

Paramedics’ Behavior Patterns When Transferring Non-Mobile Patients from the Ground to a Stretcher

Abstract
1. Introduction
2. Material and Methods
2.1. Field Data
2.2. Definition of a Non-Mobile Patient Transfer
2.3. Ergonomic Observation Grids
2.3.1. Grid Construction
2.3.2. Grid Validation
2.3.3. Grid Use and Item Reduction
2.4. Data Synthesis
3. Results
3.1. Ergonomic Observation Grids
3.2. Description of EMT-Ps’ Behavior During Non-Mobile Patient Transfers
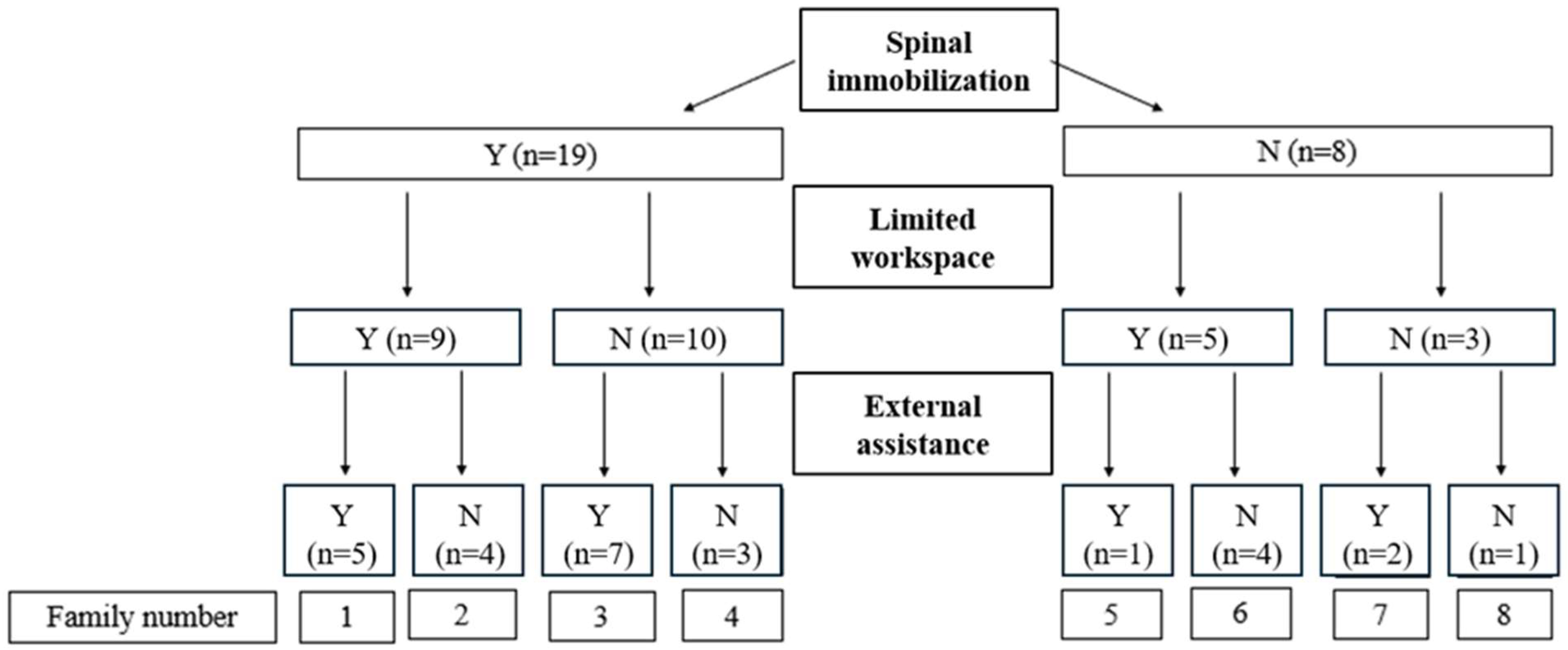
3.2.1. Spinal Immobilization and Limited Work Area
3.2.2. Spinal Immobilization and Suitable Work Area
3.2.3. Without Spinal Immobilization and with a Limited or Suitable Work Area
3.2.4. External Assistance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- U.S. Bureau of Labor Statistics (2021–2022). Survey of Occupational Injuries and Illnesses Data: U.S. Bureau of Labor Statistics (bls.gov). Available online: https://www.bls.gov/iif/nonfatal-injuries-and-illnesses-tables.htm (accessed on 8 June 2024).
- Maguire, B.J.; Smith, S. Injuries and fatalities among emergency medical technicians and paramedics in the United States. Prehosp. Disaster Med. 2013, 28, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Friedenberg, R.; Kalichman, L.; Ezra, D.; Wacht, O.; Alperovitch-Najenson, D. Work-related musculoskeletal disorders and injuries among emergency medical technicians and paramedics: A comprehensive narrative review. Arch. Environ. Occup. Health 2020, 77, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.H.; Sim, M.R.; Black, O.; Smith, P. Occupational injury risk among ambulance officers and paramedics compared with other healthcare workers in Victoria, Australia: Analysis of workers’ compensation claims from 2003 to 2012. Occup. Environ. Med. 2015, 72, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Corbeil, P.; Plamondon, A.; Tremblay, A.; Prairie, J.; Larouche, D.; Hegg-Deloye, S. Measurement of Emergency Medical Technician-Paramedics’ Exposure to Musculoskeletal Risk Factors; Institut de recherche Robert Sauvé en santé et en sécurité du travail: Montreal, QC, Canada, 2017; p. 125. [Google Scholar]
- Morales, L.; McEachern, B.M.; MacPhee, R.S.; Fischer, S.L. Patient acuity as a determinant of paramedics’ frequency of being exposed to physically demanding work activities. Appl. Ergon. 2016, 56, 187–193. [Google Scholar] [CrossRef]
- Posluszny, K.M.; Ho, D.C.; Veerasammy, S.; Taylor, C.; McDougall, R.; Fischer, S.L. A mixed methods approach to describe the efficacy of lift assist device use to reduce low back musculoskeletal disorder risk factors during three common patient extrication scenarios. Appl. Ergon. 2024, 121, 104361. [Google Scholar] [CrossRef] [PubMed]
- Lavender, S.A.; Sommerich, C.M.; Bigelow, S.; Weston, E.B.; Seagren, K.; Pay, N.A.; Sillars, D.; Ramachandran, V.; Sun, C.; Xu, Y.; et al. A biomechanical evaluation of potential ergonomic solutions for use by firefighter and EMS providers when lifting heavy patients in their homes. Appl. Ergon. 2020, 82, 102910. [Google Scholar] [CrossRef] [PubMed]
- Lavender, S.A.; Sommerich, C.M. Preventing Firefighter Injuries When Handling Obsese Patients: Understanding the Patient Handling Scenarios. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2017, 61, 1015–1016. [Google Scholar] [CrossRef]
- Lavender, S.A.; Conrad, K.M.; Reichelt, P.A.; Johnson, P.W.; Meyer, F.T. Biomechanical analyses of paramedics simulating frequently performed strenuous work tasks. Appl. Ergon. 2000, 31, 167–177. [Google Scholar] [CrossRef]
- Larouche, D.; Bellemare, M.; Prairie, J.; Hegg-Deloye, S.; Corbeil, P. Overall risk index for patient transfers in total assistance mode executed by emergency medical technician-paramedics in real work situations. Appl. Ergon. 2019, 74, 177–185. [Google Scholar] [CrossRef]
- Gallagher, S.; Marras, W.S. Tolerance of the lumbar spine to shear: A review and recommended exposure limits. Clin. Biomech. 2012, 27, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Jäger, M. Extended compilation of autopsy-material measurements on lumbar ultimate compressive strength for deriving reference values in ergonomic work design: The Revised Dortmund Recommendations. EXCLI J. 2018, 17, 362–385. [Google Scholar] [PubMed]
- Armstrong, D.P.; Budarick, A.R.; Pegg, C.E.E.; Graham, R.B.; Fischer, S.L. Feature Detection and Biomechanical Analysis to Objectively Identify High Exposure Movement Strategies When Performing the EPIC Lift Capacity test. J. Occup. Rehabil. 2021, 31, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Vallée-Marcotte, J.; Muller, A.; Robert-Lachaine, X.; Fecteau, V.; Denis, D.; Plamondon, A.; Corbeil, P. New taxonomy for assessing manual material handlers’ footstep patterns. Appl. Ergon. 2021, 94, 103424. [Google Scholar] [CrossRef]
- Plamondon, A.; Denis, D.; Delisle, A.; Lariviere, C.; Salazar, E. Biomechanical differences between expert and novice workers in a manual material handling task. Ergonomics 2010, 53, 1239–1253. [Google Scholar] [CrossRef]
- Denis, D.; Lortie, M.; Plamondon, A.; St-Vincent, M.; Gonella, M.; Irsst, G. Definition proposal of handling competency and impacts on training/Proposition d’une définition de la compétence en manutention et impacts sur la formation. Le Trav. Hum. 2013, 76, 129–153. [Google Scholar] [CrossRef]
- LeBoterf, G. Développer la Compétence des Professionnels: Construire les Parcours de Professionnalisation; Editions d’Organisation: Paris, France, 2002. [Google Scholar]
- Arial, M.; Benoit, D.; Wild, P. Exploring implicit preventive strategies in prehospital emergency workers: A novel approach for preventing back problems. Appl. Ergon. 2014, 45, 1003–1009. [Google Scholar] [CrossRef]
- Larouche, D.; Corbeil, P.; Bellemare, M.; Authier, M.; Prairie, J.; Hegg-Deloye, S. To what extent do paramedics apply safe handling principles when transferring patients from stair chairs to stretchers? Ergonomics 2019, 62, 1313–1326. [Google Scholar] [CrossRef]
- Prairie, J.; Plamondon, A.; Larouche, D.; Hegg-Deloye, S.; Corbeil, P. Paramedics’ working strategies while loading a stretcher into an ambulance. Appl. Ergon. 2017, 65, 112–122. [Google Scholar] [CrossRef]
- Armstrong, D.P.; Fischer, S.L. Understanding individual differences in lifting mechanics: Do some people adopt motor control strategies that minimize biomechanical exposure. Hum. Mov. Sci. 2020, 74, 102689. [Google Scholar] [CrossRef]
- Lavender, S.A.; Conrad, K.M.; Reichelt, P.A.; Gacki-Smith, J.; Kohok, A.K. Designing ergonomic interventions for EMS workers, Part I: Transporting patients down the stairs. Appl. Ergon. 2007, 38, 71–81. [Google Scholar] [CrossRef]
- Conrad, K.M.; Reichelt, P.A.; Lavender, S.A.; Gacki-Smith, J.; Hattle, S. Designing ergonomic interventions for EMS workers: Concept generation of patient-handling devices. Appl. Ergon. 2008, 39, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Weiler, M.R.; Lavender, S.A.; Crawford, J.M.; Reichelt, P.A.; Conrad, K.M.; Browne, M.W. Identification of factors that affect the adoption of an ergonomic intervention among Emergency Medical Service workers. Ergonomics 2012, 55, 1362–1372. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Lavender, S.A.; Sommerich, C.M. The efficacy of a lifting strap as an ergonomic intervention for EMS providers: Does it make it easier to raise a supine patient to an upright sitting posture? Appl. Ergon. 2021, 94, 103416. [Google Scholar] [CrossRef] [PubMed]
- Denis, D. Towards an Integrated Prevention Strategy for Manual Handling. Awareness Document on the Prevention of Musculoskeletal Disorders (MSDs) Related to Manual Handling Tasks; Institut de recherche Robert Sauvé en santé et en sécurité du travail: Montreal, QC, Canada, 2020; p. 28. [Google Scholar]
- Preston, C.C.; Colman, A.M. Optimal number of response categories in rating scales: Reliability, validity, discriminating power, and respondent preferences. Acta Psychol 2000, 104, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Gwet, K.L. Handbook of Inter-Rater Reliability: The Definitive Guide to Measuring the Extent of Agreement Among Raters, 4th ed.; Advances Analytics, LLC: Gaithersburg, MD, USA, 2014. [Google Scholar]
- Gallagher, S.; Schall, M.C., Jr. Musculoskeletal disorders as a fatigue failure process: Evidence, implications and research needs. Ergonomics 2017, 60, 255–269. [Google Scholar] [CrossRef]
- Lavender, S.A.; Conrad, K.M.; Reichelt, P.A.; Meyer, F.T.; Johnson, P.W. Postural analysis of paramedics simulating frequently performed strenuous work tasks. Appl. Ergon. 2000, 31, 45–57. [Google Scholar] [CrossRef]
- Schibye, B.; Sogaard, K.; Martinsen, D.; Klausen, K. Mechanical load on the low back and shoulders during pushing and pulling of two-wheeled waste containers compared with lifting and carrying of bags and bins. Clin. Biomech. 2001, 16, 549–559. [Google Scholar] [CrossRef]
- de Looze, M.P.; van Greuningen, K.; Rebel, J.; Kingma, I.; Kuijer, P.P. Force direction and physical load in dynamic pushing and pulling. Ergonomics 2000, 43, 377–390. [Google Scholar] [CrossRef]
- Knapik, G.G.; Marras, W.S. Spine loading at different lumbar levels during pushing and pulling. Ergonomics 2009, 52, 60–70. [Google Scholar] [CrossRef]
- Bazrgari, B.; Shirazi-Adl, A.; Arjmand, N. Analysis of squat and stoop dynamic liftings: Muscle forces and internal spinal loads. Eur. Spine J. 2007, 16, 687–699. [Google Scholar] [CrossRef]
- Garg, A.; Herrin, G. Stoop or squat. A biomechanical and metabolic evaluation. AIIE Trans. 1979, 11, 293–302. [Google Scholar] [CrossRef]
- Denis, D.; Gonella, M.; Comeau, M.; Lauzier, M. Questioning the value of manual material handling training: A scoping and critical literature review. Appl. Ergon. 2020, 89, 103186. [Google Scholar] [CrossRef]
- Burgess-Limerick, R. Squat, stoop, or something in between? Int. J. Ind. Ergon. 2003, 31, 143–148. [Google Scholar] [CrossRef]
- Plamondon, A.; Lariviere, C.; Denis, D.; St-Vincent, M.; Delisle, A. Sex differences in lifting strategies during a repetitive palletizing task. Appl. Ergon. 2014, 45, 1558–1569. [Google Scholar] [CrossRef]
- Maduri, A.; Pearson, B.L.; Wilson, S.E. Lumbar-pelvic range and coordination during lifting tasks. J. Electromyogr. Kinesiol. 2008, 18, 807–814. [Google Scholar] [CrossRef]
- Marras, W.S.; Davis, K.G.; Kirking, B.C.; Granata, K.P. Spine loading and trunk kinematics during team lifting. Ergonomics 1999, 42, 1258–1273. [Google Scholar] [CrossRef]
- Dennis, G.J.; Barrett, R.S. Spinal loads during two-person team lifting: Effect of matched versus unmatched standing height. Int. J. Ind. Ergon. 2003, 32, 25–38. [Google Scholar] [CrossRef]
- Resnick, M.L.; Sanchez, R. Reducing patient handling injuries through contextual training. J. Emerg. Nurs. 2009, 35, 504–508. [Google Scholar] [CrossRef]
- Nelson, A.; Baptiste, A.S. Evidence-based practices for safe patient handling and movement. Orthop. Nurs. 2006, 25, 366–379. [Google Scholar]
- Koppelaar, E.; Knibbe, J.J.; Miedema, H.S.; Burdorf, A. Determinants of implementation of primary preventive interventions on patient handling in healthcare: A systematic review. Occup. Environ. Med. 2009, 66, 353–360. [Google Scholar] [CrossRef]
- Owlia, M.; Kamachi, M.; Dutta, T. Reducing lumbar spine flexion using real-time biofeedback during patient handling tasks. Work 2020, 66, 41–51. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| With Spinal Immobilization (n = 19) | Without Spinal Immobilization (n = 8) | Total (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Limited Work Area (n = 9) | Suitable Work Area (n = 10) | Limited Work Area (n = 5) | Suitable Work Area (n = 3) | |||||||
| F/VF | U/VU | F/VF | U/VU | F/VF | U/VU | F/VF | U/VU | F/VF | U/VU | |
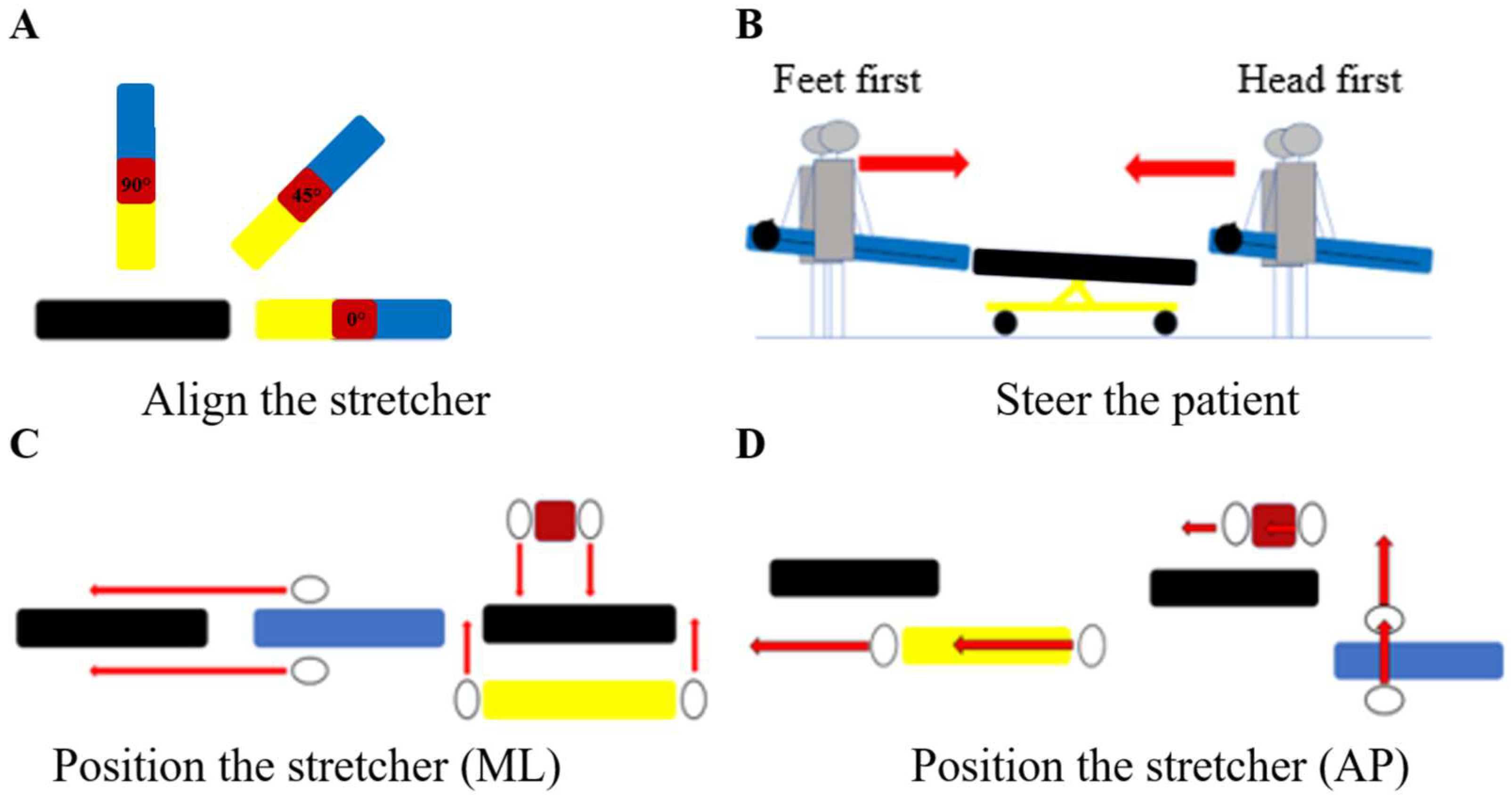
| Align | 5 (56%) | 4 (44%) | 8 (80%) | 2 (20%) | 1 (20%) | 4 (80%) | 2 (67%) | 1 (33%) | 59% | 41% |
| Steer | 4 (57%) | 3 (43%) | 4 (44%) | 5 (56%) | 2 (100%) | 0 (0%) | 1 (50%) | 1 (50%) | 55% | 45% |
| ML position | 8 (89%) | 1 (11%) | 9 (90%) | 1 (10%) | 5 (100%) | 0 (0%) | 3 (100%) | 0 (0%) | 93% | 7% |
| AP position | 5 (56%) | 4 (44%) | 7 (70%) | 3 (30%) | 1 (20%) | 4 (80%) | 0 (0%) | 3 (33%) | 44% | 56% |
| Adjust height | 7 (78%) | 2 (22%) | 9 (90%) | 1 (10%) | 4 (80%) | 1 (20%) | 1 (33%) | 2 (67%) | 78% | 22% |
| With Spinal Immobilization | Without Spinal Immobilization | |||
|---|---|---|---|---|
| Limited work area (n = 9) | Suitable work area (n = 10) | Limited work area (n = 5) | Suitable work area (n = 3) | |
| Whole-body lifting position | Squat (50%) Half squat (50%) | Squat (44%) Half squat (33%) | Squat (40%) Half squat (40%) | Squat (50%) Half squat (50%) |
| Whole-body loading position | Neutral (67%) Squat (22%) | Neutral (89%) Trunk flexion (11%) | Trunk flexion (75%) Squat (25%) | Neutral (50%) Squat (50%) |
| Postural asymmetry (pickup) | Neutral (100%) | Neutral (100%) | Neutral (100%) | Neutral (50%) Awkward (50%) |
| Postural asymmetry (travel) | Neutral (78%) Moderate (22%) | Neutral (56%) Moderate (44%) | Neutral (100%) | Neutral (50%) Moderate (50%) |
| Postural asymmetry (loading) | Neutral (89%) Awkward (11%) | Neutral (78%) Awkward (11%) | Awkward (50%) Moderate (25%) | Neutral (50%) Awkward (50%) |
| Feet position (pickup) | Even stance (100%) | Even stance (100%) | Even stance (100%) | Even stance (100%) |
| Hand position (pickup) | Low (44%) Neutral (33%) | Low (50%) Moderate (40%) | Moderate (44%) Low (44%) | Moderate (100%) |
| Lever arm (travel) | Short (56%) Large (22%) | Large (57%) Moderate (43%) | Large (60%) Moderate (20%) | Short (100%) |
| Lever arm (loading) | Moderate (63%) Large (25%) | Moderate (57%) Large (43%) | Moderate (50%) Large (25%) | Large (100%) |
| Synchronized movements (pickup) | Synchronized (78%) Unsynchronized (22%) | Synchronized (90%) Unsynchronized (10%) | Synchronized (100%) | Synchronized (67%) Unsynchronized (33%) |
| Synchronized movements (loading) | Synchronized (75%) Unsynchronized (25%) | Synchronized (70%) Unsynchronized (30%) | Synchronized (100%) | Synchronized (100%) |
| Loading methods | Fast loading (57%) Expected (43%) | Expected (100%) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanguay, M.; Bouffard, J.; Vallée-Marcotte, J.; Corbeil, P. Paramedics’ Behavior Patterns When Transferring Non-Mobile Patients from the Ground to a Stretcher. Healthcare 2025, 13, 611. https://doi.org/10.3390/healthcare13060611
Tanguay M, Bouffard J, Vallée-Marcotte J, Corbeil P. Paramedics’ Behavior Patterns When Transferring Non-Mobile Patients from the Ground to a Stretcher. Healthcare. 2025; 13(6):611. https://doi.org/10.3390/healthcare13060611
Chicago/Turabian StyleTanguay, Maïté, Jason Bouffard, Jasmin Vallée-Marcotte, and Philippe Corbeil. 2025. "Paramedics’ Behavior Patterns When Transferring Non-Mobile Patients from the Ground to a Stretcher" Healthcare 13, no. 6: 611. https://doi.org/10.3390/healthcare13060611
APA StyleTanguay, M., Bouffard, J., Vallée-Marcotte, J., & Corbeil, P. (2025). Paramedics’ Behavior Patterns When Transferring Non-Mobile Patients from the Ground to a Stretcher. Healthcare, 13(6), 611. https://doi.org/10.3390/healthcare13060611