
HIV Stigma and Discrimination in Colombian Healthcare: Insights from a National Cross-Sectional Analysis of General Practitioners
 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Population and Sample
The Selection of Participants Was Based on the Following Criteria
2.3. Questionnaire Development and Measurement
- Informed Consent;
- Sociodemographic Data (6 questions);
- Specialized Training on HIV (4 questions);
- Fear of HIV Infection (4 questions);
- Stigma and Discrimination Towards People Living with HIV (PLHIV) (6 questions);
- Stereotypes and Prejudices (7 questions).
2.4. Variables
2.5. Data Collection and Management
2.6. Ethical Statement
2.7. Statistical Analysis
3. Results
3.1. Sociodemographic and Professional Characteristics
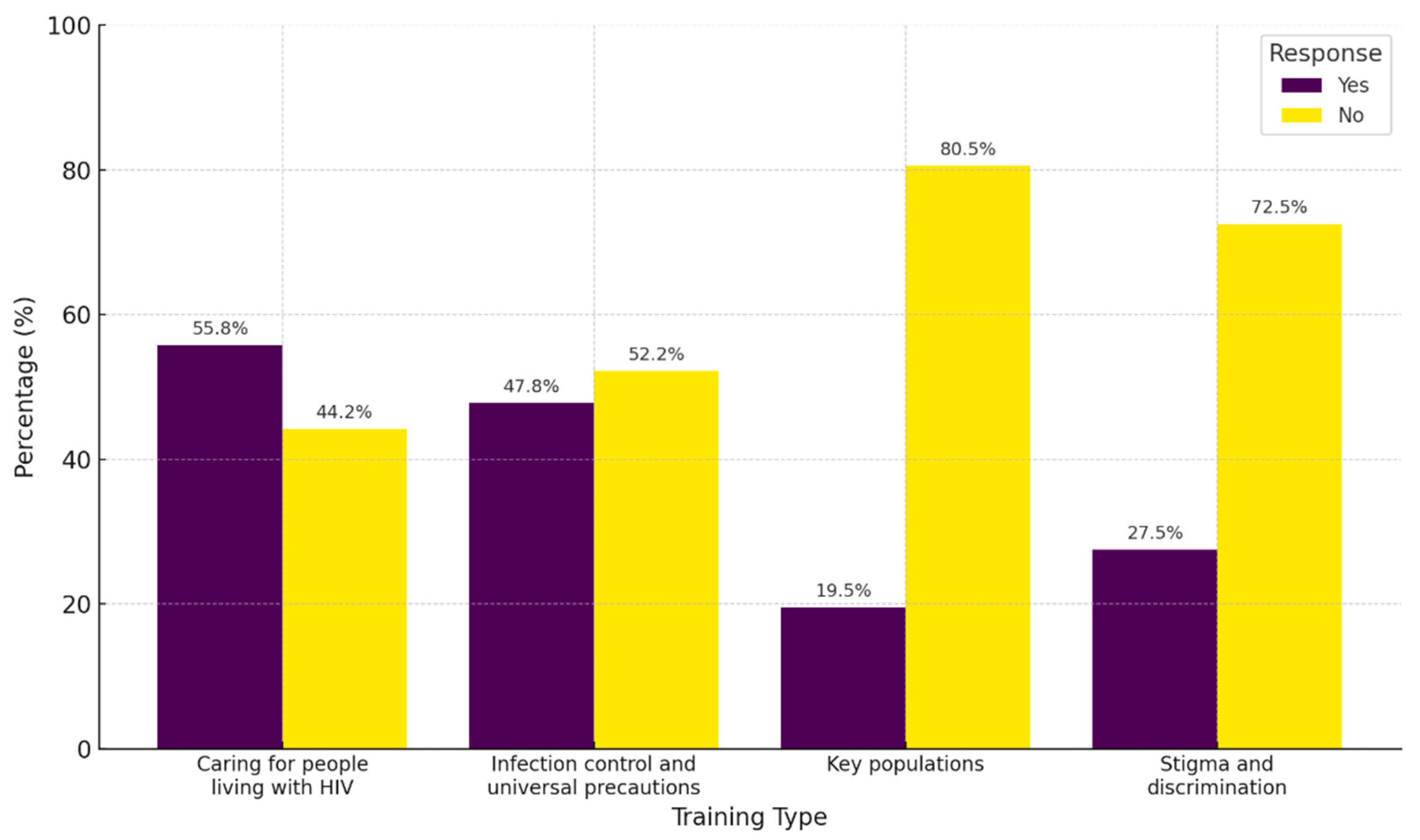
3.2. Previous Training for PLHIV
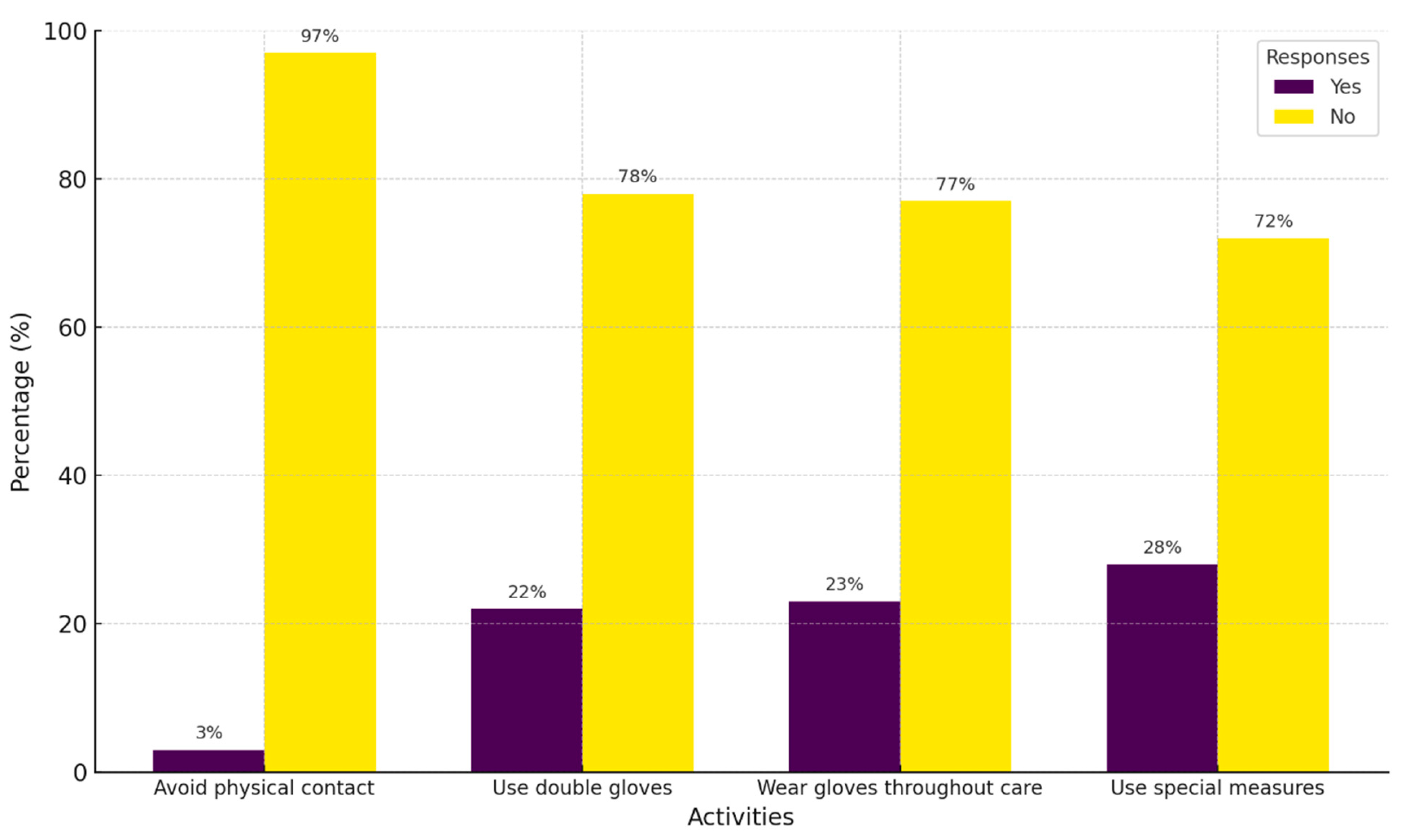
3.3. Fear of HIV Infection
3.4. Factors Associated with Fear of HIV Infection
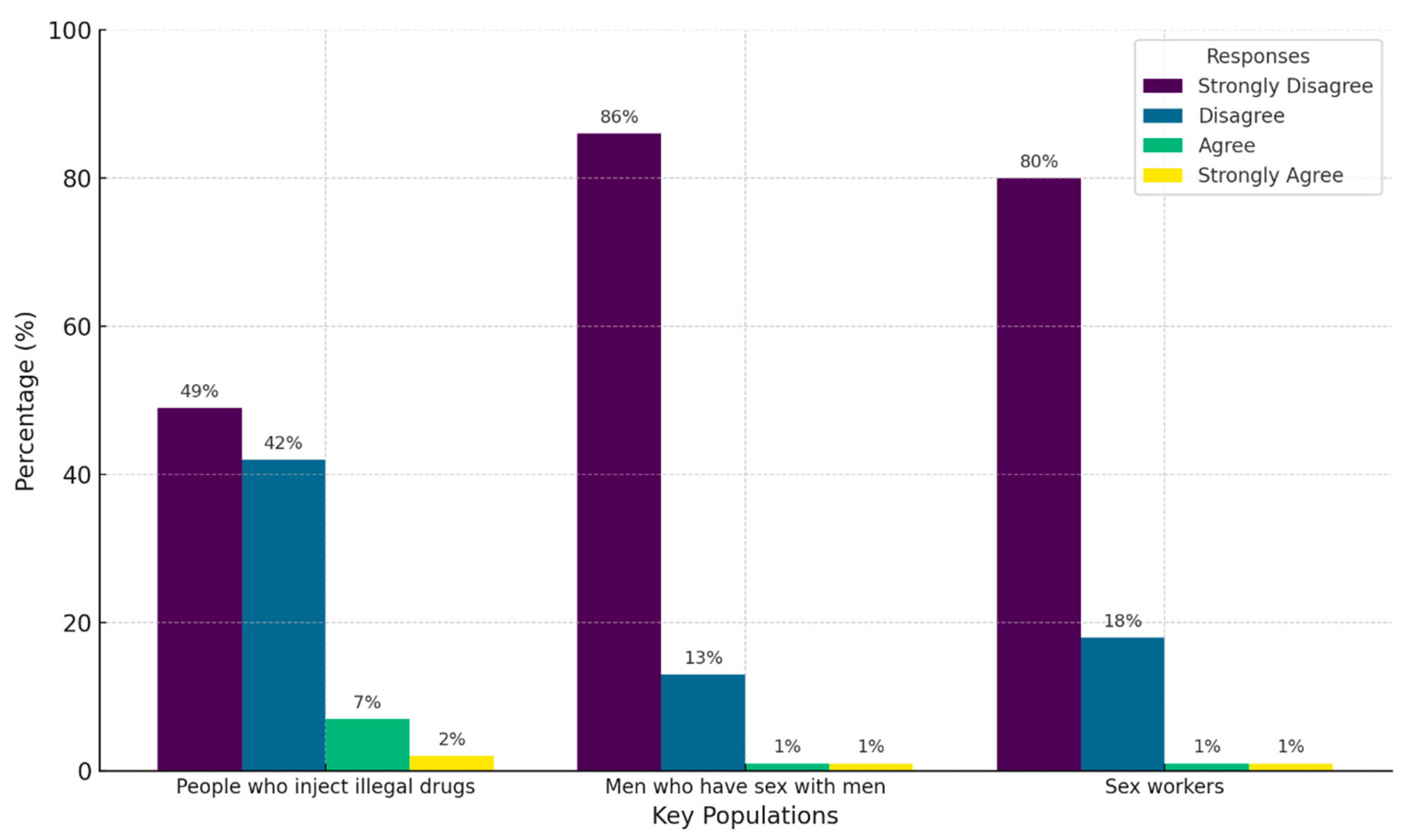
3.5. Stereotypes and Prejudices Toward PLWH
3.6. Stigma Among Physicians Toward PLWH
3.7. Factors Associated with Stigma Toward PLWH
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HIV | Human immunodeficiency virus |
| PLWHA | People living with HIV/AIDS |
| PLHIV | People living with HIV |
| CI | Confidence interval |
| OR | Odds ratio |
| UNAIDS | Joint United Nations Programme on HIV/AIDS |
References
- Smith, M.K.; Xu, R.H.; Hunt, S.L.; Wei, C.; Tucker, J.D.; Tang, W.; Luo, D.; Xue, H.; Wang, C.; Yang, L.; et al. Combating HIV Stigma in Low- and Middle-Income Healthcare Settings: A Scoping Review. J. Int. AIDS Soc. 2020, 23, e25553. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.M.; Abdelrheem, S.S.; Mohammed, H.M. Stigma and Discrimination Against People Living with HIV by Health Care Providers in Egypt. BMC Health Serv. Res. 2023, 23, 663. [Google Scholar] [CrossRef] [PubMed]
- Mendez, A.D.; Neelamegam, M.; Griner, S.B. Health Care Provider Discussions Regarding HIV/Sexually Transmitted Infection Risk Factors and Associations with HIV/Sexually Transmitted Infection Screening Among Men. Arch. Sex. Behav. 2023, 52, 2111–2121. [Google Scholar] [CrossRef] [PubMed]
- Mohammadifirouzeh, M.; Oh, K.M.; Tanner, S. HIV Stigma Reduction Interventions Among Health Care Providers and Students in Different Countries: A Systematic Review. Curr. HIV Res. 2022, 20, 20–31. [Google Scholar] [CrossRef]
- Baldwin, A.; Sileo, K.M.; Huynh, T.A.; Olfers, A.; Woo, C.J.; Greene, S.L.; Casillas, G.L.; Taylor, B.S. Applying the Health Stigma and Discrimination Framework to Assess HIV Stigma among Health Care Professionals: A Mixed Methods, Community-Based Participatory Research Study. J. Health Care Poor Underserved 2022, 33, 950–972. [Google Scholar] [CrossRef]
- Okpua, N.C.; Godwin, C.A. Healthcare Providers in Nigerian Hospitals and HIV-Related Stigma: A Systematic Review. J. Commun. Healthc. 2023, 16, 170–179. [Google Scholar] [CrossRef]
- Spence, A.B.; Wang, C.; Michel, K.; Ocampo, J.M.; Kharfen, M.; Merenstein, D.; Goparaju, L.; Kassaye, S. HIV Related Stigma among Healthcare Providers: Opportunities for Education and Training. J. Int. Assoc. Provid. AIDS Care 2022, 21, 23259582221114797. [Google Scholar] [CrossRef]
- Nyblade, L.; Mbuya-Brown, R.J.; Ezekiel, M.J.; Addo, N.A.; Sabasaba, A.N.; Atuahene, K.; Kiwia, P.; Gyamera, E.; Akyoo, W.O.; Vormawor, R.; et al. A Total Facility Approach to Reducing HIV Stigma in Health Facilities: Implementation Process and Lessons Learned. AIDS 2020, 34 (Suppl. S1), S93–S102. [Google Scholar] [CrossRef]
- Vetrova, M.V.; Cheng, D.M.; Bendiks, S.; Gnatienko, N.; Lloyd-Travaglini, C.; Jiang, W.; Luoma, J.; Blokhina, E.; Krupitsky, E.; Lioznov, D.; et al. HIV and Substance Use Stigma, Intersectional Stigma and Healthcare Among HIV-Positive PWID in Russia. AIDS Behav. 2021, 25, 2815–2826. [Google Scholar] [CrossRef]
- Khumalo, G.E.; Lutge, E.E.; Naidoo, P.; Mashamba-Thompson, T.P. Barriers and Facilitators of Rendering HIV Services by Community Health Workers in Sub-Saharan Africa: A Meta-Synthesis. Fam. Med. Community Health 2021, 9, e000958. [Google Scholar] [CrossRef]
- Knippler, E.T.; Martinez, A.J.; Amiri, I.; Madundo, K.; Mmbaga, B.T.; Goldston, D.B.; Relf, M.V.; Knettel, B.A. Challenges and Opportunities for Improving Mental Health Care and Preventing Suicide Among People Living with HIV: Perspectives of Mental Health Professionals in Tanzania. PLoS Glob. Public. Health 2024, 4, e0002762. [Google Scholar] [CrossRef] [PubMed]
- Cousins, S. HIV in Serbia: Stigma and a stagnant HIV response. Lancet HIV 2018, 5, e343–e344. [Google Scholar] [CrossRef]
- Rivera-Díaz, M.; Varas-Díaz, N.; Reyes-Estrada, M.; Coriano, D.; Ortiz, N.; Padilla, M. Mobile technology as a potential tool in research on stigma associated with HIV/AIDS among medical students. Rev. Puertorriquena Psicol. 2019, 30, 60–68. [Google Scholar] [PubMed]
- Yin, Y.; Chen, A.C.-C.; Wan, S.; Chen, H. Factors Associated With HIV-Related Stigma Toward People Living With HIV Among Nurses in Liangshan Yi Autonomous Prefecture, China: A Cross-Sectional Study. Front. Psychiatry 2021, 12, 714597. [Google Scholar] [CrossRef]
- Geter, A.; Herron, A.R.; Sutton, M.Y. HIV-Related Stigma by Healthcare Providers in the United States: A Systematic Review. AIDS Patient Care STDS 2018, 32, 418–424. [Google Scholar] [CrossRef]
- Shrestha, P.W.; Visudtibhan, P.J.; Kiertiburanakul, S. Factors Associated With HIV-Related Stigma Among Healthcare Providers at a University Hospital in Nepal. J. Int. Assoc. Provid. AIDS Care 2024, 23, 23259582241282583. [Google Scholar] [CrossRef]
- Fauk, N.K.; Ward, P.R.; Hawke, K.; Mwanri, L. HIV Stigma and Discrimination: Perspectives and Personal Experiences of Healthcare Providers in Yogyakarta and Belu, Indonesia. Front. Med. 2021, 8, 625787. [Google Scholar] [CrossRef]
- Shah, S.; Elgalib, A.; Al-Wahaibi, A.; Al-Fori, M.; Raju, P.; Al-Skaiti, M.; Al-Mashani, H.N.; Duthade, K.; Omaar, I.; Muqeetullah, M.; et al. Knowledge, Attitudes and Practices Related to HIV Stigma and Discrimination Among Healthcare Workers in Oman. Sultan Qaboos Univ. Med. J. 2020, 20, e29–e36. [Google Scholar] [CrossRef]
- Du, H.; Chi, P.; Li, X. High HIV Prevalence Predicts Less HIV Stigma: A Cross-National Investigation. AIDS Care 2018, 30, 714–721. [Google Scholar] [CrossRef]
- Koseoglu Ornek, O.; Tabak, F.; Mete, B. Stigma in Hospital: An Examination of Beliefs and Attitudes Towards HIV/AIDS Patients, Istanbul. AIDS Care 2020, 32, 1045–1051. [Google Scholar] [CrossRef]
- Jiménez Forero, L.A. Casos de VIH: Una Tendencia en Aumento en el Marco del Aseguramiento en Colombia 2023. Available online: https://cuentadealtocosto.org/vih/dia-mundial-de-respuesta-al-vih-2023/ (accessed on 17 January 2025).
- Cano Blandón, R. Las fronteras en Colombia: Su origen, evolución, pérdida e importancia en las Relaciones Internacionales. Rev. Ciudad. Estados Y Política 2022, 9, 4. [Google Scholar] [CrossRef]
- Ministerio de Salud y Protección Social ¿Se Necesitan más Médicos Especialistas en Colombia? Available online: https://www.periodicoelpulso.com.co/301-octubre-2023/generales-2.php (accessed on 17 January 2025).
- Daniel, W.W.; Cross, C.L. Biostatistics: A Foundation for Analysis in the Health Sciences, 10th ed.; John Wiley & Sons: New York, NY, USA, 2013; Volume 1, ISBN 978-1-119-28237-2. [Google Scholar]
- Health Policy Project Midiendo Estigma Y Discriminación Hacia el VIH Entre Personas que Trabajan en Facilidades de Salud 2015. Available online: https://www.healthpolicyproject.com/pubs/49_SpanishStandardizedBriefQuestionnairersion.pdf (accessed on 17 January 2025).
- Joint United Nations Programme on HIV/AIDS the Indicators for Global AIDS Monitoring (GAM). Available online: https://indicatorregistry.unaids.org/ (accessed on 17 January 2025).
- Yuan, L.; Peng, X.; Wu, D.; Chen, S.; Tang, W.; Wang, H.; Zhou, J. Stigma Toward People Living with HIV Among Healthcare Providers in Midwifery Hospitals in Shenzhen, China from 2020 to 2023. Sci. Rep. 2025, 15, 6677. [Google Scholar] [CrossRef] [PubMed]
- Nyblade, L.; Jain, A.; Benkirane, M.; Li, L.; Lohiniva, A.-L.; McLean, R.; Turan, J.M.; Varas-Díaz, N.; Cintrón-Bou, F.; Guan, J.; et al. A Brief, Standardized Tool for Measuring HIV-Related Stigma Among Health Facility Staff: Results of Field Testing in China, Dominica, Egypt, Kenya, Puerto Rico and St. Christopher & Nevis. J. Int. AIDS Soc. 2013, 16, 18718. [Google Scholar] [CrossRef]
- Loaiza-Guevara, V.; Acosta, M.A.G.; Álvarez, A.V.A.; Martínez, V.A.; Montoya, M.C.M.; Ramírez, A.A.; Izquierdo-Condoy, J.S. Exploring Psychosocial Factors Influencing Sexually Transmitted Infection Intention Testing Among Medical Students: A Cross-Sectional Study in Two Universities. Front. Public. Health 2024, 12, 1407070. [Google Scholar] [CrossRef]
- Izquierdo-Condoy, J.S.; Simbaña-Rivera, K.; Nati-Castillo, H.A.; Cassa Macedo, A.; Cardozo Espínola, C.D.; Vidal Barazorda, G.M.; Palazuelos-Guzmán, I.; Trejo García, B.; Carrington, S.J.; Ortiz-Prado, E. How Much Do Latin American Medical Students Know About Radiology? Latin-American Multicenter Cross-Sectional Study. Med. Educ. Online 2023, 28, 2173044. [Google Scholar] [CrossRef]
- Izquierdo-Condoy, J.S.; Paz, C.; Nati-Castillo, H.A.; Gollini-Mihalopoulos, R.; Aveiro-Róbalo, T.R.; Paucar, J.R.V.; Mamami, S.E.L.; Caicedo, J.F.; Loaiza-Guevara, V.; Mejía, D.C.; et al. Impact of Mobile Phone Usage on Sleep Quality Among Medical Students Across Latin America: Multicenter Cross-Sectional Study. J. Med. Internet Res. 2025, 27, e60630. [Google Scholar] [CrossRef]
- Izquierdo-Condoy, J.S.; Arias-Intriago, M.; Nati-Castillo, H.A.; Gollini-Mihalopoulos, R.; Cardozo-Espínola, C.D.; Loaiza-Guevara, V.; Dalel-Gómez, W.; Villamil, J.; Suárez-Sangucho, I.A.; Morales-Lapo, E.; et al. Exploring Smartphone Use and Its Applicability in Academic Training of Medical Students in Latin America: A Multicenter Cross-Sectional Study. BMC Med. Educ. 2024, 24, 1401. [Google Scholar] [CrossRef]
- Petroll, A.E.; Mosack, K.E. Physician Awareness of Sexual Orientation and Preventive Health Recommendations to Men Who Have Sex With Men. Sex. Transm. Dis. 2011, 38, 63–67. [Google Scholar] [CrossRef]
- Dagostini, C.M.; Bicca, Y.D.A.; Ramos, M.B.; Busnello, S.; Gionedis, M.C.; Contini, N.; Falavigna, A. Patients’ Preferences Regarding Physicians’ Gender: A Clinical Center Cross-Sectional Study. Sao Paulo Med. J. 2022, 140, 134–143. [Google Scholar] [CrossRef]
- Langi, G.G.; Rahadi, A.; Praptoraharjo, I.; Ahmad, R.A. HIV-Related Stigma and Discrimination Among Health Care Workers During Early Program Decentralization in Rural District Gunungkidul, Indonesia: A Cross-Sectional Study. BMC Health Serv. Res. 2022, 22, 356. [Google Scholar] [CrossRef]
- Attal, B.A.; Al-Rowaishan, K.M.; Akeel, A.A.; AlAmmar, F.K. HIV Stigma in the Teaching Hospitals in Sana’a, Yemen: A Conflict and Low-Resource Setting. BMC Public. Health 2021, 21, 1793. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Infection Control Standard Precautions for All Patient Care. Available online: https://www.cdc.gov/infection-control/hcp/basics/standard-precautions.html (accessed on 5 April 2025).
- Gázquez-López, M.; Álvarez-Serrano, M.A.; Martín-Salvador, A.; Pérez-Morente, M.Á.; García-García, I.; González-García, A.; Martínez-García, E. Attitudes Towards People Living with HIV/AIDS Through the EAPVVS-E: A Descriptive Analysis in Nursing Students. Nurse Educ. Today 2025, 144, 106418. [Google Scholar] [CrossRef] [PubMed]
- Gruszczyńska, E.; Rzeszutek, M. HIV/AIDS Stigma Accumulation Among People Living with HIV: A Role of General and Relative Minority Status. Sci. Rep. 2023, 13, 10709. [Google Scholar] [CrossRef] [PubMed]
- Shahar, E.; Maor, C.; Moshe-Eilon, Y. Medical Personnel Knowledge and Stigmatic Attitude Toward HIV Patients in a High-Income Country. AIDS Care 2020, 32, 1023–1029. [Google Scholar] [CrossRef]
- Anderson, J.; Fenton, K. HIV Related Stigma: A Dangerous Roadblock. BMJ 2022, 379, o2989. [Google Scholar] [CrossRef]
- Rana, B.K.; Sarfraz, M.; Reza, T.E.; Emmanuel, F. A Cross-Sectional Study to Assess HIV/AIDS-Related Stigma and Its Drivers Among Dental Healthcare Providers in Islamabad, Pakistan. Cureus 2023, 15, e46769. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | % | |
|---|---|---|---|
| Sex | Male | 208 | 35.9 |
| Female | 371 | 64.1 | |
| Age (years) | 20–26 | 267 | 46.1 |
| 27–59 | 308 | 53.2 | |
| 60 or older | 4 | 0.7 | |
| Sexual orientation | Heterosexual | 504 | 87.0 |
| Non-heterosexual | 75 | 13.0 | |
| Work setting | Academia/research | 24 | 4.1 |
| Administrative | 15 | 2.6 | |
| Outpatient services | 290 | 50.1 | |
| Hospitalization | 85 | 14.7 | |
| Acute/critical care | 165 | 28.5 | |
| Years of work experience | 0–1 | 137 | 23.7 |
| 1–5 | 262 | 45.3 | |
| 5–10 | 101 | 17 | |
| More than 10 | 79 | 13.6 | |
| Experience in specialized HIV Units | No | 510 | 88.1 |
| Yes | 69 | 11.9 | |
| Knows someone with HIV diagnosis | No | 419 | 72.4 |
| Yes | 160 | 27.6 |
| Fear of Infection | ||||||
|---|---|---|---|---|---|---|
| Low Fear (n = 397) | High Fear (n = 182) | OR (95% CI) | ||||
| n | % | n | % | |||
| Demographic characteristics | ||||||
| Age (years) | 20–26 ref. | 172 | 64.4% | 95 | 35.6% | |
| 27–59 | 222 | 72.1% | 86 | 27.9% | 0.701 (0.493–0.998) | |
| 60 or older | 3 | 75.0% | 1 | 25.0% | 0.604 (0.062–5.883) | |
| Sex | Female ref. | 248 | 66.8% | 123 | 33.2% | |
| Male | 149 | 71.6% | 59 | 28.4% | 1.253 (0.864–1.815) | |
| Sexual orientation | Non-heterosexual ref. | 57 | 76.0% | 18 | 24.0% | |
| Heterosexual | 340 | 67.5% | 164 | 32.5% | 0.655 (0.373–1.148) | |
| Knows someone with HIV diagnosis | No ref. | 276 | 65.9% | 143 | 34.1% | |
| Yes | 121 | 75.6% | 39 | 24.4% | 0.622 (0.411–0.941) | |
| Professional characteristics | ||||||
| Work setting | Academia/research ref. | 17 | 70.8% | 7 | 29.2% | |
| Administrative | 12 | 80.0% | 3 | 20.0% | 0.607 (0.130–2.836) | |
| Outpatient services | 195 | 67.2% | 95 | 32.8% | 1.183 (0.747–2.950) | |
| Hospitalization | 54 | 63.5% | 31 | 36.5% | 1.394 (0.521–3.733) | |
| Acute/critical care | 119 | 72.1% | 46 | 27.9% | 0.939 (0.365–2.412) | |
| Years of work experience (years) | 0–1 ref. | 82 | 59.9% | 55 | 40.1% | |
| 1–5 | 181 | 69.1% | 81 | 30.9% | 0.667 (0.434–1026) | |
| 5–10 | 75 | 74.3% | 26 | 25.7% | 0.517 (0.295–0.906) | |
| More than 10 | 59 | 74.7% | 20 | 25.3% | 0.505 (0.274–0.931) | |
| Experience in specialized HIV units | No ref. | 346 | 67.8% | 164 | 32.3% | |
| Yes | 51 | 73.9% | 18 | 26.1% | 0.745 (0.422–1.315) | |
| Training for the care of PLHIV | ||||||
| Training on caring for people living with HIV | No ref. | 229 | 70.9% | 94 | 29.1% | |
| Yes | 168 | 65.6% | 88 | 34.4% | 1.276 (0.897–1.815) | |
| Training on infection control and universal precautions | No ref. | 201 | 66.6% | 101 | 33.4% | |
| Yes | 196 | 70.8% | 81 | 29.2% | 0.822 (0.578–1.170) | |
| Training on key populations | No ref. | 318 | 68.2% | 148 | 31.8% | |
| Yes | 79 | 69.9% | 34 | 30.1% | 0.925 (0.592–1.446) | |
| Training on stigma and discrimination | No ref. | 280 | 66.7% | 140 | 33.3% | |
| Yes | 117 | 73.6% | 42 | 26.4% | 0.478–1.078) | |
| Stigma Level | ||||||
|---|---|---|---|---|---|---|
| Low Stigma (n = 329) | High Stigma (n = 250) | OR (95% CI) | ||||
| n | % | n | % | |||
| Demographic characteristics | ||||||
| Age (years) | 20–26 ref. | 170 | 63.7% | 97 | 36.3% | |
| 27–59 | 157 | 50.8% | 151 | 49.2% | 1.66 (1.206–2.356) | |
| 60 or older | 2 | 50.0% | 2 | 50.0% | 1.753 (0.243–12.640) | |
| Sex | Female ref. | 218 | 58.8% | 153 | 41.2% | |
| Male | 111 | 53.4% | 95 | 46.6% | 1.245 (0.885–1.753) | |
| Sexual orientation | Non-heterosexual ref. | 52 | 69.3% | 23 | 30.7% | |
| Heterosexual | 277 | 55.0% | 227 | 45.0% | 1.853 (1.100–3.120) | |
| Knows someone with HIV diagnosis | No ref. | 236 | 56.3% | 183 | 43.7% | |
| Yes | 93 | 58.1% | 67 | 41.9% | 0.929 (0.643–1.343) | |
| Professional characteristics | ||||||
| Work setting | Academia/research ref. | 14 | 58.3% | 10 | 41.7% | |
| Administrative | 8 | 53.3% | 7 | 46.7% | 1.225 (0.334–4.491) | |
| Outpatient Services | 172 | 59.3% | 118 | 40.7% | 0.960 (0.413–2.235) | |
| Hospitalization | 43 | 50.6% | 42 | 49.4% | 1.367 (0.547–3.418) | |
| Acute/critical care | 92 | 55.8% | 73 | 44.2% | 1.111 (0.466–2.645) | |
| Years of work experience (years) | 0–1 ref. | 88 | 64.2% | 49 | 35.8% | |
| 1–5 | 152 | 58.0% | 110 | 42.0% | 1.300 (0.848–1.992) | |
| 5–10 | 53 | 52.5% | 48 | 47.5% | 1.626 (0.963–2.747) | |
| More than 10 | 36 | 45.6% | 43 | 43.2% | 2.145 (1.220–3.770) | |
| Experience in specialized HIV Units | No ref. | 293 | 57.5% | 217 | 42.5% | |
| Yes | 36 | 52.2% | 37 | 47.8% | 1.238 (0.748–2.049) | |
| Training for the care of PLHIV | ||||||
| Training on caring for people living with HIV | No ref. | 132 | 51.6% | 124 | 48.4% | |
| Yes | 197 | 61.0% | 126 | 39.0% | 0.681 (0.489–0.949) | |
| Training on infection control and universal precautions | No ref. | 163 | 54.0% | 139 | 46.0% | |
| Yes | 166 | 59.9% | 111 | 40.1% | 0.784 (0.564–1.091) | |
| Training on key populations | No ref. | 256 | 54.9% | 210 | 45.1% | |
| Yes | 73 | 64.4% | 40 | 35.4% | 0.668 (0.436–1.023) | |
| Training on stigma and discrimination | No ref. | 231 | 55.0% | 189 | 45.0% | |
| Yes | 98 | 61.6% | 61 | 38.4% | 0.761 (0.524–1.105) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loaiza-Guevara, V.; Martinez Rivera, J.P.; Castillo, J.S.; Gomez, W.D.; Deig Comerma, E.; Izquierdo-Condoy, J.S. HIV Stigma and Discrimination in Colombian Healthcare: Insights from a National Cross-Sectional Analysis of General Practitioners. Healthcare 2025, 13, 1013. https://doi.org/10.3390/healthcare13091013
Loaiza-Guevara V, Martinez Rivera JP, Castillo JS, Gomez WD, Deig Comerma E, Izquierdo-Condoy JS. HIV Stigma and Discrimination in Colombian Healthcare: Insights from a National Cross-Sectional Analysis of General Practitioners. Healthcare. 2025; 13(9):1013. https://doi.org/10.3390/healthcare13091013
Chicago/Turabian StyleLoaiza-Guevara, Valentina, Juliana Paola Martinez Rivera, Juan Sebastian Castillo, Widad Dalel Gomez, Elisabet Deig Comerma, and Juan S. Izquierdo-Condoy. 2025. "HIV Stigma and Discrimination in Colombian Healthcare: Insights from a National Cross-Sectional Analysis of General Practitioners" Healthcare 13, no. 9: 1013. https://doi.org/10.3390/healthcare13091013
APA StyleLoaiza-Guevara, V., Martinez Rivera, J. P., Castillo, J. S., Gomez, W. D., Deig Comerma, E., & Izquierdo-Condoy, J. S. (2025). HIV Stigma and Discrimination in Colombian Healthcare: Insights from a National Cross-Sectional Analysis of General Practitioners. Healthcare, 13(9), 1013. https://doi.org/10.3390/healthcare13091013