
Examining the Relationship Between Urinary Incontinence and Women’s Physical Activity Engagement: Barriers and Disclosure Patterns


Abstract
1. Introduction
- Aid practitioners’ knowledge of urinary incontinence’s impact on women’s PA participation through the exploration of women’s perceptions and experiences of urine leakage during exercise;
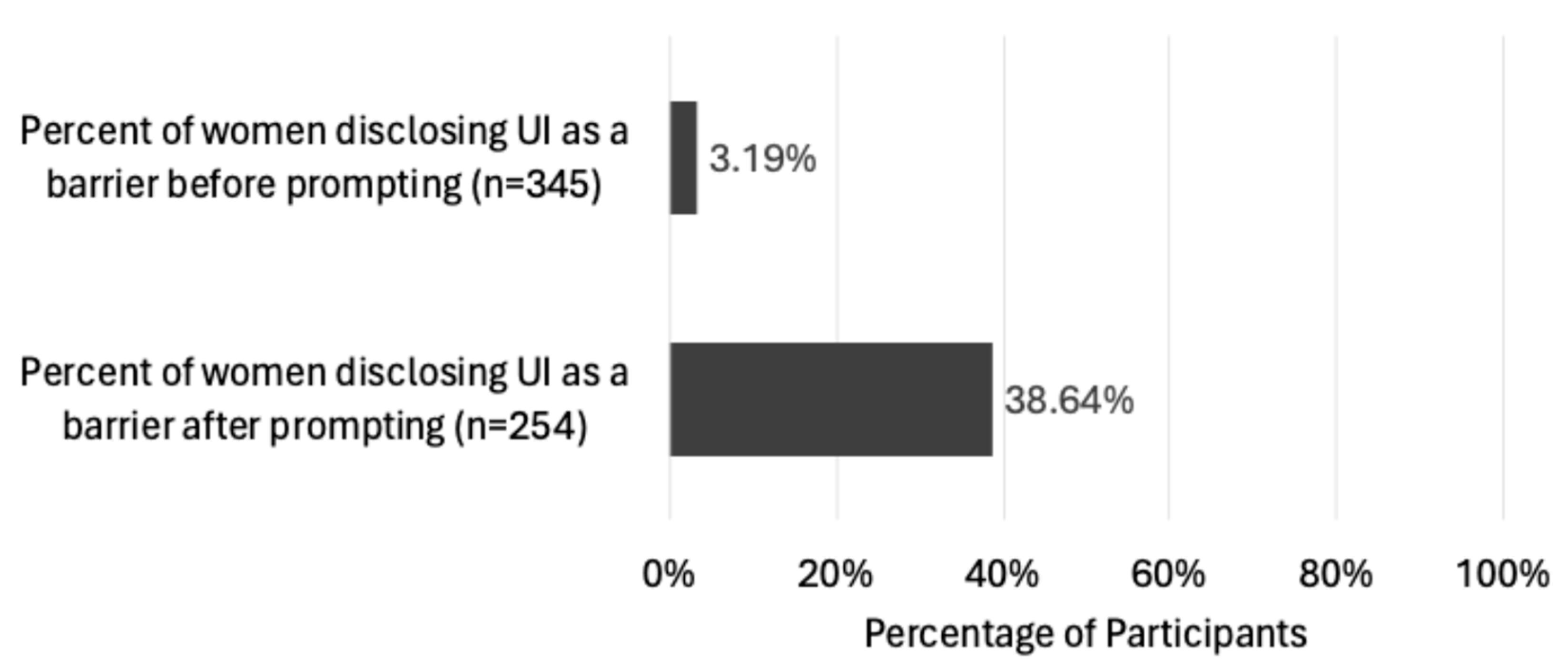
- Test whether women will disclose their UI status unprompted when questioned about barriers to PA;
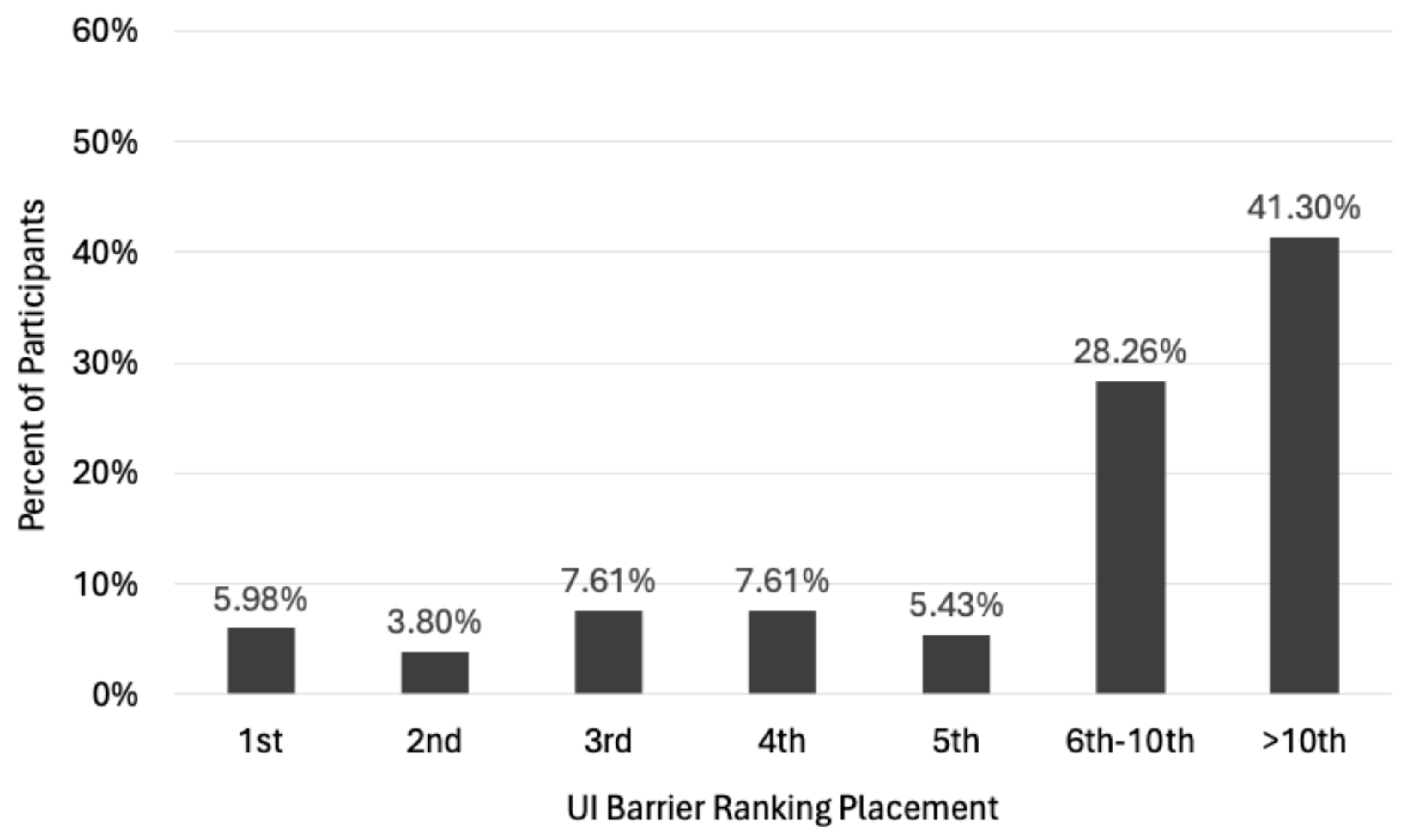
- Gain an understanding of where UI ranks amongst the most common barriers women experience to their PA participation;
- Gather insights into women’s UI disclosure both in and out of the PA environment.
2. Materials and Methods
2.1. Study Design
2.2. Procedure
2.2.1. Phase 1 Survey Participants and Recruitment
2.2.2. Phase 2 Interview Participants and Recruitment
2.3. Data Collection
2.3.1. Survey Materials and Data Collection (Phase 1)
2.3.2. Interview Schedule and Data Collection (Phase 2)
2.4. Data Analysis
2.4.1. Phase 1 Survey Data Analysis
2.4.2. Phase 2 Interview Data Analysis
3. Results and Discussion
3.1. Phase 1 Survey Findings
3.1.1. UI Prevalence Rate
3.1.2. Disclosing UI in the PA Setting
3.1.3. Ranking UI as a Barrier to PA
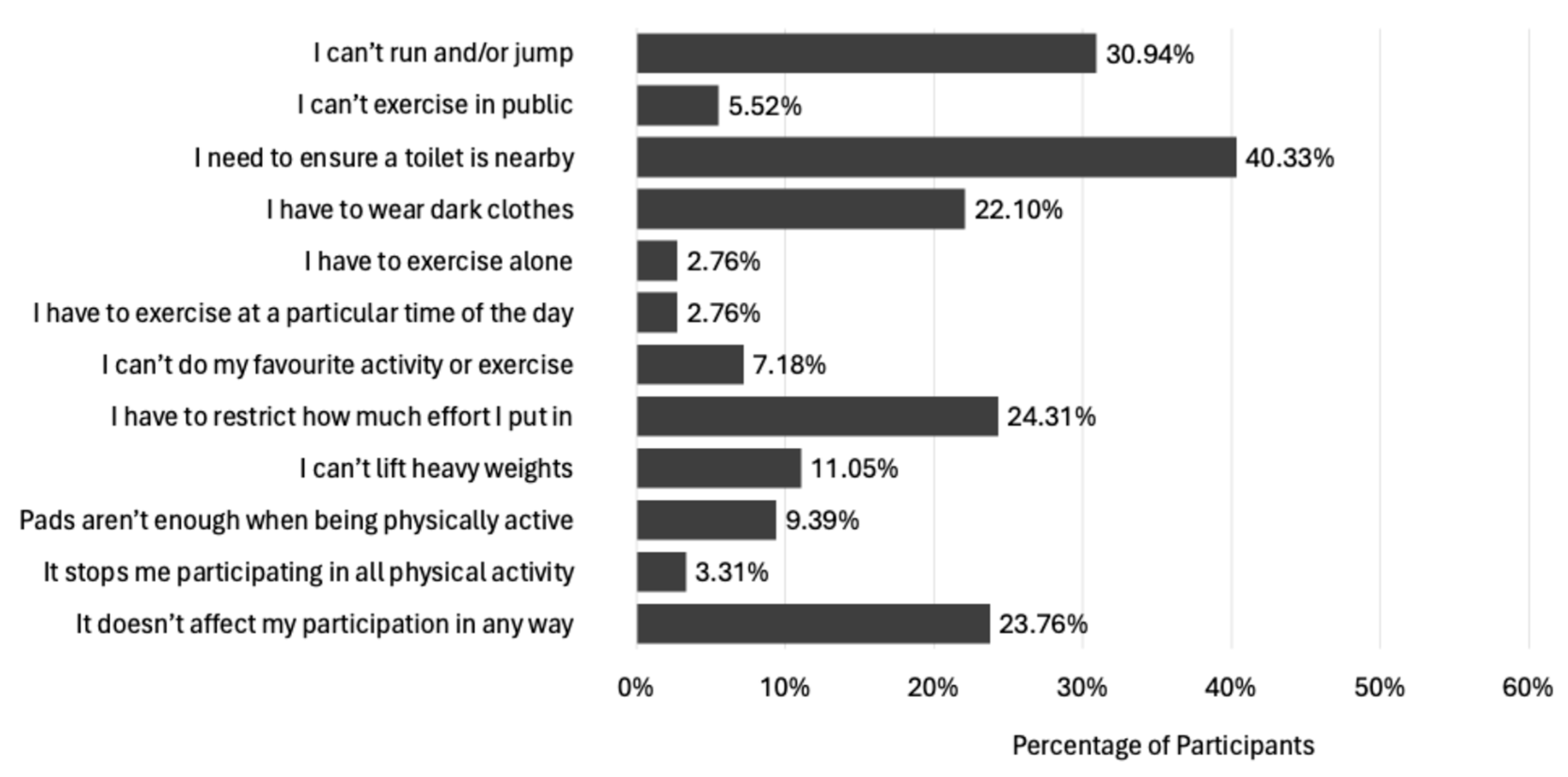
3.1.4. Effect of UI on PA Participation
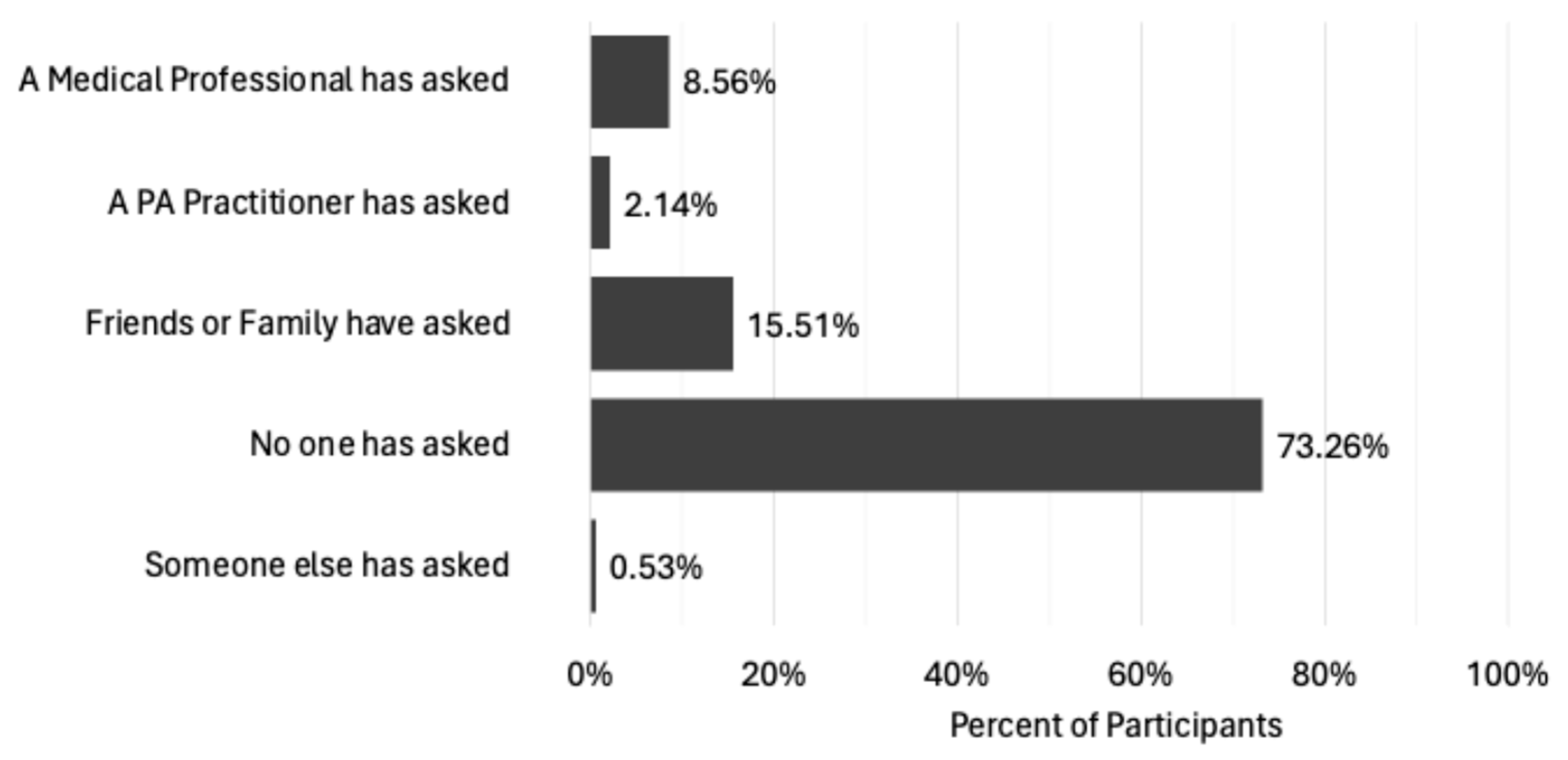
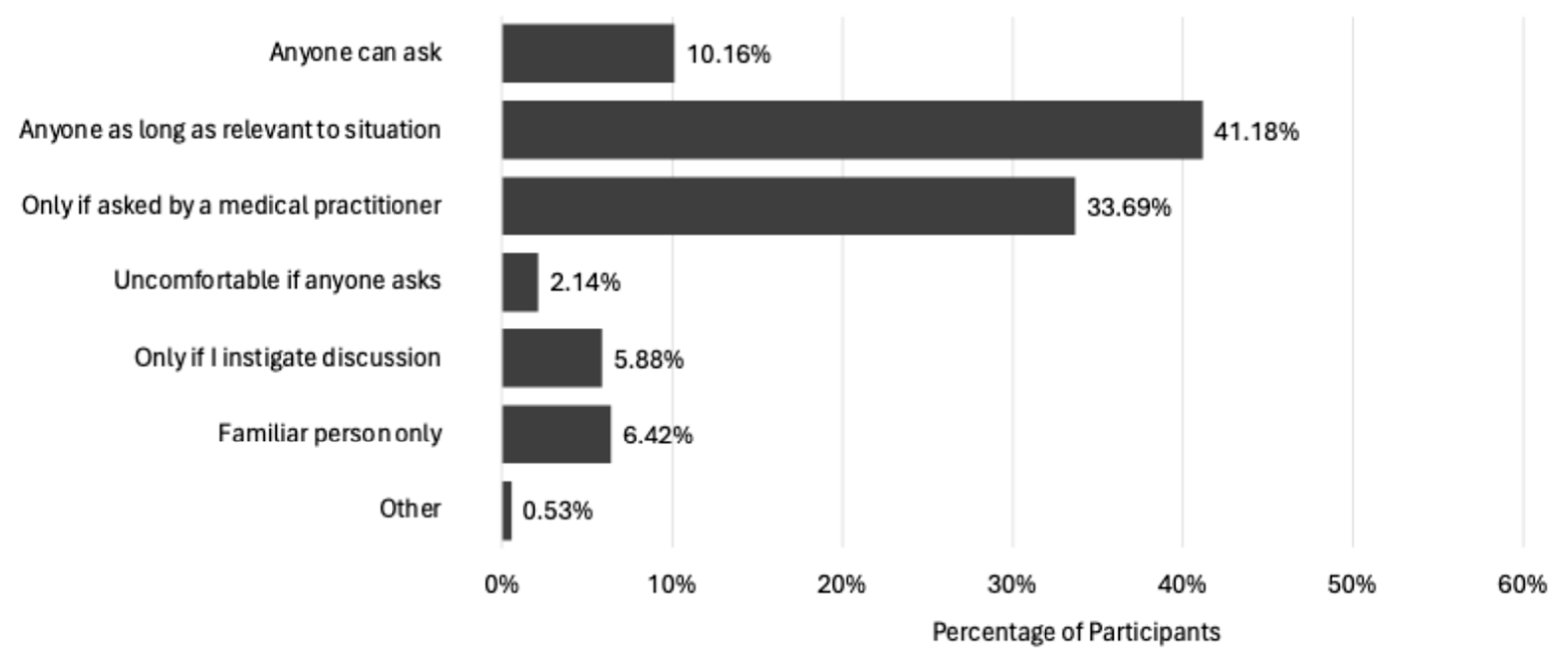
3.1.5. Being Asked to Disclose Symptoms by Others
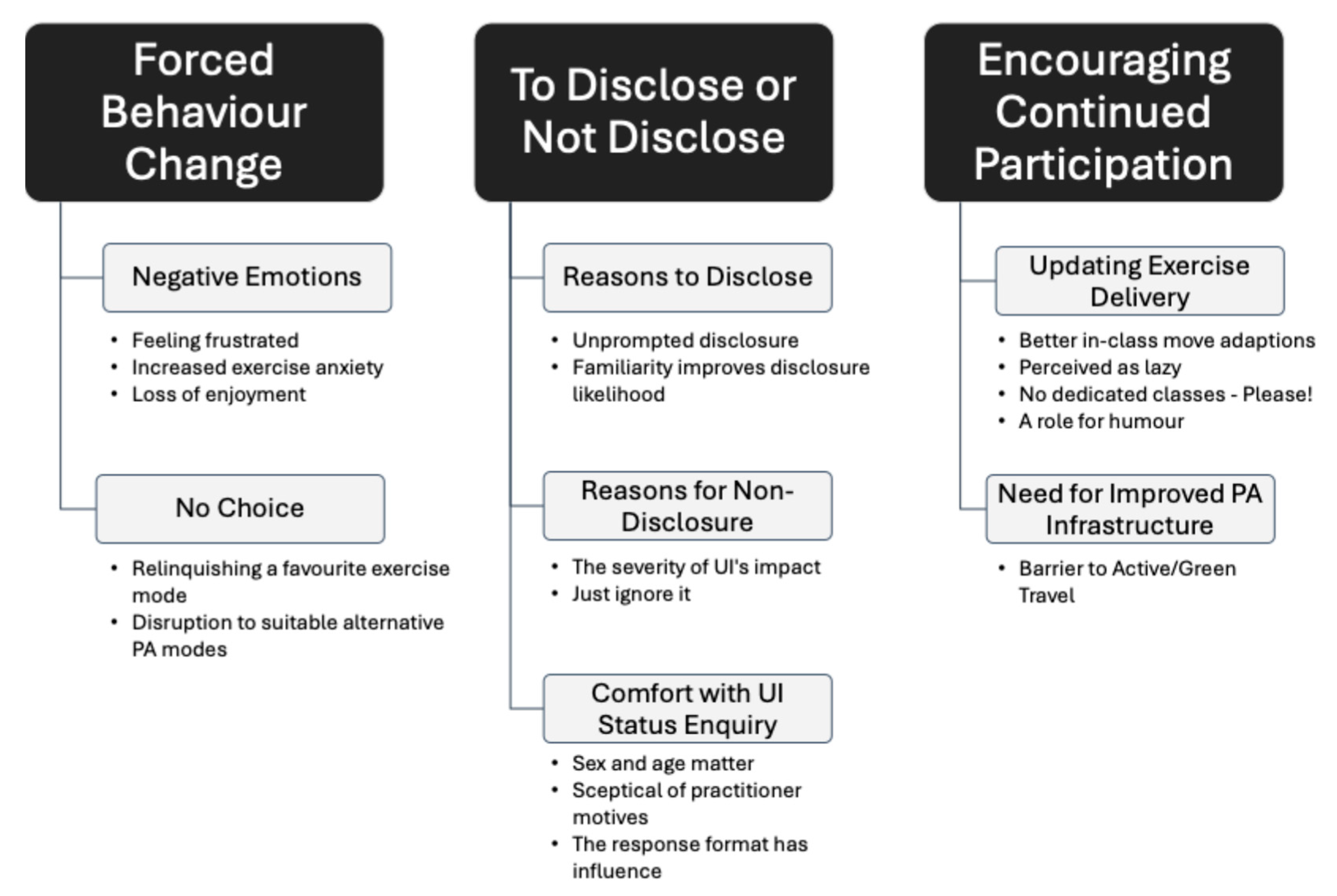
3.2. Phase 2 Interview Findings
3.2.1. Forced Behaviour Change
- Negative Emotions
“I think when I’m exercising it is that frustration of doing this because I want to get fitter. It’s frustrating, and it does make me feel angry, but I think what frustrates me the most is that the whole time I’m doing any exercise I’m always thinking about wetting”.
“I think it’s that I know I’m capable of doing more, but I don’t, because I don’t want to leak, I don’t want to be embarrassed and don’t want to feel horrible. So, I kind of feel like I’m doing half of the work that I should be doing and that I could do more”.
“I’m worried about it happening when it happens, after it happens, and it gets to the stage where you just think, ‘Oh, I just don’t want to do it’”.
“It’s the number one thing. I feel it even before I start the exercise, the anxiousness of ‘Oh God, is it actually going to happen’? You know, ‘will I get through this type of exercise without leaking or not?’”.
“I’m so focused on what’s happening in my body that I feel if I lose that concentration by talking and engaging and being present in the class, my concentration breaks on holding it all together and holding it all in. So, you know, you lose the enjoyment”.
- No Choice
“I don’t do the exercise I want to do, I do the exercise I’ve worked out I can do. And that’s the thing for me, that I would do more, and I would do different, but I don’t trust myself, and I don’t want to be in an awkward position”.
“That’s another barrier for me, the fact that can people smell me? The fact that I’m incontinent. It frightens me that other people think I smell”.
“I started trying different things like, could I do a keep-fit class? Or could I do a HIIT class or something? And I couldn’t. I wasn’t getting through any of them”.
“There’s a few classes that have popped up locally and I’ve thought ‘Oh, I’d quite like to do that’, and then I’ve thought ‘mmmm, probably just be getting myself all wet and...’, you know, that just puts me off, and I just think nah, I don’t want to do it”.
“Where I live, it’s about a mile and a half into town. I walk into town providing that my first stop has got a loo. Even in supermarkets before I set off home, I’ll think about if I need to use the loo”.
“Sometimes I think I’m perfectly fine, I’ve not had an incident, and then I’ll just walk up the street five minutes, and then it’s running down my leg and I’ve got turn around and come back”.
“It’s a mental barrier I have to overcome to even do anything. I think it’s because I was so active and fit before, where I was the one at the front leading everything and being the one that everybody looked to and now, I hide away and I’m not able to manage [exercise]”.
3.2.2. To Disclose or Not Disclose
- Reasons to Disclose UI Status
“Why did I write it? Because wetting myself stops me doing stuff. I mean, I belong to a gym, I’m okay going on the machines because you wipe the machines down afterwards and everything, but I can’t do spin or anything like that”.
“Because it’s a serious issue for me in the sense of you know, I think when you’ve been very fit and then all of a sudden to feel the mental health impact of not exercising, you know, and then trying to adapt your practice to cope with that”.
- Reasons for Non-Disclosure of UI Status
“I think it’s because you start to think, well, I really don’t want it to be a barrier. It is, but I don’t want it to be. Embarrassment would be why maybe I didn’t write it down as a cause. But I am aware that it is my number one cause, the leaking, and the urgency for needing to go to the toilet. I am aware that that is the problem for me with a lot of things. I mean, I’ve got a skipping rope. I’ve got a hula hoop, and they’re things that, just at this moment in time, I cannot cope with”.
“I think it’s still embarrassing. I think sometimes you try and you kind of try and put it to the back of your head and I think then if someone specifically asks you, you kind of go ‘Oh well, yeah, I suppose so’”.
“It would have become one of my top 10 but it is the fact that although it’s very important it’s top-trumped by other physical issues”.
- Comfort with UI Status Enquiry
“The fact that they were asking a question about it, presumably so that they could tailor their class to suit me, would be a good thing but I have to say, I would be slightly less comfortable if it was a man”.
“If it was somebody I didn’t know, and particularly somebody younger, and particularly somebody male would I? Well, I’m not sure what I would actually. I think I’d probably lose my nerve and lie”.
“I’d be less likely to go to a man. I don’t know. I just feel like they don’t understand it. And maybe this is where I see it as a female problem. Maybe it’s not just a female problem but I think because of that, it’s in my head, they really don’t get that you’ve no control over this. So yeah, no, I would much rather a woman asked”.
“If she [the instructor] seemed quite knowledgeable about it and framed it in such a way that we understand that some people can have problems with this and we can adapt our exercises to suit that. Or to even maybe target the muscles that you need, that would probably make me more comfortable that it’s not just a sort of tick-box, and they’re actually going to be able to help me”.
“I think it would be important for it to be on the questionnaire. So that then there could be a verbal conversation with the PT based on your answer”.
“If there was multiple choice components, like, if you have, have you ever experienced the following? And it’s there, then people are more likely to check that answer. Especially if there’s multiples because then they feel like, ‘Oh, I’ve said it, but it’s not blaringly flashing’, that that’s the thing”.
3.2.3. Encouraging Continued Participation
- Updating Exercise Delivery to Meet All Women’s Needs
“You’ve got to be able to adapt that lesson to lots of different people, and I just don’t think that there’s the understanding and the training in fitness to actually understand that at the moment. I just, I really don’t”.
“They’re not going to be judgmental if you’ve got to nip off for a wee. And they’ll work around that. They’ll probably not put as many star jumps in and not do things that are going to cause people to leak. They’re aware of what can make a lady wee herself, or whatever”.
“I want to do that, but I can’t and I’m not going to stand in the middle of an exercise class and tell you I can’t do a star jump because I’ll wee myself. Can you give me something that’s as energetic but takes into account the fact that I might not want to do that, not because it’s harder, I just don’t want to do a star jump”.
“If they’re just doing general PT so that there could be someone in there before me or after me, and if they see me, they just think, ‘Oh, she’s in there for PT’, and there’s no [risk] of ‘She’s in there for incontinence!’”.
“I think if there was a clear thing that said that leaking was taken into consideration, then I think I think I probably would feel more comfortable because I’d feel that the person who was taking the group actually had an understanding about it and would actually then probably discuss it with you”.
“I think it would make a massive difference because you go to classes, and I think you feel quite isolated because you look around and you think everyone else has got their shit together and I’m kind of standing there concerned about the fact I’m not doing half the exercises. I don’t feel that I can. It just makes you feel like not going back”.
“I think the thing is, without female comedians, you wouldn’t find any of this out. If you go to see some of the people that, I don’t know if you’ve ever seen any female comedians do the menopause? But you walk out of there thinking ‘crikey! I didn’t know that!’. You’re in a roomful of hormonal women who’ve lost most of the hormones and they’re all sighing a sigh of relief”.
“She [the instructor] was on Woman’s Hour or something, and it was a proper lightbulb moment. She was funny, and suddenly, instead of being something shameful, it was funny, and that was so liberating”.
- Need for Improved PA Infrastructure
“A lot of things I love to do, like riding bikes and things like that, but I won’t even attempt to ride a bike at the minute”.
“You try to keep some sort of level of fitness. But what upsets me the most now is that I can’t even walk”.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PA | Physical Activity |
| UI | Urinary Incontinence |
| NCD | Non-communicable disease |
| WHO | World Health Organisation |
| PAH | Physical Activity and Health |
| NHS | National Health Service |
| QOL | Quality of Life |
References
- Lindsay, T.; Westgate, K.; Wijndaele, K.; Hollidge, S.; Kerrison, N.; Forouhi, N.; Griffin, S.; Wareham, N.; Brage, S. Descriptive epidemiology of physical activity energy expenditure in UK adults (The Fenland study). Int. J. Behav. Nutr. Phys. Act. 2019, 16, 126. [Google Scholar] [CrossRef]
- Strain, T.; Strain, T.; Flaxman, S.; Flaxman, S.; Guthold, R.; Guthold, R.; Semenova, E.; Semenova, E.; Cowan, M.; Cowan, M.; et al. National, regional, and global trends in insufficient physical activity among adults from 2000 to 2022: A pooled analysis of 507 population-based surveys with 5·7 million participants. Lancet Glob. Health 2024, 12, e1232–e1243. [Google Scholar] [CrossRef] [PubMed]
- Birtwistle, S.; Deakin, E.; Whitford, R.; Hinchliffe, S.; Daniels-Creasey, A.; Rule, S. The Scottish Health Survey; Scottish Government: Edinburgh, UK, 2021. Available online: https://www.gov.scot/binaries/content/documents/govscot/publications/statistics/2022/11/scottish-health-survey-2021-volume-1-main-report/documents/scottish-health-survey-2021-volume-1-main-report/scottish-health-survey-2021-volume-1-main-report/govscot%3Adocument/scottish-health-survey-2021-volume-1-main-report.pdf (accessed on 10 January 2023).
- Gordon, E.H.; Hubbard, R.E. Differences in frailty in older men and women. Med. J. Aust. 2020, 212, 183–188. [Google Scholar] [CrossRef]
- Huang, T.-Y.; Chou, M.-Y.; Liang, C.-K.; Lin, Y.-T.; Chen, R.-Y.; Wu, P.-F. Physical activity plays a crucial role in multidomain intervention for frailty prevention. Aging Clin. Exp. Res. 2023, 35, 1283–1292. [Google Scholar] [CrossRef]
- Dent, E.; Via, J.D.; Bozanich, T.; Hoogendijk, E.O.; Gebre, A.K.; Smith, C.; Zhu, K.; Prince, R.L.; Lewis, J.R.; Sim, M. Frailty increases the long-term risk for fall and fracture-related hospitalizations and all-cause mortality in community-dwelling older women. J. Bone Miner. Res. 2024, 39, 222–230. [Google Scholar] [CrossRef]
- Carcel, C.; Carcel, C.; Haupt, S.; Haupt, S.; Arnott, C.; Arnott, C.; Yap, M.L.; Yap, M.L.; Henry, A.; Henry, A.; et al. A life-course approach to tackling noncommunicable diseases in women. Nat. Med. 2024, 30, 51–60. [Google Scholar] [CrossRef] [PubMed]
- WHO. Non-Communicable Diseases (NCDs). 2020. Available online: https://www.who.int/gho/ncd/en/ (accessed on 17 April 2024).
- Schuch, F.B.; Stubbs, B. The Role of Exercise in Preventing and Treating Depression. Optom. Vis. Sci. 2019, 18, 299–304. [Google Scholar] [CrossRef]
- López-Ortiz, S.; Lista, S.; Valenzuela, P.L.; Pinto-Fraga, J.; Carmona, R.; Caraci, F.; Caruso, G.; Toschi, N.; Emanuele, E.; Gabelle, A.; et al. Effects of physical activity and exercise interventions on Alzheimer’s disease: An umbrella review of existing meta-analyses. J. Neurol. 2022, 270, 711–725. [Google Scholar] [CrossRef]
- James, S.-N.; Chiou, Y.-J.; Fatih, N.; Needham, L.P.; Schott, J.M.; Richards, M. Timing of physical activity across adulthood on later-life cognition: 30 years follow-up in the 1946 British birth cohort. J. Neurol. Neurosurg. Psychiatry 2023, 94, 349–356. [Google Scholar] [CrossRef]
- Owen-Williams, R. Leading Causes of Death, UK: 2001 to 2018. Office of National Statistics. 2020. Available online: https://backup.ons.gov.uk/wp-content/uploads/sites/3/2020/03/Leading-causes-of-death-UK-2001-to-2018.pdf (accessed on 17 April 2024).
- Pedersen, M.R.L.; Hansen, A.F.; Elmose-Østerlund, K. Motives and Barriers Related to Physical Activity and Sport across Social Backgrounds: Implications for Health Promotion. Int. J. Environ. Res. Public Health 2021, 18, 5810. [Google Scholar] [CrossRef]
- Laakkonen, E.K.; Kulmala, J.; Aukee, P.; Hakonen, H.; Kujala, U.M.; Lowe, D.A.; Kovanen, V.; Tammelin, T.; Sipilä, S. Female reproductive factors are associated with objectively measured physical activity in middle-aged women. PLoS ONE 2017, 12, e0172054. [Google Scholar] [CrossRef]
- Garner, G.; Price, W.F. Physical Activity for Women; Tollefson, M., Eriksen, N., Pathak, N., Eds.; CRS Press: Oxon, UK, 2022; pp. 41–62. [Google Scholar]
- D’Ancona, C.; Haylen, B.; Oelke, M.; Abranches-Monteiro, L.; Arnold, E.; Goldman, H.; Hamid, R.; Homma, Y.; Marcelissen, T.; Rademakers, K.; et al. The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol. Urodyn. 2019, 38, 433–477. [Google Scholar] [CrossRef] [PubMed]
- Helfand, B.T.; Smith, A.R.; Lai, H.H.; Yang, C.C.; Gore, J.L.; Erickson, B.A.; Kreder, K.J.; Cameron, A.P.; Weinfurt, K.P.; Griffith, J.W.; et al. Prevalence and Characteristics of Urinary Incontinence in a Treatment Seeking Male Prospective Cohort: Results from the LURN Study. J. Urol. 2018, 200, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Milsom, I.; Gyhagen, M. The prevalence of urinary incontinence. Climacteric 2018, 22, 217–222. [Google Scholar] [CrossRef]
- Calgary Women’s Pelvic Health Research Group; Brennand, E.; Ruiz-Mirazo, E.; Tang, S.; Kim-Fine, S. Urinary leakage during exercise: Problematic activities, adaptive behaviors, and interest in treatment for physically active Canadian women. Int. Urogynecology J. 2018, 29, 497–503. [Google Scholar] [CrossRef]
- Culleton-Quinn, E.; Bø, K.; Fleming, N.; Mockler, D.; Cusack, C.; Daly, D. Elite female athletes’ experiences of symptoms of pelvic floor dysfunction: A systematic review. Int. Urogynecology J. 2022, 33, 2681–2711. [Google Scholar] [CrossRef]
- Dakic, J.G.; Hay-Smith, J.; Lin, K.-Y.; Cook, J.; Frawley, H.C. Experience of Playing Sport or Exercising for Women with Pelvic Floor Symptoms: A Qualitative Study. Sports Med. Open 2023, 9, 25. [Google Scholar] [CrossRef]
- Kenne, K.; Bradley, C.S. Female Urinary Incontinence; Springer: Cham, Switzerland, 2022; pp. 107–125. [Google Scholar] [CrossRef]
- Fakari, F.R.; Hajian, S.; Darvish, S.; Majd, H.A. Explaining factors affecting help-seeking behaviors in women with urinary incontinence: A qualitative study. BMC Health Serv. Res. 2021, 21, 60. [Google Scholar] [CrossRef]
- Southall, K.; Tuazon, J.R.; Djokhdem, A.H.; Heuvel, E.A.v.D.; Wittich, W.; Jutai, J.W. Assessing the stigma content of urinary incontinence intervention outcome measures. J. Rehabil. Assist. Technol. Eng. 2017, 4, 2055668317738943. [Google Scholar] [CrossRef] [PubMed]
- Fante, J.F.; Silva, T.D.; Mateus-Vasconcelos, E.C.L.; Ferreira, C.H.J.; Brito, L.G.O. Do Women have Adequate Knowledge about Pelvic Floor Dysfunctions? A Systematic Review. Rev. Bras. Hematol. Hemoter. 2019, 41, 508–519. [Google Scholar] [CrossRef]
- Cardoso, A.M.B.; Lima, C.R.O.d.P.; Ferreira, C.W.S. Prevalence of urinary incontinence in high-impact sports athletes and their association with knowledge, attitude and practice about this dysfunction. Eur. J. Sport Sci. 2018, 18, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; SAGE Publications Ltd.: London, UK, 2017. [Google Scholar]
- MacLennan, A.H.; Taylor, A.W.; Wilson, D.H.; Wilson, D. The prevalence of pelvic floor disorders and their relationship to gender, age, parity and mode of delivery. Br. J. Obstet. Gynaecol. 2000, 107, 1460–1470. [Google Scholar]
- Haakstad, L.A.H.; Gjestvang, C.; Lamerton, T.; Bø, K. Urinary incontinence in a fitness club setting—Is it a workout problem? Int. Urogynecology J. 2020, 31, 1795–1802. [Google Scholar] [CrossRef]
- Andrade, C. The Limitations of Online Surveys. Indian J. Psychol. Med. 2020, 42, 575–576. [Google Scholar] [CrossRef] [PubMed]
- Storey, D.; Tait, A. Survey Research. Anesthesiology 2019, 130, 192–202. [Google Scholar]
- Sparkes, A.C.; Smith, B. Qualitative Research Methods in Sport, Exercise and Health; Routledge: Oxon, UK, 2014. [Google Scholar]
- McGrath, C.; Palmgren, P.J.; Liljedahl, M. Twelve tips for conducting qualitative research interviews. Med. Teach. 2019, 41, 1002–1006. [Google Scholar] [CrossRef]
- Pinto, A.; Rodriguez, A.; Smith, J. Researching sensitive topics in healthcare. Évid. Based Nurs. 2022, 25, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Gill, P.; Stewart, K.; Treasure, E.; Chadwick, B. Methods of data collection in qualitative research: Interviews and focus groups. Br. Dent. J. 2008, 204, 291–295. [Google Scholar] [CrossRef]
- Jenner, B.M.; Myers, K.C. Intimacy, rapport, and exceptional disclosure: A comparison of in-person and mediated interview contexts. Int. J. Soc. Res. Methodol. 2019, 22, 165–177. [Google Scholar] [CrossRef]
- Larivière, C.D.; Crough, Q.; Eastwood, J. The Effects of Rapport Building on Information Disclosure in Virtual Interviews. J. Police Crim. Psychol. 2023, 38, 452–460. [Google Scholar] [CrossRef]
- Elmir, R.; Schmied, V.; Jackson, D.; Wilkes, L. Interviewing people about potentially sensitive topics. Nurse Res. 2011, 19, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Dickson-Swift, V.; James, E.L.; Kippen, S.; Liamputtong, P. Doing sensitive research: What challenges do qualitative researchers face? Qual. Res. 2007, 7, 327–353. [Google Scholar] [CrossRef]
- Brinkmann, S. Qualitative Interviewing: Conversational Knowledge Through Research Interviews, 2nd ed.; Oxford University Press: New York, NY, USA, 2022. [Google Scholar]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide, 1st ed.; SAGE Publications Ltd.: London, UK, 2022. [Google Scholar]
- Maguire, M.; Delahunt, B. Doing a Thematic Analysis: A Practical, Step-by-Step Guide for Learning and Teaching Scholars. All Irel. J. Teach. Learn. High. Educ. 2017, 9, 3. [Google Scholar]
- Nygaard, I.E.; Shaw, J.M. Physical activity and the pelvic floor. Am. J. Obstet. Gynecol. 2016, 214, 164–171. [Google Scholar] [CrossRef]
- Teixeira, R.V.; Colla, C.; Sbruzzi, G.; Mallmann, A.; Paiva, L.L. Prevalence of urinary incontinence in female athletes: A systematic review with meta-analysis. Int. Urogynecology J. 2018, 29, 1717–1725. [Google Scholar] [CrossRef]
- Dakic, J.G.; Cook, J.; Hay-Smith, J.; Lin, K.-Y.; Ekegren, C.; Frawley, H.C. Pelvic Floor Symptoms Are an Overlooked Barrier to Exercise Participation: A Cross-Sectional Online Survey of 4556 Women Who Are Symptomatic. Phys. Ther. 2021, 102, pzab284. [Google Scholar] [CrossRef] [PubMed]
- Lane, G.I.; Hagan, K.; Erekson, E.; Minassian, V.A.; Grodstein, F.; Bynum, J. Patient–Provider Discussions About Urinary Incontinence Among Older Women. J. Gerontol. Ser. A 2021, 76, 463–469. [Google Scholar] [CrossRef]
- Sheehan, L.; Albaugh, J.; Gartley, C.B.; Park, J.; George, N.; Hayward, S.; LaPorte, P.; Yednock, T.L.; Adil, A.; Haneef, A. Understanding the Benefits and Risks of Disclosing Urinary Incontinence: A Qualitative Study. Urol. Nurs. 2022, 42, 121. [Google Scholar] [CrossRef]
- Sullivan, R.; McNicholas, T.; Claffey, P.; Kenny, R.A.; Briggs, R. Unreported urinary incontinence: Population-based prevalence and factors associated with non-reporting of symptoms in community-dwelling people ≥ 50 years. Eur. Geriatr. Med. 2021, 12, 405–412. [Google Scholar] [CrossRef]
- Brown, N.; Bowmer, Y. A Comparison of Perceived Barriers and Motivators to Physical Activity in Young and Middle-Aged Women. Women Sport Phys. Act. J. 2019, 27, 52–59. [Google Scholar] [CrossRef]
- Richards, E.A.; Woodcox, S. Barriers and Motivators to Physical Activity Prior to Starting a Community-Based Walking Program. Int. J. Environ. Res. Public Health 2021, 18, 10659. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, Y.; Brown, W.J.; Mielke, G.I. Trajectories of physical activity from mid to older age in women: 21 years of data from the Australian Longitudinal Study on Women’s Health. Int. J. Behav. Nutr. Phys. Act. 2024, 21, 4. [Google Scholar] [CrossRef]
- Kim, M.M.; Ladi-Seyedian, S.-S.; Ginsberg, D.A.; Kreydin, E.I. The Association of Physical Activity and Urinary Incontinence in US Women: Results from a Multi-Year National Survey. Urology 2022, 159, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Elbandrawy, A.M.; Mahmoud, S.G.; AboElinin, M.F.; Yousef, A.M. Effect of Aerobic Walking Exercise on Stress Urinary Incontinence in Postmenopausal Women. Women Sport Phys. Act. J. 2022, 30, 11–17. [Google Scholar] [CrossRef]
- Tang, Y.; Guo, X.; Wang, Y.; Liu, Z.; Cao, G.; Zhou, Y.; Chen, M.; Liu, J.; Mu, J.; Yuan, M. Rumba Dance Combined with Breathing Training as an Exercise Intervention in the Management of Stress Urinary Incontinence in Postmenopausal Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 20, 522. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, L.; Delpe, S.; Priest, T.; Reynolds, W.S. Physical Activity and Stress Incontinence in Women. Curr. Bladder Dysfunct. Rep. 2019, 14, 174–179. [Google Scholar] [CrossRef]
- Tcymbal, A.; Demetriou, Y.; Kelso, A.; Wolbring, L.; Wunsch, K.; Wäsche, H.; Woll, A.; Reimers, A.K. Effects of the built environment on physical activity: A systematic review of longitudinal studies taking sex/gender into account. Environ. Health Prev. Med. 2020, 25, 75. [Google Scholar] [CrossRef]
- Campisi, T.; Georgiadis, G.; Basbas, S. Developing Cities for Citizens: Supporting Gender Equity for Successful and Sustainable Urban Mobility. In Computational Science and Its Applications—ICCSA 2022 Workshops; Gervasi, O., Murgante, B., Misra, S., Rocha, A.M.A.C., Garau, C., Eds.; ICCSA 2022. Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2022; pp. 410–422. [Google Scholar] [CrossRef]
- Stephen, K.; van Woerden, H.; MacRury, S. Assessing prevalence of urinary incontinence in Scottish fitness instructors and experience of teaching pelvic floor muscle exercises: An online survey. J. Public Health 2018, 41, e44–e50. [Google Scholar] [CrossRef]
- Dakic, J.G.; Hay-Smith, J.; Cook, J.; Lin, K.-Y.; Calo, M.; Frawley, H. Effect of Pelvic Floor Symptoms on Women’s Participation in Exercise: A Mixed-Methods Systematic Review With Meta-analysis. J. Orthop. Sports Phys. Ther. 2021, 51, 345–361. [Google Scholar] [CrossRef]
- Mendes, A.; Hoga, L.; Gonçalves, B.; Silva, P.; Pereira, P. Adult women’s experiences of urinary incontinence: A systematic review of qualitative evidence. JBI Évid. Synth. 2017, 15, 1350–1408. [Google Scholar] [CrossRef]
- Ficko, Z.; Li, Z.; Hyams, E.S. Urology is a Sensitive Area: Assessing Patient Preferences for Male or Female Urologists. Urol. Pract. 2018, 5, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Foster, P.; Luebke, M.; Razzak, A.N.; Anderson, D.J.; Hasoon, J.; Viswanath, O.; Kaye, A.D.; Urits, I. Stigmatization as a Barrier to Urologic Care: A Review. Health Psychol. Res. 2023, 11, 84273. [Google Scholar] [CrossRef]
- Groutz, A.; Gordon, D.; Shimonov, M.; Amir, H. Do women with pelvic floor disorders prefer to be treated by female urogynecologists? Health Care Women Int. 2020, 41, 543–552. [Google Scholar] [CrossRef]
- Howlett, N.; Trivedi, D.; A Troop, N.; Chater, A.M. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl. Behav. Med. 2018, 9, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Hallgren, M.; Nguyen, T.-T.; Owen, N.; Vancampfort, D.; Dunstan, D.W.; Wallin, P.; Andersson, G.; Ekblom-Bak, E. Associations of sedentary behavior in leisure and occupational contexts with symptoms of depression and anxiety. Prev. Med. 2020, 133, 106021. [Google Scholar] [CrossRef] [PubMed]
- Fadlilah, M.; Akriana, F.; Tan, C.H.; Rashid, N.A. Literature Review of Physical Exercise, Anxiety In Menopause Women. J. Inspirasi Kesehat. 2023, 1, 65–70. [Google Scholar] [CrossRef]
- Sarkar, D.; Tandon, M.; Pal, D.K. Comprehensive study of anxiety and depression in females with urinary incontinence. Urol. J. 2023, 90, 757–762. [Google Scholar] [CrossRef]
- Lakicevic, N.; Gentile, A.; Mehrabi, S.; Cassar, S.; Parker, K.; Roklicer, R.; Bianco, A.; Drid, P. Make Fitness Fun: Could Novelty Be the Key Determinant for Physical Activity Adherence? Front. Psychol. 2020, 11, 577522. [Google Scholar] [CrossRef]
- Steltenpohl, C.N.; Shuster, M.; Peist, E.; Pham, A.; Mikels, J.A. Me Time, or We Time? Age Differences in Motivation for Exercise. Gerontologist 2018, 59, 709–717. [Google Scholar] [CrossRef]
- Royse, L.A.; Baker, B.S.; Warne-Griggs, M.D.; Miller, K.; Weitzel, K.J.; Ball, S.D.; Duren, D.L. “It’s not time for us to sit down yet”: How group exercise programs can motivate physical activity and overcome barriers in inactive older adults. Int. J. Qual. Stud. Health Well-Being 2023, 18, 2216034. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.; Alexander, A.C. A Qualitative Exploration of Womens’ Experiences Who Belong to a “Fitness Community”. Am. J. Health Educ. 2020, 51, 22–30. [Google Scholar] [CrossRef]
- Peinado-Molina, R.A.; Martínez-Vázquez, S.; Hernández-Martínez, A.; Martínez-Galiano, J.M. Impact and Influence of Urinary Incontinence on Physical Activity Levels. Eur. Urol. Open Sci. 2023, 55, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Toye, F.; Barker, K.L. A meta-ethnography to understand the experience of living with urinary incontinence: ‘Is it just part and parcel of life? BMC Urol. 2020, 20, 1. [Google Scholar] [CrossRef]
- Jensen, L.C.G.; Axelsen, S. Urinary incontinence and work capacity. Dan. Med. J. 2023, 70, A04230271. [Google Scholar]
- McArthur, D.; Dumas, A.; Woodend, K.; Beach, S.; Stacey, D. Factors influencing adherence to regular exercise in middle-aged women: A qualitative study to inform clinical practice. BMC Women’s Health 2014, 14, 49. [Google Scholar] [CrossRef]
- Walsh, A.; Simpson, E.E.A. Health cognitions mediate physical (in)activity and walking in midlife women. Maturitas 2020, 131, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Bauer, S.R.; Kenfield, S.A.; Sorensen, M.; Subak, L.L.; Phelan, S.; Gupta, L.R.; Chen, B.; Suskind, A.M.; Park, A.J.; Iglesia, C.; et al. Physical Activity, Diet, and Incident Urinary Incontinence in Postmenopausal Women: Women’s Health Initiative Observational Study. J. Gerontol. Ser. A 2021, 76, 1600–1607. [Google Scholar] [CrossRef]
- Greed, C. Join the queue: Including women’s toilet needs in public space. Sociol. Rev. 2019, 67, 908–926. [Google Scholar] [CrossRef]
- Gümüşsoy, S.; Kavlak, O.; Dönmez, S. Investigation of body image, self-esteem, and quality of life in women with urinary incontinence. Int. J. Nurs. Pract. 2019, 25, e12762. [Google Scholar] [CrossRef]
- Dąbrowska-Galas, M.; Dąbrowska, J. Physical Activity Level and Self-Esteem in Middle-Aged Women. Int. J. Environ. Res. Public Health 2021, 18, 7293. [Google Scholar] [CrossRef]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Penguin: London, UK, 1990. [Google Scholar]
- Zhang, D.; Sun, X.; Zhu, H.; Wang, H.; Sun, X.; Wang, J. Help-seeking behavior for nonsevere stress urinary incontinence among elderly women in communities, Beijing, China. Int. Urogynecology J. 2023, 34, 2565–2572. [Google Scholar] [CrossRef] [PubMed]
- Dakic, J.G.; Cook, J.; Hay-Smith, J.; Lin, K.-Y.; Frawley, H. Pelvic floor disorders stop women exercising: A survey of 4556 symptomatic women. J. Sci. Med. Sport 2021, 24, 1211–1217. [Google Scholar] [CrossRef]
- Jouanny, C.; Abhyankar, P.; Maxwell, M. A mixed methods systematic literature review of barriers and facilitators to help-seeking among women with stigmatised pelvic health symptoms. BMC Women’s Health 2024, 24, 217. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M. The Oxford Handbook of Self-Determination Theory; Ryan, R.M., Ed.; Oxford University Press: New York, NY, USA, 2023. [Google Scholar] [CrossRef]
- Ryan, R.M.; Williams, G.C.; Patrick, H.; Deci, E.L. Self-Determination Theory and Physical Activity: The Dynamics of Motivation in Development and Wellness. Hell. J. Psychol. 2009, 6, 107–124. [Google Scholar]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef]
- Baum, F.; Musolino, C.; Gesesew, H.A.; Popay, J. New Perspective on Why Women Live Longer Than Men: An Exploration of Power, Gender, Social Determinants, and Capitals. Int. J. Environ. Res. Public Health 2021, 18, 661. [Google Scholar] [CrossRef] [PubMed]
- McKinney, J.L.; Clinton, S.C.; Keyser, L.E. Women’s Health Across the Lifespan: A Sex- and Gender-Focused Perspective. Phys. Ther. 2024, 104. [Google Scholar] [CrossRef] [PubMed]
- Scime, N.V.; Hetherington, E.; Metcalfe, A.; Chaput, K.H.; Dumanski, S.M.; Seow, C.H.; Brennand, E.A. Association between chronic conditions and urinary incontinence in females: A cross-sectional study using national survey data. CMAJ Open 2022, 10, E296–E303. [Google Scholar] [CrossRef]
- Hebert, E.P.; McGuin, J. Adult exercisers’ attitudes toward female and male personal fitness trainers: Influence of gender, age, and exercise experience. Sport J. 2024, 30, 120. [Google Scholar]
- Fisher, J.P.; Platts, C.; Stopforth, M. Attitudes Toward and Preferences for Male and Female Personal Trainers. Int. J. Exerc. Sci. 2013, 6, 256–268. [Google Scholar] [CrossRef]
- Bø, K.; Bratland-Sanda, S.; Sundgot-Borgen, J. Urinary incontinence among group fitness instructors including yoga and pilates teachers. Neurourol. Urodyn. 2011, 30, 370–373. [Google Scholar] [CrossRef]
- Bø, K. Urinary Incontinence, Pelvic Floor Dysfunction, Exercise and Sport. Sports Med. 2004, 34, 451–464. [Google Scholar] [CrossRef]
- Brubaker, L.; Shott, S.; Tomezsko, J.; Goldberg, R.P. Pelvic Floor Fitness Using Lay Instructors. Obstet. Gynecol. 2008, 111, 1298–1304. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V.; Boulton, E.; Davey, L.; McEvoy, C. The online survey as a qualitative research tool. Int. J. Soc. Res. Methodol. 2021, 24, 641–654. [Google Scholar] [CrossRef]
- Kays, K.; Gathercoal, K.; Buhrow, W. Does survey format influence self-disclosure on sensitive question items? Comput. Hum. Behav. 2012, 28, 251–256. [Google Scholar] [CrossRef]
- Suka, M.; Shimazaki, T. Effectiveness of using humor appeal in health promotion materials: Evidence from an experimental study in Japan. Arch. Public Health 2023, 81, 212. [Google Scholar] [CrossRef]
- Miller, E.; Bergmeier, H.J.; Blewitt, C.; O’Connor, A.; Skouteris, H. A systematic review of humour-based strategies for addressing public health priorities. Aust. N. Z. J. Public Health 2021, 45, 568–577. [Google Scholar] [CrossRef]
- Haynes, E.; Green, J.; Garside, R.; Kelly, M.P.; Guell, C. Gender and active travel: A qualitative data synthesis informed by machine learning. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 135. [Google Scholar] [CrossRef]
- Habermehl, V.; McFarlane, C. In Desperate Need: Public Sanitation in Contemporary London. Antipode 2024, 57, 193–214. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency | % of N | Mean | Min | Max | |
|---|---|---|---|---|---|
| Age (years old) (n = 345) | 47.7 | 18 | 79 | ||
| 18–35 | 21 | 6.1 | |||
| 36–55 | 272 | 78.8 | |||
| 56–65 | 32 | 9.3 | |||
| >65 | 20 | 5.8 | |||
| Education Level (n = 345) | |||||
| Secondary Education or less | 61 | 17.7 | |||
| Further Education | 17 | 4.9 | |||
| Undergraduate | 182 | 52.8 | |||
| Postgraduate | 85 | 24.6 | |||
| Self-Reported Physical Activity (minutes/week) (n = 189) * | 179.21 | 0 | 1440 | ||
| No Exercise | 23 | 12.2 | |||
| 1–149 | 87 | 46.0 | |||
| 150–300 | 48 | 25.4 | |||
| 301–600 | 26 | 13.8 | |||
| >600 | 5 | 2.7 |
| Frequency | % of N | Mean | Min | Max | |
|---|---|---|---|---|---|
| Age (years old) | 55.29 | 46 | 68 | ||
| 46–55 | 8 | 57.1 | |||
| 56–65 | 3 | 21.4 | |||
| >65 | 3 | 21.4 | |||
| Education Level | |||||
| Secondary Education or less | 2 | 14.3 | |||
| Further Education | 8 | 57.1 | |||
| Undergraduate | 2 | 14.3 | |||
| Postgraduate | 2 | 14.3 | |||
| Self-Reported Physical Activity (minutes/week) * | 176.43 | 0 | 420 | ||
| 0–59 | 2 | 14.3 | |||
| 60–149 | 5 | 35.7 | |||
| 150–300 | 4 | 28.6 | |||
| 301–600 | 3 | 21.4 | |||
| Leak Urine During Physical Activity | |||||
| Yes | 14 | 100 | |||
| No | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gard, A.J.M.; Lavallee, D. Examining the Relationship Between Urinary Incontinence and Women’s Physical Activity Engagement: Barriers and Disclosure Patterns. Healthcare 2025, 13, 856. https://doi.org/10.3390/healthcare13080856
Gard AJM, Lavallee D. Examining the Relationship Between Urinary Incontinence and Women’s Physical Activity Engagement: Barriers and Disclosure Patterns. Healthcare. 2025; 13(8):856. https://doi.org/10.3390/healthcare13080856
Chicago/Turabian StyleGard, Amanda J. M., and David Lavallee. 2025. "Examining the Relationship Between Urinary Incontinence and Women’s Physical Activity Engagement: Barriers and Disclosure Patterns" Healthcare 13, no. 8: 856. https://doi.org/10.3390/healthcare13080856
APA StyleGard, A. J. M., & Lavallee, D. (2025). Examining the Relationship Between Urinary Incontinence and Women’s Physical Activity Engagement: Barriers and Disclosure Patterns. Healthcare, 13(8), 856. https://doi.org/10.3390/healthcare13080856