

Combined Physical–Cognitive Therapies for the Health of Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis
 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sources of Information
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
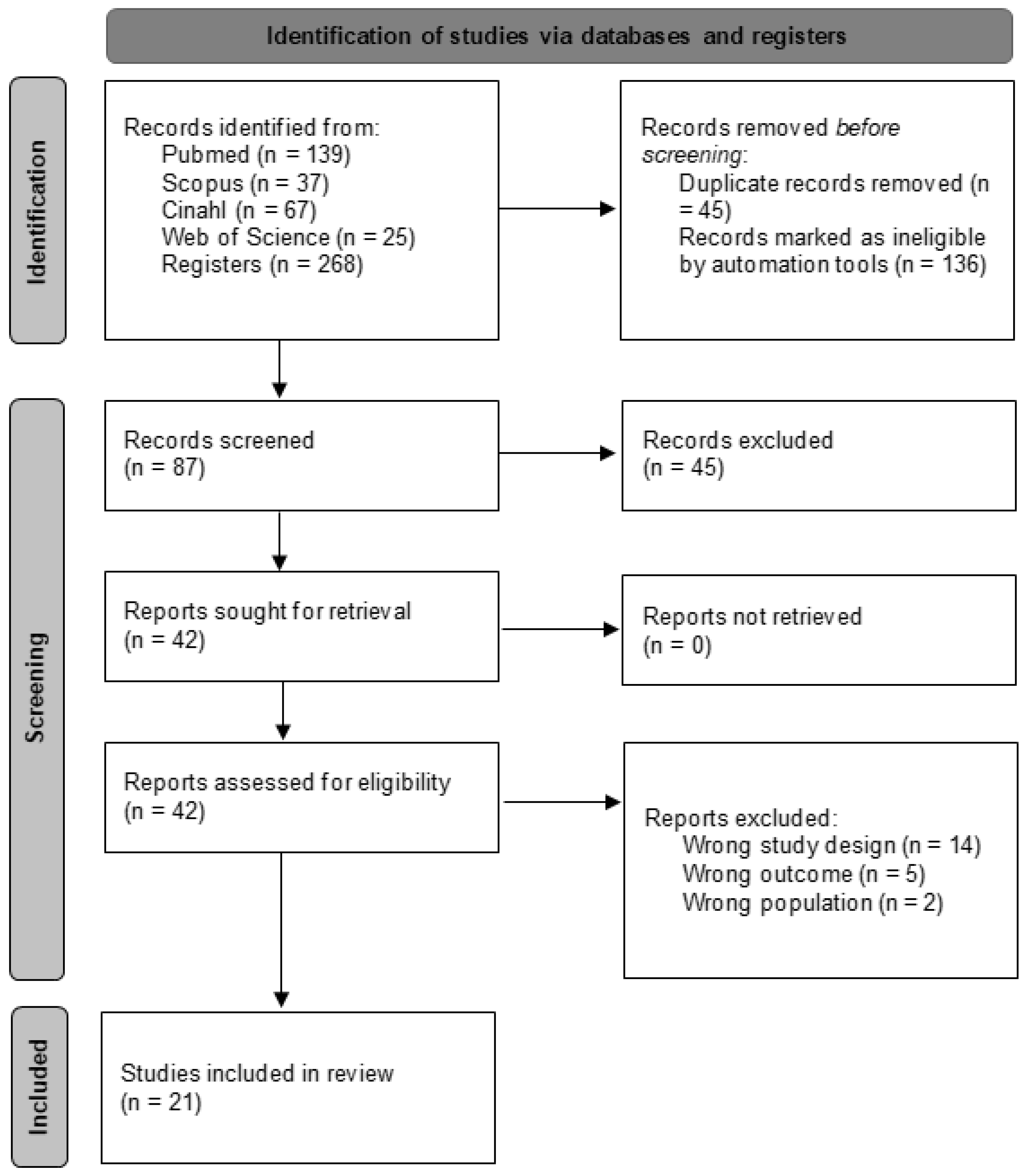
2.5. Study Selection Process
2.6. Data Extraction
2.7. Assessment of Methodological Quality
2.8. Analytic Decisions for Meta-Analysis
3. Results
3.1. Study Selection Process
3.2. Methodological Quality
3.3. Characteristics of the Studies
3.4. Study Results
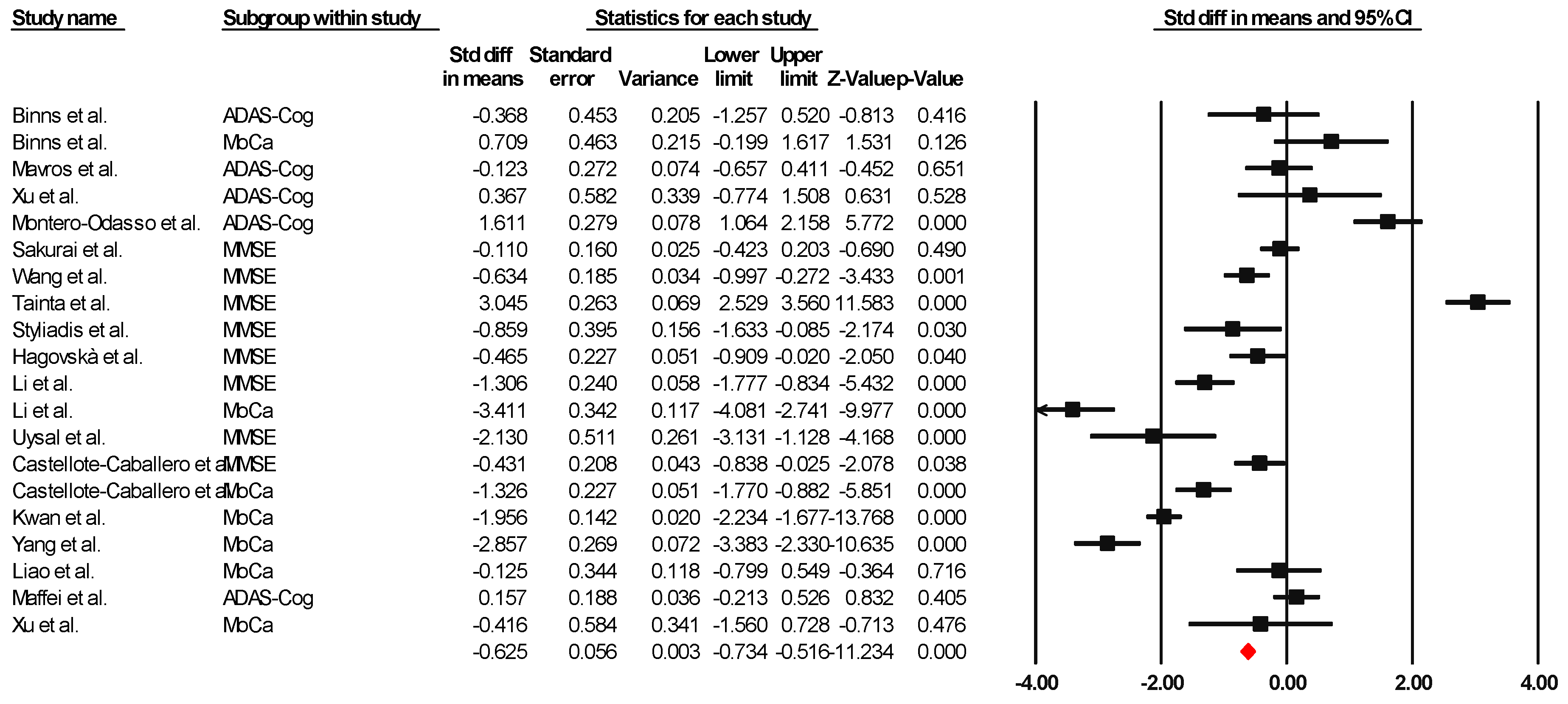
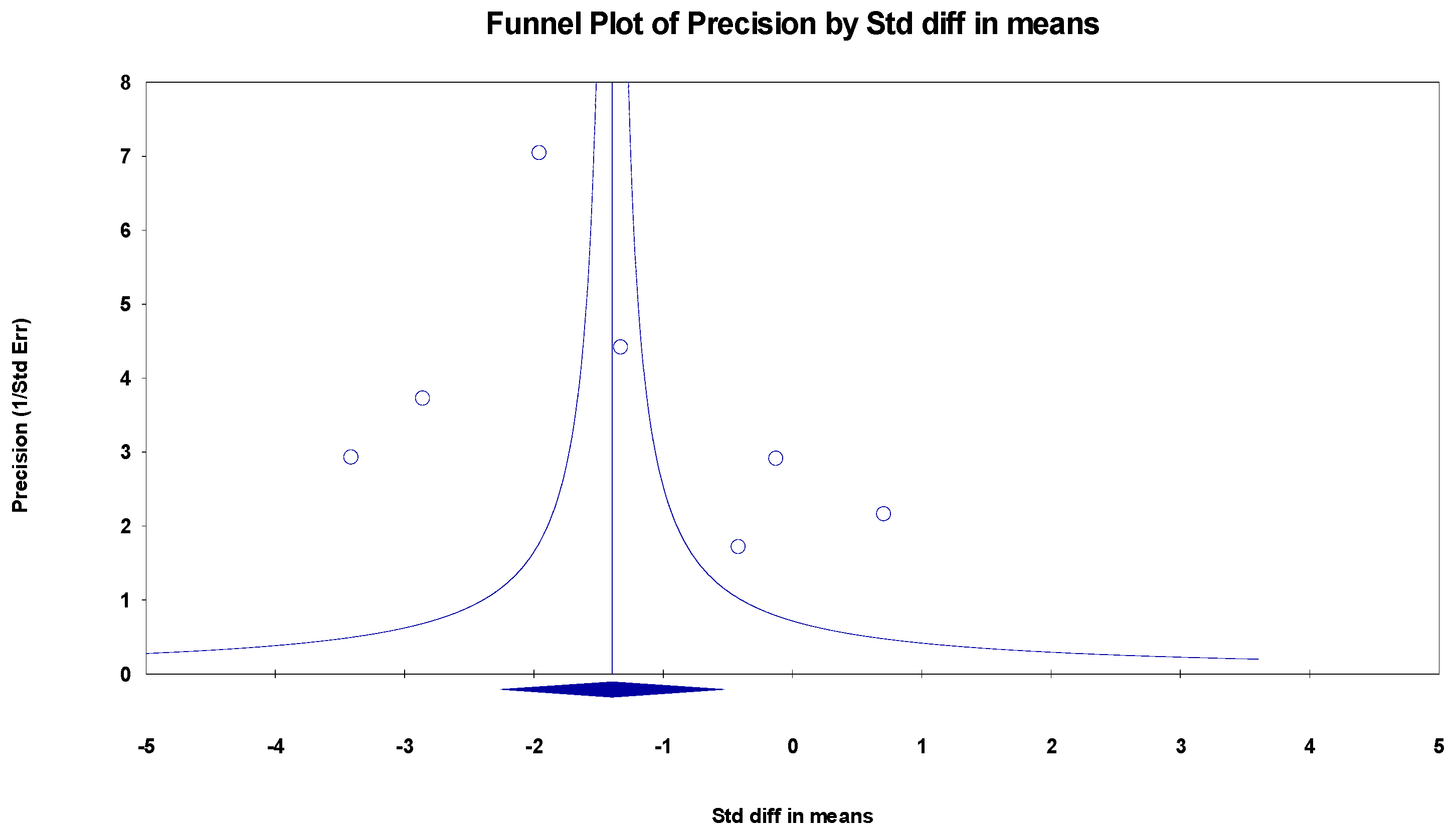
3.5. Meta-Analysis
3.5.1. Subgroup Analysis
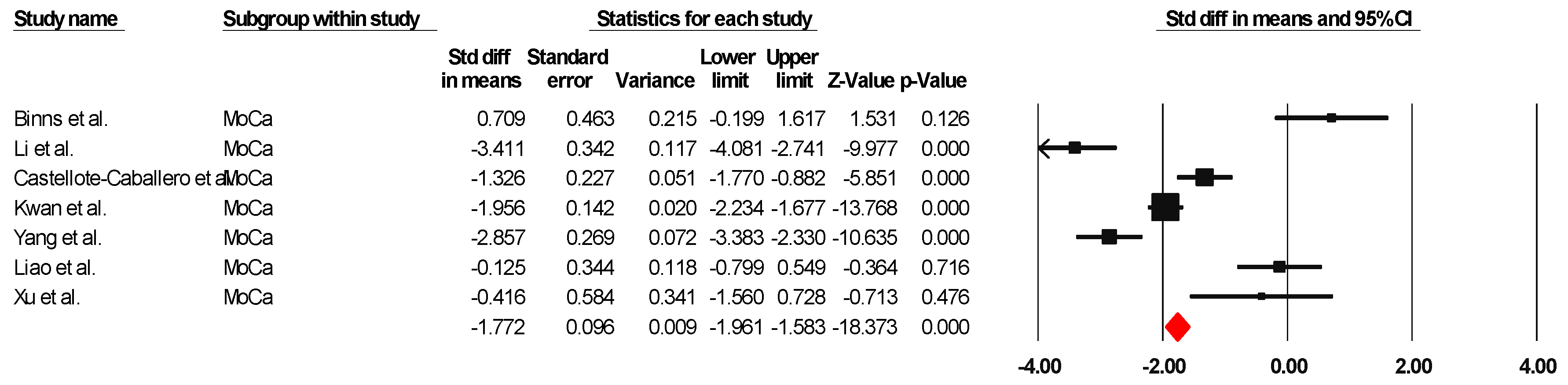
MoCa
MMSE
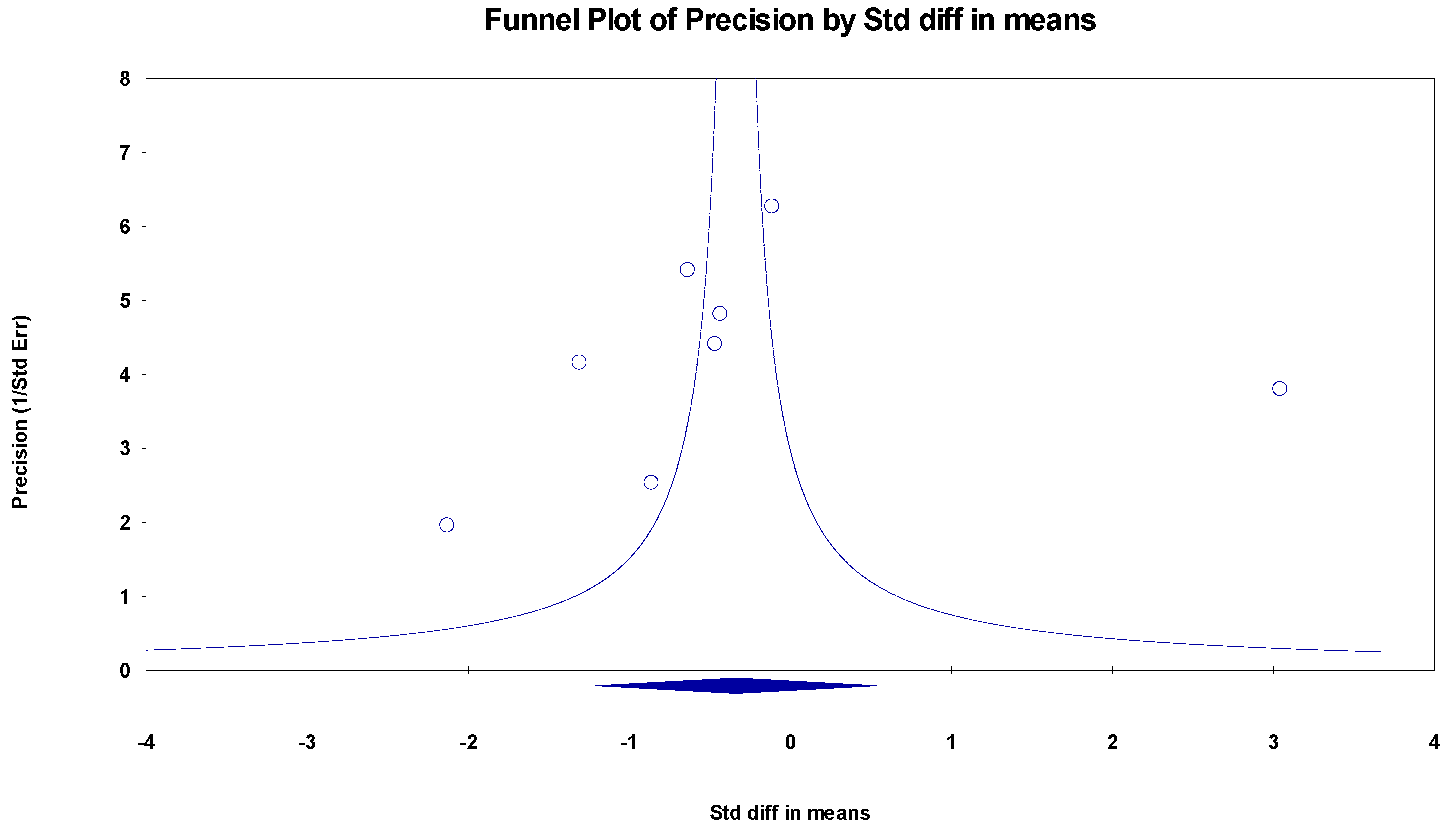
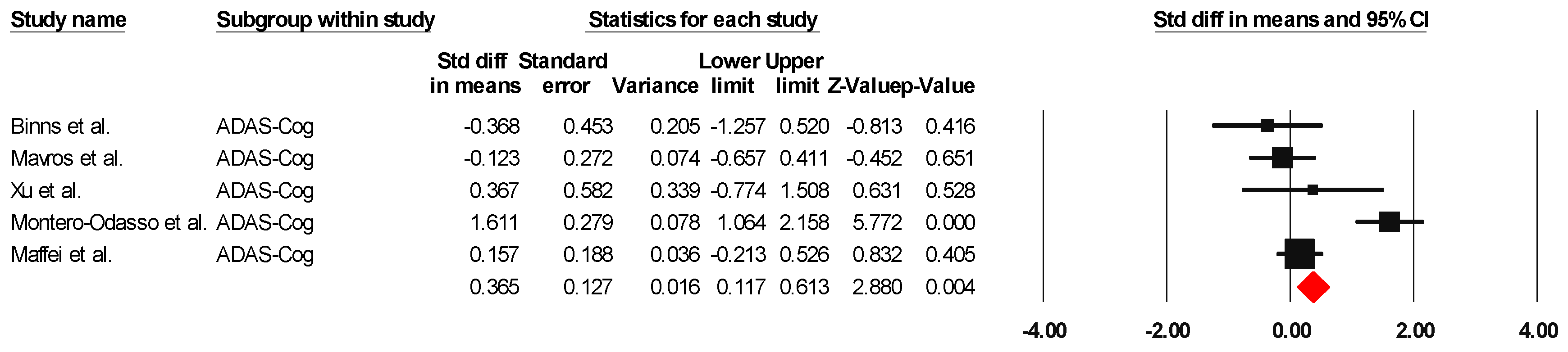
ADAS-Cog
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cahill, S. WHO’s global action plan on the public health response to dementia: Some challenges and opportunities. Aging Ment. Health 2020, 2, 197–199. [Google Scholar] [CrossRef]
- Roberts, R.; Knopman, D.S. Classification and epidemiology of MCI. Clin. Geriatr. Med. 2013, 29, 753–772. [Google Scholar] [CrossRef] [PubMed]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.O.; Nordberg, A.; Bäckman, L.; Albert, M.; Almkvist, O.; et al. Mild cognitive impairment--beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Aurtenetxe, S.; García-Pacios, J.; Del Río, D.; López, M.E.; Pineda-Pardo, J.A.; Marcos, A.; Delgado Losada, M.L.; López-Frutos, J.M.; Maestú, F. Interference Impacts Working Memory in Mild Cognitive Impairment. Front. Neurosci. 2016, 10, 443. [Google Scholar] [CrossRef]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Writing Group of Chinese Guidelines for Diagnosis and Treatment of Dementia and Cognitive Impairment, Chinese Medical Doctor Association Neurologist Branch Cognitive Disorders Professional, Committee. Chinese guidelines for diagnosis and treatment of dementia and cognitive impairment in 2018 (five): Diagnosis and treatment of mild cognitive impairment. Natl. Med. J. China 2018, 17, 1294–1301. [Google Scholar]
- Ishikawa, K.M.; Davis, J.; Chen, J.J.; Lim, E. The prevalence of mild cognitive impairment by aspects of social isolation. PLoS ONE 2022, 17, e0269795. [Google Scholar] [CrossRef]
- Franco-García, J.M.; Denche-Zamorano, Á.; Carlos-Vivas, J.; Castillo-Paredes, A.; Mendoza-Holgado, C.; Pérez-Gómez, J. Subjective Cognitive Impairment and Physical Activity: Investigating Risk Factors and Correlations among Older Adults in Spain. J. Funct. Morphol. Kinesiol. 2024, 9, 150. [Google Scholar] [CrossRef]
- Valenzuela, P.L.; Castillo-García, A.; Morales, J.S.; Izquierdo, M.; Serra-Rexach, J.A.; Santos-Lozano, A.; Lucia, A. Physical Exercise in the Oldest Old. Compr. Physiol. 2019, 9, 1281–1304. [Google Scholar]
- Lautenschlager, N.T.; Cox, K.L.; Flicker, L.; Foster, J.K.; Van Bockxmeer, F.M.; Xiao, J.; Greenop, K.R.; Almeida, O.P. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: A randomized trial. JAMA 2008, 300, 1027–1037. [Google Scholar] [CrossRef]
- Di Lorito, C.; Bosco, A.; Booth, V.; Goldberg, S.; Harwood, R.H.; Van der Wardt, V. Adherence to exercise interventions in older people with mild cognitive impairment and dementia: A systematic review and meta-analysis. Prev. Med. Rep. 2020, 19, 101139. [Google Scholar] [CrossRef] [PubMed]
- Gates, N.J.; Rutjes, A.W.; Di Nisio, M.; Karim, S.; Chong, L.Y.; March, E.; Martínez, G.; Vernooij, R.W. Computerised cognitive training for maintaining cognitive function in cognitively healthy people in late life. Cochrane Database Syst. Rev. 2019, 3, CD012277. [Google Scholar] [CrossRef] [PubMed]
- Yeo, H.; Yoon, S.; Lee, J.; Kurtz, M.M.; Choi, K. A meta-analysis of the effects of social-cognitive training in schizophrenia: The role of treatment characteristics and study quality. Br. J. Clin. Psychol. 2021, 61, 1. [Google Scholar] [CrossRef] [PubMed]
- Bherer, L.; Gagnon, C.; Langeard, A.; Lussier, M.; Desjardins-Crépeau, L.; Berryman, N.; Bosquet, L.; Vu, T.T.M.; Fraser, S.; Li, K.Z.H.; et al. Synergistic Effects of Cognitive Training and Physical Exercise on Dual-Task Performance in Older Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 1533–1541. [Google Scholar] [CrossRef]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Rieker, J.A.; Reales, J.M.; Muiños, M.; Ballesteros, S. The Effects of Combined Cognitive-Physical Interventions on Cognitive Functioning in Healthy Older Adults: A Systematic Review and Multilevel Meta-Analysis. Front. Hum. Neurosci. 2022, 16, 838968. [Google Scholar] [CrossRef]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- Goetz, L.H.; Schork, N.J. Personalized medicine: Motivation, challenges, and progress. Fertil. Steril. 2018, 109, 952–963. [Google Scholar] [CrossRef]
- Sanjuán, M.; Navarro, E.; Calero, M.D. Effectiveness of Cognitive Interventions in Older Adults: A Review. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 876–898. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, P.J. Improving health literacy using the power of digital communications to achieve better health outcomes for patients and practitioners. Front. Digit. Health 2023, 5, 1264780. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Gildengers, A.G.; Butters, M.A. Physical activity and brain plasticity in late adulthood. Dialogues Clin. Neurosci. 2013, 15, 99–108. [Google Scholar] [CrossRef]
- Stern, Y.; Arenaza-Urquijo, E.M.; Bartrés-Faz, D.; Belleville, S.; Cantilon, M.; Chetelat, G.; Ewers, M.; Franzmeier, N.; Kempermann, G.; Kremen, W.S.; et al. The Reserve, Resilience and Protective Factors PIA Empirical Definitions and Conceptual Frameworks Workgroup. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement. 2020, 16, 1305–1311. [Google Scholar] [CrossRef]
- Song, D.; Yu, D.S.F. Effects of a moderate-intensity aerobic exercise programme on the cognitive function and quality of life of community-dwelling elderly people with mild cognitive impairment: A randomised controlled trial. Int. J. Nurs. Stud. 2019, 9, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.Y.; Ku, Y.; Zanto, T.P.; Gazzaley, A. Effects of noninvasive brain stimulation on cognitive function in healthy aging and Alzheimer’s disease: A systematic review and meta-analysis. Neurobiol. Aging 2015, 36, 2348–2359. [Google Scholar] [CrossRef]
- Jacova, C.; Kertesz, A.; Blair, M.; Fisk, J.D.; Feldman, H.H. Neuropsychological testing and assessment for dementia. Alzheimers Dement. 2007, 3, 299–317. [Google Scholar] [CrossRef]
- Zhu, X.; Yin, S.; Lang, M.; He, R.; Li, J. The more the better? A meta-analysis on effects of combined cognitive and physical intervention on cognition in healthy older adults. Ageing Res. Rev. 2016, 31, 67–79. [Google Scholar] [CrossRef]
- Gavelin, H.M.; Dong, C.; Minkov, R.; Bahar-Fuchs, A.; Ellis, K.A.; Lautenschlager, N.T.; Mellow, M.L.; Wade, A.T.; Smith, A.E.; Finke, C.; et al. Combined physical and cognitive training for older adults with and without cognitive impairment: A systematic review and network meta-analysis of randomized controlled trials. Ageing Res. Rev. 2021, 66, 101232. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The prisma 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023); Cochrane: London, UK, 2023; Available online: www.training.cochrane.org/handbook (accessed on 22 November 2023).
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy evidence database (pedro) scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Binns, E.; Kerse, N.; Peri, K.; Cheung, G.; Taylor, D. Combining cognitive stimulation therapy and fall prevention exercise (CogEx) in older adults with mild to moderate dementia: A feasibility randomised controlled trial. Pilot Feasibility Stud. 2020, 25, 6. [Google Scholar] [CrossRef]
- Train the Brain Consortium. Randomized trial on the effects of a combined physical/cognitive training in aged MCI subjects: The Train the Brain study. Sci. Rep. 2017, 7, 39471. [Google Scholar]
- Bray, N.W.; Pieruccini-Faria, F.; Witt, S.T.; Bartha, R.; Doherty, T.J.; Nagamatsu, L.S.; Almeida, Q.J.; Liu-Ambrose, T.; Middleton, L.E.; Bherer, L.; et al. Combining exercise with cognitive training and vitamin D3 to improve functional brain connectivity (FBC) in older adults with mild cognitive impairment (MCI). Results from the SYNERGIC trial. Geroscience 2023, 45, 1967–1985. [Google Scholar] [CrossRef]
- Castellote-Caballero, Y.; del Carmen Carcelén Fraile, M.; Aibar-Almazán, A.; Afanador-Restrepo, D.F.; González-Martín, A.M. Effect of combined physical–cognitive training on the functional and cognitive capacity of older people with mild cognitive impairment: A randomized controlled trial. BMC Med. 2024, 22, 281. [Google Scholar] [CrossRef] [PubMed]
- Damirchi, A.; Hosseini, F.; Babaei, P. Mental Training Enhances Cognitive Function and BDNF More Than Either Physical or Combined Training in Elderly Women With MCI: A Small-Scale Study. Am. J. Alzheimer’s Dis. Other Demen. 2018, 33, 20–29. [Google Scholar] [CrossRef]
- Liao, Y.Y.; Hsuan Chen, I.; Lin, Y.J.; Chen, Y.; Hsu, W.C. Effects of virtual reality-based physical and cognitive training on executive function and dual-task gait performance in older adults with mild cognitive impairment: A randomized control trial. Front. Aging Neurosci. 2019, 11, 162. [Google Scholar] [CrossRef]
- Sakurai, T.; Sugimoto, T.; Akatsu, H.; Doi, T.; Fujiwara, Y.; Hirakawa, A.; Kinoshita, F.; Kuzuya, M.; Lee, S.; Matsumoto, N.; et al. Japan-Multimodal Intervention Trial for the Prevention of Dementia: A randomized controlled trial. Alzheimer’s Dement. 2024, 20, 3918–3930. [Google Scholar] [CrossRef]
- Wang, P.; Yang, T.; Peng, W.; Wang, M.; Chen, X.; Yang, Y.; Huang, Y.; Jiang, Y.; Wang, F.; Sun, S.; et al. Effects of a Multicomponent Intervention With Cognitive Training and Lifestyle Guidance for Older Adults at Risk of Dementia: A Randomized Controlled Trial. J. Clin. Psychiatry 2024, 85, 23. [Google Scholar] [CrossRef] [PubMed]
- Kwan, R.Y.C.; Liu, J.; Sin, O.S.K.; Fong, K.N.; Qin, J.; Wong, J.C.Y.; Lai, C. Effects of Virtual Reality Motor-Cognitive Training for Older People with Cognitive Frailty: Multicentered Randomized Controlled Trial. J. Med. Internet Res. 2024, 26, e57809. [Google Scholar] [CrossRef]
- Tainta, M.; Ecay-Torres, M.; de Arriba, M.; Barandiaran, M.; Otaegui-Arrazola, A.; Iriondo, A.; Garcia-Sebastian, M.; Estanga, A.; Saldias, J.; Clerigue, M.; et al. GOIZ ZAINDU study: A FINGER-like multidomain lifestyle intervention feasibility randomized trial to prevent dementia in Southern Europe. Alzheimers Res. Ther. 2024, 16, 44. [Google Scholar]
- Styliadis, C.; Kartsidis, P.; Paraskevopoulos, E.; Ioannides, A.A.; Bamidis, P.D. Neuroplastic effects of combined computerized physical and cognitive training in elderly individuals at risk for dementia: An eLORETA controlled study on resting states. Neural Plast. 2015, 2015, 172192. [Google Scholar] [PubMed]
- Yang, Q.H.; Lyu, X.; Lin, Q.R.; Wang, Z.W.; Tang, L.; Zhao, Y.; Lyu, Q.Y. Effects of a multicomponent intervention to slow mild cognitive impairment progression: A randomized controlled trial. Int. J. Nurs. Stud. 2022, 125, 104110. [Google Scholar] [PubMed]
- Hagovská, M.; Olekszyová, Z. Impact of the combination of cognitive and balance training on gait, fear and risk of falling and quality of life in seniors with mild cognitive impairment. Geriatr. Gerontol. Int. 2016, 16, 1043–1050. [Google Scholar] [CrossRef]
- Mavros, Y.; Gates, N.; Wilson, G.C.; Jain, N.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. Mediation of Cognitive Function Improvements by Strength Gains After Resistance Training in Older Adults with Mild Cognitive Impairment: Outcomes of the Study of Mental and Resistance Training. J. Am. Geriatr. Soc. 2017, 65, 550–559. [Google Scholar]
- Xu, Z.; Zhang, D.; Lee, A.T.; Sit, R.W.; Wong, C.; Lee, E.K.; Yip, B.H.; Tiu, J.Y.; Lam, L.C.; Wong, S.Y.; et al. A pilot feasibility randomized controlled trial on combining mind-body physical exercise, cognitive training, and nurse-led risk factor modification to reduce cognitive decline among older adults with mild cognitive impairment in primary care. PeerJ 2020, 8, e9845. [Google Scholar] [CrossRef]
- Li, L.; Liu, M.; Zeng, H.; Pan, L. Multi-component exercise training improves the physical and cognitive function of the elderly with mild cognitive impairment: A six-month randomized controlled trial. Ann. Palliat. Med. 2021, 10, 8919–8929. [Google Scholar] [CrossRef]
- Uysal, İ.; Başar, S.; Aysel, S.; Kalafat, D.; Büyüksünnetçi, A.Ö. Aerobic exercise and dual-task training combination is the best combination for improving cognitive status, mobility and physical performance in older adults with mild cognitive impairment. Aging Clin. Exp. Res. 2023, 35, 271–281. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Zou, G.; Speechley, M.; Almeida, Q.J.; Liu-Ambrose, T.; Middleton, L.E.; Camicioli, R.; Bray, N.W.; Li, K.Z.; Fraser, S.; et al. Effects of Exercise Alone or Combined with Cognitive Training and Vitamin D Supplementation to Improve Cognition in Adults with Mild Cognitive Impairment: A Randomized Clinical Trial. JAMA Netw. Open 2023, 6, E2324465. [Google Scholar] [CrossRef]
- Fairchild, J.K.; Myers, J.; Louras, P.; Jo, B.; McNerney, M.W.; Hallmayer, J.; Yesavage, J. Multimodal Exercise and Cognitive Training Program Improves Cognitive Function in Amnestic Mild Cognitive Impairment. Am. J. Geriatr. Psychiatry 2024, 32, 463–474. [Google Scholar] [CrossRef]
- Lipardo, D.S.; Tsang, W.W.N. Effects of combined physical and cognitive training on fall prevention and risk reduction in older persons with mild cognitive impairment: A randomized controlled study. Clin. Rehabil. 2020, 34, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.Y.; Tseng, H.Y.; Lin, Y.J.; Wang, C.J.; Hsu, W.C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 2020, 56, 47–57. [Google Scholar] [CrossRef]
- Savović, J.; Jones, H.E.; Altman, D.G.; Harris, R.J.; Jüni, P.; Pildal, J.; Als-Nielsen, B.; Balk, E.M.; Gluud, C.; Gluud, L.L.; et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Ann. Intern. Med. 2012, 157, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Falck, R.S.; David, J.C.; Best, J.R.; Crockett, R.A.; Liu-Ambrose, T. Impact of exercise training on physical and cognitive function among older adults: A systematic review and meta-analysis. Neurobiol. Aging 2019, 79, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Gates, N.; Singh, M.A.F.; Sachdev, P.S.; Valenzuela, M. The effect of exercise training on cognitive function in older adults with mild cognitive impairment: A meta-analysis of randomized controlled trials. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2013, 21, 1086–1097. [Google Scholar] [CrossRef]
- Law, C.; Lam, F.M.H.; Chung, R.C.K.; Pang, M.Y.C. Physical exercise attenuates cognitive decline and reduces behavioural problems in people with mild cognitive impairment and dementia: A systematic review. J. Physiother. 2020, 66, 9–18. [Google Scholar] [CrossRef]
- Sanders, L.M.J.; Hortobágyi, T.; la Bastide-van Gemert, S.; van der Zee, E.A.; van Heuvelen, M.J.G. Dose-response relationship between exercise and cognitive function in older adults with and without cognitive impairment: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0210036. [Google Scholar] [CrossRef]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef]
- Öhman, H.; Savikko, N.; Strandberg, T.E.; Pitkälä, K.H. Effect of physical exercise on cognitive performance in older adults with mild cognitive impairment or dementia: A systematic review. Dement. Geriatr. Cogn. Disord. 2014, 38, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Ströhle, A.; Schmidt, D.K.; Schultz, F.; Fricke, N.; Staden, T.; Hellweg, R.; Priller, J.; Rapp, M.A.; Rieckmann, N. Drug and exercise treatment of alzheimer disease and mild cognitive impairment: A systematic review and meta-analysis of effects on cognition in randomized controlled trials. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2015, 23, 1234–1249. [Google Scholar] [CrossRef]
- Song, D.; Yu, D.S.F.; Li, P.W.C.; Lei, Y. The effectiveness of physical exercise on cognitive and psychological outcomes in individuals with mild cognitive impairment: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2018, 79, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Silva, T.B.L.D.; Santos, G.D.; Moreira, A.P.B.; Ishibashi, G.A.; Verga, C.E.R.; Moraes, L.C.D.; Lessa, P.P.; Cardoso, N.P.; Ordonez, T.N.; Brucki, S.M.D. Cognitive interventions in mature and older adults, benefits for psychological well-being and quality of life: A systematic review study. Dement. Neuropsychol. 2021, 15, 428–439. [Google Scholar] [CrossRef] [PubMed]
- Lam, L.C.; Chau, R.C.; Wong, B.M.; Fung, A.W.; Tam, C.W.; Leung, G.T.; Kwok, T.C.; Leung, T.Y.; Ng, S.P.; Chan, W.M. A 1-year randomized controlled trial comparing mind body exercise (Tai Chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J. Am. Med. Dir. Assoc. 2012, 13, 568.e15–568.e20. [Google Scholar] [CrossRef]
- Sungkarat, S.; Boripuntakul, S.; Chattipakorn, N.; Watcharasaksilp, K.; Lord, S.R. Effects of Tai Chi on Cognition and Fall Risk in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2017, 65, 721–727. [Google Scholar] [CrossRef]
- Wei, Z.; Zhao, X.; Liu, Y. A meta-analysis of the consequences of cognitive training on the cognitive function of aged mild cognitive impairment patients. Psychogeriatrics 2024, 24, 1371–1388. [Google Scholar] [CrossRef]
- Lampit, A.; Hallock, H.; Valenzuela, M. Computerized cognitive training in cognitively healthy older adults: A systematic review and meta-analysis of effect modifiers. PLoS Med. 2014, 11, e1001756. [Google Scholar] [CrossRef]
- Chen, X.; Maguire, B.; Brodaty, H.; O’Leary, F. Dietary Patterns and Cognitive Health in Older Adults: A Systematic Review. J. Alzheimer’s Dis. 2019, 67, 583–619. [Google Scholar] [CrossRef]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Izquierdo, M. Role of physical exercise on cognitive function in healthy older adults: A systematic review of randomized clinical trials. Ageing Res. Rev. 2017, 37, 117–134. [Google Scholar] [CrossRef]
- Guo, W.; Zang, M.; Klich, S.; Kawczyński, A.; Smoter, M.; Wang, B. Effect of Combined Physical and Cognitive Interventions on Executive Functions in OLDER Adults: A Meta-Analysis of Outcomes. Int. J. Environ. Res. Public Health 2020, 17, 6166. [Google Scholar] [CrossRef] [PubMed]
- Stillman, C.M.; Cohen, J.; Lehman, M.E.; Erickson, K.I. Mediators of Physical Activity on Neurocognitive Function: A Review at Multiple Levels of Analysis. Front. Hum. Neurosci. 2016, 10, 626. [Google Scholar] [CrossRef] [PubMed]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of combined physical and cognitive training on cognition: A systematic review. BMC Geriatr. 2016, 18, 141. [Google Scholar] [CrossRef] [PubMed]
- Castaño, L.A.A.; Castillo de Lima, V.; Barbieri, J.F.; de Lucena, E.G.P.; Gáspari, A.F.; Arai, H.; Teixeira, C.V.L.; Coelho-Júnior, H.J.; Uchida, M.C. Resistance Training Combined With Cognitive Training Increases Brain Derived Neurotrophic Factor and Improves Cognitive Function in Healthy Older Adults. Front. Psychol. 2022, 13, 870561. [Google Scholar] [CrossRef]
- Aminirakan, D.; Losekamm, B.; Wollesen, B. Effects of combined cognitive and resistance training on physical and cognitive performance and psychosocial well-being of older adults ≥65: Study protocol for a randomised controlled trial. BMJ Open 2024, 14, e082192. [Google Scholar] [CrossRef]
- Karssemeijer, E.G.A.; Aaronson, J.A.; Bossers, W.J.; Smits, T.; Olde Rikkert, M.G.M.; Kessels, R.P.C. Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res. Rev. 2017, 40, 75–83. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Binns et al. [35] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7 |
| Maffei et al. [36] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Bray et al. [37] | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 6 |
| Castellote-Caballero et al. [38] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Damirchi et al. [39] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 |
| Liao et al. [40] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 6 |
| Sakurai et al. [41] | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 6 |
| Wang et al. [42] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Kwan et al. [43] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Tainta et al. [44] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 8 |
| Styliadis et al. [45] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Yang et al. [46] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Hagovská et al. [47] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 8 |
| Mavros et al. [48] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Xu et al. [49] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7 |
| Li et al. [50] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7 |
| Uysal et al. [51] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
| Montero-Odasso et al. [52] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 8 |
| Fairchild et al. [53] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 7 |
| Lipardo et al. [54] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 7 |
| Liao et al. [55] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 6 |
| Author and Year | Sex | Sample CG/IG | Control Group | Intervention Group | |||
|---|---|---|---|---|---|---|---|
| Age | Treatment | Exercise Parameters | Results | ||||
| Binns et al. [35] | F: 74.5% M: 25.5% | 9/11 | Cognitive stimulation therapy | 85.6 | Cognitive therapy Aerobics Strength Balance | F: 2 times/week #S: 14 sessions D: 60 min | Thirty-six residents were screened, with twenty-three participants randomized to intervention (CogEx, n = 10) or control (CST, n = 13) groups. The assessments took 45 min to 1.5 h, and there was repetition between the two cognitive measures. Ten facilitators completed training with the manualized program. Exercises were combined into an hour-long CST session; however, limited balance training occurred, with participants exercising predominantly in sitting positions. The facilitators felt the participants engaged more and were safer sitting. |
| Maffei et al. [36] | F: 47.8% M: 52.2% | 58/55 | Usual life routine | 74.5 ± 4.6 | Cognitive training Physical exercise Music therapy | F: 3 times/week #S: 84 sessions D: 60 min | The significant beneficial effect of combined training on the ADAS-Cog was detected (p = 0.007) in the MCI-training group and (p = 0.026) in the MCI-no training group. The difference between groups was statistically significant (p < 0.0001); training increased parahippocampal CBF, but no effect on GM volume loss was evident. Increased BOLD activity, indicative of decreased neuronal efficiency, was found only in untrained MCI subjects. |
| Bray et al. [37] | F: 47.8% M: 52.2% | 17/73 | Physical exercise control Cognitive training control Vitamin D control | 73.9 ± 6.5 | Physical exercise Cognitive training Vitamin D | F: 3 times/week #S: 60 sessions D: 90 min | In the FBC region of interest, there was a significant between-arm difference in T0 Salience Network connectivity in model four. The intervention arm demonstrated a significant between-arm increase (T6–T0) in connectivity for a single cluster in model four (p-FDR < 0.05). On the right hippocampus, intervention arms demonstrated a significant between-arm increase (T6–T0) in model one (p-FDR < 0.01 and <0.05), two (p-FDR = <0.001), and four (p-FDR = <0.01). On the left hippocampus, there was a significant between-arm difference in connectivity with the left inferior frontal and precentral gyrus at T0 in model four. The intervention arm demonstrated a significant between-arm increase (T6–T0) in only model four (p-FDR < 0.01). |
| Castellote-Caballero et al. [38] | F: 77.7% M: 22.3% | 47/48 | Cognitive stimulation | 72.1 ± 4.25 | Cognitive stimulation Psychomotor sessions | F: 2 times/week #S: 24 sessions D: 45–50 min | The results show significant improvements in both aspects, such as balance (p = 0.035), gait (p = 0.001), upper and lower body strength (p = 0.000 and p = 0.001), flexibility (p = 0.000), physical function (p = 0.001), cognitive function (p = 0.041), cognitive impairment (p = 0.000), verbal fluency (p = 0.000), and executive functions (p = 0.000) in the group that carried out the intervention compared with the control group. |
| Damirchi et al. [39] | F: 100% | 9/35 | Waitlist | 68.4 | Physical training Mental training Combined training | F: 3 times/week #S: 24 sessions D: 30–60 min | Analysis of variance with Tukey post hoc test revealed a significant increase in working memory (p = 0.012) and brain-derived neurotrophic factor (p = 0.024) in the ME group compared with the control group. Furthermore, compared with the physical training group, the ME group demonstrated better working memory (p = 0.014) and processing speed (p = 0.024). |
| Liao et al. [40] | F: 67.7% M: 32.3% | 16/18 | Combined physical and cognitive training | 74.3 | VR-combined physical and cognitive training | F: 3 times/week #S: 36 sessions D: 30–60 min | Both groups significantly improved in the SCWT and the single-task and motor dual-task gait performance measures. However, only the VR group showed improvements in cognitive dual-task gait performance and the DTC of cadence. Moreover, the VR group showed more improvements than the CPC group in the TMT-B and DTC of cadence with borderline significance. |
| Sakurai et al. [41] | F: 52% M: 48% | 218/215 | General health-related information | 74.4 | Management of vascular risk factors Exercise Nutritional counseling Cognitive training | F: 1 time/week #S: 78 sessions D: 90 min | The between-group difference in composite score changes was 0.047 (95% CI: −0.029 to 0.124) for cognitive tests. Secondary analyses indicated positive impacts of interventions on several secondary health outcomes. The interventions appeared to be particularly effective for individuals with high attendance during exercise sessions and those with the apolipoprotein E ε4 allele and elevated plasma glial fibrillary acidic protein levels. |
| Wang et al. [42] | F: 60% M: 40% | 61/62 | Routine health education program | 67.1 | Cognitive training (mnemonic strategy training) Lifestyle guidance intervention (diet, sleep, and exercise guidance) | F: 5 times/week #S: 45 sessions D: 20–90 min | For cognitive outcomes, the linear mixed-effect model results showed significant time × group effects in the MMSE (Cohen d = 0.63 [95% CI, 0.27 to 1.00], F = 10.25, p = 0.002). This study found significant time × group effects in AVLT-immediate (Cohen d = 0.47 [95% CI, 0.11 to 0.83], F = 8.18, p = 0.005), AVLT-delayed (Cohen d = 0.45 [95% CI, 0.10 to 0.81], F = 4.59, p = 0.034), LMT-delayed (Cohen d = 0.71 [95% CI, 0.34 to 1.07], F = 4.59, p = 0.034), DSST (Cohen d = 0.27 [95% CI, −0.08 to 0.63], F = 4.83, p = 0.030), and DST (Cohen d = 0.69 [95% CI, 0.33 to 1.05], F = 8.58, p = 0.004). |
| Kwan et al. [43] | F: 78.2% M: 22.8% | 147/146 | Usual care | 74.5 ± 6.8 | VR motor–cognitive training (VRMCT) | F: 2 times/week #S: 16 sessions D: 60 min | VRMCT was effective in promoting global cognitive function (interaction effect: p = 0.03), marginally promoting executive function (interaction effect: p = 0.07), and reducing frailty (interaction effect: p = 0.03). The effects were not statistically significant on other outcomes. |
| Tainta et al. [44] | F: 58% M: 42% | 64/61 | Regular health advice | 75.6 ± 6.5 | Cardiovascular risk factor monitoring Nutritional workshops Cognitive stimulation and training Physical exercise | F: 3 times/week #S: 144 sessions D: 90 min | More than 70% of the participants had high overall adherence to the intervention activities. The risk of cognitive decline was higher in the RHA group than in the MD-Int group in terms of executive function (p = 0.019) and processing speed scores (p = 0.026). |
| Styliadis et al. [45] | F: 64.3% M: 35.7% | 28/42 | Active control group (training protocol consisting of watching a documentary and answering a questionnaire) Passive control group (participants did not engage in any activity) | 70.8 ± 5.7 | Combined physical and cognitive training | F: 5 times/week #S: 40 sessions D: 60 min | A significant training effect was identified only after the combined training scheme: a decrease in the post- compared with the pre-training activity of the precuneus/posterior cingulate cortex in delta, theta, and beta bands. This effect was correlated to improvements in cognitive capacity as evaluated by MMSE scores [(score difference in delta (p = 0.043) and theta bands (p = 0.015)]. The results indicate this type of training shows indices of a positive neuroplastic effect in MCI patients and that EEG may serve as an index of gains versus cognitive declines and neurodegeneration. |
| Yang et al. [46] | F: 52.7% M: 47.3% | 57/55 | Usual care | 70.2 ± 6.0 | Dietary intervention Physical training Cognitive training Monitoring of metabolic indicators and vascular risk factors | F: 2 times/week #S: 47 sessions D: 60–90 min | At baseline, clinical characteristics did not differ significantly between groups. Significant interaction effects between time and group were detected (p < 0.001), indicating that the scores of five outcomes (cognitive function, short physical performance battery, Timed Up and Go Test, quality of life, and depression) of the intervention and control groups changed differently over time. Participants in the intervention group had a significantly greater improvement in cognitive function, physical function, and quality of life and fewer depression symptoms compared with the control group at baseline and follow-up periods. |
| Hagovskà et al. [47] | F: 48.7% M: 51.3% | 40/40 | Balance training | 67.1 | CogniPlus training program Balance training | F: 2 times/week #S: 20 sessions D: 30 min | The two groups showed significant differences recorded after training in the Mini-Mental State Examination. Before the training, there were no significant differences recorded between the groups in global cognitive functions as assessed by the MMSE. After the training, there were significant differences in favor of the experimental group (p < 0.05). The Timed Up and Go Test with dual tasking, balanced by the Tinetti test, demonstrated the quality of life in favor of the experimental group (p < 0.03–0.001). There were no significant differences between the groups in assessing fear of falling or other monitored parameters. |
| Mavros et al. [48] | F: 68% M: 32% | 27/73 | Sham cognitive training Sham progressive resistance training | Aged ≥ 55 | Cognitive training Progressive resistance training | F: 3 to 2 times/week #S: 58 sessions D: 60–100 min | PRT increased upper (standardized mean difference (SMD) = 0.69, 95% confidence interval = 0.47, 0.91), lower (SMD = 0.94, 95% CI = 0.69–1.20), and whole-body (SMD = 0.84, 95% CI = 0.62–1.05) strength, and percentage change in VO2peak (8.0%, 95% CI = 2.2–13.8) was significantly higher than sham exercise. Higher strength scores, but not greater VO2peak, were significantly associated with improvements in cognition (p < 0.05). Greater lower body strength significantly mediated the effect of PRT on ADAS-Cog improvements (indirect effect: b = 0.64, 95% CI = 1.38 to 0.004; direct effect: b = 0.37, 95% CI = 1.51–0.78) and global domain (indirect effect: b = 0.12, 95% CI = 0.02–0.22; direct effect: b = 0.003, 95% CI = 0.17–0.16) but not for the executive domain (indirect effect: b = 0.11, 95% CI = 0.04–0.26; direct effect: b = 0.03, 95% CI = 0.17–0.23). |
| Xu et al. [49] | F: 73.3% M: 26.3% | 6/13 | Health advice | 74 ± 5.2 | Cognitive training Mind–body physical exercise Nurse-led risk factor modification | F: 3 times/week #S: 36 sessions D: 30 min | Significant within-group changes were observed in HK-MoCA in RFM (4.50 ± 2.59, p = 0.008), cost of health service utilization in CPR (−4000, quartiles: −6800 to −200, p = 0.043), fish and seafood in HA (−1.10 ± 1.02, p = 0.047), and sugar in HA (2.69 ± 1.80, p = 0.015). Group × time interactions were noted in HK-MoCA favoring the RFM group (p = 0.000), DAD score favoring the CPR group (p = 0.027), GAS-20 favoring the CPR group (p = 0.026), number of servings of fish and seafood (p = 0.004), and sugar (p < 0.001) eaten per day. |
| Li et al. [50] | F: 60.7% M: 39.3% | 42/42 | General community health instruction | 71.1 | Aerobic training Strength training Balance training Coordination training Sensitivity training | F: 5 times/week #S: 120 sessions D: 30 min | The average CM-PPT score increased from 11.36 ± 2.69 to 11.88 ± 2.40 and 12.83 ± 2.19 in 3 and 6 months, respectively, after the intervention, while the control group showed a decrease from 10.79 ± 2.73 to 10.24 ± 2.62 in 3 months and 9.21 ± 2.09 in 6 months. CM-PPT scores with the main intervention effect and the interaction between intervention and time were both statistically significant (p < 0.05), indicating that the physical functions of participants with MCI were improved after intervention. The average MoCA score increased from 21.52 ± 2.05 to 23.48 ± 1.47 (3 months) and 25.19 ± 1.29 (6 months) after intervention, while the control group showed a decrease from 21.14 ± 1.97 to 20.21 ± 1.88 and 19.45 ± 2.00 in 3 and 6 months. The MMSE score showed the same trend as the MoCA score. The MoCA score with the main intervention effect; the MMSE and MoCA scores with the effect of time; and the MMSE and MoCA scores with the interaction between the intervention and time were all statistically significant (p < 0.05), showing that the cognitive function of participants with MCI was improved by the intervention. |
| Uysal et al. [51] | F: 16.7% M: 83.3% | 12/36 | Exclusively lower extremity strengthening exercises | 73.7 | Aerobic exercise Dual-task training Lower extremity strengthening exercise | F: 3 times/week #S: 36 sessions D: 30 min | In all three intervention groups, there was a significant improvement in cognitive status, balance, mobility, activity-specific balance confidence, physical performance, mood, and quality of life (p < 0.05). The most remarkable change was observed in the ADG regarding cognitive status, mobility, and physical performance parameters (p < 0.05). In addition, the most significant improvement in balance parameters was recorded both in the DG and ADG (p < 0.05). The highest increase in functional exercise capacity was detected both in the AG and the ADG (p < 0.05). Furthermore, both exercise combinations were superior to the control group in terms of improving mood and quality of life (p < 0.05). |
| Montero-Odasso et al. [52] | F: 49.1% M: 50.9% | 34/141 |
Balance–toning exercise Sham cognitive training Placebo vitamin D | 73.1 ± 6.6 | Aerobic and resistance training Cognitive training Vitamin D | F: 3 times/week #S: 60 sessions D: 90 min | At 6 months, all active arms (i.e., arms 1 through 4) with aerobic–resistance exercise, regardless of the addition of cognitive training or vitamin D, improved ADAS-Cog-13 compared with the control (mean difference, −1.79 points; 95% CI, −3.27 to −0.31 points; p = 0.02; d = 0.64). Compared with exercise alone (arms 3 and 4), exercise and cognitive training (arms 1 and 2) improved the ADAS-Cog-13 score (mean difference, −1.45 points; 95% CI, −2.70 to −0.21 points; p = 0.02; d = 0.39). No significant improvement was found with vitamin D. Finally, the multidomain intervention (arm 1) improved the ADAS-Cog-13 score significantly compared with the control (mean difference, −2.64 points; 95% CI, −4.42 to −0.80 points; p = 0.005; d = 0.71). Changes in ADAS-Cog-Plus were not significant. |
| Fairchild et al. [53] | F: 4.2% M: 95.8% | 36/36 |
Stretching exercise Cognitive training | 72.4 ± 9.5 | Aerobic and resistance training Cognitive training | F: 3 times/week #S: 72 sessions D: 60 min | Controlling for age and employment status, linear mixed-effects models revealed that all participants experienced significant improvement in the delayed recall of a word list, learning and memory, and executive function. Only the CARE + CT condition significantly improved processing speed and functional capacity. APOE4 status impacted the cognitive benefits of those with the SE + CT condition. |
| Lipardo et al. [54] | F: 79% M: 21% | 23/69 | Waitlist | 69 ± 8.3 | Physical training Cognitive training | F: 3 times/week #S: 36 sessions D: 60–90 min | No significant difference was observed across time or groups in fall incidence rate at 12 weeks (p = 0.152) and 36 weeks (p = 0.954). The groups did not statistically differ in other measures except for a significant improvement in dynamic balance based on the Timed Up and Go Test in the training group (9.0 s with p = 0.001) and in the cognitive training alone group (8.6 s with p = 0.012) compared with the waitlist group (11.1 s) at 36 weeks. |
| Liao et al. [55] | F: 67.6% M: 32.4% | 16/18 | Combined physical and cognitive training | 74.3 | VR-based physical and cognitive training | F: 3 times/week #S: 36 sessions D: 60 min | Both groups showed improved executive function and verbal memory (immediate recall). However, only the VR group showed significant improvements in global cognition (p < 0.001), verbal memory (delayed recall, p = 0.002), and IADL (p < 0.001) after the intervention. The group × time interaction effects further demonstrated that IADLs were more significantly improved with VR training than CPC training (p = 0.006). The hemodynamic data revealed decreased activation in prefrontal areas after training (p = 0.015), indicative of increased neural efficiency, in the VR-trained subjects. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Perete, J.M.; Carcelén-Fraile, M.d.C.; Cano-Sánchez, J.; Aibar-Almazán, A.; Castellote-Caballero, Y.; Mesas-Aróstegui, M.A.; García-Gutiérrez, A.; Hita-Contreras, F. Combined Physical–Cognitive Therapies for the Health of Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Healthcare 2025, 13, 591. https://doi.org/10.3390/healthcare13060591
Muñoz-Perete JM, Carcelén-Fraile MdC, Cano-Sánchez J, Aibar-Almazán A, Castellote-Caballero Y, Mesas-Aróstegui MA, García-Gutiérrez A, Hita-Contreras F. Combined Physical–Cognitive Therapies for the Health of Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Healthcare. 2025; 13(6):591. https://doi.org/10.3390/healthcare13060591
Chicago/Turabian StyleMuñoz-Perete, Juan Miguel, María del Carmen Carcelén-Fraile, Javier Cano-Sánchez, Agustín Aibar-Almazán, Yolanda Castellote-Caballero, María Aurora Mesas-Aróstegui, Andrés García-Gutiérrez, and Fidel Hita-Contreras. 2025. "Combined Physical–Cognitive Therapies for the Health of Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis" Healthcare 13, no. 6: 591. https://doi.org/10.3390/healthcare13060591
APA StyleMuñoz-Perete, J. M., Carcelén-Fraile, M. d. C., Cano-Sánchez, J., Aibar-Almazán, A., Castellote-Caballero, Y., Mesas-Aróstegui, M. A., García-Gutiérrez, A., & Hita-Contreras, F. (2025). Combined Physical–Cognitive Therapies for the Health of Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Healthcare, 13(6), 591. https://doi.org/10.3390/healthcare13060591