
The Impact and Burden of Chronic Rhinosinusitis with Nasal Polyps on Patients and Their Family Caregivers: A Nationally Representative Survey

 , ,
, ,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire
2.3. Study Population
2.4. Statistical Analysis
3. Results
3.1. Demographics of the Study Population
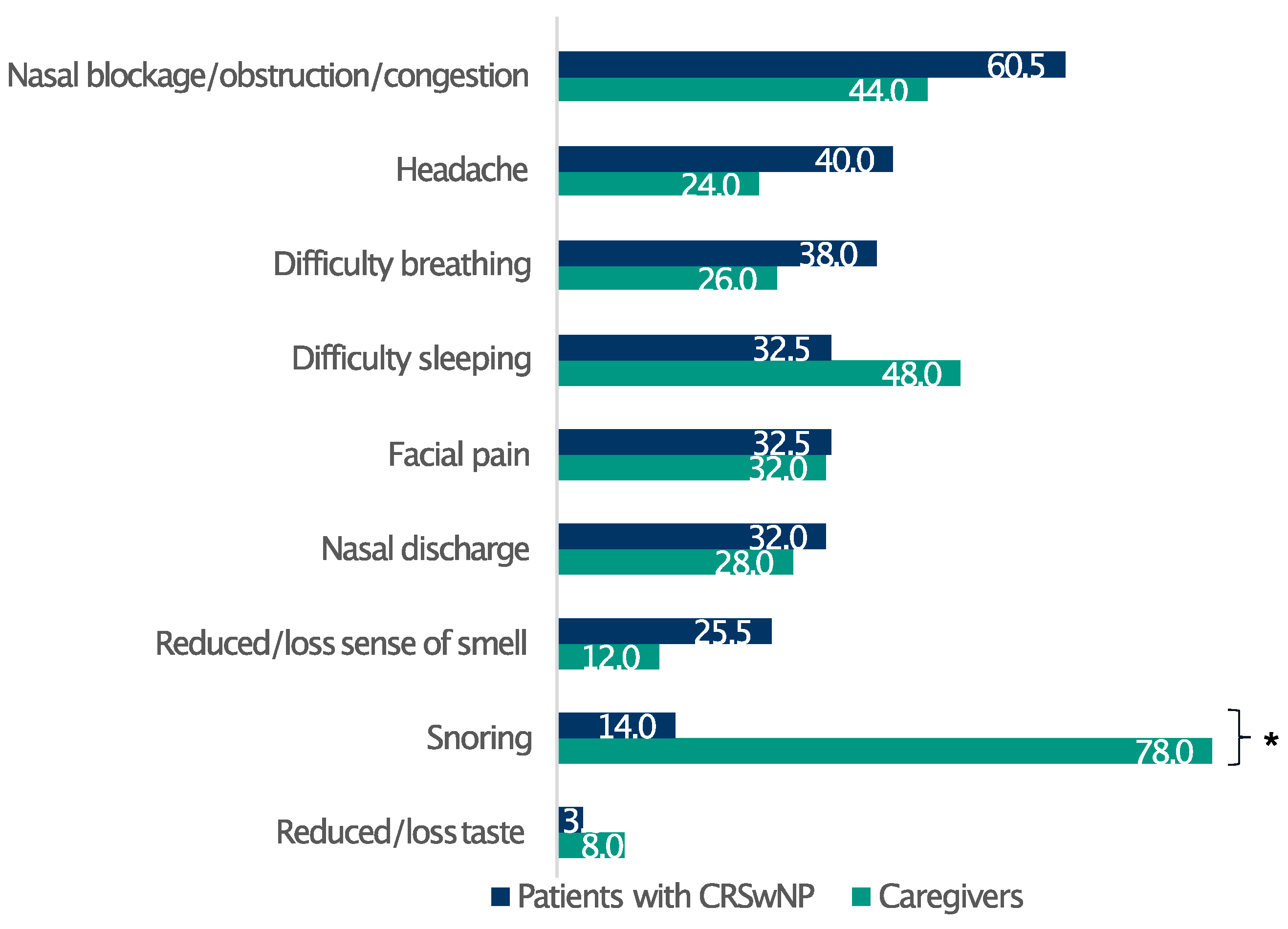
3.2. Symptoms
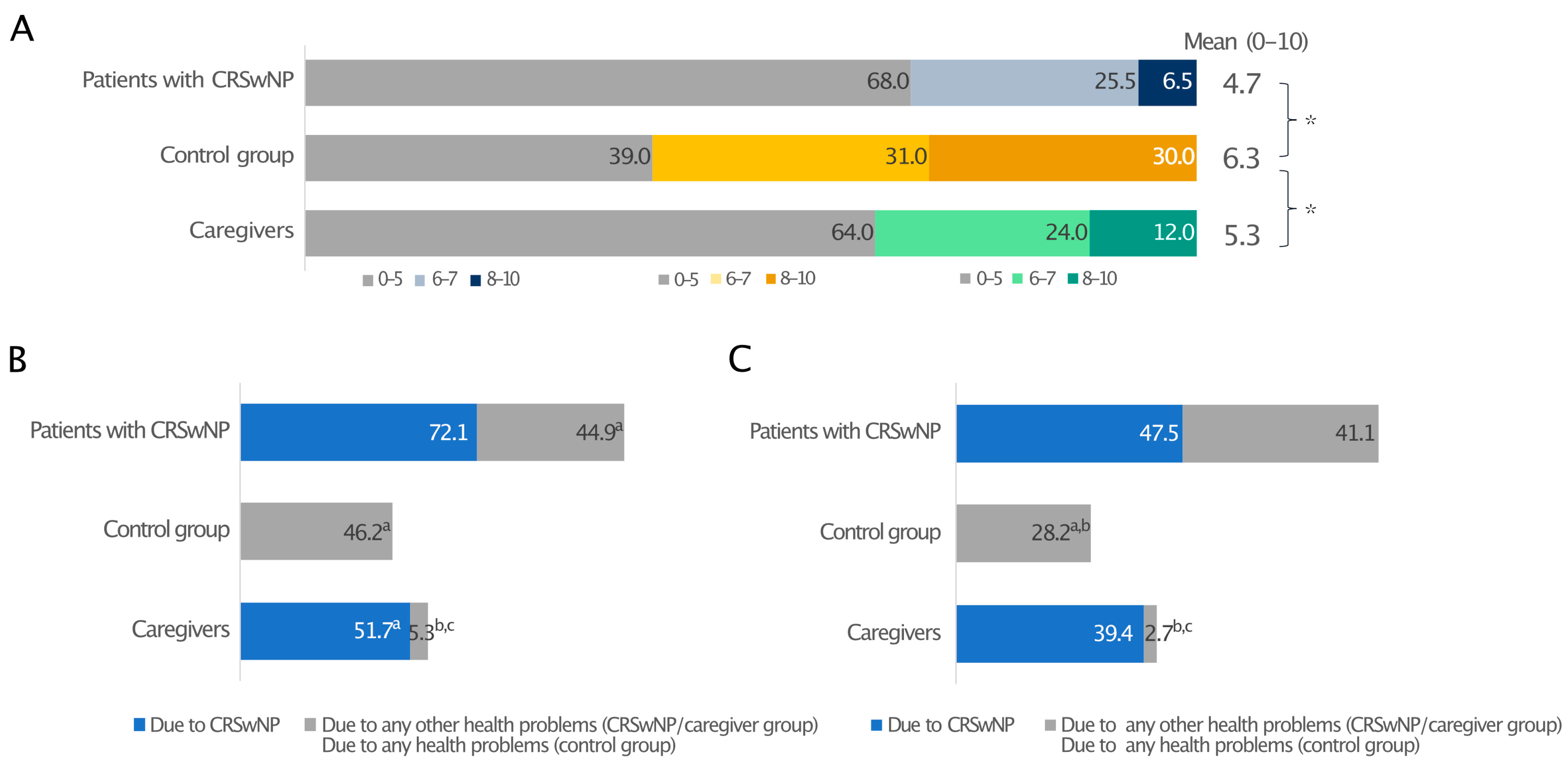
3.3. Sleep Impairment and Daily Drowsiness
3.4. Patient Journey
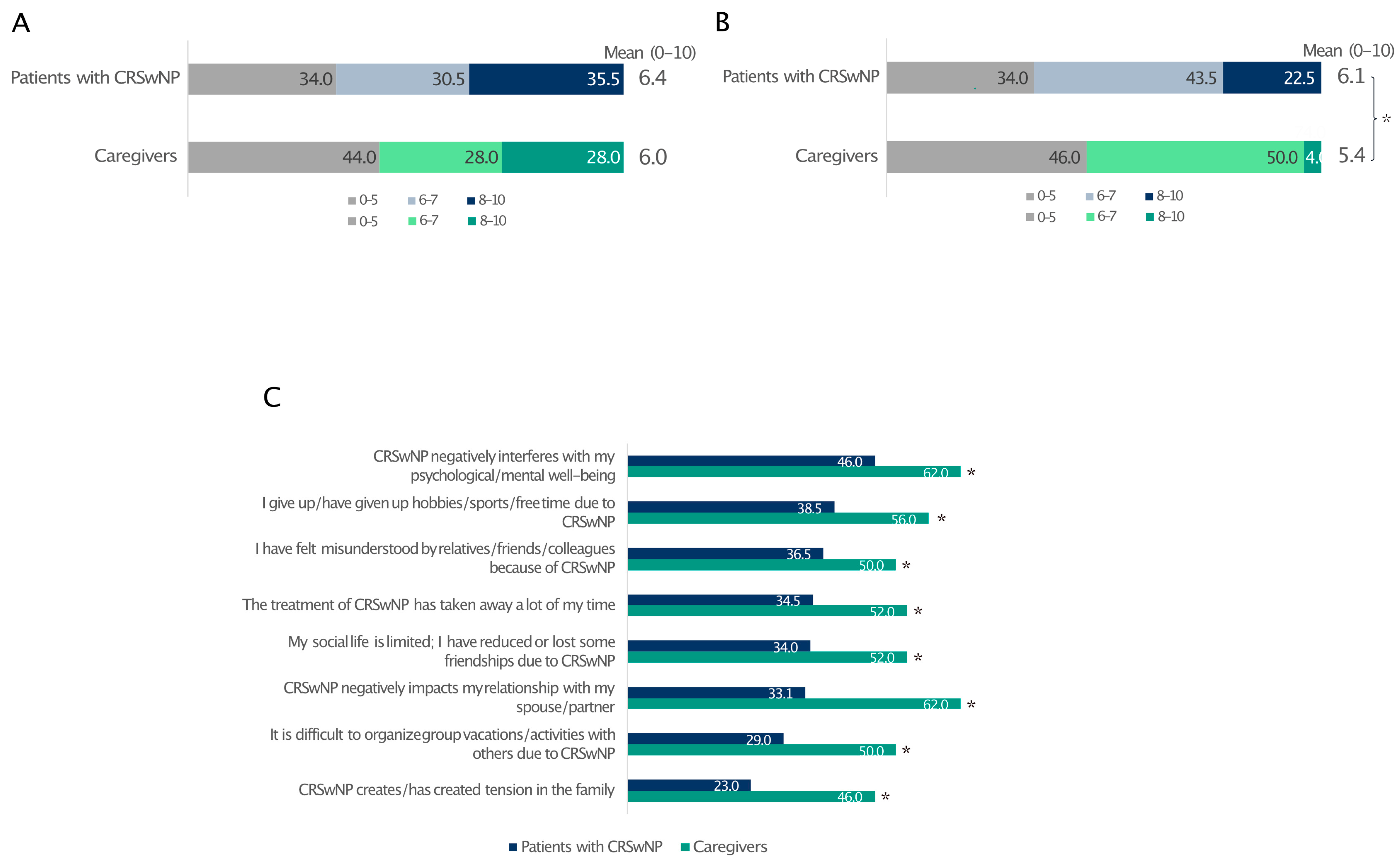
3.5. Emotional Burden and Daily Limitations
3.6. Quality of Life and Social/Couple Relationships
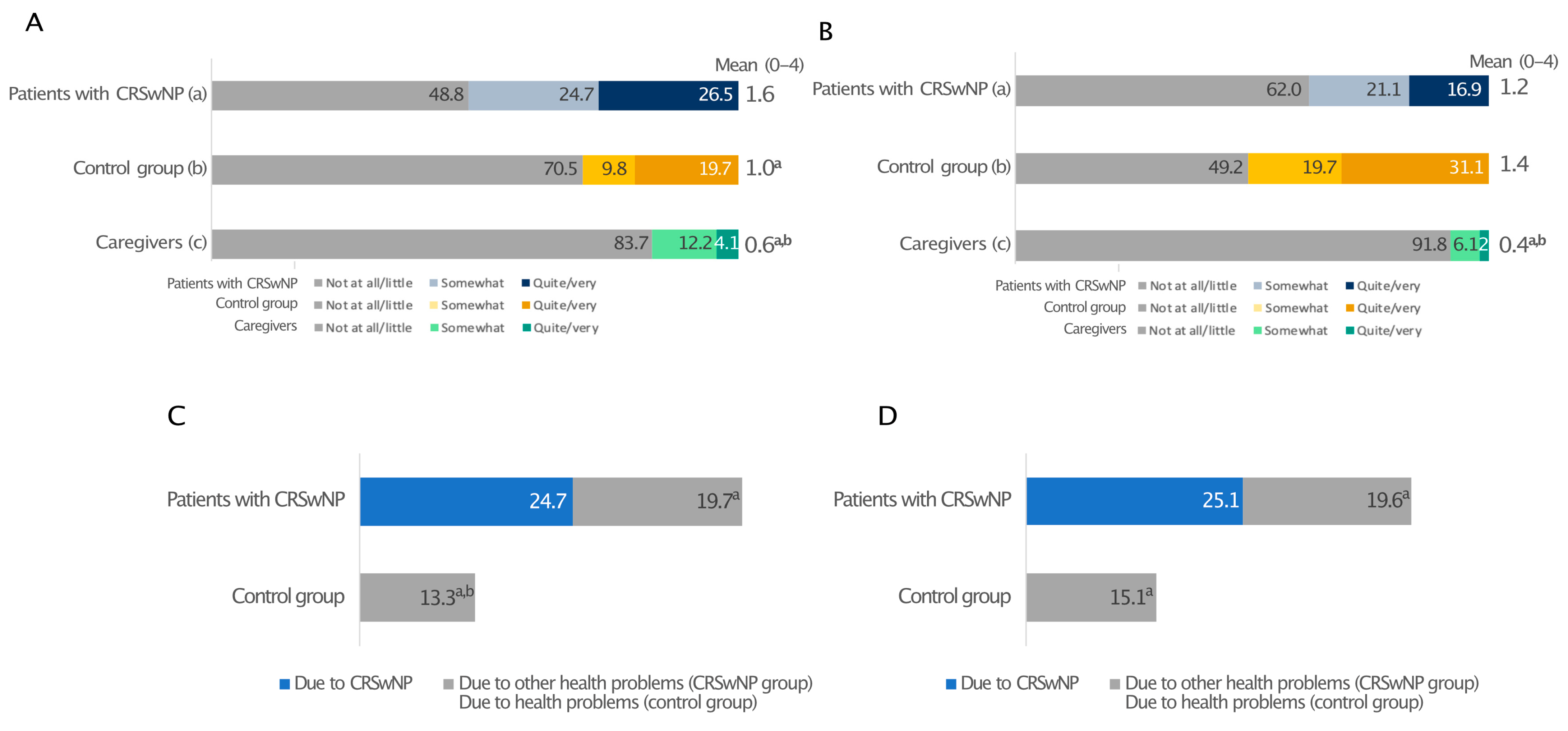
3.7. Working/School Life
3.8. Unmet Patient Needs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bachert, C.; Bhattacharyya, N.; Desrosiers, M.; Khan, A.H. Burden of Disease in Chronic Rhinosinusitis with Nasal Polyps. J. Asthma Allergy 2021, 14, 127–134. [Google Scholar] [CrossRef]
- Bachert, C.; Marple, B.; Schlosser, R.J.; Hopkins, C.; Schleimer, R.P.; Lambrecht, B.N.; Bröker, B.M.; Laidlaw, T.; Song, W.-J. Adult chronic rhinosinusitis. Nat. Rev. Dis. Prim. 2020, 6, 86. [Google Scholar] [CrossRef]
- Laidlaw, T.M.; Mullol, J.; Woessner, K.M.; Amin, N.; Mannent, L.P. Chronic Rhinosinusitis with Nasal Polyps and Asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Stevens, W.W.; Schleimer, R.P.; Kern, R.C. Chronic Rhinosinusitis with Nasal Polyps. J. Allergy Clin. Immunol. Pract. 2016, 4, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Heffler, E.; Blasi, F.; Latorre, M.; Menzella, F.; Paggiaro, P.; Pelaia, G.; Senna, G.; Canonica, G.W.; SANI Network. The Severe Asthma Network in Italy: Findings and Perspectives. J. Allergy Clin. Immunol. Pract. 2019, 7, 1462–1468. [Google Scholar] [CrossRef]
- Mullol, J.; Azar, A.; Buchheit, K.M.; Hopkins, C.; Bernstein, J.A. Chronic Rhinosinusitis With Nasal Polyps: Quality of Life in the Biologics Era. J. Allergy Clin. Immunol. Pract. 2022, 10, 1434–1453.e9. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Zhou, A.; Emmanuel, B.; Garcia, D.; Rosta, E. Systematic literature review of humanistic and economic burdens of chronic rhinosinusitis with nasal polyposis. Curr. Med. Res. Opin. 2020, 36, 1913–1926. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J. Executive summary of EPOS 2020 including integrated care pathways. Rhinology 2020, 58, 82–111. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, R.R.; Kingdom, T.T.; Smith, T.L.; Bleier, B.; DeConde, A.; Luong, A.U.; Poetker, D.M.; Soler, Z.; Welch, K.C.; Wise, S.K.; et al. International consensus statement on allergy and rhinology: Rhinosinusitis 2021. Int. Forum Allergy Rhinol. 2021, 11, 213–739. [Google Scholar]
- Davis, G.E.; Zeiger, R.S.; Emmanuel, B.; Chung, Y.; Tran, T.N.; Evans, K.A.; Chen, S.; Katial, R.; Kreindler, J.L.; Tkacz, J. Systemic Corticosteroid-related Adverse Outcomes and Health Care Resource Utilization and Costs Among Patients with Chronic Rhinosinusitis with Nasal Polyposis. Clin. Ther. 2022, 44, 1187–1202. [Google Scholar] [CrossRef]
- Lombardi, C.; Asero, R.; Bagnasco, D.; Blasi, F.; Bonini, M.; Bussi, M.; Canevari, R.F.; Canonica, G.W.; Castelnuovo, P.; Cecchi, L.; et al. ARIA-ITALY multidisciplinary consensus on nasal polyposis and biological treatments. World Allergy Organ. J. 2021, 14, 100592. [Google Scholar] [CrossRef]
- Rank, M.A.; Chu, D.K.; Bognanni, A.; Oykhman, P.; Bernstein, J.A.; Ellis, A.K.; Golden, D.B.; Greenhawt, M.; Horner, C.C.; Ledford, D.K.; et al. The Joint Task Force on Practice Parameters GRADE guidelines for the medical management of chronic rhinosinusitis with nasal polyposis. J. Allergy Clin. Immunol. 2023, 151, 386–398. [Google Scholar] [CrossRef]
- Lourijsen, E.S.; Fokkens, W.J.; Reitsma, S. Direct and indirect costs of adult patients with chronic rhinosinusitis with nasal polyps. Rhinology. 2020, 58, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Stull, D.E.; Roberts, L.; Frank, L.; Heithoff, K. Relationship of nasal congestion with sleep, mood, and productivity. Curr. Med. Res. Opin. 2007, 23, 811–819. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Toma, S.; Hopkins, C. Stratification of SNOT-22 scores into mild, moderate or severe and relationship with other subjective instruments. Rhinology 2016, 54, 129–133. [Google Scholar] [CrossRef]
- Hellings, P.W. SWOT Analysis of Chronic Rhinosinusitis Care Anno 2022. J. Allergy Clin. Immunol. Pract. 2022, 10, 1468–1471. [Google Scholar] [CrossRef]
- Neri, I.; Galli, E.; Baiardini, I.; Picozza, M.; Rossi, A.B.; Matruglio, P.; Moretti, D.; Cipriani, F. Implications of Atopic Dermatitis on the Quality of Life of 6-11 Years Old Children and Caregivers (PEDI-BURDEN). J. Asthma Allergy 2023, 16, 383–396. [Google Scholar] [CrossRef]
- Stingeni, L.; Belloni Fortina, A.; Baiardini, I.; Hansel, K.; Moretti, D.; Cipriani, F. Atopic Dermatitis and Patient Perspectives: Insights of Bullying at School and Career Discrimination at Work. J. Asthma Allergy 2021, 14, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Luke, L.; Lee, L.; Gokani, S.A.; Boak, D.; Boardman, J.; Philpott, C. Understanding the Impact of Chronic Rhinosinusitis with Nasal Polyposis on Smell and Taste: An International Patient Experience Survey. J. Clin. Med. 2023, 12, 5367. [Google Scholar] [CrossRef]
- Ferri, S.; Montagna, C.; Casini, M.; Malvezzi, L.; Pirola, F.; Russo, E.; Racca, F.; Messina, M.R.; Puggioni, F.; Nappi, E.; et al. Sleep quality burden in chronic rhinosinusitis with nasal polyps and its modulation by dupilumab. Ann. Allergy Asthma Immunol. 2024, 132, 69–75. [Google Scholar] [CrossRef]
- Schneider, S.; Campion, N.J.; Villazala-Merino, S.; Liu, D.T.; Bartosik, T.; Landegger, L.D.; Ahmadi, N.; Mueller, C.A.; Vyskocil, E.; Stanek, V.; et al. Associations between the Quality of Life and Nasal Polyp Size in Patients Suffering from Chronic Rhinosinusitis without Nasal Polyps, with Nasal Polyps or Aspirin-Exacerbated Respiratory Disease. J. Clin. Med. 2020, 9, 925. [Google Scholar] [CrossRef]
- Seys, S.F.; De Bont, S.; Fokkens, W.J.; Bachert, C.; Alobid, I.; Bernal-Sprekelsen, M.; Bjermer, L.; Callebaut, I.; Cardell, L.O.; Carrie, S.; et al. Real-life assessment of chronic rhinosinusitis patients using mobile technology: The mySinusitisCoach project by EUFOREA. Allergy 2020, 75, 2867–2878. [Google Scholar] [CrossRef]
- Orb, Q.; Orlandi, R.R.; Alt, J.A. Sleep dysfunction and its association to chronic rhinosinusitis: Updated review. Laryngoscope Investig. Otolaryngol. 2017, 2, 46–52. [Google Scholar] [CrossRef]
- Krueger, J.M. The role of cytokines in sleep regulation. Curr. Pharm. Des. 2008, 14, 3408–3416. [Google Scholar] [CrossRef] [PubMed]
- Muzio, M.; Sironi, M.; Polentarutti, N.; Mantovani, A.; Colotta, F. Induction by transforming growth factor-β1 of the interleukin-1 receptor antagonist and of its intracellular form in human polymorphonuclear cells. Eur. J. Immunol. 1994, 24, 3194–3198. [Google Scholar] [CrossRef] [PubMed]
- Alt, J.A.; Sautter, N.B.; Mace, J.C.; Detwiller, K.Y.; Smith, T.L. Antisomnogenic cytokines, quality of life, and chronic rhinosinusitis: A pilot study. Laryngoscope 2014, 124, E107–E114. [Google Scholar] [CrossRef]
- Erskine, S.E.; Philpott, C.M. An unmet need: Patients with smell and taste disorders. Clin. Otolaryngol. 2020, 45, 197–203. [Google Scholar] [CrossRef]
- Wang, Z.; Yu, S.; Liu, Y.; Han, Y.; Zhao, W.; Zhang, W. Effectiveness of family centred interventions for family caregivers: A systematic review and meta-analysis of randomized controlled trials. J. Clin. Nurs. 2024, 33, 1958–1975. [Google Scholar] [CrossRef] [PubMed]
- Talley, R.C.; Crews, J.E. Framing the public health of caregiving. Am. J. Public Health 2007, 97, 224–228. [Google Scholar] [CrossRef]
- Adams, K.N.; Farquhar, D.; Senior, B.A.; Thorp, B.D.; Zanation, A.M.; Ebert, C.S. A Pilot Comparison between Caregiver’s and Patient’s Perceived Quality of Life in Chronic Rhinosinusitis. Am. J. Rhinol. Allergy 2018, 32, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Oakley, G.M.; Smith, K.A.; Ashby, S.; Orlandi, R.R.; Alt, J.A. Sleep Dysfunction is an Independent Predictor of Productivity Losses in Patients with Chronic Rhinosinusitis. Ann. Otol. Rhinol. Laryngol. 2021, 130, 1332–1339. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.P.; Phillips, K.M.; Hoehle, L.P.; Feng, A.L.; Bergmark, R.W.; Caradonna, D.S.; Gray, S.T.; Sedaghat, A.R. Depression symptoms and lost productivity in chronic rhinosinusitis. Ann. Allergy Asthma Immunol. 2017, 118, 286–289. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Group (n = 200) | Control Group (n = 100) | |
|---|---|---|
| Age (years) | 43 | 51 |
| Female/male (%) | 56/44 | 52/48 |
| Severity of CRSwNPs (%) | ||
| Mild (SNOT-22 score 8–20) | 2.5 | NA |
| Moderate (SNOT-22 score >20–50) | 14.0 | |
| Severe (SNOT-22 score >50) | 83.5 | |
| Mean SNOT-22 | 6.89 | |
| CRSwNPs and asthma (%) | ||
| CRSwNPs with mild asthma | 17.5 | NA |
| CRSwNPs with moderate asthma | 12.5 | |
| CRSwNPs with severe asthma | 5.0 | |
| CRSwNPs with other condition/s ^ | 3 | |
| Mean number of past and current comorbidities | 3.5 | 1.5 |
| Past and current comorbidities (%) | ||
| Pollen allergies * | 49.5 | 16.0 |
| Dust allergies * | 47.0 | 16.0 |
| Allergic conjunctivitis * | 32.5 | 13.0 |
| Food allergies * | 30.0 | 12.0 |
| Hay fever * | 25.0 | 7.0 |
| Atopic dermatitis * | 24.5 | 11.0 |
| Pet fur allergies * | 22.5 | 7.0 |
| Severe eating disorders * | 7.5 | 1.0 |
| Comorbidities in the family circle (%) | ||
| Plant and pollen allergies * | 52.0 | 30.0 |
| Dust allergies * | 48.0 | 26.0 |
| Asthma * | 36.0 | 18.0 |
| CRSwNPs * | 30.5 | 2.0 |
| Atopic dermatitis * | 28.0 | 10.0 |
| Eosinophilic esophagitis * | 16.0 | 3.0 |
| Insect bite allergies * | 15.5 | 4.0 |
| None of the above * | 19.0 | 38.0 |
| Patient Group (n = 200) | |||
|---|---|---|---|
| Mean disease duration (years) | 11.3 | ||
| Mean time from first symptoms to diagnosis (years) | 7.2 | ||
| Specialist (%) | Consulted with first symptoms | Made diagnosis | Currently under specialist management |
| ENT | 52.0 | 62.0 | 53.5 |
| GP | 27.0 | 19.5 | 26.0 |
| Allergologist | 11.0 | 11.5 | 10.0 |
| Chest physician | 4.0 | 5.0 | 7.0 |
| Immunologist | 1.0 | 1.0 | 2.0 |
| Did not remember | 5.0 | 1.0 | 12.5 ^ |
| Patient Group (n = 200) | ||
|---|---|---|
| Past and current nasal irrigations (%) | ||
| Often | 52.0 | |
| Rarely | 29.7 | |
| Never | 18.3 | |
| Currently in pharmacological treatment, yes/no (%) | 53.1/46.9 | |
| Mean duration of pharmacological treatment (years) | 7.3 | |
| Pharmacological treatment (%) | In the last 6 months (n = 175) | Previously |
| Corticosteroid spray | 55.4 | 65.7 |
| Oral corticosteroids | 20.0 | 41.1 |
| Injectable corticosteroids | 5.8 | 10.3 |
| Other ^ | 5.8 | 9.0 |
| No pharmacological treatment | 13.7 | NA |
| Past use of biologics (%) | 12 | |
| Benralizumab | 5.5 | |
| Mepolizumab | 5.5 | |
| Omalizumab | 3.0 | |
| Dupilumab | 1.5 | |
| Specialist who prescribed pharmacological treatment in the last 6 months (%) | ||
| ENT | 63.2 | |
| GP | 17.1 | |
| Allergologist | 9.9 | |
| Chest physician | 6.6 | |
| Immunologist | 1.3 | |
| Other | 1.4 | |
| Unknown | 0.7 | |
| Mean monthly spending on treatments (%), EUR | ||
| 0–10 | 31.0 | |
| 11–40 | 37.5 | |
| 41–80 | 26.5 | |
| >80 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malvezzi, L.; Seccia, V.; Moffa, A.; Canevari, F.R.M.; Baiardini, I.; Barbaglia, S.; Battistini, M.; Cantoni, E.; Cipriani, F.; Pirronello, M.; et al. The Impact and Burden of Chronic Rhinosinusitis with Nasal Polyps on Patients and Their Family Caregivers: A Nationally Representative Survey. Healthcare 2025, 13, 430. https://doi.org/10.3390/healthcare13040430
Malvezzi L, Seccia V, Moffa A, Canevari FRM, Baiardini I, Barbaglia S, Battistini M, Cantoni E, Cipriani F, Pirronello M, et al. The Impact and Burden of Chronic Rhinosinusitis with Nasal Polyps on Patients and Their Family Caregivers: A Nationally Representative Survey. Healthcare. 2025; 13(4):430. https://doi.org/10.3390/healthcare13040430
Chicago/Turabian StyleMalvezzi, Luca, Veronica Seccia, Antonio Moffa, Frank Rikki Mauritz Canevari, Ilaria Baiardini, Simona Barbaglia, Mattia Battistini, Eleonora Cantoni, Filippo Cipriani, Marta Pirronello, and et al. 2025. "The Impact and Burden of Chronic Rhinosinusitis with Nasal Polyps on Patients and Their Family Caregivers: A Nationally Representative Survey" Healthcare 13, no. 4: 430. https://doi.org/10.3390/healthcare13040430
APA StyleMalvezzi, L., Seccia, V., Moffa, A., Canevari, F. R. M., Baiardini, I., Barbaglia, S., Battistini, M., Cantoni, E., Cipriani, F., Pirronello, M., Sala, G., Stassaldi, A., & De Corso, E. (2025). The Impact and Burden of Chronic Rhinosinusitis with Nasal Polyps on Patients and Their Family Caregivers: A Nationally Representative Survey. Healthcare, 13(4), 430. https://doi.org/10.3390/healthcare13040430