
Health Inequity in the Distribution of Diseases Among Adults in the City of Pécs, Hungary, 2024



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants
2.4. Variables
Operational Definitions
2.5. Data Sources
2.6. Study Size
2.7. Statistical Methods
2.8. Ethical Considerations
3. Results
3.1. Socio-Demographic Variables
3.2. Descriptive Statistics
3.3. Inequity Analysis
3.3.1. Simple Measures of Inequity
3.3.2. Complex Measures of Inequity
Disease Proportion Based on Education
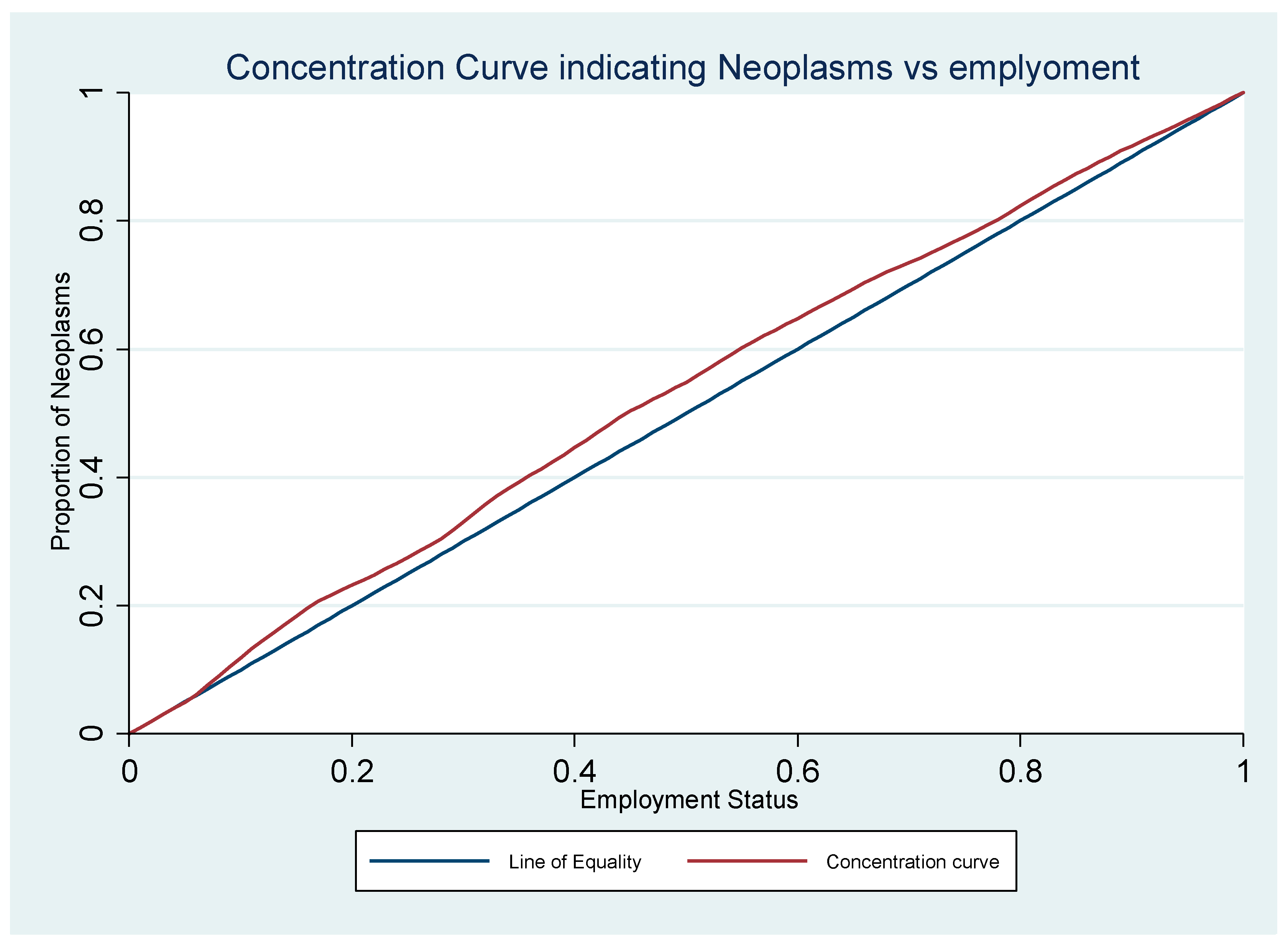
Disease Proportion Based on Employment
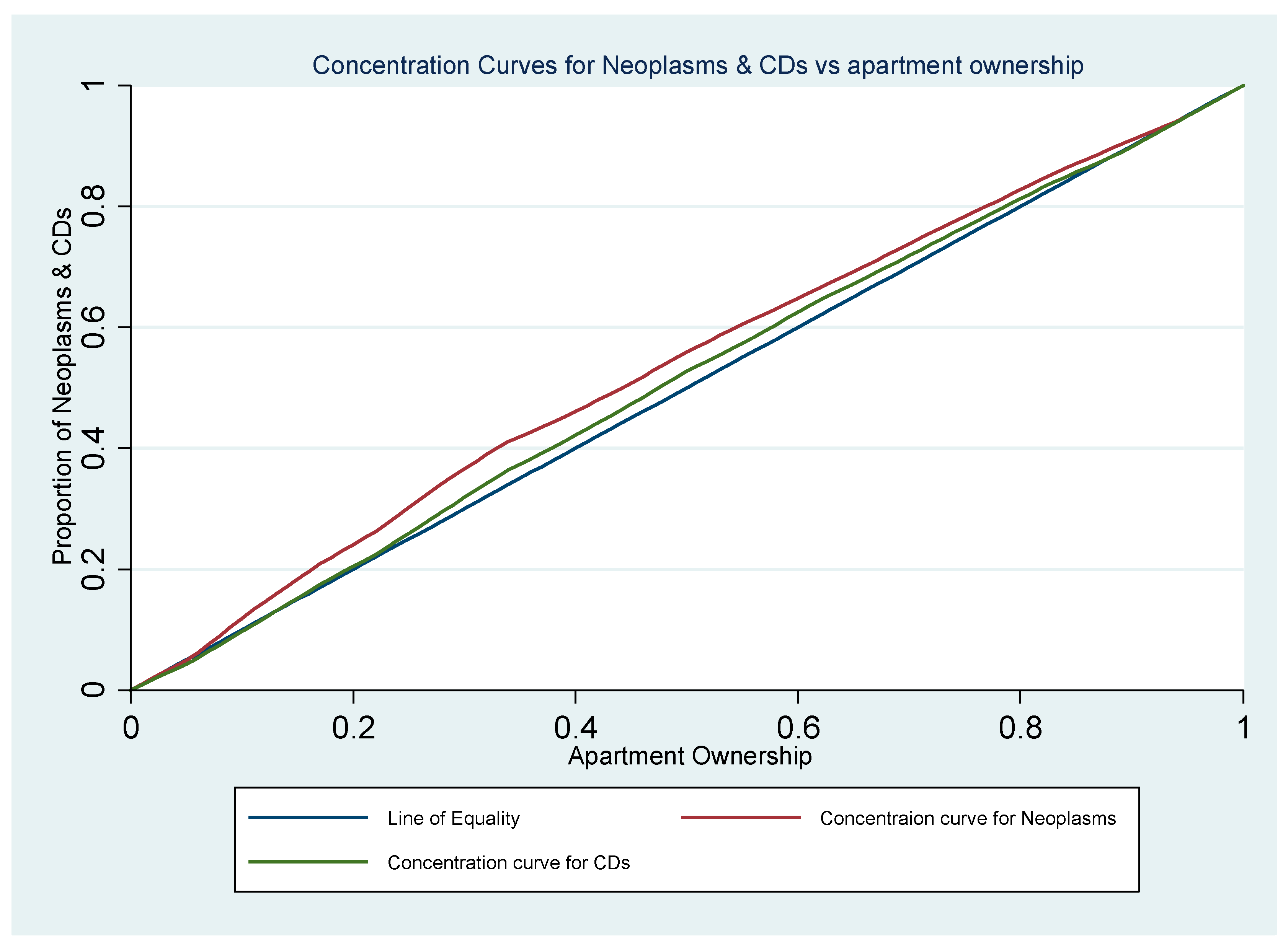
Disease Proportion Based on Apartment Ownership
4. Discussion
5. Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marmot, M.; Allen, J.; Bell, R.; Bloomer, E.; Goldblatt, P. WHO European review of social determinants of health and the health divide. Lancet 2012, 380, 1011–1029. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, M. The concepts and Principles of Equity and Health. Int. J. Health Serv. 1992, 22, 429–445. [Google Scholar] [CrossRef] [PubMed]
- Starfield, B. The hidden inequity in health care. Starfield Int. J. Equity Health 2011, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- UN. Academic Impact. In Sustainable Development Goals 2016; United Nations: New York, NY, USA, 2016. [Google Scholar]
- WHO. Hand Book on: Health Inequality Monitoring with a Special Focus on Low- and Middle-Income Countries; WHO: Luxembourg, 2013; p. 126. [Google Scholar]
- Schlotheuber, A.; Hosseinpoor, A.R. Summary Measures of Health Inequality: A Review of Existing Measures and Their Application. Int. J. Environ. Res. Public Health 2022, 19, 3697. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Meerding, W.J.; Kunst, A.E. Economic Costs of Health Inequalities in the European Union. J. Epidemiol. Community Health 2011, 65, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Xavier, A.; Price, C.; von Nordheim, F. Solidarity in Health: The European Commission Sets Out New Actions on Health Inequalities; Eurohealth: São Paulo, Brazil, 2009; Volume 15. [Google Scholar]
- EuroHealthNet. EuroHealthNet. EuroHealthNet Country Exchange Visit. In Health Equity and the Preventive Care Act in Germany 2017; Bundeszentrale für gesundheitliche Aufklärung (BZgA): Berlin, Germany, 2017. [Google Scholar]
- Phelan, J.C.; Link, B.G.; Tehranifar, P. Social Conditions as Fundamental Causes of Health Inequalities: Theory, Evidence, and Policy Implications. J. Health Soc. Behav. 2010, 51 (Suppl. S1), S28–S40. [Google Scholar] [CrossRef] [PubMed]
- WHO/Europe. Healthy, Prosperous Lives for All: The European Health Equity Status Report; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- EC. Knowledge for Policy: Social Gradient in Health Glossary Item 2020. Available online: https://knowledge4policy.ec.europa.eu/glossary-item/social-gradient-health_en (accessed on 27 May 2020).
- Sanson-Fisher, R.W.; Williams, N.; Outram, S. Health inequities: The need for action by schools of medicine. Med. Teach. 2008, 30, 389–394. [Google Scholar] [CrossRef] [PubMed]
- OECD; EU. Health at a Glance: Europe 2020: State of Health in the EU Cycle; OECD: Paris, France, 2020. [Google Scholar]
- OECD. Preventing Ageing Unequally; OECD: Paris, France, 2017. [Google Scholar]
- Pivarnyik, B. EU report gives Hungarian health-care a poor bill of health. The Budapest Beacon, 14 June 2017. [Google Scholar]
- Bíró, A.; Hajdu, T.; Kertesi, G.; Prinz, D. Life expectancy inequalities in Hungary over 25 years: The role of avoidable deaths. Popul. Stud. 2021, 75, 443–455. [Google Scholar] [CrossRef] [PubMed]
- Brinkhoff, T. Pécs in Pécs (Baranya). Available online: https://www.citypopulation.de/en/hungary/baranya/p%C3%A9cs/19415__p%C3%A9cs/ (accessed on 27 December 2024).
- WHO. ICD-10 Version: 2019. World Health Organization 2019. Available online: https://icd.who.int/browse10/2019/en#/E10-E14 (accessed on 15 February 2023).
- PHS. Measuring Health Inequalities. Improving Health 2021. 24 December 2021. Available online: https://www.healthscotland.scot/ (accessed on 12 March 2024).
- Salvatore Vaccarella, E.D.V.; Sierra, M.S.; Conway, D.I.; Mackenbach, J.P. Social inequalities in cancer within countries. In Reducing Social Inequalities in Cancer: Evidence and Priorities for Research; Salvatore Vaccarella, J.L.-T., Saracci, R., Conway, D.I., Straif, K., Wild, C.P., Eds.; International Agency for Research on Cancer: Lyon, France, 2019; Volume 168, pp. 63–78. [Google Scholar]
- McNamara, C.L.; Balaj, M.; Thomson, K.H.; Eikemo, T.A.; Solheim, E.F.; Bambra, C. The socioeconomic distribution of non-communicable diseases in Europe: Findings from the European Social Survey (2014) special module on the social determinants of health. Eur. J. Public Health 2017, 27, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Jemal, A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950–2014: Over Six Decades of Changing Patterns and Widening Inequalities. J. Environ. Public Health 2017, 2017, 2819372. [Google Scholar] [CrossRef] [PubMed]
- OECD. Beating Cancer Inequalities in the EU: Spotlight on Cancer Prevention and Early Detection; OECD Health Policy Studies; OECD Publishing: Paris, France, 2024. [Google Scholar] [CrossRef]
- Gronewold, J.; Kropp, R.; Lehmann, N.; Schmidt, B.; Weyers, S.; Siegrist, J.; Dragano, N.; Jöckel, K.H.; Erbel, R.; Hermann, D.M. Association of social relationships with incident cardiovascular events and all-cause mortality. Heart (Br. Card. Soc.) 2020, 106, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, H.T.; Bredahl Kristensen, F.P. Cardiovascular diseases and health inequalities in Europe—A pressing public health challenge. Lancet Reg. Health-Eur. 2023, 33, 100722. [Google Scholar] [CrossRef] [PubMed]
- Xia, M.; An, J.; Safford, M.M.; Colantonio, L.D.; Sims, M.; Reynolds, K.; Moran, A.E.; Zhang, Y. Cardiovascular Risk Associated With Social Determinants of Health at Individual and Area Levels. JAMA Netw. Open 2024, 7, e248584. [Google Scholar] [CrossRef] [PubMed]
- Højstrup, S.; Thomsen, J.H.; Prescott, E. Disparities in cardiovascular disease and treatment in the Nordic countries. Lancet Reg. Health-Eur. 2023, 33, 100699. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P. Health Inequalities: Persistence and Change in European Welfare States; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Bambra, C.; Eikemo, T.A. Welfare state regimes, unemployment and health: A comparative study of the relationship between unemployment and self-reported health in 23 European countries. J. Epidemiol. Community Health 2009, 63, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Hernández, D.; Swope, C.B. Housing as a Platform for Health and Equity: Evidence and Future Directions. Am. J. Public Health 2019, 109, 1363–1366. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.F.; Ma, G.X.; Miranda, J.; Eng, E.; Castille, D.; Brockie, T.; Jones, P.; Airhihenbuwa, C.O.; Farhat, T.; Zhu, L.; et al. Structural Interventions to Reduce and Eliminate Health Disparities. Am. J. Public Health 2019, 109 (Suppl. S1), S72–S78. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Disease | Zip Codes Grouped by Education | Difference (Cat 5 − Cat 1) | Ratio (Cat 5/Cat 1) | ||||
|---|---|---|---|---|---|---|---|
| Cat 1 | Cat 2 | Cat 3 | Cat 4 | Cat 5 | |||
| Respiratory disease | 0.2288 | 0.2622 | 0.2451 | 0.2515 | 0.2378 | 0.009 | 1.0393 |
| Circulatory disease | 0.3372 | 0.3551 | 0.3358 | 0.3581 | 0.2922 | −0.045 | 0.8665 |
| Neoplasms | 0.0202 | 0.0247 | 0.0263 | 0.0281 | 0.0204 | 0.0002 | 1.0099 |
| Zip codes grouped by Employment | |||||||
| Cat 1 | Cat 2 | Cat 3 | Cat 4 | Cat 5 | |||
| Respiratory disease | 0.2479 | 0.2568 | 0.2406 | 0.2500 | 0.2617 | 0.0138 | 1.0557 |
| Circulatory disease | 0.3426 | 0.3676 | 0.3375 | 0.3362 | 0.3165 | −0.0261 | 0.9239 |
| Neoplasms | 0.0275 | 0.0268 | 0.0234 | 0.0230 | 0.0202 | −0.0073 | 0.7352 |
| Zip codes grouped by apartment ownership | |||||||
| Cat 1 | Cat 2 | Cat 3 | Cat 4 | Cat 5 | |||
| Respiratory disease | 0.2549 | 0.2479 | 0.2481 | 0.2712 | 0.2406 | −0.0143 | 0.9440 |
| Circulatory disease | 0.3496 | 0.3732 | 0.3607 | 0.3360 | 0.3186 | −0.0310 | 0.9113 |
| Neoplasms | 0.0300 | 0.0295 | 0.0243 | 0.0215 | 0.0215 | −0.0085 | 0.7163 |
| Disease | Concentration Index | 95% Confidence Interval Lower Bound | 95% Confidence Interval Upper Bound | p-Value |
|---|---|---|---|---|
| Respiratory diseases | 0.0020 | −0.0199 | 0.0239 | 0.8610 |
| Neoplasms | 0.0254 | −0.0283 | 0.0791 | 0.3683 |
| Circulatory diseases | −0.0130 | −0.0421 | 0.0161 | 0.3955 |
| Disease | Concentration Index | 95% Confidence Interval Lower Bound | 95% Confidence Interval Upper Bound | p-Value |
|---|---|---|---|---|
| Respiratory diseases | 0.0029 | −0.0183 | 0.0242 | 0.7914 |
| Neoplasms | −0.0528 | −0.0975 | −0.0080 | 0.0345 * |
| Circulatory diseases | −0.0148 | −0.0418 | 0.0123 | 0.3001 |
| Disease | Concentration Index | 95% Confidence Interval Lower Bound | 95% Confidence Interval Upper Bound | p-Value |
|---|---|---|---|---|
| Respiratory diseases | −0.0098 | −0.0303 | 0.0108 | 0.3654 |
| Neoplasms | −0.0742 | −0.1102 | −0.0382 | 0.0010 * |
| Circulatory diseases | −0.0280 | −0.0520 | −0.00389 | 0.0369 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gube, A.A.; Lohner, S.; Vitrai, J. Health Inequity in the Distribution of Diseases Among Adults in the City of Pécs, Hungary, 2024. Healthcare 2025, 13, 681. https://doi.org/10.3390/healthcare13060681
Gube AA, Lohner S, Vitrai J. Health Inequity in the Distribution of Diseases Among Adults in the City of Pécs, Hungary, 2024. Healthcare. 2025; 13(6):681. https://doi.org/10.3390/healthcare13060681
Chicago/Turabian StyleGube, Addisu Alemayehu, Szimonetta Lohner, and Jozsef Vitrai. 2025. "Health Inequity in the Distribution of Diseases Among Adults in the City of Pécs, Hungary, 2024" Healthcare 13, no. 6: 681. https://doi.org/10.3390/healthcare13060681
APA StyleGube, A. A., Lohner, S., & Vitrai, J. (2025). Health Inequity in the Distribution of Diseases Among Adults in the City of Pécs, Hungary, 2024. Healthcare, 13(6), 681. https://doi.org/10.3390/healthcare13060681