

Barriers and Facilitators of Access to Healthcare Among Immigrants with Disabilities: A Qualitative Meta-Synthesis



Abstract
1. Introduction
2. U.S. and Canadian Healthcare Systems
3. Methods
3.1. Methodological Framework
3.2. Database and Search Description
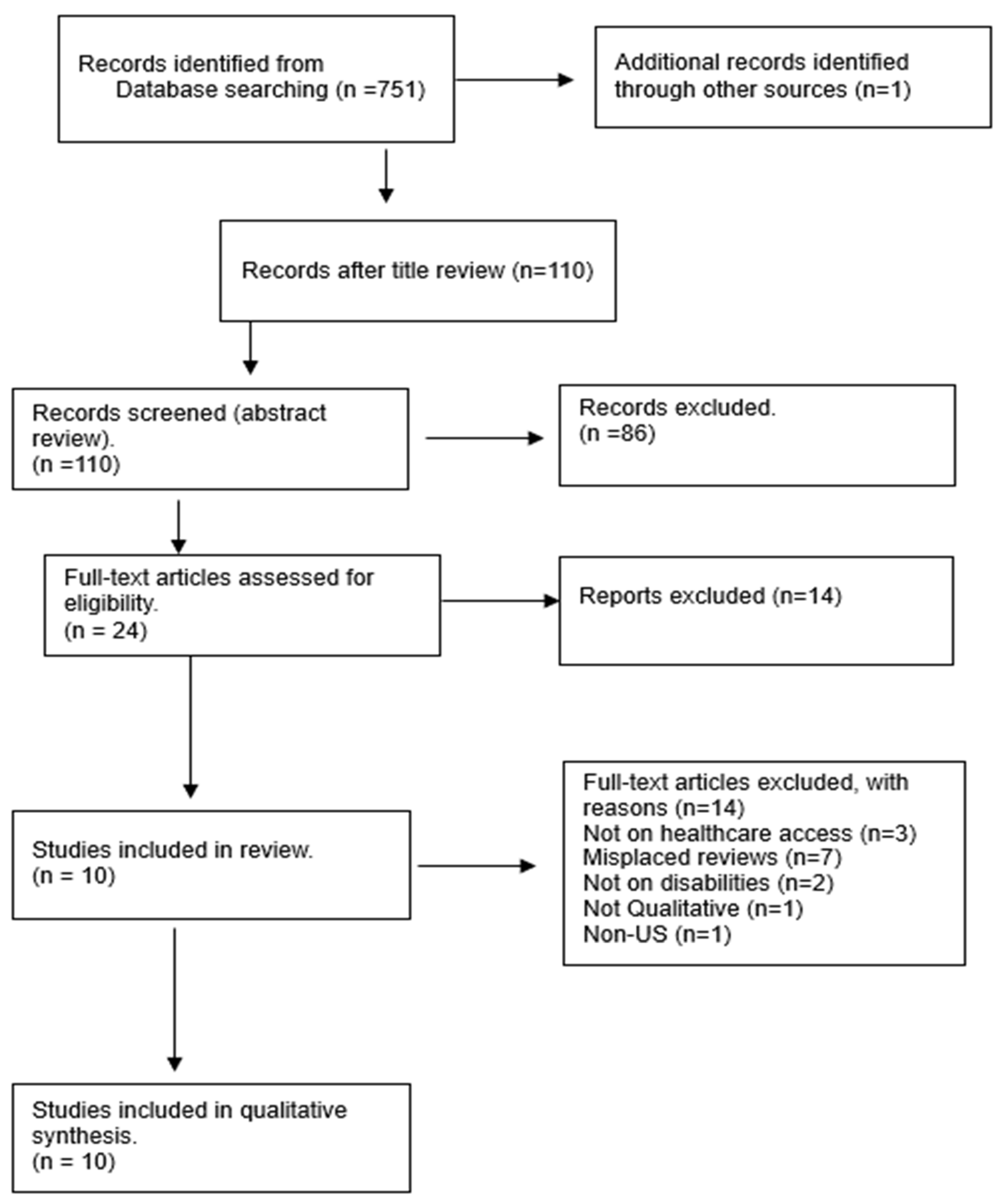
3.3. Search Results, Review, and Selection Criteria
3.4. Data Extraction, Analysis, and Quality
4. Results
4.1. Attributes of Sample Studies
4.2. Theme 1: Structural Barriers
4.2.1. Bureaucracy and Complexity of the System
4.2.2. Healthcare Cost
4.2.3. Transportation Challenges
4.2.4. Information and Communication Gaps
4.2.5. Long Wait Times
4.2.6. Lack of Integrated Services
4.3. Theme 2: Cultural and Personal Barriers
4.3.1. Cultural Beliefs, Denial, and Trust
4.3.2. Stigma and Discrimination
4.3.3. Awareness and Language Gaps
4.3.4. Lack of Social Support
4.4. Theme 3: Facilitators of Access to Healthcare
4.4.1. Immediate Family and Relatives
4.4.2. Community Health Centers
4.4.3. Social Workers’ Support
5. Discussion
5.1. Policy and Practice Implications
5.2. Limitations
5.2.1. Limited Literature to Synthesize
5.2.2. Contextual Limitations
5.2.3. Demographic Limitations
5.2.4. The Interruption of COVID-19
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bolter, J. Explainer: Who Is An Immigrant? 2019. Available online: https://www.migrationpolicy.org/sites/default/files/Explainer-WhoIsAnImmigrant-PRINT-Final.pdf (accessed on 9 July 2024).
- United Nations. General Assembly Convention on the Rights of Persons with Disabilities: Resolution/Adopted by the General Assembly, 2007, A/RES/61/106. 2007. Available online: https://www.un.org/en/development/desa/population/migration/generalassembly/docs/globalcompact/A_RES_61_106.pdf (accessed on 9 July 2024).
- Government of Canada. 2011 Census of Population—Data Products. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/index-eng.cfm (accessed on 9 July 2024).
- Paola, E.; Dulce, G. Urban Institute. Available online: https://www.urban.org/sites/default/files/2022-04/Being%20an%20Immigrant%20with%20Disabilities.pdf (accessed on 9 July 2024).
- Waldman, K.; Koyanagi, A.; Wang, J.S.-H.; Ko, J.; DeVylder, J.; Oh, H. Acculturative stress, disability, and health treatment utilization among Asian and Latin American immigrants in the United States. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 1275–1284. [Google Scholar] [CrossRef]
- Aceron, S.; Savage, T.A. Factors Affecting the Adjustment to Disability for New Immigrants. Top. Stroke Rehabil. 2004, 11, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Tarraf, W.; Mahmoudi, E.; Dillaway, H.E.; González, H.M. Health spending among working-age immigrants with disabilities compared to those born in the US. Disabil. Health J. 2016, 9, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Mirza, M.; Luna, R.; Mathews, B.; Hasnain, R.; Hebert, E.; Niebauer, A.; Mishra, U.D. Barriers to healthcare access among refugees with disabilities and chronic health conditions resettled in the US Midwest. J. Immigr. Minor. Health 2014, 16, 733–742. [Google Scholar] [CrossRef]
- Abdullah, F.; Zhang, Y.; Lardaro, T.; Black, M.; Colombani, P.M.; Chrouser, K.; Pronovost, P.J.; Chang, D.C. Analysis of 23 million US hospitalizations: Uninsured children have higher all-cause in-hospital mortality. J. Public Health 2010, 32, 236–244. [Google Scholar] [CrossRef]
- Singh, G.K.; Lin, S.C. Marked Ethnic, Nativity, and Socioeconomic Disparities in Disability and Health Insurance among US Children and Adults: The 2008–2010 American Community Survey. BioMed Res. Int. 2013, 2013, e627412. [Google Scholar] [CrossRef] [PubMed]
- Newbold, B. The short-term health of Canada’s new immigrant arrivals: Evidence from LSIC. Ethn. Health 2009, 14, 315–336. [Google Scholar] [CrossRef] [PubMed]
- Mirza, M.; Heinemann, A.W. Service needs and service gaps among refugees with disabilities resettled in the United States. Disabil. Rehabil. 2012, 34, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Peterson-Besse, J.J.; Walsh, E.S.; Horner-Johnson, W.; Goode, T.D.; Wheeler, B. Barriers to health care among people with disabilities who are members of underserved racial/ethnic groups: A scoping review of the literature. Med. Care 2014, 52, S51–S63. [Google Scholar] [CrossRef] [PubMed]
- Alsharaydeh, E.A.; Alqudah, M.; Lee, R.L.T.; Chan, S.W.-C. Challenges, Coping, and Resilience Among Immigrant Parents Caring for a Child With a Disability: An Integrative Review. J. Nurs. Scholarsh. 2019, 51, 670–679. [Google Scholar] [CrossRef]
- Thomson, M.S.; Chaze, F.; George, U.; Guruge, S. Improving Immigrant Populations’ Access to Mental Health Services in Canada: A Review of Barriers and Recommendations. J. Immigr. Minor. Health 2015, 17, 1895–1905. [Google Scholar] [CrossRef] [PubMed]
- Reihani, A.R.; Zimmerman, H.G.; Fernando, N.; Saunders, D.R.; Edberg, M.; Carter, E. Barriers and facilitators to improving access to healthcare for recently resettled Afghan refugees: A transformative qualitative study. J. Health Soc. Sci. 2021, 6, 59–72. [Google Scholar]
- Finfgeld-Connett, D. A Guide to Qualitative Meta-Synthesis; Routledge: New York, NY, USA, 2018; Available online: https://api.taylorfrancis.com/content/books/mono/download?identifierName=doi&identifierValue=10.4324/9781351212793&type=googlepdf (accessed on 9 May 2024).
- Béland, D.; Marchildon, G.P.; Medrano, A.; Rocco, P. Policy feedback, varieties of federalism, and the politics of health-care funding in the United States, Mexico, and Canada. Polit. Policy 2024, 52, 51–69. [Google Scholar] [CrossRef]
- Berchick, E.R.; Barnett, J.C.; Upton, R.D. Health Insurance Coverage in the United States: 2018. 2019. Available online: https://www.census.gov/library/publications/2019/demo/p60-267.html (accessed on 15 April 2024).
- Gauld, R.; Burgers, J.; Dobrow, M.; Minhas, R.; Wendt, C.; Cohen, A.B.; Luxford, K. Healthcare system performance improvement: A comparison of key policies in seven high-income countries. J. Health Organ. Manag. 2014, 28, 2–20. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.B.; Hartman, M.; Lassman, D.; Catlin, A. The National Health Expenditure Accounts Team National Health Care Spending In 2019: Steady Growth For The Fourth Consecutive Year: Study examines national health care spending for 2019. Health Aff. 2021, 40, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Vankar, P. Topic: Health Care System in Canada. Available online: https://www.statista.com/topics/10006/health-care-system-in-canada/ (accessed on 2 November 2024).
- Flood, C.M.; Thomas, B.; McGibbon, E. Canada’s primary care crisis: Federal government response. Healthc. Manag. Forum 2023, 36, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Sonia, K.; Cecile, R.; Marie, M.; Lucie, N. The Universality of the Canadian Health Care System in Question: Barriers to Services for Immigrants and Refugees. Available online: https://www.researchgate.net/publication/254191735_The_Universality_of_the_Canadian_Health_Care_System_in_Question_Barriers_to_Services_for_Immigrants_and_Refugees (accessed on 2 November 2024).
- Finfgeld-Connett, D. Generalizability and transferability of meta-synthesis research findings. J. Adv. Nurs. 2010, 66, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Finfgeld-Connett, D. Intimate Partner Abuse Among Older Women: Qualitative Systematic Review. Clin. Nurs. Res. 2014, 23, 664–683. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Hamidi, F.; Karachiwalla, Z. Structural accessibility barriers and service gaps facing refugees with disabilities in the United States. J. Enabling Technol. 2022, 16, 189–203. [Google Scholar] [CrossRef]
- Khanlou, N.; Haque, N.; Sheehan, S.; Jones, G. “It is an Issue of not Knowing Where to Go”: Service Providers’ Perspectives on Challenges in Accessing Social Support and Services by Immigrant Mothers of Children with Disabilities. J. Immigr. Minor. Health 2015, 17, 1840–1847. [Google Scholar] [CrossRef] [PubMed]
- Khanlou, N.; Haque, N.; Mustafa, N.; Vazquez, L.M.; Mantini, A.; Weiss, J. Access Barriers to Services by Immigrant Mothers of Children with Autism in Canada. Int. J. Ment. Health Addict. 2017, 15, 239–259. [Google Scholar] [CrossRef]
- Rivard, M.; Millau, M.; Magnan, C.; Mello, C.; Boulé, M. Snakes and ladders: Barriers and facilitators experienced by immigrant families when accessing an autism spectrum disorder diagnosis. J. Dev. Phys. Disabil. 2019, 31, 519–539. [Google Scholar] [CrossRef]
- Fellin, M.; Desmarais, C.; Lindsay, S. An examination of clinicians’ experiences of collaborative culturally competent service delivery to immigrant families raising a child with a physical disability. Disabil. Rehabil. 2015, 37, 1961–1969. [Google Scholar] [CrossRef] [PubMed]
- Sritharan, B.; Koola, M.M. Barriers faced by immigrant families of children with autism: A program to address the challenges. Asian J. Psychiatry 2019, 39, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.R.; Miguel, J.; Trejos, J. ASD Diagnosis and Treatment Experiences Among Mexican Heritage Families. J. Autism Dev. Disord. 2023, 53, 1017–1033. [Google Scholar] [CrossRef] [PubMed]
- Bogenschutz, M. “We Find a Way”: Challenges and Facilitators for Health Care Access Among Immigrants and Refugees With Intellectual and Developmental Disabilities. Med. Care 2014, 52, S64–S70. [Google Scholar] [CrossRef] [PubMed]
- Son, E.; Moring, N.S.; Igdalsky, L.; Parish, S.L. Navigating the health-care system in community: Perspectives from Asian immigrant parents of children with special health-care needs. J. Child Health Care 2018, 22, 251–268. [Google Scholar] [CrossRef]
- Decoteau, C.L. Learning to See Otherwise—Claire Laurier Decoteau, 2017. Available online: https://journals.sagepub.com/doi/abs/10.1177/1466138115592413 (accessed on 25 March 2024).
- Welterlin, A.; LaRue, R.H. Serving the needs of immigrant families of children with autism. Disabil. Soc. 2007, 22, 747–760. [Google Scholar] [CrossRef]
- Fisher, H.; Atzil-Slonim, D.; Bar-Kalifa, E.; Rafaeli, E.; Peri, T. Emotional experience and alliance contribute to therapeutic change in psychodynamic therapy. Psychotherapy 2016, 53, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Filler, T.; Jameel, B.; Gagliardi, A.R. Barriers and facilitators of patient centered care for immigrant and refugee women: A scoping review. BMC Public Health 2020, 20, 1013. [Google Scholar] [CrossRef] [PubMed]
- Arfa, S.; Solvang, P.K.; Berg, B.; Jahnsen, R. Disabled and immigrant, a double minority challenge: A qualitative study about the experiences of immigrant parents of children with disabilities navigating health and rehabilitation services in Norway. BMC Health Serv. Res. 2020, 20, 134. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zeng, W.; Wang, Y.; Magaña, S. Barriers to Service Access for Immigrant Families of Children With Developmental Disabilities: A Scoping Review. Intellect. Dev. Disabil. 2022, 60, 382–404. [Google Scholar] [CrossRef] [PubMed]
- Tefera, G.M.; Yu, M. Immigrant Women’s Access to Healthcare Services in the United States: A Qualitative Meta-Synthesis. J. Soc. Serv. Res. 2022, 48, 285–299. [Google Scholar] [CrossRef]
- Aborode, A.T.; Lawal, L.; Agwuna, F.O.; Adewunmi, R.O.; Ubechu, S.C.; Badri, R. Health disparities among illegal immigrants and homeless people in the USA: A struggle within. IJS Glob. Health 2023, 6, e0362. [Google Scholar] [CrossRef]
- Gui, X.; Chen, Y.; Pine, K.H. Navigating the Healthcare Service “Black Box”: Individual Competence and Fragmented System. Proc. ACM Hum.-Comput. Interact. 2018, 2, 61:1–61:26. [Google Scholar] [CrossRef]
- Pandey, M.; Maina, R.G.; Amoyaw, J.; Li, Y.; Kamrul, R.; Michaels, C.R.; Maroof, R. Impacts of English language proficiency on healthcare access, use, and outcomes among immigrants: A qualitative study. BMC Health Serv. Res. 2021, 21, 741. [Google Scholar] [CrossRef] [PubMed]
- Zghal, A.; El-Masri, M.; McMurphy, S.; Pfaff, K. Exploring the Impact of Health Care Provider Cultural Competence on New Immigrant Health-Related Quality of Life: A Cross-Sectional Study of Canadian Newcomers. J. Transcult. Nurs. 2021, 32, 508–517. [Google Scholar] [CrossRef]
- Cabieses, B.; Belo, K.; Calderón, A.C.; Rada, I.; Rojas, K.; Araoz, C.; Knipper, M. The impact of stigma and discrimination-based narratives in the health of migrants in Latin America and the Caribbean: A scoping review. Lancet Reg. Health–Am. 2024, 40, 100660. [Google Scholar] [CrossRef] [PubMed]
- Jacquez, F.; Vaughn, L.; Zhen-Duan, J.; Graham, C. Health Care Use and Barriers to Care among Latino Immigrants in a New Migration Area. J. Health Care Poor Underserved 2016, 27, 1761–1778. [Google Scholar] [CrossRef] [PubMed]
- King, G.; Meyer, K. Service integration and co-ordination: A framework of approaches for the delivery of co-ordinated care to children with disabilities and their families. Child Care Health Dev. 2006, 32, 477–492. [Google Scholar] [CrossRef] [PubMed]
- Lynnerup, C.; Rossing, C.; Sodemann, M.; Ryg, J.; Pottegård, A.; Nielsen, D. Health care professionals’ perspectives on medication safety among older migrants with cognitive impairment exposed to polypharmacy—A qualitative explorative study. Explor. Res. Clin. Soc. Pharm. 2022, 5, 100128. [Google Scholar] [CrossRef]
- Beach, M.C.; Price, E.G.; Gary, T.L.; Robinson, K.A.; Gozu, A.; Palacio, A.; Smarth, C.; Jenckes, M.W.; Feuerstein, C.; Bass, E.B.; et al. Cultural Competency: A Systematic Review of Health Care Provider Educational Interventions. Med. Care 2005, 43, 356–373. [Google Scholar] [CrossRef]
- Kalich, A.; Heinemann, L.; Ghahari, S. A Scoping Review of Immigrant Experience of Health Care Access Barriers in Canada. J. Immigr. Minor. Health 2016, 18, 697–709. [Google Scholar] [CrossRef] [PubMed]
- Handtke, O.; Schilgen, B.; Mösko, M. Culturally competent healthcare—A scoping review of strategies implemented in healthcare organizations and a model of culturally competent healthcare provision. PLoS ONE 2019, 14, e0219971. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | Explanation/Rationale |
|---|---|---|
| Target population and focus: IWDs | Non-immigrant population Not related to disability and access to healthcare | The focus of this qualitative meta-synthesis was to explore the experiences and perspectives of IWDs |
| Studies performed in the U.S. and Canada | To maintain contextual relevance | |
| Qualitative approach | Quantitative or mixed study | The project is a qualitative meta-synthesis |
| Articles written in English | The research team spoke English | |
| Published between 2013 and 2024 | To focus on findings within the last ten years | |
| Research reports of original research | Literature, systematic reviews, and commentaries | To understand and synthesize actual real-life experiences and perspectives of IWDs |
| Author | Location | Purpose | Target Population | Sample | Design/Method |
|---|---|---|---|---|---|
| [28] | Baltimore | “The purpose of the scoping study was to understand the experiences of refugees with disabilities” (p. 189). | Refugees and migrants and their families | 6 | Snowball sampling, interviews, and semi-structured interviews. |
| [29] | Toronto | “The objectives of the Mothers Project were to understand the social support experiences and service needs of immigrant mothers of children with disabilities, and to investigate service providers’ perspectives on the challenges faced by immigrant mothers in accessing social support and services” (p. 1841). | Health service providers | 27 | Single-stage purposive sampling strategy and in-depth interviews. |
| [30] | Canada | “This paper presents findings from a larger study, Mothers Project, which explored the perspectives of mothers and service providers regarding social support needs, challenges and experiences of immigrant mothers of children with disabilities in Toronto, Canada” (p. 242). | Immigrant mothers of children with autism | 21 | Interviews. |
| [31] | Quebec | “The objectives of the present study were as follows: to (1) document the obstacles experienced by immigrant families in obtaining an ASD diagnosis for their child, (2) document the factors that facilitated their access to a diagnosis, (3) identify prevailing attitudes toward ASD in participants’ culture of origin, and (4) record the advice that participants would give to other immigrant families in their own trajectory to obtain a diagnosis” (p. 521). | Immigrant families | 24 | Semi-structured interviews using a sociodemographic questionnaire. |
| [32] | Ontario | “To examine the barriers and facilitators to health and social service access and utilization for immigrant parents raising a child with a physical disability, in order to understand their specific needs and experiences of care” (p. 135). | First-generation immigrants from Asia, Africa, and the Caribbean | 5 | Semi-structured interviews were analyzed using grounded theory. |
| [8] | Chicago | “There is a need to explore this population’s access to appropriate healthcare services in order to identify service disparities and improve interventions” (p. 733). | Disabled and chronically ill refugees | 18 | Community-based participatory research, semi-structured key informant interviews, and community meetings. |
| [33] | Toronto | “The objectives of this article are (1) to understand the barriers that immigrant families of children with ASD face and (2) to describe a culturally sensitive program model to address the barriers and provide targeted and accessible resources to these immigrant families” (p. 53). | Immigrants with ASD | 21 | Literature review. |
| [34] | U.S. | “To understand the ASD diagnosis and treatment pathways for U.S. families” (p. 1017). | Mexican-heritage mothers of children with ASD | 38 | Multiple-case design. |
| [35] | U.S. | “This qualitative study seeks to discover the particular challenges that IWDs face when accessing health care and the facilitating factors that assist them in this process” (p. S64). | Immigration from three communities | 9 | Purposive sampling, Multicase study design, interviews, and participant observation. |
| [36] | U.S. | “This study aimed to explore how Asian immigrant parents of CSHCNs view their child’s healthcare access, quality, and utilization” (p. 251). | Children with special healthcare needs | 22 |
Semi-structured, standardized interview guided by grounded theory analysis. |
| Checklist | Study | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| [28] | [29] | [30] | [31] | [32] | [12] | [33] | [34] | [35] | [36] | |
| Was there a clear statement of the aims of the research? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Is a qualitative methodology appropriate? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the research design appropriate to address the aims of the research? | Yes | Yes | Yes | Yes | Yes | Yes | Not applicable | Yes | Yes | Yes |
| Was the recruitment strategy appropriate to the aims of the research? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the data collected in a way that addressed the research issue? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Has the relationship between the researcher and participants been adequately considered? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Have ethical issues been taken into consideration? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Was the data analysis sufficiently rigorous? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Is there a clear statement of findings? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| How valuable is the research? | Very valuable | Very valuable | Very valuable | Very valuable | Very valuable | Very valuable | Very valuable | Very valuable | Very valuable | Very valuable |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngondwe, P.; Tefera, G.M. Barriers and Facilitators of Access to Healthcare Among Immigrants with Disabilities: A Qualitative Meta-Synthesis. Healthcare 2025, 13, 313. https://doi.org/10.3390/healthcare13030313
Ngondwe P, Tefera GM. Barriers and Facilitators of Access to Healthcare Among Immigrants with Disabilities: A Qualitative Meta-Synthesis. Healthcare. 2025; 13(3):313. https://doi.org/10.3390/healthcare13030313
Chicago/Turabian StyleNgondwe, Ponsiano, and Gashaye Melaku Tefera. 2025. "Barriers and Facilitators of Access to Healthcare Among Immigrants with Disabilities: A Qualitative Meta-Synthesis" Healthcare 13, no. 3: 313. https://doi.org/10.3390/healthcare13030313
APA StyleNgondwe, P., & Tefera, G. M. (2025). Barriers and Facilitators of Access to Healthcare Among Immigrants with Disabilities: A Qualitative Meta-Synthesis. Healthcare, 13(3), 313. https://doi.org/10.3390/healthcare13030313