

Advanced Glycation End Products and Mobility Decline: A Novel Perspective on Aging


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
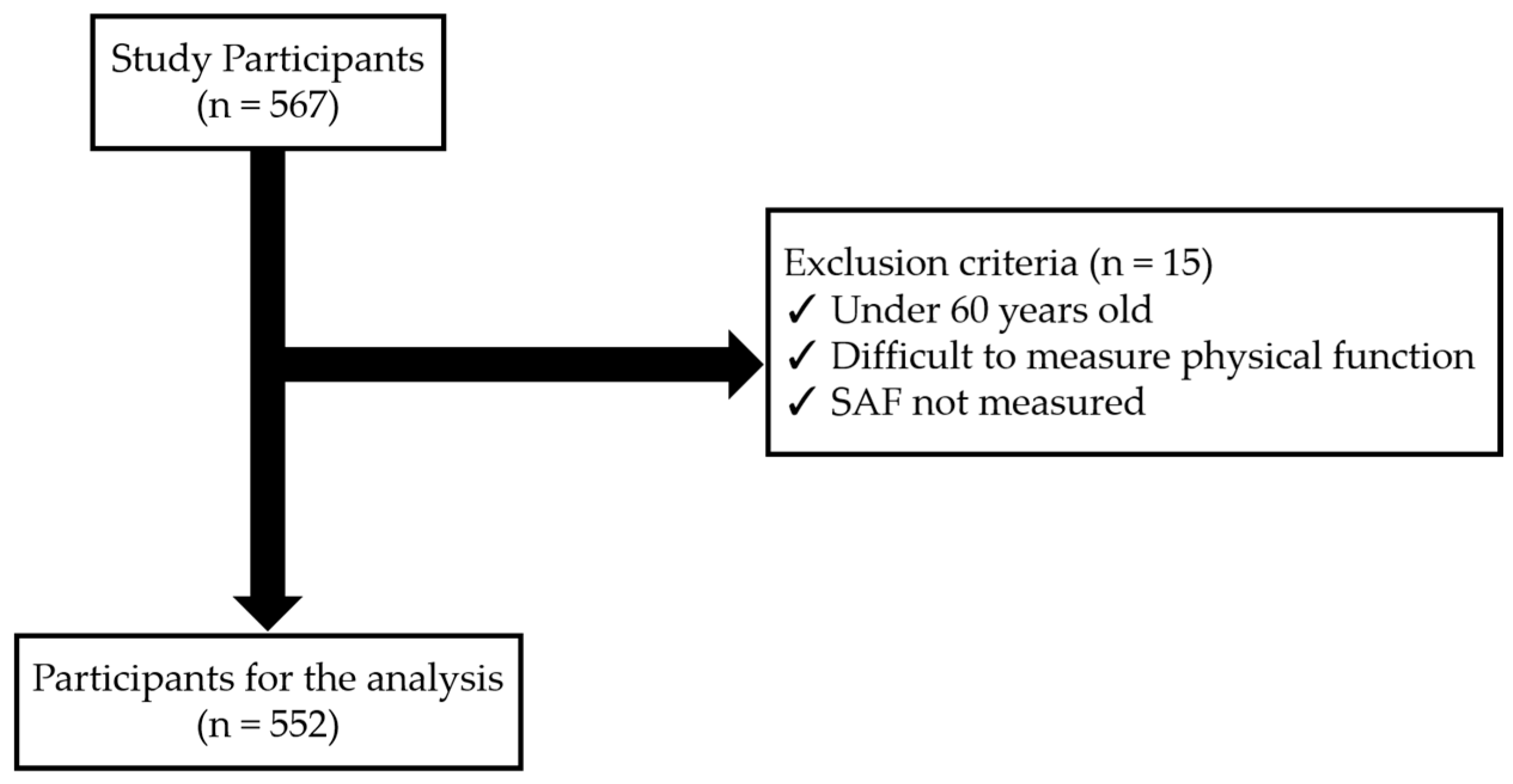
2.2. Study Participants
2.3. SAF Measurement
2.4. Measurement of Lower Limb Strength
2.5. Measurement of Gait Speed
2.6. Static Balance Measurement
2.7. Dynamic Balance Measurement
2.8. Statistical Analysis
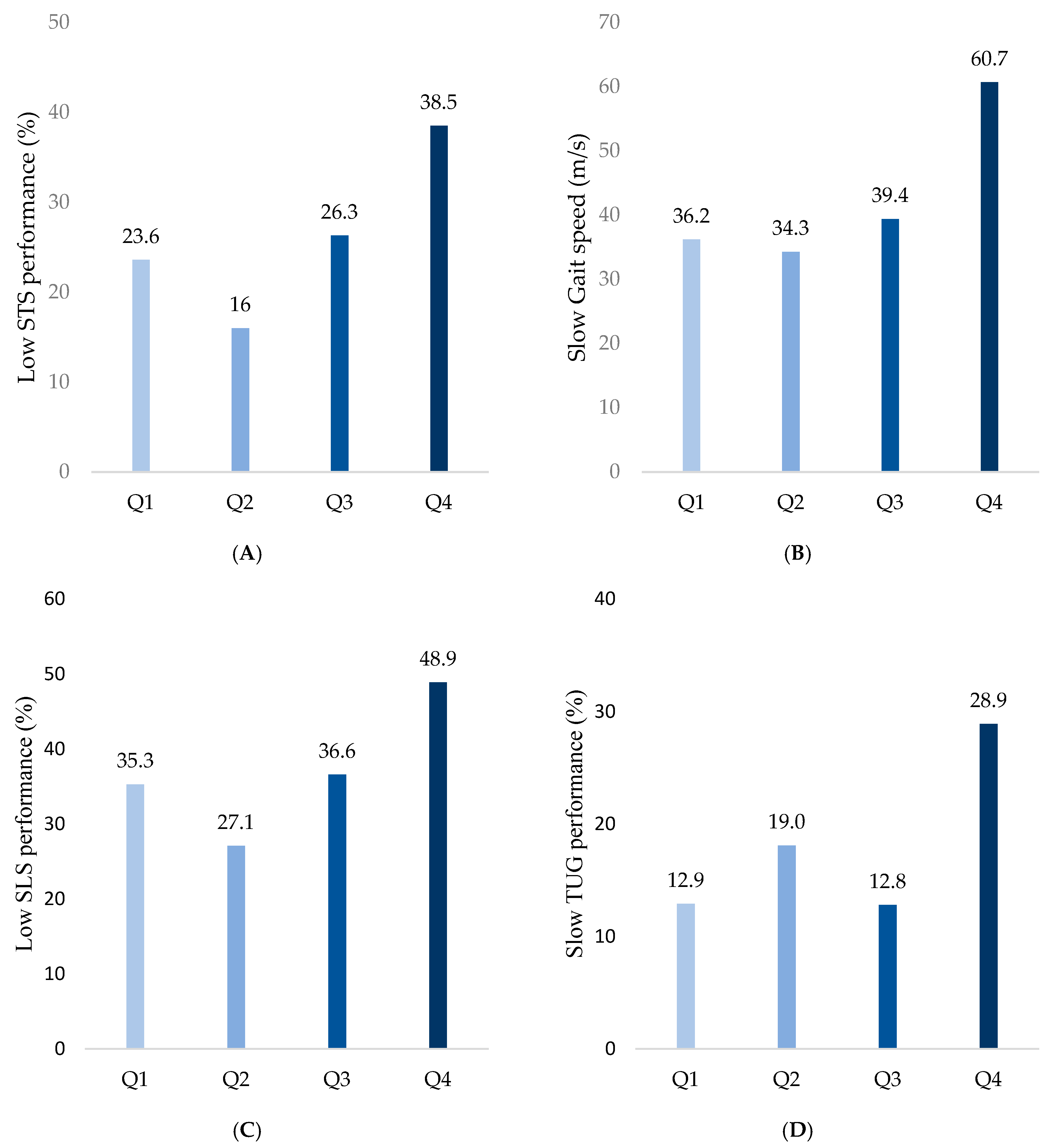
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- La Grow, S.; Yeung, P.; Towers, A.; Alpass, F.; Stephens, C. The Impact of Mobility on Quality of Life among Older Persons. J. Aging Health 2013, 25, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Gomes, E.S.A.; Ramsey, K.A.; Rojer, A.G.M.; Reijnierse, E.M.; Maier, A.B. The Association of Objectively Measured Physical Activity and Sedentary Behavior with (Instrumental) Activities of Daily Living in Community-Dwelling Older Adults: A Systematic Review. Clin. Interv. Aging 2021, 16, 1877–1915. [Google Scholar] [CrossRef]
- Rantakokko, M.; Mänty, M.; Rantanen, T. Mobility Decline in Old Age. Exerc. Sport Sci. Rev. 2013, 41, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Billot, M.; Calvani, R.; Urtamo, A.; Sánchez-Sánchez, J.L.; Ciccolari-Micaldi, C.; Chang, M.; Roller-Wirnsberger, R.; Wirnsberger, G.; Sinclair, A.; Vaquero-Pinto, N.; et al. Preserving Mobility in Older Adults with Physical Frailty and Sarcopenia: Opportunities, Challenges, and Recommendations for Physical Activity Interventions. Clin. Interv. Aging 2020, 15, 1675. [Google Scholar] [CrossRef]
- Aveiro, M.C.; Driusso, P.; Barham, E.J.; Pavarini, S.C.I.; Oishi, J. Mobility and the Risk of Falls among Elderly People of the Community of São Carlos. Cien. Saude Colet. 2012, 17, 2481–2488. [Google Scholar] [CrossRef]
- Ward, R.E.; Beauchamp, M.K.; Latham, N.K.; Leveille, S.G.; Percac-Lima, S.; Kurlinski, L.; Ni, P.; Goldstein, R.; Jette, A.M.; Bean, J.F. Neuromuscular Impairments Contributing to Persistently Poor and Declining Lower-Extremity Mobility among Older Adults: New Findings Informing Geriatric Rehabilitation. Arch. Phys. Med. Rehabil. 2016, 97, 1316. [Google Scholar] [CrossRef]
- Gouveia, É.R.; Gouveia, B.R.; Ihle, A.; Kliegel, M.; Marques, A.; Freitas, D.L. Balance and Mobility Relationships in Older Adults: A Representative Population-Based Cross-Sectional Study in Madeira, Portugal. Arch. Gerontol. Geriatr. 2019, 80, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Waqas, K.; Chen, J.; Rivadeneira, F.; Uitterlinden, A.G.; Voortman, T.; Carola Zillikens, M. Skin Autofluorescence, a Noninvasive Biomarker of Advanced Glycation End-Products, Is Associated with Frailty: The Rotterdam Study. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 2032–2039. [Google Scholar] [CrossRef]
- Kasper, M.; Funk, R.H. Age-Related Changes in Cells and Tissues Due to Advanced Glycation End Products (AGEs). Arch. Gerontol. Geriatr. 2001, 32, 233–243. [Google Scholar] [CrossRef]
- Mori, H.; Kuroda, A.; Araki, M.; Suzuki, R.; Taniguchi, S.; Tamaki, M.; Akehi, Y.; Matsuhisa, M. Advanced Glycation End-products Are a Risk for Muscle Weakness in Japanese Patients with Type 1 Diabetes. J. Diabetes Investig. 2016, 8, 377. [Google Scholar] [CrossRef]
- Chrysanthou, M.; Estruch, I.M.; Rietjens, I.M.C.M.; Wichers, H.J.; Hoppenbrouwers, T. In Vitro Methodologies to Study the Role of Advanced Glycation End Products (AGEs) in Neurodegeneration. Nutrients 2022, 14, 363. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Bandinelli, S.; Sun, K.; Guralnik, J.M.; Ferrucci, L. Relationship of an Advanced Glycation End Product, Plasma Carboxymethyl-Lysine, with Slow Walking Speed in Older Adults: The InCHIANTI Study. Eur. J. Appl. Physiol. 2010, 108, 191–195. [Google Scholar] [CrossRef]
- Drenth, H.; Zuidema, S.; Bunt, S.; Bautmans, I.; van der Schans, C.; Hobbelen, H. The Contribution of Advanced Glycation End Product (AGE) Accumulation to the Decline in Motor Function. Eur. Rev. Aging Phys. Act. 2016, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.W.; Li, C.I.; Liu, C.S.; Lin, C.H.; Lin, W.Y.; Li, T.C.; Lin, C.C. Relationship among Urinary Advanced Glycation-End Products, Skeletal Muscle Mass and Physical Performance in Community-Dwelling Older Adults. Geriatr. Gerontol. Int. 2019, 19, 1017–1022. [Google Scholar] [CrossRef]
- Chen, J.H.; Lin, X.; Bu, C.; Zhang, X. Role of Advanced Glycation End Products in Mobility and Considerations in Possible Dietary and Nutritional Intervention Strategies. Nutr. Metab. 2018, 15, 72. [Google Scholar] [CrossRef]
- Kazakos, K.; Tzilini, M.; Folinas, D.; Chatzidimitriou, M.; Papaliangas, V. Skin Autofluorescence a Non-Invasive Biomarker of Ages and Its Association to Metabolic Parameters in a Greek Diabetic Population. Diabetes Res. Open J. 2021, 7, 12–15. [Google Scholar] [CrossRef]
- Momma, H.; Niu, K.; Kobayashi, Y.; Guan, L.; Sato, M.; Guo, H.; Chujo, M.; Otomo, A.; Yufei, C.; Tadaura, H.; et al. Skin Advanced Glycation End Product Accumulation and Muscle Strength among Adult Men. Eur. J. Appl. Physiol. 2011, 111, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.H.; Tsai, S.C.; Lin, H.W.; Chen, C.N.; Hwu, C.M. Increased Serum Levels of Advanced Glycation End Products Are Negatively Associated with Relative Muscle Strength in Patients with Type 2 Diabetes Mellitus. BMC Endocr. Disord. 2022, 22, 118. [Google Scholar] [CrossRef]
- Sadeghi, H.; Jehu, D.A.; Daneshjoo, A.; Shakoor, E.; Razeghi, M.; Amani, A.; Hakim, M.N.; Yusof, A. Effects of 8 Weeks of Balance Training, Virtual Reality Training, and Combined Exercise on Lower Limb Muscle Strength, Balance, and Functional Mobility Among Older Men: A Randomized Controlled Trial. Sports Health 2021, 13, 606. [Google Scholar] [CrossRef]
- Korean Statistical Information Service. Updated 9 July 2021. Available online: https://www.kostat.go.kr/board.es?mid=a10301010000&bid=10820&act=view&list_no=432917 (accessed on 30 August 2024).
- Koetsier, M.; Nur, E.; Chunmao, H.; Lutgers, H.L.; Links, T.P.; Smit, A.J.; Rakhorst, G.; Graaff, R. Skin Color Independent Assessment of Aging Using Skin Autofluorescence. Opt. Express 2010, 18, 14416. [Google Scholar] [CrossRef]
- Park, T.S.; Shin, M.J. Comprehensive Assessment of Lower Limb Function and Muscle Strength in Sarcopenia: Insights from the Sit-to-Stand Test. Ann. Geriatr. Med. Res. 2024, 28, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.T.; Nguyen, H.T.T.; Nguyen, H.T.T.; Nguyen, T.X.; Nguyen, T.N.; Nguyen, T.T.H.; Nguyen, A.L.; Pham, T.; Vu, H.T.T. Walking Speed Assessed by 4-Meter Walk Test in the Community-Dwelling Oldest Old Population in Vietnam. Int. J. Environ. Res. Public Health 2022, 19, 9788. [Google Scholar] [CrossRef]
- Perera, S.; Patel, K.V.; Rosano, C.; Rubin, S.M.; Satterfield, S.; Harris, T.; Ensrud, K.; Orwoll, E.; Lee, C.G.; Chandler, J.M.; et al. Gait Speed Predicts Incident Disability: A Pooled Analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, E.; Seiger, Å.; Hirschfeld, H. One-Leg Stance in Healthy Young and Elderly Adults: A Measure of Postural Steadiness? Clin. Biomech. 2004, 19, 688–694. [Google Scholar] [CrossRef]
- Vellas, B.J.; Wayne, S.J.; Romero, L.; Baumgartner, R.N.; Rubenstein, L.Z.; Garry, P.J. One-Leg Balance Is an Important Predictor of Injurious Falls in Older Persons. J. Am. Geriatr. Soc. 1997, 45, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.; Teixeira, J.E.; Forte, P. The Reliability of the Timed Up and Go Test among Portuguese Elderly. Healthcare 2023, 11, 928. [Google Scholar] [CrossRef]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go Test a Useful Predictor of Risk of Falls in Community Dwelling Older Adults: A Systematic Review and Meta-Analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef]
- Haus, J.M.; Carrithers, J.A.; Trappe, S.W.; Trappe, T.A. Collagen, Cross-Linking, and Advanced Glycation End Products in Aging Human Skeletal Muscle. J. Appl. Physiol. 2007, 103, 2068–2076. [Google Scholar] [CrossRef]
- Semba, R.D.; Nicklett, E.J.; Ferrucci, L. Does Accumulation of Advanced Glycation End Products Contribute to the Aging Phenotype? J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 963–975. [Google Scholar] [CrossRef]
- Lord, S.R.; Murray, S.M.; Chapman, K.; Munro, B.; Tiedemann, A. Sit-to-Stand Performance Depends on Sensation, Speed, Balance, and Psychological Status in Addition to Strength in Older People. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M539–M543. [Google Scholar] [CrossRef]
- Alcazar, J.; Kamper, R.S.; Aagaard, P.; Haddock, B.; Prescott, E.; Ara, I.; Suetta, C. Relation between Leg Extension Power and 30-s Sit-to-Stand Muscle Power in Older Adults: Validation and Translation to Functional Performance. Sci. Rep. 2020, 10, 16337. [Google Scholar] [CrossRef] [PubMed]
- Hafer, J.F.; Boyer, K.A. Age Related Differences in Segment Coordination and Its Variability during Gait. Gait Posture 2018, 62, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Neptune, R.R.; Sasaki, K.; Kautz, S.A. The Effect of Walking Speed on Muscle Function and Mechanical Energetics. Gait Posture 2008, 28, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, K.; Makabe, H. Correlation Between Skin Autofluorescence and Muscle Activities of Lower Limb in Aging Without Disease and Disability. Gerontol. Geriatr. Med. 2022, 8, 23337214221140224. [Google Scholar] [CrossRef]
- Couppé, C.; Brüggebusch Svensson, R.; Kongsgaard, M.; Kovanen, V.; Grosset, J.-F.; Snorgaard, O.; Bencke, J.; Overgaard Larsen, J.; Bandholm, T.; Møller Christensen, T.; et al. Human Achilles Tendon Glycation and Function in Diabetes. J. Appl. Physiol. 2016, 120, 130–137. [Google Scholar] [CrossRef]
- Waqas, K.; Chen, J.; Trajanoska, K.; Ikram, M.A.; Uitterlinden, A.G.; Rivadeneira, F.; Zillikens, M.C. Skin Autofluorescence, a Noninvasive Biomarker for Advanced Glycation End-Products, Is Associated with Sarcopenia. J. Clin. Endocrinol. Metab. 2022, 107, e793–e803. [Google Scholar] [CrossRef]
- Tabara, Y.; Ikezoe, T.; Yamanaka, M.; Setoh, K.; Segawa, H.; Kawaguchi, T.; Kosugi, S.; Nakayama, T.; Ichihashi, N.; Tsuboyama, T.; et al. Advanced Glycation End Product Accumulation Is Associated with Low Skeletal Muscle Mass, Weak Muscle Strength, and Reduced Bone Density: The Nagahama Study. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 1446–1453. [Google Scholar] [CrossRef]
- Fusco, A.; Giancotti, G.F.; Fuchs, P.X.; Wagner, H.; Varalda, C.; Capranica, L.; Cortis, C. Dynamic Balance Evaluation: Reliability and Validity of a Computerized Wobble Board. J. Strength Cond. Res. 2020, 34, 1709–1715. [Google Scholar] [CrossRef]
- Yim-Chiplis, P.K.; Talbot, L.A. Defining and Measuring Balance in Adults. Biol. Res. Nurs. 2000, 1, 321–331. [Google Scholar] [CrossRef]
- Woollacott, M.H.; Tang, P.F. Balance Control during Walking in the Older Adult: Research and Its Implications. Phys. Ther. 1997, 77, 646–660. [Google Scholar] [CrossRef]
- Guskiewicz, K.M.; Perrin, D.H. Research and Clinical Applications of Assessing Balance. J. Sport Rehabil. 1996, 5, 45–63. [Google Scholar] [CrossRef]
- Muehlbauer, T.; Gollhofer, A.; Granacher, U. Associations Between Measures of Balance and Lower-Extremity Muscle Strength/Power in Healthy Individuals Across the Lifespan: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1671–1692. [Google Scholar] [CrossRef] [PubMed]
- Arnold, P.; Njemini, R.; Vantieghem, S.; Gorus, E.; Pool-Goudzwaard, A.; Buyl, R.; Bautmans, I. Reaction Time in Healthy Elderly Is Associated with Chronic Low-Grade Inflammation and Advanced Glycation End Product. Exp. Gerontol. 2018, 108, 118–124. [Google Scholar] [CrossRef]
- Iida, H.; Takegami, Y.; Osawa, Y.; Funahashi, H.; Ozawa, Y.; Ido, H.; Asamoto, T.; Otaka, K.; Tanaka, S.; Nakashima, H.; et al. Association between Advanced Glycation End-Products and Fall Risk in Older Adults: The Yakumo Study. Geriatr. Gerontol. Int. 2024, 24, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Sanchis-Gomar, F.; Montagnana, M. Biological Markers in Older People at Risk of Mobility Limitations. Curr. Pharm. Des. 2014, 20, 3222–3244. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Total Population | |
|---|---|
| N | 552 |
| SAF, AU | 2.92 ± 0.62 |
| Age (years) | 76.33 ± 7.98 |
| Sex (men, %) | 23 |
| BMI (kg/m2) | 24.49 ± 3.65 |
| Diabetes status (Yes, %) | 27 |
| Smoke status (Yes, %) | 12.6 |
| ASMI (kg/m2) | 6.54 ± 1.42 |
| CC (cm) | 33.78 ± 3.17 |
| Q1 | Q2 | Q3 | Q4 | p | |
|---|---|---|---|---|---|
| N | 140 | 144 | 133 | 135 | |
| SAF (AU) | 2.25 ± 0.31 | 2.65 ± 0.18 | 3.07 ± 0.13 | 3.75 ± 0.39 | <0.001 *** |
| Age (years) | 76.39 ± 8.61 | 74.26 ± 8.01 | 75.86 ± 7.24 | 78.96 ± 7.27 | <0.001 *** |
| Sex (men,%) | 12.9 | 20.8 | 19.7 | 42.5 | <0.001 *** |
| BMI (kg/m2) | 24.96 ± 3.97 | 24.50 ± 3.64 | 24.15 ± 3.29 | 24.34 ± 3.65 | 0.333 |
| Diabetes (Yes, %) | 17.5 | 25.4 | 33.1 | 38.6 | 0.001 *** |
| Smoke (Yes, %) | 8.3 | 11.3 | 10.2 | 20.7 | 0.001 *** |
| ASMI (kg/m2) | 6.34 ± 1.32 | 6.58 ± 1.35 | 6.40 ± 1.43 | 6.83 ± 1.53 | 0.042 * |
| CC (cm) | 33.87 ± 3.42 | 34.04 ± 3.16 | 33.45 ± 3.02 | 33.71 ± 3.04 | 0.517 |
| STS (reps) | 14.51 ± 4.88 | 15.25 ± 4.69 | 13.63 ± 5.04 | 11.96 ± 4.61 | <0.001 *** |
| Gait speed (m/s) | 0.87 ± 0.24 | 0.87 ± 0.26 | 0.85 ± 0.23 | 0.73 ± 0.25 | <0.001 *** |
| SLS (s) | 19.64 ± 19.26 | 21.66 ± 20.15 | 18.99 ± 20.67 | 12.88 ± 15.87 | <0.001 *** |
| TUG (s) | 9.64 ± 4.12 | 9.85 ± 5.27 | 10.35 ± 5.91 | 13.13 ± 8.29 | <0.001 ** |
| SAF AGEs | Age | Sex (Men) | BMI | Diabetes | Smoke | ASMI | CC | STS | Gait Speed | SLS | TUG | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SAF AGEs | 1 | |||||||||||
| Age | 0.178 *** | 1 | ||||||||||
| Sex (men) | 0.201 *** | 0.085 * | 1 | |||||||||
| BMI | −0.114 ** | 0.088 * | −0.078 | 1 | ||||||||
| Diabetes | 0.181 *** | 0.028 | 0.004 | 0.094 * | 1 | |||||||
| Smoke | −0.119 ** | −0.009 | −0.529 *** | 0.024 | 0.003 | 1 | ||||||
| ASMI | 0.027 | −0.177 *** | 0.699 *** | 0.511 *** | 0.049 | −0.393 *** | 1 | |||||
| CC | −0.110 ** | −0.258 *** | 0.294 *** | 0.555 *** | 0.003 | −0.144 ** | 0.697 *** | 1 | ||||
| STS | −0.211 *** | −0.437 *** | −0.031 | −0.051 | −0.058 | −0.006 | 0.084 | 0.196 *** | 1 | |||
| Gait speed | −0.243 *** | −0.398 *** | −0.058 | −0.095 * | −0.081 | 0.053 | 0.012 | 0.121 ** | 0.513 *** | 1 | ||
| SLS | −0.201 *** | −0.559 *** | −0.025 | −0.099 * | −0.117 ** | −0.009 | 0.088 * | 0.204 *** | 0.508 *** | −0.523 ** | 1 | |
| TUG | 0.239 *** | 0.517 *** | −0.021 | 0.111 ** | 0.107 * | 0.041 | −0.100 * | −0.204 *** | −0.625 *** | −0.787 *** | −0.608 *** | 1 |
| Low STS Performance | Slow Gait Speed | Low SLS Performance | Slow TUG | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Q1 | Reference | Reference | Reference | Reference | ||||
| Q2 | 1.10 (0.54–2.24) | 0.794 | 1.17 (0.70–1.96) | 0.563 | 1.33 (0.77–2.23) | 0.311 | 1.93 (0.99–3.80) | 0.055 |
| Q3 | 1.61 (0.82–3.17) | 0.166 | 1.13 (0.67–1.92) | 0.637 | 1.56 (0.90–2.70) | 0.113 | 0.90 (0.42–1.91) | 0.778 |
| Q4 | 2.43 (1.29–4.59) | 0.006 ** | 2.28 (1.35–3.84) | 0.002 *** | 2.52 (1.43–4.46) | 0.001 *** | 2.00 (1.05–3.85) | 0.035 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.J.; Lee, M.J.; Kim, J. Advanced Glycation End Products and Mobility Decline: A Novel Perspective on Aging. Healthcare 2025, 13, 613. https://doi.org/10.3390/healthcare13060613
Park HJ, Lee MJ, Kim J. Advanced Glycation End Products and Mobility Decline: A Novel Perspective on Aging. Healthcare. 2025; 13(6):613. https://doi.org/10.3390/healthcare13060613
Chicago/Turabian StylePark, Hyeong Jun, Moon Jin Lee, and Jiyoun Kim. 2025. "Advanced Glycation End Products and Mobility Decline: A Novel Perspective on Aging" Healthcare 13, no. 6: 613. https://doi.org/10.3390/healthcare13060613
APA StylePark, H. J., Lee, M. J., & Kim, J. (2025). Advanced Glycation End Products and Mobility Decline: A Novel Perspective on Aging. Healthcare, 13(6), 613. https://doi.org/10.3390/healthcare13060613