
Multifactorial Analysis of Oral Health-Related Quality of Life in Children with Special Health Care Needs: A Case-Control Study

 , , , and
, , , and
Abstract
1. Introduction
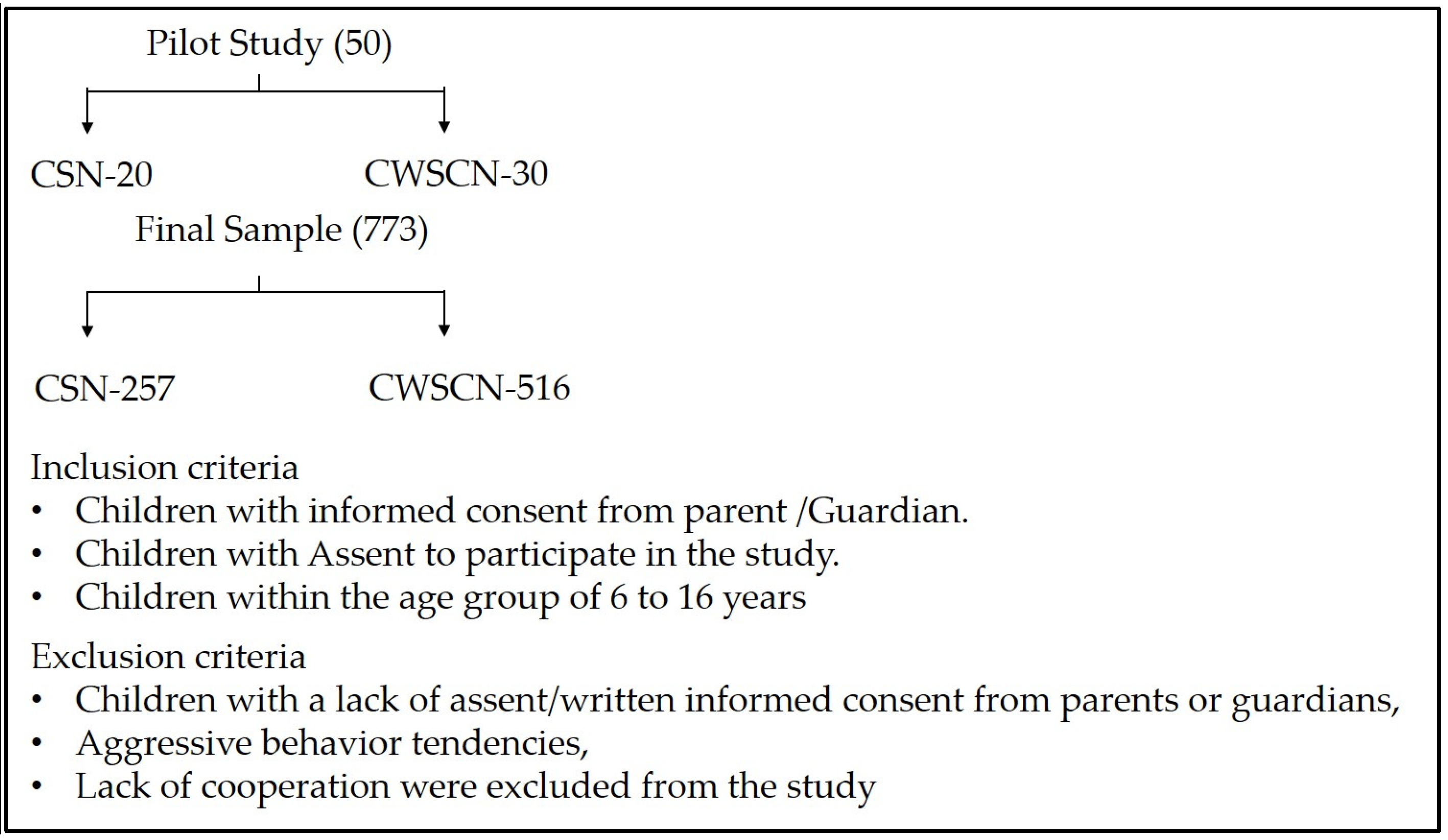
2. Materials and Methods
- Sociodemographic details: age, sex, parents’ education, parents’ occupation, and family income.
- Dietary habits: 72-h recall data, which spanned a weekend and 2 weekdays, number of meals, form, frequency, consistency, and time of sugar intake were recorded.
- Oral hygiene practices: Method of tooth cleaning, material used, frequency of cleaning, and use of fluoridated toothpaste.
- The medication history, previous dental visits, and type and duration of disability were also recorded.
- (1)
- Physical impact: A total of 9 questions (difficulty in pronunciation, deterioration of taste, diet unsatisfactory due to dental problems, interruption during meals due to dental problems, difficulty in relaxing due to dental problems, difficulty in doing usual jobs due to dental problems, totally unable to function due to dental issues, irritability with others due to dental problems, and less satisfaction in life due to dental issues).
- (2)
- Pain impact: Total of 2 questions (Pain in the mouth; Discomfort while chewing food).
- (3)
- Psychological impact: Total of 3 questions (self-conscious about teeth, mouth, and denture; tensed due to problems of teeth and mouth; embarrassment due to dental issues).
3. Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CSN | Children with Special needs |
| CWSCN | Children without special care needs |
| OHIP | Oral Health Impact Profile |
References
- American Academy of Pediatric Dentistry. Management of Dental Patients with Special Health care Needs. The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2024; pp. 343–350. [Google Scholar]
- Emerson, E.; Hatton, C. The socio-economic circumstances of children at risk of disability in Britain. Disabil. Soc. 2007, 22, 563–580. [Google Scholar] [CrossRef]
- Gavic, L.; Brekalo, M.; Tadin, A. Caregiver Perception of the Oral-Health-Related Quality of Life of Children with Special Needs: An Exploratory Study. Epidemiologia 2024, 5, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Patidar, D.; Sogi, S.; Patidar, D.C. Oral Health Status of Children with Special Healthcare Need: A Retrospective Analysis. Int. J. Clin. Pediatr. Dent. 2022, 15, 433–437. [Google Scholar] [PubMed]
- Alkhabuli, J.O.S.; Essa, E.Z.; Al-Zuhair, A.M.; Jaber, A.A. Oral health status and treatment needs for children with special needs: A cross-sectional study. Braz. Res. Pediatr. Dent. Integr. Clin. 2020, 19, e4877. [Google Scholar] [CrossRef]
- Mehta, V.; Tripathy, S.; Merchant, Y.; Mathur, A.; Negi, S.; Shamim, M.A.; Abullais, S.S.; Al-Qarni, M.A.; Karobari, M.I. Oral health status of children with intellectual and developmental disabilities in India: A systematic review and meta-analysis. BMC Pediatr. 2024, 24, 748. [Google Scholar] [CrossRef]
- Asiri, F.Y.I.; Tennant, M.; Kruger, E. Oral health of individuals with cerebral palsy in Saudi Arabia: A systematic review. Community Dent. Oral Epidemiol. 2024, 52, 121–129. [Google Scholar] [CrossRef]
- Dye, B.A. The Global Burden of Oral Disease: Research and Public Health Significance. J. Dent. Res. 2017, 96, 361–363. [Google Scholar] [CrossRef]
- Chimbinha, Í.G.M.; Ferreira, B.N.C.; Miranda, G.P.; Guedes, R.S. Oral-health-related quality of life in adolescents: Umbrella review. BMC Public Health 2023, 23, 1603. [Google Scholar] [CrossRef]
- Puthiyapurayil, J.; Anupam Kumar, T.V.; Syriac, G.R.M.; Kt, R.; Najmunnisa. Parental perception of oral health related quality of life and barriers to access dental care among children with intellectual needs in Kottayam, central Kerala—A cross sectional study. Spec. Care Dent. 2022, 42, 177–186. [Google Scholar] [CrossRef]
- Tounsi, A.; AlJameel, A.; AlKathiri, M.; AlAhmari, R.; Sultan, S.B. Oral Health-related Quality of Life of Children with Special Health Care Needs in Riyadh: A Cross-sectional Study. Oral Health Prev. Dent. 2024, 22, 285–292. [Google Scholar]
- Hegazi, F.; Alghamdi, N.; Alhajri, D.; Alabdulqader, L.; Alhammad, D.; Alshamrani, L.; Bedi, S.; Sharma, S. Association between Dental Fear and Children’s Oral Health-Related Quality of Life. Int. J. Environ. Res. Public Health 2024, 21, 1195. [Google Scholar] [CrossRef] [PubMed]
- Chai, H.H.; Sun, I.G.; Duangthip, D.; Gao, S.S.; Lo, E.C.M.; Chu, C.H. Oral Health-Related Quality of Life of Hong Kong Kindergarten Children Receiving Silver Diamine Fluoride Therapy. Dent. J. 2024, 12, 248. [Google Scholar] [CrossRef] [PubMed]
- Salerno, C.; Campus, G.; Bontà, G.; Vilbi, G.; Conti, G.; Cagetti, M.G. Oral health-related quality of life in children and adolescent with autism spectrum disorders and neurotypical peers: A nested case-control questionnaire survey. Eur. Arch. Paediatr. Dent. 2024, 26, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Abideen, M.Z.U.; Bushara, N.A.A.; Baig, M.N.; Siddiqui, Y.D.; Ejaz, I.; Tareen, J.; Siddiqui, A.A.; Bushara, N.A.A.; Dilshar, Y.D.; Siddiqui, A.A., III. Shining a Spotlight on Stigma: Exploring Its Impact on Oral Health-Seeking Behaviours Through the Lenses of Patients and Caregivers. Cureus 2024, 16, e63025. [Google Scholar]
- da Silva, G.C.B.; Firmino, R.T.; Nóbrega, W.F.S.; d’Ávila, S. Oral habits, sociopsychological orthodontic needs, and sociodemographic factors perceived by caregivers impact oral health-related quality of life in children with and without autism? Int. J. Paediatr. Dent. 2024, 34, 593–607. [Google Scholar] [CrossRef]
- Al-Qahtani, Z.; Wyne, A.H. Caries experience and oral hygiene status of blind, deaf and mentally retarded female children in Riyadh, Saudi Arabia. Odonto-Stomatol. Trop. Trop. Dent. J. 2004, 27, 37–40. [Google Scholar]
- Fink, K.; Alkayed, K.; Schwindling, F.S.; Wiesmüller, V. Oral Health-Related Quality of Life among Refugees: A Questionnaire-Based Study. Healthcare 2024, 12, 1525. [Google Scholar] [CrossRef]
- Gemp, S.; Ziebolz, D.; Haak, R.; Mauche, N.; Prase, M.; Dogan-Sander, E.; Görges, F.; Strauß, M.; Schmalz, G. Oral Health-Related Quality of Life in Adult Patients with Depression or Attention Deficit Hyperactivity Disorder (ADHD). J. Clin. Med. 2023, 12, 7192. [Google Scholar] [CrossRef]
- Slade, G.D. Derivation and validation of a short-form oral health impact profile. Community Dent. Oral Epidemiol. 1997, 25, 284–290. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health, Version for Children and Youth (ICFCY); WHO: Geneva, Switzerland, 2007. [Google Scholar]
- World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Almerich-Silla, J.M.; Montiel-Company, J.M.; Bellot-Arcís, C.; Almerich-Torres, G. Oral health-related quality of life in children with special health care needs: A systematic review and meta-analysis. J. Clin. Med. 2021, 10, 4329. [Google Scholar]
- Costa, M.F.; de Souza, M.C.; de Souza, E.H.A.; de Oliveira, A.C.B.; Martins, C.C. Oral health-related quality of life of children with cerebral palsy and their families. Spec. Care Dent. 2022, 42, 161–168. [Google Scholar]
- El Tantawi, M.; AlAnsari, A. Oral health-related quality of life of children with autism spectrum disorder: A cross-sectional study. BMC Oral. Health 2021, 21, 1–8. [Google Scholar]
- Farsi, N.J.; Alsharif, A.M.; Almutairi, A.A. Oral health status and oral health-related quality of life in children with Down syndrome: A systematic review. Spec. Care Dent. 2023, 43, 19–32. [Google Scholar]
- Gomes, C.C.; Ribeiro, R.A.; Ferreira, E.F.; Abreu, M.H. Impact of oral health conditions on the quality of life of children with intellectual disabilities. BMC Oral. Health 2020, 20, 55. [Google Scholar]
- Liu, Y.; Wang, Y.; Sun, X.; Zhang, Y. Oral health status and oral health-related quality of life in children with congenital heart disease. Front. Pediatr. 2023, 11, 1111663. [Google Scholar]
- Twetman, S.; Fontana, M. Prevention of dental caries in children with special health care needs: A systematic review. Acta Odontol. Scand. 2021, 79, 1–10. [Google Scholar]
- Zotti, F.; Dalessandri, D.; Visetti, G.; Paganelli, C.; Caprio, M. Oral health-related quality of life in children with rare diseases: A cross-sectional study. Orphanet J. Rare Dis. 2022, 17, 1–10. [Google Scholar]
- Adulyanon, S.; Vourapukjaru, J.; Sheiham, A. Oral impacts affecting daily performance in a low dental disease Thai population. Community Dent. Oral Epidemiol. 1996, 24, 385–389. [Google Scholar] [CrossRef]
- Atchison, K.A.; Dolan, T.A. Development of the Geriatric Oral Health Assessment Index. J. Dent. Educ. 1990, 54, 680–687. [Google Scholar] [CrossRef]
- Slade, G.D.; Spencer, A.J. Development and evaluation of the Oral Health Impact Profile. Community Dent. Health 1994, 11, 3–11. [Google Scholar]
- John, M.T.; Reissmann, D.R.; Čelebić, A.; Baba, K.; Kende, D.; Larsson, P.; Rener-Sitar, K. Integration of oral health-related quality of life instruments. J. Dent. 2016, 53, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Campos, L.A.; Peltomäki, T.; Marôco, J.; Campos, J.A.D.B. Use of Oral Health Impact Profile-14 (OHIP-14) in Different Contexts. What Is Being Measured? Int. J. Environ. Res. Public Health 2021, 18, 13412. [Google Scholar] [CrossRef] [PubMed]
- Quadri, M.F.A.; Alwadani, M.A.; Talbi, K.M.; Hazzazi, R.A.A.; Eshaq, R.H.A.; Alabdali, F.H.J.; Wadani, M.H.M.; Tartaglia, G.; Ahmad, B. Exploring associations between oral health measures and oral health-impacted daily performances in 12–14-year-old schoolchildren. BMC Oral Health 2022, 22, 304. [Google Scholar] [CrossRef] [PubMed]
- Ningrum, V.; Bakar, A.; Shieh, T.M.; Shih, Y.H. The Oral Health Inequities between Special Needs Children and Normal Children in Asia: A Systematic Review and Meta-Analysis. Healthcare 2021, 9, 410. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.; Robertson, A.S.; Phelps, S. Unmet Dental Care Needs Among Children with Special Health Care Needs: Implications for the Medical Home. Pediatrics 2005, 116, e426–e431. [Google Scholar] [CrossRef]
- Al-Maweri, S.A.; Halboub, E.S.; Al-Soneidar, W.A.; Al-Sufyani, G.A. Oral lesions and dental status of autistic children in Yemen: A case-control study. J. Int. Soc. Prev. Community Dent. 2014, 4 (Suppl. S3), S199–S203. [Google Scholar] [CrossRef]
- Yashoda, R.; Puranik, M.P. Oral health status and parental perception of child oral health related quality-of-life of children with autism in Bangalore, India. J. Indian Soc. Pedod. Prev. Dent. 2014, 32, 135–139. [Google Scholar]
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31 (Suppl. S1), 3–23. [Google Scholar] [CrossRef]
- Almajed, O.S.; Alayadi, H.; Sabbah, W. Inequalities in the Oral Health-Related Quality of Life Among Children in Saudi Arabia. Cureus 2023, 15, e49456. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Di Blasio, M.; Ronsivalle, V.; Cicciù, M. Children oral health and parents education status: A cross-sectional study. BMC Oral Health 2023, 23, 787. [Google Scholar] [CrossRef]
- Chaffee, B.W.; Rodrigues, P.H.; Kramer, P.F.; Vítolo, M.R.; Feldens, C.A. Oral health-related quality-of-life scores differ by socioeconomic status and caries experience. Community Dent. Oral Epidemiol. 2017, 45, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Ellakany, P.; Madi, M.; Fouda, S.M.; Ibrahim, M.; AlHumaid, J. The Effect of Parental Education and Socioeconomic Status on Dental Caries among Saudi Children. Int. J. Environ. Res. Public Health 2021, 18, 11862. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; König, H.-H.; Kretzler, B.; Zwar, L.; Lieske, B.; Seedorf, U.; Walther, C.; Aarabi, G. Does Oral Health-Related Quality of Life Differ by Income Group? Findings from a Nationally Representative Survey. Int. J. Environ. Res. Public. Health 2022, 19, 10826. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Peres, M.A.; Watt, R.G. The Relationship between Income and Oral Health: A Critical Review. J. Dent. Res. 2019, 98, 853–860. [Google Scholar] [CrossRef]
- Alsubaie, A.M.; Almohaimede, K.A.; Aljadoa, A.F.; Jarallah, O.J.; Althnayan, Y.I.; Alturki, Y.A. Socioeconomic factors affecting patients’ utilization of primary care services at a Tertiary Teaching Hospital in Riyadh, Saudi Arabia. J. Fam. Community Med. 2016, 23, 6–11. [Google Scholar] [CrossRef]
- Alahmadi, Y.M. Evaluation of Health Literacy and Associated Factors Among Adults Living in Saudi Arabia: A Cross-Sectional Study. Inq. A J. Med. Care Organ. Provis. Financ. 2023, 60, 469580231161428. [Google Scholar] [CrossRef]
- Almajed, O.S.; Aljouie, A.A.; Alharbi, M.S.; Alsulaimi, L.M. The Impact of Socioeconomic Factors on Pediatric Oral Health: A Review. Cureus 2024, 16, e53567. [Google Scholar] [CrossRef]
- AlHaqwi, A.I.; AlDrees, T.M.; AlRumayyan, A.; AlFarhan, A.I.; Alotaibi, S.S.; AlKhashan, H.I.; Badri, M. Shared clinical decision making. A Saudi Arabian perspective. Saudi Med. J. 2015, 36, 1472–1476. [Google Scholar] [CrossRef]
- AlFaris, E.; Irfan, F.; Abouammoh, N.; Zakaria, N.; Ahmed, A.M.; Kasule, O.; Aldosari, D.M.; AlSahli, N.A.; Alshibani, M.G.; Ponnamperuma, G. Physicians’ professionalism from the patients’ perspective: A qualitative study at a single-family practice in Saudi Arabia. BMC Med. Ethics 2023, 24, 39. [Google Scholar] [CrossRef]
- Moynihan, P.; Petersen, P.E. Diet, nutrition and the prevention of dental diseases. Public. Health Nutr. 2004, 7, 201–226. [Google Scholar] [CrossRef]
- dos Santos, A.P.; Nadanovsky, P.; de Oliveira, B.H. A systematic review and meta-analysis of the effects of fluoride toothpastes on the prevention of dental caries in the primary dentition of preschool children. Community Dent. Oral Epidemiol. 2013, 41, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Al-Rethaiaa, A.S.; Fahmy, A.E.; Al-Shwaiyat, N.M. Obesity and eating habits among college students in Saudi Arabia: A cross-sectional study. Nutr. J. 2010, 9, 39. [Google Scholar] [CrossRef] [PubMed]
- Alsadhan, S. Oral health practices and dietary habits of intermediate school children in Riyadh, Saudi Arabia. Saudi Dent. J. 2016, 28, 85–91. [Google Scholar]
- Algarni, A.A.; Aljohani, M.A.; Mohammedsaleh, S.A.; Alrehaili, R.O.; Zulali, B.H. Awareness of professional fluoride application and its caries prevention role among women in KSA. J. Taibah Univ. Med. Sci. 2022, 17, 1000–1005. [Google Scholar] [CrossRef]
- Alshehri, M.; Kujan, O. Parental views on fluoride tooth brushing and its impact on oral health: A cross-sectional study. J. Int. Soc. Prev. Community Dent. 2015, 5, 451–456. [Google Scholar]

{kind=link}
| Variables | CSN (n = 257) | Percentage | CWSCN (n = 516) | Percentage |
|---|---|---|---|---|
| Age of child | ||||
| 6–11-yrs | 137 | 53.3 | 241 | 46.7 |
| 12–16-yrs | 120 | 46.7 | 275 | 53.3 |
| Sex | ||||
| Male | 132 | 51.4 | 270 | 52.3 |
| Female | 125 | 48.6 | 246 | 47.7 |
| Parental education | ||||
| Primary school or less | 45 | 17.5 | 77 | 14.9 |
| Intermediate and high | 212 | 82.5 | 439 | 85.1 |
| Parental occupation | ||||
| Both parents in job | 33 | 12.8 | 143 | 27.7 |
| One of the parent in job | 224 | 87.2 | 373 | 72.3 |
| Family income/month | ||||
| ≤10,000 SR | 175 | 68.1 | 222 | 43.0 |
| >10,000 SR | 82 | 31.9 | 294 | 57.0 |
| Variables | Oral Health Impact Profile (Mean ± SD) | |||
|---|---|---|---|---|
| Physical Impact | Pain Impact | Psychological Impact | Personal Satisfaction | |
| Age of child | ||||
| CSN-6–11-yrs (n = 137) | 2.7 ± 2.0 | 3.1 ± 2.1 | 2.9 ± 1.8 | 3.2 ± 1.8 |
| CWSCN-6–11-yrs (n = 241) | 2.1 ± 0.9 | 2.2 ± 0.8 | 1.3 ± 0.7 | 2.3 ± 0.9 |
| t test, p value | 0.041 | 0.032 | 0.018 | 0.001 |
| CSN-12–16-yrs (n = 120) | 3.5 ± 1.8 | 3.8 ± 1.9 | 3.1 ± 2.1 | 2.9 ± 1.3 |
| CWSCN-12–16-yrs (n = 275) | 2.3 ± 0.9 | 2.4 ± 0.9 | 2.2 ± 0.9 | 2.1 ± 0.7 |
| t test, p value | 0.031 | 0.043 | 0.052 | 0.061 |
| Sex | ||||
| CSN | ||||
| Male (n = 132) | 3.3 ± 1.9 | 3.4 ± 1.9 | 2.5 ± 1.5 | 2.7 ± 0.9 |
| Female (n = 125) | 2.9 ± 1.3 | 2.9 ± 1.2 | 3.0 ± 1.7 | 2.5 ± 0.8 |
| t test, p value | 0.041 | 0.043 | 0.044 | 0.051 |
| CWSCN | ||||
| Male (n = 270) | 2.4 ± 1.0 | 2.7 ± 1.3 | 2.4 ± 1.1 | 2.1 ± 0.5 |
| Female (n = 246) | 2.2 ± 0.7 | 2.5 ± 0.9 | 2.9 ± 1.3 | 2.4 ± 0.7 |
| t test | 0.063 | 0.051 | 0.042 | 0.054 |
| Parental education | ||||
| CSN | ||||
| Primary school or less (n = 45) | 3.3 ± 1.6 | 3.1 ± 1.4 | 3.4 ± 1.6 | 2.7 ± 1.1 |
| Intermediate and high (n = 212) | 2.4 ± 1.1 | 2.5 ± 1.1 | 2.7 ± 1.3 | 2.2 ± 0.9 |
| t test, p value | 0.001 | 0.001 | 0.003 | 0.053 |
| CWSCN | ||||
| Primary school or less (n = 77) | 2.8 ± 1.2 | 2.7 ± 1.3 | 2.9 ± 1.4 | 2.6 ± 1.1 |
| Intermediate and high (n = 439) | 2.2 ± 0.8 | 2.1 ± 0.6 | 2.3 ± 1.1 | 2.2 ± 0.9 |
| t test, p value | 0.042 | 0.046 | 0.043 | 0.053 |
| Parental occupation | ||||
| CSN | ||||
| Both parents in job (n = 33) | 3.2 ± 1.6 | 3.3 ± 1.7 | 3.1 ±1.7 | 2.7 ± 1.5 |
| One of the parents in the job (n = 224) | 3.1 ± 1.6 | 2.9 ± 1.3 | 3.2 ± 1.7 | 2.3 ± 0.9 |
| t test, p value | 0.062 | 0.051 | 0.121 | 0.073 |
| CWSCN | ||||
| Both parents in job (n = 143) | 2.4 ± 0.9 | 2.5 ± 1.1 | 2.7 ±1.3 | 2.5 ± 1.1 |
| One of the parents in the job (n = 373) | 2.3 ±0.7 | 2.1 ± 0.7 | 2.3 ± 1.1 | 2.1 ± 0.8 |
| t test, p value | 0.062 | 0.052 | 0.064 | 0.063 |
| Family income/month | ||||
| CSN | ||||
| ≤10,000 SR (n = 175) | 3.1 ± 1.5 | 3.2 ± 1.7 | 2.9 ± 1.5 | 2.9 ± 1.6 |
| >10,000 SR (n = 82) | 2.9 ± 1.2 | 2.8 ± 1.2 | 2.6 ± 1.1 | 2.7 ± 1.1 |
| t test, p value | 0.052 | 0.051 | 0.052 | 0.063 |
| CWSCN | ||||
| ≤10,000 SR (n = 222) | 2.5 ± 1.3 | 2.3 ± 1.1 | 2.4 ± 1.1 | 2.7 ± 1.1 |
| >10,000 SR (n = 294) | 2.3 ± 1.1 | 2. 1 ± 0.9 | 2.6 ± 1.2 | 2.3 ± 0.7 |
| t test, p value | 0.064 | 0.052 | 0.071 | 0.063 |
| Variables | Groups | Oral Health Impact Profile (Mean ± SD) | |||
|---|---|---|---|---|---|
| Physical Impact | Pain Impact | Psychological Impact | Personal Satisfaction | ||
| Special need status | CSN (n = 257) | 2.8 ± 1.6 | 3.1 ± 1.8 | 2.9 ± 1.4 | 3.2 ± 1.7 |
| CWSCN (n = 516) | 2.3 ± 1.1 | 2.6 ± 1.2 | 2.5 ± 1.1 | 2.4 ± 1.1 | |
| t test | 0.021 | 0.001 | 0.027 | 0.001 | |
| Caries status | With caries (n = 714) | 3.1 ± 1.6 | 3.4 ± 1.9 | 3.2 ± 1.8 | 3.1 ± 1.6 |
| Caries free (n = 59) | 1.2 ± 0.3 | 1.1 ± 0.1 | 1.3 ± 1.2 | 2.1 ± 0.8 | |
| t test | 0.001 | 0.001 | 0.001 | 0.001 | |
| Dietary status | Frequent Sugar consumption (n = 421) | 2.7 ± 1.3 | 2.9 ± 1.4 | 3.2 ± 1.9 | 2.9 ± 0.7 |
| No frequent consumption (n = 352) | 2.1 ± 1.1 | 2.2 ± 1.3 | 2.5 ± 1.6 | 2.2 ± 1.1 | |
| t test | 0.042 | 0.041 | 0.023 | 0.041 | |
| Oral hygiene status (Tooth brushing frequency) | ≥two times daily (n = 178) | 2.2 ± 1.1 | 2.4 ± 1.1 | 2.1 ± 0.9 | 2.2 ± 1.1 |
| ≤once daily (n = 595) | 2.7 ± 1.5 | 2.8 ± 1.5 | 3.2 ± 1.5 | 2.7 ± 1.2 | |
| t test | 0.032 | 0.041 | 0.001 | 0.033 | |
| Material used to clean tooth | FT (n = 268) | 2.3 ± 1.1 | 2.2 ± 1.1 | 2.4 ± 1.1 | 2.3 ± 0.9 |
| NFT (n = 455) | 2.9 ± 1.5 | 3.1 ± 1.6 | 2.7 ± 1.5 | 2.9 ± 1.2 | |
| Do not know (n = 50) | 2.4 ± 1.1 | 2.3 ± 1.1 | 2.2 ± 0.9 | 2.5 ± 1.1 | |
| ANOVA, p value | 0.031 | 0.027 | 0.028 | 0.031 | |
| Tukey-Post Hoc | NFT > FT | NFT > FT | NFT > FT | NFT > FT | |
| OHIP | B | Adjusted OR | Lower Bound | Upper Bound | p Value |
|---|---|---|---|---|---|
| Intercept | −2.312 | 0.023 | |||
| CSN | 1.172 | 3.11 | 1.23 | 5.21 | 0.0001 |
| CWSCN # | 1.0 | ||||
| 6–11-yr # | 1.0 | ||||
| 12–16-yr | 0.54 | 1.02 | 0.01 | 1.69 | 0.053 |
| Male | 1.642 | 1.87 | 0.12 | 2.89 | 0.024 |
| Female # | 1.0 | ||||
| Primary school or less education | 1.792 | 1.92 | 0.17 | 3.11 | 0.029 |
| Intermediate or higher # | 1.0 | ||||
| With caries | 1.282 | 2.96 | 1.16 | 5.11 | 0.0001 |
| Caries free # | 1.0 | ||||
| Frequent Sugar consumption | 1.103 | 1.63 | 0.08 | 3.12 | 0.041 |
| No frequent Sugar consumption # | 1.0 | ||||
| ≥two times daily # | 1.0 | ||||
| ≤once daily | 1.141 | 1.89 | 0.12 | 4.17 | 0.031 |
| Fluoridated toothpaste # | 1.0 | ||||
| Non-fluoridated toothpaste | 0.84 | 2.11 | 0.91 | 4.88 | 0.0001 |
| Do not know | 0.53 | 0.82 | 0.01 | 1.22 | 0.124 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fahmi, M.K.; Basha, S.; Noor Mohamed, R.; Redwan, A.; Alsaggaf, A.U.; Morad, M.H.S.; Al-Thobaiti, Y.E. Multifactorial Analysis of Oral Health-Related Quality of Life in Children with Special Health Care Needs: A Case-Control Study. Healthcare 2025, 13, 919. https://doi.org/10.3390/healthcare13080919
Fahmi MK, Basha S, Noor Mohamed R, Redwan A, Alsaggaf AU, Morad MHS, Al-Thobaiti YE. Multifactorial Analysis of Oral Health-Related Quality of Life in Children with Special Health Care Needs: A Case-Control Study. Healthcare. 2025; 13(8):919. https://doi.org/10.3390/healthcare13080919
Chicago/Turabian StyleFahmi, Mohammed Khalil, Sakeenabi Basha, Roshan Noor Mohamed, Alaa Redwan, Arwa U. Alsaggaf, Majd Hashim S. Morad, and Yasser Eid Al-Thobaiti. 2025. "Multifactorial Analysis of Oral Health-Related Quality of Life in Children with Special Health Care Needs: A Case-Control Study" Healthcare 13, no. 8: 919. https://doi.org/10.3390/healthcare13080919
APA StyleFahmi, M. K., Basha, S., Noor Mohamed, R., Redwan, A., Alsaggaf, A. U., Morad, M. H. S., & Al-Thobaiti, Y. E. (2025). Multifactorial Analysis of Oral Health-Related Quality of Life in Children with Special Health Care Needs: A Case-Control Study. Healthcare, 13(8), 919. https://doi.org/10.3390/healthcare13080919