
Evaluation of Health Promotion in International Schools Using the Schools for Health in Europe (SHE) Rapid Assessment Tool

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling
2.2. Data Collection
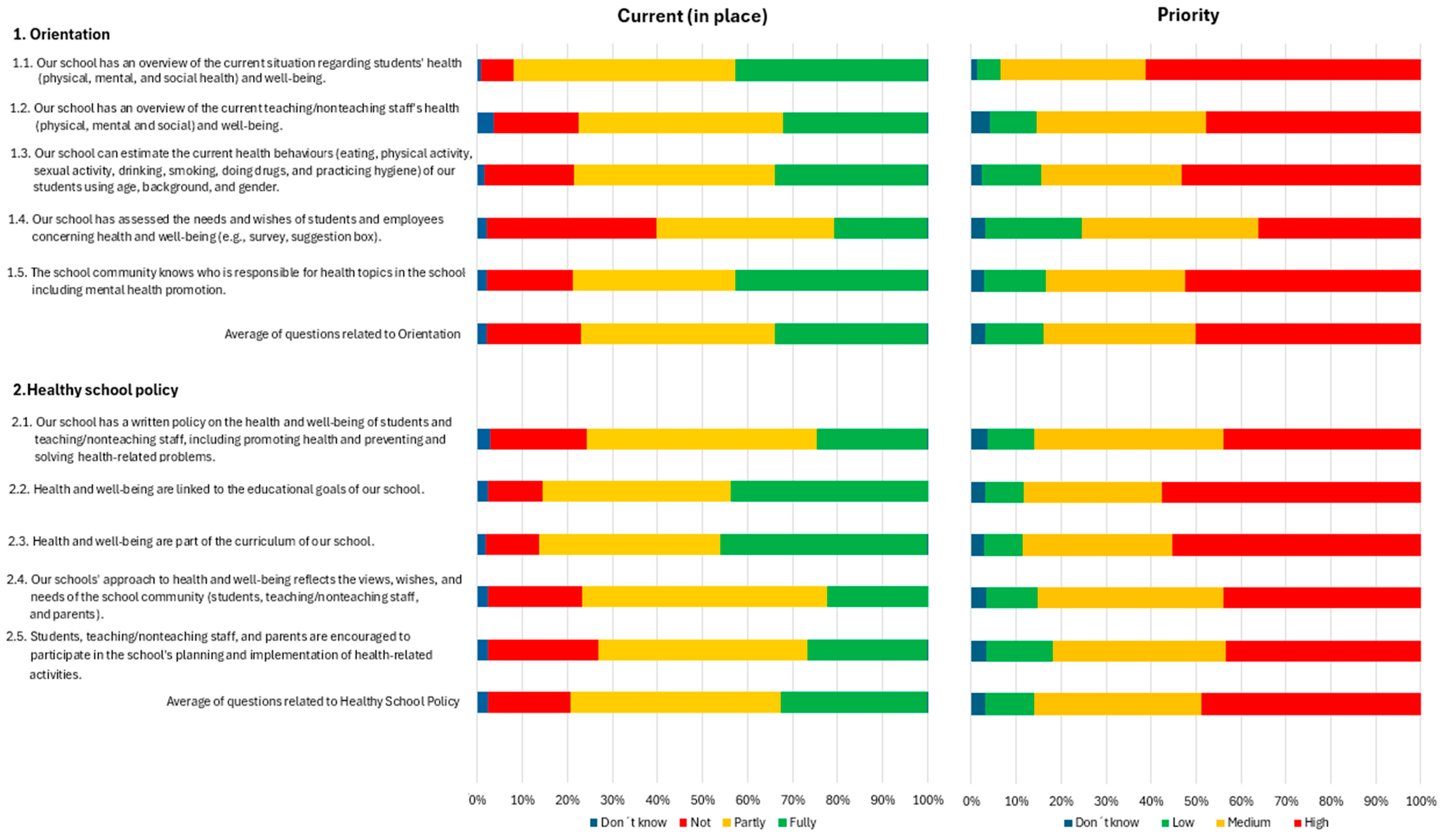
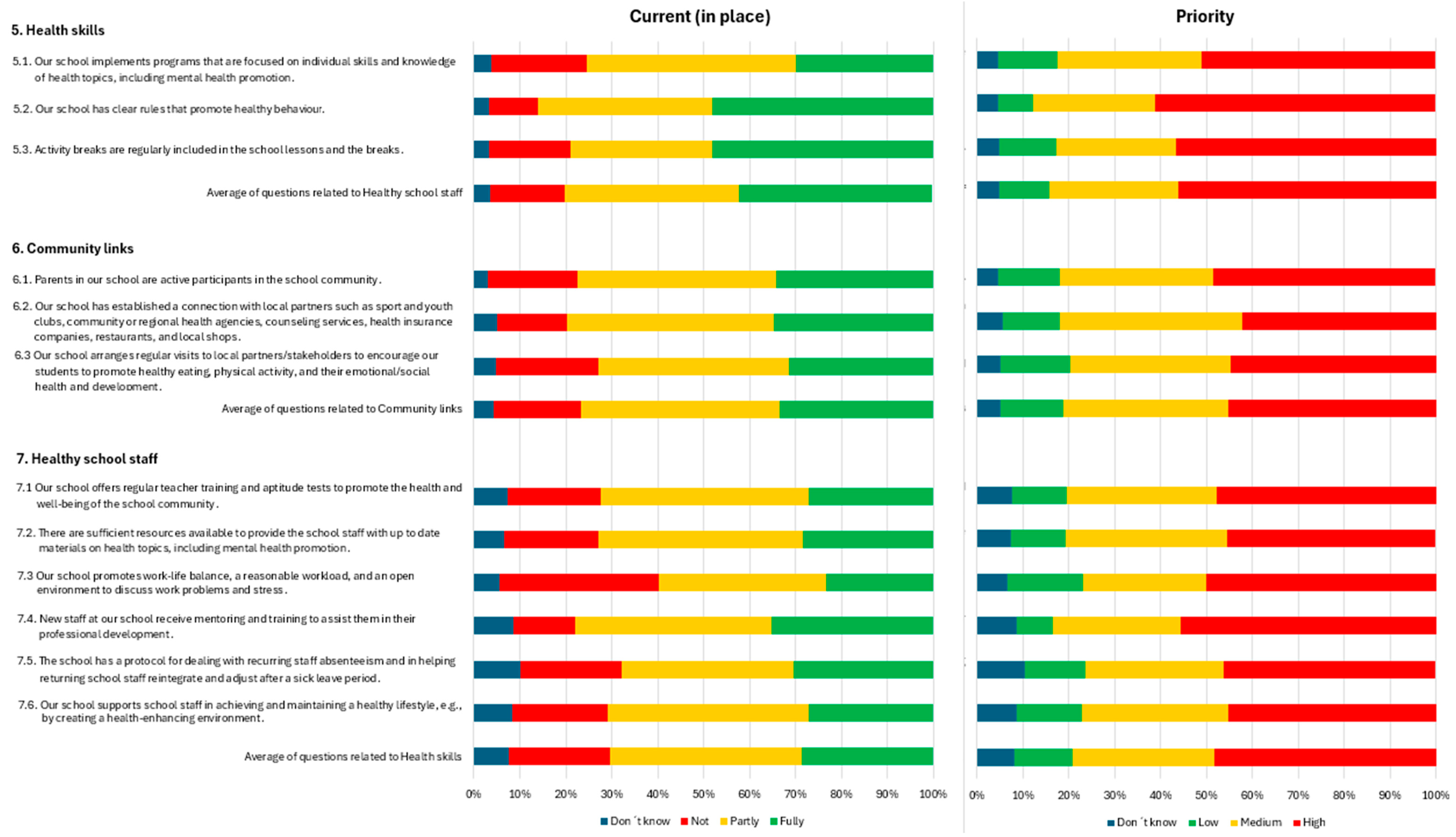
2.3. Variables
- Current—the school’s current situation on a three-point scale:
- 1 = not in place.
- 2 = partly in place.
- 3 = fully in place.
- 4 = don’t know.
- Priority—the priority that the school community gives to the question on a three-point scale:
- 1 = low/no priority.
- 2 = medium priority.
- 3 = high priority.
- 4 = don’t know.
2.4. Data Analysis
3. Results
4. Discussion
4.1. Main Findings
4.2. Characteristics of the Population
4.3. Health Promotion Assessment
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maziak, W.; Ward, K.D.; Stockton, M.B. Childhood Obesity: Are We Missing the Big Picture? Obes. Rev. 2008, 9, 35–42. [Google Scholar] [CrossRef]
- Viola, P.C.d.A.F.; Ribeiro, S.A.V.; Carvalho, R.R.S.d.; Andreoli, C.S.; Novaes, J.F.d.; Priore, S.E.; Carvalho, C.A.d.; Franceschini, S.d.C.C. Socioeconomic Status, Screen Time, and Time Spent at School, and Children’s Food Consumption. Cienc. Saude Coletiva 2023, 28, 257–267. [Google Scholar] [CrossRef]
- Bennett, A.E.; Cunningham, C.; Johnston Molloy, C. An Evaluation of Factors Which Can Affect the Implementation of a Health Promotion Programme under the Schools for Health in Europe Framework. Eval. Program Plan. 2016, 57, 50–54. [Google Scholar] [CrossRef]
- Llivina, T.S.; Creus, M.R.H.; Caballero, C.R. Informe: Diagnóstico de Situación Sobre Avances Conseguidos, Necesidades y Retos En Promoción y Educación Para La Salud En La Escuela En España; Ministerio de Educación, Política Social y Deporte y Ministerio de Sanidad y Consumo: Madrid, Spain, 2008; Available online: https://www.libreria.educacion.gob.es/libro/informe-diagnostico-de-situacion-sobre-avances-conseguidos-necesidades-y-retos-en-promocion-y-educacion-para-la-salud-en-la-escuela-en-espana_174293/ (accessed on 6 July 2024).
- Yonis, O.B.; Khader, Y.; Taha, H.; Al-Madhwahi, A.; Khudair, S.A.; Tanaka, E.; Al Nsour, M. Psychosocial and Emotional Well-Being of Syrian Refugee Children and Adolescents in Jordan: In-Camp versus out-of-Camp Comparative Analysis. Narra J. 2024, 4, e849. [Google Scholar] [CrossRef] [PubMed]
- Riquelme, M. Educación Para La Salud Escolar. In EEPap: Curso de Actualizacion de Pediatria; Exlibris Ediciones: Madrid, Spain, 2012; pp. 185–186. [Google Scholar]
- Leger, L.S.; Young, I.; Blanchard, C.; Perry, M. Promover La Salud En La Escuela: De La Evidencia a La Acción. 2010. Available online: http://www.iuhpe.org/images/PUBLICATIONS/THEMATIC/HPS/Evidence-Action_SP.pdf (accessed on 5 November 2019).
- Stewart-Brown, S. What Is the Evidence on School Health Promotion in Improving Health or Preventing Disease and, Specifically, What Is the Effectiveness of the Health Promoting Schools Approach? Available online: https://iris.who.int/bitstream/handle/10665/344683/9789289056830-eng.pdf?sequence=3&isAllowed=y (accessed on 6 July 2024).
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic Review of the Relationships between Objectively Measured Physical Activity and Health Indicators in School-Aged Children and Youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef]
- Saunders, T.J.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Olds, T.; Connor Gorber, S.; Kho, M.E.; Sampson, M.; et al. Combinations of Physical Activity, Sedentary Behaviour and Sleep: Relationships with Health Indicators in School-Aged Children and Youth. Appl. Physiol. Nutr. Metab. 2016, 41, S283–S293. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.M.; Cooke, S.M. Educating for a Healthy, Sustainable World: An Argument for Integrating Health Promoting Schools and Sustainable Schools. Health Promot. Int. 2007, 22, 346–353. [Google Scholar] [CrossRef]
- World Health Organization Making Every School a Health-Promoting School: Implementation Guidance. Available online: https://www.who.int/publications/i/item/9789240025073 (accessed on 5 June 2024).
- Barnekow, V.; Buijs, G.; Clift, S.; Jensen, B.B.; Paulus, P.; Rivett, D.; Young, I. Health-Promoting Schools: A Resource for Developing Indicators; WHO Regional Office for Europe: Copenhagen, Denmark, 2006. [Google Scholar]
- Bamekow Rasmussen, V. The European Network of Health Promoting Schools—From to Kyrgyzstan. Promot. Educ. 2005, 12, 169–172. [Google Scholar] [CrossRef]
- Turunen, H.; Sormunen, M.; Jourdan, D.; von Seelen, J.; Buijs, G. Health Promoting Schools—A Complex Approach and a Major Means to Health Improvement. Health Promot. Int. 2017, 32, 177–184. [Google Scholar] [CrossRef]
- Buijs, G.J. Better Schools through Health: Networking for Health Promoting Schools in Europe. Eur. J. Educ. 2009, 44, 507–520. [Google Scholar] [CrossRef]
- Bada, E.; Darlignton, E.; Masson, J.; Santos, R.M. European Standards and Indicators for Health Promoting Schools; Schools for Health in Europe Network Foundation: Haderslev, Denmark, 2019. [Google Scholar]
- OPS; OMS; UNESCO. Hacer Que Todas Las Escuelas Sean Promotoras de La Salud. Pautas e Indicadores Mundiales. 2022. Available online: https://iris.paho.org/bitstream/handle/10665.2/55711/9789275325124_spa.pdf?sequence=1&isAllowed=y (accessed on 14 June 2023).
- SHE Network Vilnius Resolution: Better Schools Through Health. Available online: https://www.schoolsforhealth.org/sites/default/files/editor/conference%20statements/Vilnius%20resolution/english-vilnius-resolution.pdf (accessed on 5 June 2024).
- Vilaça, T.; Emily, D.; Miranda-Velasco, M.J.; Martinis, O.; Masson, J. SHE School Manual 2.0; Schools for Health in Europe Network Foundation (SHE): Haderslev, Denmark, 2020. [Google Scholar]
- Weber, M.W.; Black, M.; Carai, S.; Jullien, S. WHO Strategies to Improve Child and Adolescents Health in Europe. Glob. Pediatr. 2024, 9, 100215. [Google Scholar] [CrossRef]
- Grupo de Trabajo de Escuelas Promotoras de Salud. Guia Escuelas Promotoras de Salud; Grupo de Trabajo de Escuelas Promotoras de Salud: Madrid, Spain, 2023. [Google Scholar]
- OPS; OMS; UNESCO. Hacer de Cada Escuela de La Región de Las Américas Una Escuela Promotora de Salud. Guía de Implementación Para Instituciones Educativas. 2023. Available online: https://iris.paho.org/bitstream/handle/10665.2/61898/9789275328132_spa.pdf?sequence=5&isAllowed=y (accessed on 22 March 2024).
- SEK Education Group SEK International Schools. Available online: https://www.sek.es/l/colegio-internacional/?gad_source=1&gclid=Cj0KCQjwn7mwBhCiARIsAGoxjaLkpSIHgESYm4SPhxgnZo3pcKv4FwbEO4XP8Y05eGRhtYwU8pNFWmIaAjlkEALw_wcB&gclsrc=aw.ds (accessed on 5 June 2024).
- García-Vázquez, J. Effects of the School for Health Network on Students’ Behaviour in Asturias (Spain). Health Promot. Int. 2017, 32, 271–279. [Google Scholar] [CrossRef]
- Konu, A.; Lintonen, T. Theory-Based Survey Analysis of Well-Being in Secondary Schools in Finland. Health Promot. Int. 2006, 21, 27–36. [Google Scholar] [CrossRef]
- Hildebrand, D.A.; Jacob, T.; Garrard-Foster, D. Food and Fun for Everyone: A Community Nutrition Education Program for Third- and Fourth-Grade Students Suitable for School Wellness Programs. J. Nutr. Educ. Behav. 2012, 44, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Hung, T.T.M.; Chiang, V.C.L.; Dawson, A.; Lee, R.L.T. Understanding of Factors That Enable Health Promoters in Implementing Health-Promoting Schools: A Systematic Review and Narrative Synthesis of Qualitative Evidence. PLoS ONE 2014, 9, e108284. [Google Scholar] [CrossRef]
- Lee, A.; Lo, A.S.C.; Keung, M.W.; Kwong, C.M.A.; Wong, K.K. Effective Health Promoting School for Better Health of Children and Adolescents: Indicators for Success. BMC Public Health 2019, 19, 1088. [Google Scholar] [CrossRef] [PubMed]
- Shackleton, N.; Jamal, F.; Viner, R.M.; Dickson, K.; Patton, G.; Bonell, C. School-Based Interventions Going Beyond Health Education to Promote Adolescent Health: Systematic Review of Reviews. J. Adolesc. Health 2016, 58, 382–396. [Google Scholar] [CrossRef]
- Owusu-Addo, E.; Edusah, S.E.; Sarfo-Mensah, P. The Utility of Stakeholder Involvement in the Evaluation of Community-Based Health Promotion Programmes. Int. J. Health Promot. Educ. 2015, 53, 291–302. [Google Scholar] [CrossRef]
- Maciver, D.; Hunter, C.; Johnston, L.; Forsyth, K. Using Stakeholder Involvement, Expert Knowledge and Naturalistic Implementation to Co-Design a Complex Intervention to Support Children’s Inclusion and Participation in Schools: The CIRCLE Framework. Children 2021, 8, 217. [Google Scholar] [CrossRef]
- Lloyd, J.; McHugh, C.; Minton, J.; Eke, H.; Wyatt, K. The Impact of Active Stakeholder Involvement on Recruitment, Retention and Engagement of Schools, Children and Their Families in the Cluster Randomised Controlled Trial of the Healthy Lifestyles Programme (HeLP): A School-Based Intervention to Prevent Obesity. Trials 2017, 18, 378. [Google Scholar] [CrossRef]
- Daly-Smith, A.; Quarmby, T.; Archbold, V.S.J.; Corrigan, N.; Wilson, D.; Resaland, G.K.; Bartholomew, J.B.; Singh, A.; Tjomsland, H.E.; Sherar, L.B.; et al. Using a Multi-Stakeholder Experience-Based Design Process to Co-Develop the Creating Active Schools Framework. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 13. [Google Scholar] [CrossRef] [PubMed]
- Sattar, T.; Ullah, M.I.; Ahmad, B. The Role of Stakeholders Participation, Goal Directness and Learning Context in Determining Student Academic Performance: Student Engagement as a Mediator. Front. Psychol. 2022, 13, 875174. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo-Sanjoaquín, J.; Murillo-Pardo, B.; Corral-Abós, A.; Lorente-Echeverría, S.; Zaragoza Casterad, J. Barriers to and Ways of Facilitating the Implementation of Aragon’s Health-Promoting School Network. Health Educ. J. 2023, 82, 251–262. [Google Scholar] [CrossRef]
- Avison, C. Engagement Des Intervenants à Améliorer Les Politiques Scolaires: Élaboration et Mise En Œuvre. Can. J. Public Health 2010, 101, S22–S25. [Google Scholar] [CrossRef]
- Lee, A.; Lo, A.; Li, Q.; Keung, V.; Kwong, A. Health Promoting Schools: An Update. Appl. Health Econ. Health Policy 2020, 18, 605–623. [Google Scholar] [CrossRef]
- Deschesnes, M.; Drouin, N.; Tessier, C.; Couturier, Y. Schools’ Capacity to Absorb a Healthy School Approach into Their Operations: Insights from a Realist Evaluation. Health Educ. 2014, 114, 208–224. [Google Scholar] [CrossRef]
- Simovska, V.; Dadaczynski, K.; Viig, N.G.; Bowker, S.; Woynarowska, B.; de Ruiter, S.; Buijs, G. HEPS Tool for Schools: A Guide for School Policy Development on Healthy Eating and Physical Activity; NIGZ: Woerden, The Netherlands, 2010; ISBN -978-9-0692-8261-9. [Google Scholar]
- Lane, H.G.; Deitch, R.; Wang, Y.; Black, M.M.; Dunton, G.F.; Aldoory, L.; Turner, L.; Parker, E.A.; Henley, S.C.; Saksvig, B.; et al. “Wellness Champions for Change”, a Multi-Level Intervention to Improve School-Level Implementation of Local Wellness Policies: Study Protocol for a Cluster Randomized Trial. Contemp. Clin. Trials 2018, 75, 29–39. [Google Scholar] [CrossRef]
- Hoelscher, D.M.; Moag-Stahlberg, A.; Ellis, K.; Vandewater, E.A.; Malkani, R. Evaluation of a Student Participatory, Low-Intensity Program to Improve School Wellness Environment and Students’ Eating and Activity Behaviors. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 59. [Google Scholar] [CrossRef]
- Eriksson, U.; Hochwälder, J.; Carlsund, Å.; Sellström, E. Health Outcomes among Swedish Children: The Role of Social Capital in the Family, School and Neighbourhood. Acta Paediatr. 2012, 101, 513–517. [Google Scholar] [CrossRef]
- Amirah, S.; Abdurrahman, M.F.; Akbar, R.F.A.; Mulya, I.C. Music Therapy Improves Social Interaction and Verbal Communication Skill among Children with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Narra X 2023, 1, 1–10. [Google Scholar] [CrossRef]
- Hawkins, G.T.; Chung, C.S.; Hertz, M.F.; Antolin, N. The School Environment and Physical and Social-Emotional Well-Being: Implications for Students and School Employees. J. Sch. Health 2023, 93, 799–812. [Google Scholar] [CrossRef] [PubMed]
- Bonell, C.; Jamal, F.; Harden, A.; Wells, H.; Parry, W.; Fletcher, A.; Petticrew, M.; Thomas, J.; Whitehead, M.; Campbell, R.; et al. Systematic Review of the Effects of Schools and School Environment Interventions on Health: Evidence Mapping and Synthesis. Public Health Res. 2013, 1, 1–320. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Hernando, B.; Gasch-Gallén, Á.; Antón-Solanas, I.; Gea-Caballero, V.; Juárez-Vela, R.; Gállego-Diéguez, J.; Carboneres-Tafaner, M.I.; Echániz-Serrano, E.; Lasso-Olayo, L.; Santolalla-Arnedo, I. A Comparative Study of Life Skills, Lifestyle Habits and Academic Performance in Health Promoting and Non-Health Promoting Schools in the Autonomous Community of Aragon, Spain. PeerJ 2022, 10, e13041. [Google Scholar] [CrossRef] [PubMed]
- Bejster, M.; Cygan, H.; Stock, J.; Ashworth, J. Engaging the School Community in a Nutrition and Physical Activity Program: The Role of the 21st-Century School Nurse. NASN Sch. Nurse 2020, 35, 260–265. [Google Scholar] [CrossRef]
- Pitt Barnes, S.; Lang, J.E. Supporting School Staff: Insights From Employee Health and Well-Being Programs. J. Sch. Health 2023, 93, 842–852. [Google Scholar] [CrossRef]
- Abdin, S.; Welch, R.K.; Byron-Daniel, J.; Meyrick, J. The Effectiveness of Physical Activity Interventions in Improving Well-Being across Office-Based Workplace Settings: A Systematic Review. Public Health 2018, 160, 70–76. [Google Scholar] [CrossRef]
- Schools for Health in Europe Network. School Health Promotion: Evidence for Effective Action; Schools for Health in Europe Network: Utrecht, The Netherlands, 2022. [Google Scholar]
- Ramos, M.; Tejera, E.; Cabeza, E. Evaluation of the Health Promoting Schools (CEPS) Program in the Balearic Islands, Spain. Int. J. Environ. Res. Public Health 2022, 19, 10756. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Characteristics n (%) | Total Sample 929 (100) | 95% Confidence Interval |
|---|---|---|
| Sex | ||
| Male | 374 (40.3) | 37.1–43.4 |
| Female | 555 (59.7) | 56.6–62.9 |
| Age (years) | ||
| Mean (Standard deviation) | 25.9 (16.3) | 24.9–27.0 |
| Median (Interquartile range) | 18 (12–43) | |
| Relationship with the school | ||
| Students | 531 (57.2) | 54.0–60.3 |
| Teachers | 198 (21.3) | 18.7–23.9 |
| Parents | 142 (15.3) | 13.0–17.6 |
| Management team | 30 (3.2) | 2.1–4.4 |
| Social worker or psychologist | 9 (1) | 0.4–1.6 |
| Administration and services staff | 9 (1) | 0.4–1.6 |
| Catering staff | 5 (0.5) | 0.1–1 |
| Nurses and doctors | 3 (0.3) | 0.1–0.6 |
| Maintenance staff | 2 (0.2) | 0.01–0.5 |
| Continents nationality | ||
| Europe | 766 (82.5) | 80.0–84.9 |
| America | 75 (8.1) | 6.3–9.8 |
| Asia | 68 (7.3) | 5.6–8.9 |
| Africa | 17 (1.8) | 1–2.7 |
| Oceania | 3 (0.3) | 0.1–0.5 |
| Open-Text Responses n (%) | 245 (100) |
|---|---|
| Related to the environment/school/teachers | 66 (27.0) |
| Related to physical exercise and food | 53 (21.6) |
| Related to SQFR (Suggestions, Questions, Feedback, and Requests) regarding the questions in the quick assessment tool. | 28 (11.4) |
| Related to emotional well-being | 26 (10.6) |
| Related to healthy leisure | 26 (10.6) |
| Related to affective sexual education | 2 (0.8) |
| Related to other reasons | 44 (18.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrio-Cortes, J.; Díaz-Quesada, M.; Martínez-Cuevas, M.; McGill, A.; Lozano-Hernández, C.M.; Ruiz-Zaldibar, C.; Beca-Martínez, M.T.; Ruiz-López, M. Evaluation of Health Promotion in International Schools Using the Schools for Health in Europe (SHE) Rapid Assessment Tool. Healthcare 2025, 13, 633. https://doi.org/10.3390/healthcare13060633
Barrio-Cortes J, Díaz-Quesada M, Martínez-Cuevas M, McGill A, Lozano-Hernández CM, Ruiz-Zaldibar C, Beca-Martínez MT, Ruiz-López M. Evaluation of Health Promotion in International Schools Using the Schools for Health in Europe (SHE) Rapid Assessment Tool. Healthcare. 2025; 13(6):633. https://doi.org/10.3390/healthcare13060633
Chicago/Turabian StyleBarrio-Cortes, Jaime, María Díaz-Quesada, María Martínez-Cuevas, Amelia McGill, Cristina María Lozano-Hernández, Cayetana Ruiz-Zaldibar, María Teresa Beca-Martínez, and Montserrat Ruiz-López. 2025. "Evaluation of Health Promotion in International Schools Using the Schools for Health in Europe (SHE) Rapid Assessment Tool" Healthcare 13, no. 6: 633. https://doi.org/10.3390/healthcare13060633
APA StyleBarrio-Cortes, J., Díaz-Quesada, M., Martínez-Cuevas, M., McGill, A., Lozano-Hernández, C. M., Ruiz-Zaldibar, C., Beca-Martínez, M. T., & Ruiz-López, M. (2025). Evaluation of Health Promotion in International Schools Using the Schools for Health in Europe (SHE) Rapid Assessment Tool. Healthcare, 13(6), 633. https://doi.org/10.3390/healthcare13060633