
A Protocol for Enhancing Allied Health Care for Older People in Residential Care: The EAHOP Intervention

 , ,
, ,  , , , ,
, , , ,  , , , , , , and
, , , , , , and
Abstract
1. Background
1.1. Research Questions
- Is an integrated transdisciplinary allied health service model effective in preventing falls, addressing frailty, and promoting engagement in people transitioning to or living in residential aged care?
- Can an integrated transdisciplinary allied health service model improve outcomes focused on falls, frailty, and engagement, compared to baseline measures, in people transitioning to or living in residential aged care?
- What are the care experiences of residents, carers, staff, and other key stakeholders when an integrated transdisciplinary allied health service model is implemented in residential aged care?
1.2. Objectives
- Implement and evaluate a new integrated and transdisciplinary model of allied health intervention in relation to the impact on falls, frailty, engagement, quality of life, and cost-effectiveness.
- Evaluate the process (or implementation) of the new allied health service model by asking key stakeholders (residents, families, care staff, and nursing staff) about their experiences of participating in the model.
- Produce evidence-informed guidelines for residential aged care providers in Australia to implement an integrated transdisciplinary allied health service.
2. Methods
2.1. Study Design
2.2. Study Setting
2.3. Participants
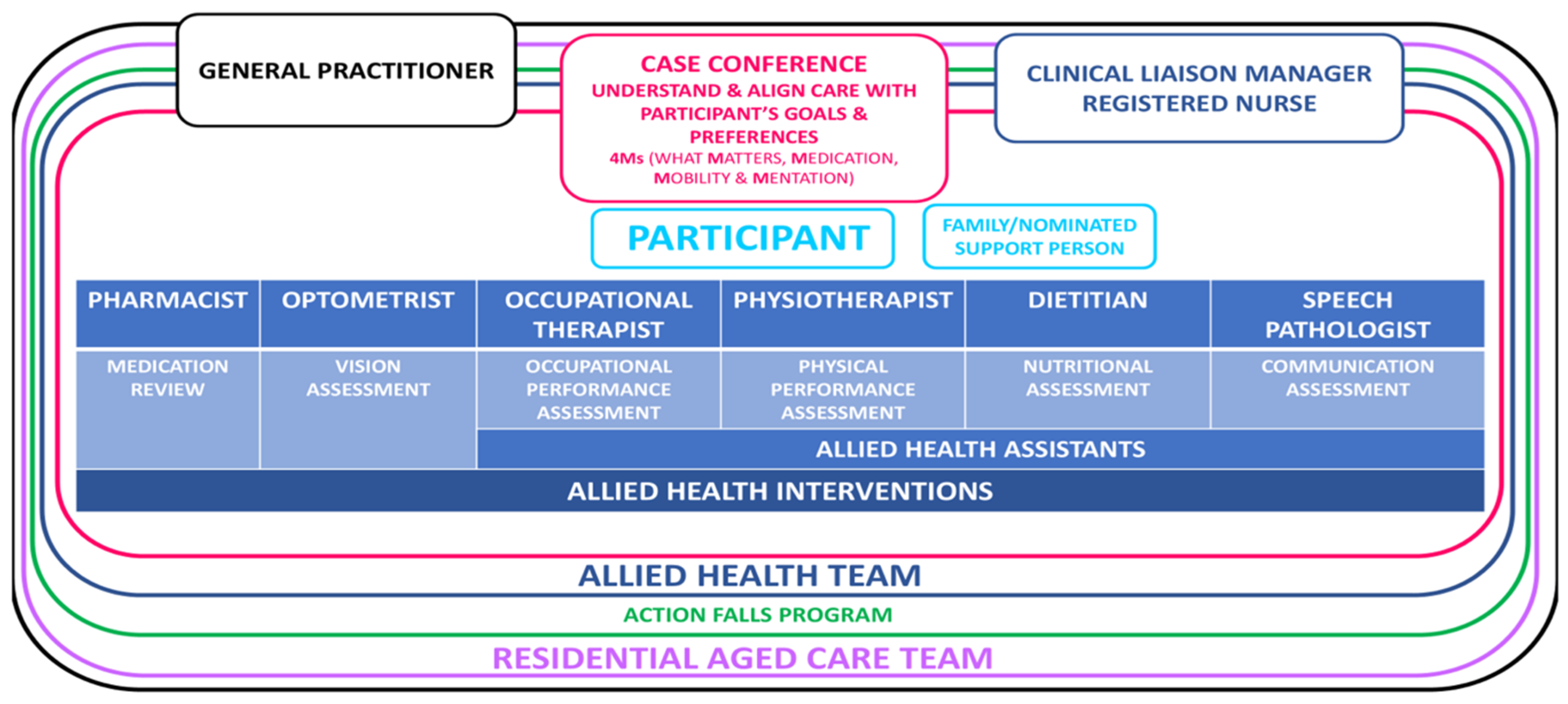
2.4. Conceptual and Operational Framework
2.4.1. Model of Care
- What Matters: Know and align care with each older adult’s goals and care preferences.
- Mentation: Prevent, identify, treat and manage dementia, depression, and delirium across care settings.
- Medication: If medication is necessary, it should not interfere with What Matters to the older person.
- Mobility: Ensure that older people move safely every day.
2.4.2. Case Conferencing
2.4.3. Clinical Liaison Manager
2.4.4. Allied Health Professionals and General Practitioner
2.4.5. Allied Health Assistants
2.5. Intervention
Action Falls Program
2.6. SampleSsize
2.7. Data Collection and Monitoring
2.8. Outcome Measures
2.9. Program Evaluation
- To ascertain if the transdisciplinary model has met the project aim of improving quality of care.
- To identify barriers and enablers to implementation of the program as planned, with the aim of developing an implementation guideline.
- To provide a detailed description of program resourcing.

{kind=link}
| Implementation Outcome | Measurement Details |
|---|---|
| Feasibility |
|
| Access and Uptake |
|
| Acceptability |
|
2.10. Economic Evaluation
2.11. Fidelity Assessment
3. Data Analysis
3.1. Quantitative Analysis
3.2. Qualitative Analysis
4. Ethics Review
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Institute of Health and Welfare GEN Aged Care Data. People Using Aged Care. 2024. Available online: http://www.gen-agedcaredata.gov.au/topics/people-using-aged-care (accessed on 1 October 2024).
- Inacio, M.C.; Moldovan, M.; Whitehead, C.; Sluggett, J.K.; Crotty, M.; Corlis, M.; Visvanathan, R.; Wesselingh, S.; Caughey, G.E. The risk of fall-related hospitalisations at entry into permanent residential aged care. BMC Geriatr. 2021, 21, 686. [Google Scholar] [CrossRef]
- Whitney, J.; Close, J.C.T.; Jackson, S.H.D.; Lord, S.R. Understanding Risk of Falls in People With Cognitive Impairment Living in Residential Care. J. Am. Med. Dir. Assoc. 2012, 13, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Trends in Hospitalised Injury Due to Falls in Older People 2007–2008 to 2016–2017; Australian Institute of Health and Welfare: Canberra, Australian, 2019.
- Jadczak, A.D.; Robson, L.; Cooper, T.; Bell, J.S.; Visvanathan, R.; FIRST Study Collaborators. The Frailty In Residential Sector over Time (FIRST) study: Methods and baseline cohort description. BMC Geriatr. 2021, 21, 99. [Google Scholar]
- Kojima, G. Frailty as a predictor of hospitalisation among community-dwelling older people: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Causey-Upton, R. A Model for Quality of Life: Occupational Justice and Leisure Continuity for Nursing Home Residents. Phys. Occup. Ther. Geriatr. 2015, 33, 175–188. [Google Scholar] [CrossRef]
- du Toit, S.H.; Casteleijn, D.; Adams, F.; Morgan-Brown, M. Occupational justice within residential aged care settings—Time to focus on a collective approach. Br. J. Occup. Ther. 2019, 82, 578–581. [Google Scholar] [CrossRef]
- Royal Commission into Aged Care Quality and Safety (RCACQS). 2021; Final Report Volume 1. Available online: https://agedcare.royalcommission.gov.au/ (accessed on 10 October 2024).
- Frändin, K.; Grönstedt, H.; Helbostad, J.L.; Bergland, A.; Andresen, M.; Puggaard, L.; Harms-Ringdahl, K.; Granbo, R.; Hellström, K. Long-Term Effects of Individually Tailored Physical Training and Activity on Physical Function, Well-Being and Cognition in Scandinavian Nursing Home Residents: A Randomized Controlled Trial. Gerontology 2016, 62, 571–580. [Google Scholar] [CrossRef]
- Eager, K.; Westera, A.; Snoek, M.; Kobel, C.; Loggie, C.; Gordon, R. How Australian Residential Aged Care Staffing Levels Compare with International and National Benchmarks: A Research Study Commissioned by the Royal Commission into Aged Care Quality and Safety. 2019. Available online: https://hdl.handle.net/10779/uow.27702252.v1 (accessed on 1 October 2024).
- Gibson, D.; Isbel, S. Reform and reverberation: Australian aged care policy changes and the unintended consequences for allied health. Aust. Occup. Ther. J. 2024, 71, 392–407. [Google Scholar] [CrossRef]
- Jorm, A.F.; Mackinnon, A.J.; Henderson, A.S.; Scott, R.; Christensen, H.; Korten, A.E.; Cullen, J.S.; Mulligan, R. The Psychogeriatric Assessment Scales: A multi-dimensional alternative to categorical diagnoses of dementia and depression in the elderly. Psychol. Med. 1995, 25, 447–460. [Google Scholar] [CrossRef]
- Institute for Healthcare Improvment. Age-Friendly Health Systems: Guide to Using the 4Ms in the Care of Older Adults; Institute for Healthcare Improvement: Boston, MA, USA, 2020. [Google Scholar]
- Hewitt, J.; Goodall, S.; Clemson, L.; Henwood, T.; Refshauge, K. Progressive Resistance and Balance Training for Falls Prevention in Long-Term Residential Aged Care: A Cluster Randomized Trial of the Sunbeam Program. J. Am. Med. Dir. Assoc. 2018, 19, 361–369. [Google Scholar] [CrossRef]
- D’Cunha, N.M.; Isbel, S.T.; Frost, J.; Fearon, A.; McKune, A.J.; Naumovski, N.; Kellett, J. Effects of a virtual group cycling experience on people living with dementia: A mixed method pilot study. Dementia 2021, 20, 1518–1535. [Google Scholar] [CrossRef] [PubMed]
- Logan, P.A.; Horne, J.C.; Gladman, J.R.F.; Gordon, A.L.; Sach, T.; Clark, A.; Robinson, K.; Armstrong, S.; Stirling, S.; Leighton, P.; et al. Multifactorial Falls Prevention Programme Compared with Usual Care in UK Care Homes for Older People: Multicentre Cluster Randomised Controlled Trial with Economic Evaluation. BMJ 2021, 375. [Google Scholar] [CrossRef] [PubMed]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.; Hutchinson, C.; McBain, C.; Walker, R.; Milte, R.; Khadka, J.; Ratcliffe, J. Developing dimensions for a preference-based quality of life instrument for older people receiving aged care services in the community. Qual. Life Res. 2021, 30, 555–565. [Google Scholar] [CrossRef]
- Kaehr, E.W.; Pape, L.C.; Malmstrom, T.K.; Morley, J.E. FRAIL-NH predicts outcomes in long term care. J. Nutr. Health Aging 2016, 20, 192–198. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with selfreported disability and prediction of mortality and nursing home admission. J. Gerontol. Med. Sci. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Kempen, G.I.J.M.; Yardley, L.; Van Haastregt, J.C.M.; Zijlstra, G.A.R.; Beyer, N.; Hauer, K.; Todd, C. The Short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 2008, 37, 45–50. [Google Scholar] [CrossRef]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? J. Parenter. Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef]
- Frisancho, A.R. New standards of weight and body composition by frame size and height for assessment of nutritional status of adults and the elderly. Am. J. Clin. Nutr. 1984, 40, 808–819. [Google Scholar] [CrossRef]
- Gort-van Dijk, D.; Weerink, L.B.M.; Milovanovic, M.; Haveman, J.W.; Hemmer, P.H.J.; Dijkstra, G.; Lindeboom, R.; Campmans-Kuijpers, M.J. Bioelectrical Impedance Analysis and Mid-Upper Arm Muscle Circumference Can Be Used to Detect Low Muscle Mass in Clinical Practice. Nutrients 2021, 13, 2350. [Google Scholar] [CrossRef]
- Carswell, A.; McColl, M.A.; Baptiste, S.; Law, M.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: A Research and Clinical Literature Review. Can. J. Occup. Ther. 2004, 71, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Mangione, C.M.; Lee, P.P.; Gutierrez, P.R.; Spritzer, K.; Berry, S.; Hays, R.D.; the National Eye Institute Visual Function Questionnaire Field Test Investigators. Development of the 25-list-item National Eye Institute Visual Function Questionnaire. Arch. Ophthalmol. 2001, 119, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Strøm, B.S.; Engedal, K.; Benth, J.Š.; Grov, E.-K. Psychometric evaluation of the Holden Communication Scale (HCS) for persons with dementia. BMJ Open 2016, 6, e013447. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, D.L.; Steverink, N.; Frijters, D.H.; Hirdes, J.P.; Ooms, M.E.; Ribbe, M.W. A revised Index for Social Engagement for long-term care. J. Gerontol. Nurs. 2008, 34, 40–48. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar]
- Warden, V.; Hurley, A.C.; Volicer, L. Development and psychometric evaluation of the Pain Assessment in Advanced Dementia (PAINAD) scale. J. Am. Med. Dir. Assoc. 2003, 4, 9–15. [Google Scholar] [CrossRef]
- Hasson, H.; Blomberg, S.; Duner, A. Fidelity and moderating factors in complex interventions: A case study of a continuum of care program for frail elderly people in health and social care. Implement Sci. 2012, 7, 23. [Google Scholar] [CrossRef]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
| Description | |
|---|---|
| Occupational Therapy | Participants will identify goals relating to activities of everyday living with specific reference to self-care, leisure activities, and productivity that are meaningful to them that they would like to be engaged with and/or become more satisfied with. The occupational therapist will develop goal-directed and individually tailored occupational therapy interventions to improve performance and satisfaction with the identified occupational performance challenges. These will be discussed with Health and Lifestyle staff to support ongoing sustainable implementation with the individual. |
| Physiotherapy | Participants will engage in exercise based upon the SUNBEAM program [15] involving 2 h per week of individually tailored strength and balance exercises prescribed by the physiotherapist for 25 weeks (total 50 h) and then a maintenance program for the duration of the intervention. In some instances, participants may not be suitable for the SUNBEAM program. In these cases, they will be offered an individualised virtual cycling experience [16] once a week for the intervention’s duration. |
| Dietetics and Nutrition | Participants diagnosed with weight loss or at risk of malnutrition will be provided with an individualised, high-protein, high-energy diet by fortifying menu items such as porridge, soups, mashed potato, and desserts, and/or oral nutrition supplements. In addition, the dietitian will provide modified menus to Food Service staff and training to Food Service staff on how to fortify menu items as per modified menus. |
| Speech Pathology | Participants will receive individualised interventions focused on communication partner training over a period of up to 36 weeks. The speech pathology intervention may include communication repair strategies, an education component, role play, practice, and recording of communication interactions to identify and address communication challenges. |
| Optometry | Participants will receive an onsite, mobile assessment by an optometrist evaluating visual function (including refraction, confrontation fields, visual acuity, ocular structure (macula and optic nerve lenticular assessment, and intra-ocular pressure) to address visual impairments that may contribute to fall risk. Actions arising from the assessment of visual function may include new spectacle prescriptions or referral of participants for management of ocular disease. |
| Pharmacy | Participants will receive an onsite medication review by a pharmacist who will provide recommendations regarding the resident’s medication to the participant’s GP, nursing staff, and family members. After the initial medication review, participants will receive a 2-week follow-up visit to understand how medication decisions are implemented in the medication treatment and charts. Each participant will have an initial case conference and then a follow-up visit from the pharmacist every 3 months (online or in person). |
| Increase Mean Response After Intervention | Power |
|---|---|
| 2.5 | 0.99 |
| 2 | 0.94 |
| 1.75 | 0.84 |
| 1 | 0.63 |
| Primary Outcome Measures | |
|---|---|
| Falls: Number of falls in past 12 months Number of falls during intervention period Number of falls after intervention | |
| Quality of Life Aged Care Consumers (QOL-ACC) [19] | |
| Frailty: The Frail in Nursing Homes (Frail-NH) Scale [20] and the and Patient Health Questionnaire (PHQ9) [22] | |
| Short Physical Performance Battery (SPPB) [21] | |
| Secondary outcome measures | Allied health discipline |
| Short Falls Efficacy Scale—International (Short FES-I) [23] | Physiotherapy |
| Subjective Global Assessment (SGA) [24] Mid-arm muscle circumference [25,26] Quantitative analysis of dietary intake will be calculated before and after fortification | Nutrition and Dietetics |
| Canadian Occupational Performance Measure (COPM) [27] | Occupational Therapy |
| Number of medications (that contributed to increased risk of falls) ceased/changed at case conferences Number of case conferences and pharmacist follow-ups Rate of GP agreement on pharmacist recommendations | Pharmacy |
| Number of new or updated spectacles recommended Number of referrals arising from vision assessment The National Eye Institute Visual Functioning Questionnaire—25 (VFQ-25 + 10) [28] | Optometry |
| Holden Communication Scale [29] Number of communication breakdowns occurring The number of resolutions (strategies used to repair the communication breakdowns) | Speech Pathology |
| Revised Index for Social Engagement (RISE) [30] | All |
| Brief Pain Inventory (short form) [31] or PAINAD [32] | All |
| ACTION Falls: number of ACTION falls checklists completed [17] | All |
| Hospital leave days | All |
| Program satisfaction survey | All |
| Qualitative interviews | All |
| Program evaluation | All |
| Economic analysis | All |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isbel, S.; D’Cunha, N.M.; Wiseman, L.; Dawda, P.; Kosari, S.; Pearce, C.; Fearon, A.; Sabeti, F.; Hewitt, J.; Kellett, J.; et al. A Protocol for Enhancing Allied Health Care for Older People in Residential Care: The EAHOP Intervention. Healthcare 2025, 13, 341. https://doi.org/10.3390/healthcare13030341
Isbel S, D’Cunha NM, Wiseman L, Dawda P, Kosari S, Pearce C, Fearon A, Sabeti F, Hewitt J, Kellett J, et al. A Protocol for Enhancing Allied Health Care for Older People in Residential Care: The EAHOP Intervention. Healthcare. 2025; 13(3):341. https://doi.org/10.3390/healthcare13030341
Chicago/Turabian StyleIsbel, Stephen, Nathan M. D’Cunha, Lara Wiseman, Paresh Dawda, Sam Kosari, Claire Pearce, Angela Fearon, Faran Sabeti, Jennifer Hewitt, Jane Kellett, and et al. 2025. "A Protocol for Enhancing Allied Health Care for Older People in Residential Care: The EAHOP Intervention" Healthcare 13, no. 3: 341. https://doi.org/10.3390/healthcare13030341
APA StyleIsbel, S., D’Cunha, N. M., Wiseman, L., Dawda, P., Kosari, S., Pearce, C., Fearon, A., Sabeti, F., Hewitt, J., Kellett, J., Naunton, M., Southwood, H., Logan, P., Subramanian, R., Chadborn, N. H., Davey, R., Bail, K., Goss, J. R., Ambikairajah, A., ... Gibson, D. (2025). A Protocol for Enhancing Allied Health Care for Older People in Residential Care: The EAHOP Intervention. Healthcare, 13(3), 341. https://doi.org/10.3390/healthcare13030341