; Thomas, J.; Strand, M.J.; Bai, X.; Ramamoorthy, P.; Rothman, M.S.; et al. Patients with nontuberculous mycobacterial lung disease exhibit unique body and immune phenotypes. Am. J. Respir. Crit. Care Med. 2013, 187, 197–205. [Google Scholar] [CrossRef]
- Tsuyuguchi, K.; Suzuki, K.; Matsumoto, H.; Tanaka, E.; Amitani, R.; Kuze, F. Effect of oestrogen on Mycobacterium avium complex pulmonary infection in mice. Clin. Exp. Immunol. 2001, 123, 428–434. [Google Scholar] [CrossRef]
- Mirsaeidi, M.; Sadikot, R.T. Gender susceptibility to mycobacterial infections in patients with non-CF bronchiectasis. Int. J. Mycobacteriol. 2015, 4, 92–96. [Google Scholar] [CrossRef]
- Gupta, M.; Srikrishna, G.; Klein, S.L.; Bishai, W.R. Genetic and hormonal mechanisms underlying sex-specific immune responses in tuberculosis. Trends Immunol. 2022, 43, 640–656. [Google Scholar] [CrossRef]
- Buttle, T.S.; Hummerstone, C.Y.; Billahalli, T.; Ward, R.J.B.; Barnes, K.E.; Marshall, N.J.; Spong, V.C.; Bothamley, G.H. The monocyte-to-lymphocyte ratio: Sex-specific differences in the tuberculosis disease spectrum, diagnostic indices and defining normal ranges. PLoS ONE 2021, 16, e0247745. [Google Scholar] [CrossRef] [PubMed]
- Lyadova, I.V.; Panteleev, A.V. Th1 and Th17 Cells in Tuberculosis: Protection, Pathology, and Biomarkers. Mediat. Inflamm. 2015, 2015, 854507. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Sun, Q.; Zhang, Y.; Li, X.; Liang, Q.; Guo, R.; Zhang, L.; Han, X.; Wang, J.; Shao, L.; et al. Systemic immune dysregulation in severe tuberculosis patients revealed by a single-cell transcriptome atlas. J. Infect. 2023, 86, 421–438. [Google Scholar] [CrossRef] [PubMed]
- Kwak, N.; Moon, J.; Kim, J.Y.; Park, J.W.; Yim, J.J. Clinical course of nontuberculous mycobacterial pulmonary disease in patients with rheumatoid arthritis. Adv. Rheumatol. 2024, 64, 20. [Google Scholar] [CrossRef]
- Kim, J.Y.; Han, A.; Lee, H.; Ha, J.; Lee, K.W.; Suh, K.S.; Yi, N.J.; Min, S.; Hong, S.K.; Kim, Y.C.; et al. The Clinical Course and Prognosis of Patients With Nontuberculous Mycobacterial Pulmonary Disease After Solid Organ Transplantation. J. Korean Med. Sci. 2023, 38, e46. [Google Scholar] [CrossRef]
- Bagcchi, S. WHO’s Global Tuberculosis Report 2022. Lancet Microbe 2023, 4, e20. [Google Scholar] [CrossRef]
- Borgdorff, M.W.; Floyd, K.; Broekmans, J.F. Interventions to reduce tuberculosis mortality and transmission in low- and middle-income countries. Bull. World Health Organ. 2002, 80, 217–227. [Google Scholar]
- Cui, X.; Gao, L.; Cao, B. Management of latent tuberculosis infection in China: Exploring solutions suitable for high-burden countries. Int. J. Infect. Dis. 2020, 92s, S37–S40. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | NTM-PD | PTB | p |
|---|---|---|---|
| Age (years) | 53.1 ± 14.3 | 45.1 ± 17.6 | 0.001 |
| Female [n (%)] | 62 (59.0) | 38 (36.2) | 0.001 |
| Height (cm) | 161.40 ± 7.27 | 163.56 ± 7.95 | 0.041 |
| Weight (kg) | 50.68 ± 9.39 | 53.56 ± 10.46 | 0.037 |
| BMI (kg/m2) | 19.19 ± 3.36 | 20.59 ± 3.13 | 0.009 |
| Time from symptom onset to diagnosis (month) | 16 (5~37) | 3 (2~9) | 0.001 |
| Comorbidities [n (%)] | |||
| COPD | 13 (12.4) | 5 (4.8) | 0.049 |
| DM | 5 (4.8) | 18 (17.1) | 0.004 |
| PMH [n (%)] | |||
| Chest trauma and surgery | 8 (7.6) | 1 (1.0) | 0.041 |
| Chronic dust exposure | 6 (5.7) | 6 (5.7) | 1.000 |
| Symptoms [n (%)] | |||
| Expectoration | 85 (81.0) | 77 (73.3) | 0.189 |
| Irritating dry cough | 6 (5.7) | 11 (10.5) | 0.206 |
| Hemoptysis | 54 (51.4) | 29 (27.6) | 0.001 |
| Dyspnea | 76 (72.4) | 58 (55.2) | 0.010 |
| Chest pain | 14 (13.3) | 10 (9.5) | 0.386 |
| Systemic symptoms 1 | 42 (40.0) | 62 (59.0) | 0.006 |
| Fever | 14 (13.3) | 24 (22.9) | 0.073 |
| Night sweats | 17 (16.2) | 30 (28.6) | 0.031 |
| asthenia | 10 (9.5) | 9 (8.6) | 0.810 |
| Weight loss | 17 (16.2) | 34 (32.4) | 0.006 |
| Test Items | NTM-PD | PTB | p |
|---|---|---|---|
| Routine blood test | |||
| WBC (×109/L) | 5.92 (4.88~7.55) | 6.68 (5.01~8.42) | 0.144 |
| Neutrophils (×109/L) | 3.53 (2.78~4.94) | 4.23 (3.02~6.00) | 0.020 |
| Lymphocytes (×109/L) | 1.43 (1.10~1.91) | 1.35 (0.93~1.66) | 0.059 |
| Monocytes (×109/L) | 0.47 (0.35~0.63) | 0.51 (0.42~0.76) | 0.042 |
| ML ratio 1 | 0.30 (0.21~0.55) | 0.45 (0.29~0.64) | 0.001 |
| PLT (×109/L) | 211 (163~275) | 251 (202~341) | 0.001 |
| Serum proteins (g/L) | |||
| TP | 66.4 (62.6~71.2) | 69.8 (63.5~74.9) | 0.010 |
| ALB | 39.6 (36.8~43.0) | 40.2 (34.6~43.7) | 0.601 |
| GLB | 26.3 (23.7~28.9) | 29.4 (26.4~32.7) | 0.001 |
| Immunological test | |||
| C3 (g/L) | 1.15 (1.01~1.27) | 1.26 (1.17~1.49) | 0.001 |
| C4 (g/L) | 0.27 (0.23~0.31) | 0.31 (0.26~0.36) | 0.004 |
| IgG (g/L) | 14.8 (12.2~16.6) | 15.4 (12.4~18.2) | 0.276 |
| IgA (g/L) | 2.67 (1.96~3.65) | 2.49 (1.84~3.17) | 0.234 |
| IgM (g/L) | 1.28 (0.80~1.79) | 1.07 (0.73~1.68) | 0.197 |
| Infection indicators | |||
| CRP (mg/L) | 5.6 (1.4~33.2) | 22.4 (6.9~49.1) | 0.001 |
| PCT (ng/mL) | 0.16 (0.11~0.32) | 0.19 (0.13~0.41) | 0.312 |
| ESR (mm/h) | 23 (11~47) | 34 (15~69) | 0.013 |
| PPD test [n (%)] | 0.005 | ||
| Negative | 60 (57.1) | 20 (19.0) | |
| Weakly positive | 6 (5.7) | 10 (9.5) | |
| Positive | 25 (23.8) | 52 (49.5) | |
| Strongly positive | 14 (13.3) | 23 (21.9) | |
| TB antibody [n (%)] | |||
| Positive | 18 (17.1) | 37 (35.2) | 0.003 |
| T-SPOT [n (%)] | |||
| Positive | 44 (41.9) | 84 (80.0) | 0.001 |
| Sputum acid-fast stain 2 [n (%)] | 0.280 | ||
| + | 17 (16.2) | 12 (11.4) | |
| ++ | 18 (17.1) | 11 (10.5) | |
| +++ | 9 (8.6) | 10 (9.5) | |
| ++++ | 5 (4.8) | 11 (10.5) | |
| Sputum culture 3 [n (%)] | 50 | 0.001 | |
| + | 23 (21.9) | 7 (6.7) | |
| ++ | 36 (34.3) | 9 (8.6) | |
| +++ | 38 (36.2) | 25 (23.8) | |
| ++++ | 8 (7.6) | 64 (60.9) | |
| 1+~2+:3+~4+ ratio | 59/46 | 16/89 | 0.001 |
| CT Findings [n (%)] | NTM-PD | PTB | p |
|---|---|---|---|
| Bilateral lung lesions | 95 (90.5) | 80 (76.2) | 0.005 |
| Multiple lobe involvement | 98 (93.3) | 89 (84.8) | 0.047 |
| Upper lobe | 89 (84.8) | 78 (74.3) | 0.060 |
| Right middle lobe/Left lingual lobe | 81 (77.1) | 59 (56.2) | 0.001 |
| Lower lobe | 83 (79.0) | 87 (82.9) | 0.482 |
| Patchy shadow | 89 (84.8) | 84 (80.0) | 0.365 |
| Fibrous stripe | 77 (73.3) | 54 (51.4) | 0.001 |
| Nodular shadow | 73 (69.5) | 76 (72.4) | 0.648 |
| Ground glass opacity | 4 (3.8) | 7 (6.7) | 0.353 |
| Consolidation | 9 (8.6) | 22 (21.0) | 0.011 |
| Cavity | 50 (47.6) | 56 (53.3) | 0.408 |
| Bronchiectasis | 65 (61.9) | 16 (15.2) | 0.001 |
| Emphysema/pulmonary bulla | 48 (45.7) | 22 (21.0) | 0.001 |
| Atelectasis | 19 (18.1) | 11 (10.5) | 0.115 |
| Pleural effusion | 16 (15.2) | 24 (22.9) | 0.160 |
| Risk Factors | β Regression Coefficient | p | OR | 95%CI |
|---|---|---|---|---|
| NTM-PD predictors | ||||
| Female sex | 0.919 | 0.025 | 2.51 | 1.12–5.60 |
| Bronchiectasis | 1.779 | 0.001 | 5.92 | 2.56–13.71 |
| Hemoptysis | 0.789 | 0.037 | 2.20 | 1.05–4.62 |
| Emphysema/pulmonary bulla | 0.991 | 0.021 | 2.69 | 1.16–6.24 |
| PTB predictor | ||||
| Systemic symptoms 1 | −0.802 | 0.046 | 0.45 | 0.20–0.99 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, W.; Chen, J.; Chen, Z.; Quan, J.; Huang, Z. Differentiating Nontuberculous Mycobacterial Pulmonary Disease from Pulmonary Tuberculosis in Resource-Limited Settings: A Pragmatic Model for Reducing Misguided Antitubercular Treatment. Healthcare 2025, 13, 1065. https://doi.org/10.3390/healthcare13091065
Zhang W, Chen J, Chen Z, Quan J, Huang Z. Differentiating Nontuberculous Mycobacterial Pulmonary Disease from Pulmonary Tuberculosis in Resource-Limited Settings: A Pragmatic Model for Reducing Misguided Antitubercular Treatment. Healthcare. 2025; 13(9):1065. https://doi.org/10.3390/healthcare13091065
Chicago/Turabian StyleZhang, Wei, Jun Chen, Zhenhua Chen, Jun Quan, and Zebing Huang. 2025. "Differentiating Nontuberculous Mycobacterial Pulmonary Disease from Pulmonary Tuberculosis in Resource-Limited Settings: A Pragmatic Model for Reducing Misguided Antitubercular Treatment" Healthcare 13, no. 9: 1065. https://doi.org/10.3390/healthcare13091065
APA StyleZhang, W., Chen, J., Chen, Z., Quan, J., & Huang, Z. (2025). Differentiating Nontuberculous Mycobacterial Pulmonary Disease from Pulmonary Tuberculosis in Resource-Limited Settings: A Pragmatic Model for Reducing Misguided Antitubercular Treatment. Healthcare, 13(9), 1065. https://doi.org/10.3390/healthcare13091065