Abstract
Objectives: Evidence regarding the impacts of systemic inflammation on nocturnal sleep in advanced cancer patients is limited. We determined the association of serum C-reactive protein (CRP) levels with sleep in patients with non-imminent and those with imminent death. Methods: This was a secondary analysis of an observational study conducted in patients newly referred to a palliative care unit. Nocturnal sleep was assessed based on the “sleeping time” measured using a sheet-type non-wearable sensor. Patients were divided into long-survival and short-survival groups depending on the median survival (11 days), and within each group, the patients were categorized according to CRP levels: low (<1 mg/dL), moderate (1–10 mg/dL), and high (≥10 mg/dL). To evaluate correlations between CRP levels and sleeping time, binomial logistic analysis was performed. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Results: A total of 535 patients were included in the main analysis. In the long-survival group (n = 273), the high-CRP patients had significantly longer sleeping time than the low-CRP patients (OR 2.81, 95% CI 1.19–6.65, p-value 0.019), whereas there were no significant correlations in the short-survival group (n = 262). Conclusions: Higher CRP levels were associated with longer sleeping time in patients with non-imminent death, whereas there were no correlations in patients whose death was imminent. The clinical implications of serum CRP levels appear to vary with life expectancy in terminally ill patients with cancer. Further research is necessary to verify the present findings.
1. Introduction
Crosstalk between tumor and host immune system produces pro-inflammatory cytokines, leading to systemic inflammation [1,2,3,4,5,6]. Evidence suggests that systemic inflammation is involved in the mechanisms responsible for cancer cachexia [1,2,3,4,5,6]. In patients with cancer cachexia, pro-inflammatory cytokines are amplified through alterations in the central nervous system (CNS), particularly the hypothalamic–pituitary–adrenal (HPA) axis, causing sympathetic nerve dominance [7,8,9,10]. In addition, activation of the HPA axis and sympathetic nerve dominance provoke muscle atrophy and sleep disorders and insufficiencies through the secretion of glucocorticoids by the adrenal gland [7,11]. Thus, systemic inflammation generates a variety of physical and psychological symptoms in individuals with advanced cancer. Multiple events appear to be induced by CNS inflammation in individuals affected by cancer cachexia [12].
Previous studies reported that pain and symptoms have frequently been detected in cancer patients with systemic inflammation [13,14,15,16,17,18,19]. Moreover, psychological symptoms are more frequently observed in cachectic patients with cancer than in non-cachectic patients [20]. Furthermore, serum C-reactive protein (CRP) levels have been considered as a surrogate of systemic inflammation, which was associated with survival, daily activities, and physical and psychological symptoms in individuals with incurable advanced cancer in palliative care settings [15,19,21,22,23,24,25,26].
However, there is insufficient evidence to show that systemic inflammation contributes to the genesis of psychological symptoms through alterations in the CNS/HPA axis in patients with advanced cancer [12,20]. Moreover, there is limited evidence regarding the negative impacts of systemic inflammation on the status of night sleep in this population, although sleep disorders and insufficiencies are associated with activation of the HPA axis and sympathetic nerve dominance [11]. Furthermore, no reports have shown whether the clinical implications of serum CRP levels vary with life expectancy in patients with advanced cancer.
Therefore, we determined the association of serum CRP levels with night sleep (i.e., total sleeping time and restlessness were measured using a sheet-type non-wearable sensor) in non-imminent death and imminent death patients with advanced cancer who were admitted to a palliative care unit. Furthermore, we also investigated the relationship between serum CRP levels and the severity of symptoms, drug use (opioid oral morphine, benzodiazepine, and/or psychotropic drugs), and the patients’ delirium.
2. Participants and Methods
2.1. Sites and Participants
Herein, a secondary analysis of an observational study with a retrospective design was performed. The study was conducted in a palliative care unit with 27 beds (located in a cancer-designated hospital with 940 beds) in Japan between March 2019 and December 2022. The aim of the study was to determine the effectiveness of a sheet-type non-wearable sensing device in terminally ill patients with cancer, who had a survival of days to weeks [27].
All patients meeting the eligibility criteria were enrolled. The inclusion criteria were (1) patients admitted to a palliative care unit, (2) patients aged ≥18 years, and (3) patients diagnosed with locally advanced or metastatic cancer. The exclusion criteria were (1) patients who were scheduled to be discharged within one week, (2) patients or family members who refused to participate in the study, (3) poor patient condition that did not allow for transfer to the bed with a Nemuri SCAN device, and (4) patients who were discharged alive.
2.2. Measurements
The status of night sleep was assessed based on the sleeping time and activity scores measured using a sheet-type non-wearable sensor (length, 28.4 cm; width, 77.5 cm; thickness, 1.8 cm), namely a Nemuri SCAN device (Paramount Bed Co., Ltd., Tokyo, Japan). The highly sensitive pressure sensor is placed under a mattress and detects the movement of patients lying on top of the mattress. Nemuri SCAN identifies whether a subject is asleep or awake using movement data to measure total sleeping time. Nemuri SCAN also analyses the intensity and frequency of body movements every minute, which are recorded as activity scores, excluding breathing and heartbeats. Activity scores range from 0 to 960 scores/min because data are sampled at 16 Hz (16 times per second). Average activity scores (i.e., scores/minute) are used for analyses. The accuracy of these assessments has been validated, showing that these parameters can serve as objective measurements of the status of night sleep. Activity scores evaluated using a sheet-type sensor can assess not only agitation but also sedation levels [27,28].
A calibrated version of the Nemuri SCAN device was used in the study. We set up Nemuri SCAN under the participants’ bed mattresses and obtained data on their sleeping or awake status and activities every minute for 24 h from the day of admission to the day of discharge. The data were recorded on a storage medium built into the device. Data on patient sleeping status (i.e., total sleeping time and activity score) were extracted from the device by one of the researchers (ST), who was blinded to the clinical data. We exclusively used Nemuri SCAN data obtained during the night (23:00–6:00) for this study.
Physicians in the palliative care unit extracted data on patient characteristics from the medical records upon admission. They also collected the results of blood tests performed within three days after admission. When no data on blood was collected, physicians recorded the latest blood test results obtained before death. They also retrieved data on the severities of symptoms (i.e., pain, dyspnea, fatigue, and nausea) assessed using the Integrated Palliative care Outcome Scale (IPOS) [29,30], opioid oral morphine milligram equivalent based on the Clinical Guidelines from the Japanese Society of Palliative Medicine [31], presence of benzodiazepine and/or psychotropic drugs, and scores of the modified Richmond Agitation–Sedation Scale (mRASS) [32,33] from three days, one week, two weeks, three weeks, and four weeks prior to a patient’s death. The mRASS scores were recorded by nurses in the palliative care unit three times per day (i.e., 8:30–17:00, 17:00–1:00, and 1:00–8:30), documented on the medical record within the routine practice. Both the IPOS and mRASS were translated into Japanese, which were validated in patients with advanced cancer in palliative care settings [34,35]. The nurses were blinded to the Nemuri SCAN data of participating patients.
A database for this secondary analysis was created to pair the blood test results with Nemuri SCAN data obtained during the night (23:00–6:00) on the same day. Furthermore, data on symptoms, opioid oral morphine milligram equivalent, benzodiazepine and/or psychotropic drugs, and mRASS scores obtained within three days of the given day were considered.
We hypothesized that total sleeping time shortens and restlessness worsens as systemic inflammation becomes more severe in patients with imminent death compared to those with non-imminent death.
2.3. Statistical Analysis
Patient characteristics were presented as numbers (%) or medians (interquartile range), where appropriate. Participants were divided into three groups according to their serum levels of CRP: (1) low (CRP levels < 1 mg/dL), (2) moderate (1 ≤ CRP levels < 10 mg/dL), and (3) high (CRP levels ≥ 10 mg/dL). These cutoffs were predefined based on a clinical rationale and previous clinical research [15,19,36,37]. Comparisons among the three categories were made using the Kruskal–Wallis test or chi-squared test, where appropriate.
To examine differences in the clinical implications of CRP levels based on survival time, patients above and below the median survival (11 days) were divided into two groups because of no validated cutoff value: long-survival group (≥11 days) and short-survival group (≤10 days). After that, to evaluate correlations between CRP levels and sleeping time and associations between CRP levels and activity scores in both the long- and short-survival groups, binomial logistic analysis was performed. Dependent variables (i.e., sleeping time and activity scores) were divided into two groups using their respective median values, because no appropriate cutoff values have been shown. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated after adjusting for independent variables considered to be potential risk factors for affecting night sleep in patients with advanced cancer, including age, sex, primary tumor site, opioid oral morphine milligram equivalent (per 10 mg), benzodiazepine and/or psychotropic drugs (yes or no), and CRP level (three categories). We entered these variables into the logistic regression models because they were considered potential confounding variables [19].
All results were considered to be significant if the p-value was less than 0.05. All analyses were performed using SPSS software version 22.0.
3. Results
A total of 1209 patients were admitted to the palliative care unit during the observation period. Among them, 2 declined consent, 25 were excluded due to technical issues (e.g., unable to be transferred to the bed with Nemuri SCAN because of their poor condition), and 71 were discharged alive. Thus, a total of 1111 patients were enrolled in the original study. Of these patients, 568 were excluded due to a lack of Nemuri SCAN and CRP data on the same day, and 2 were excluded because data were obtained on the day that continuous sedation was initiated. Finally, 541 patients were included in this secondary analysis (Figure 1).
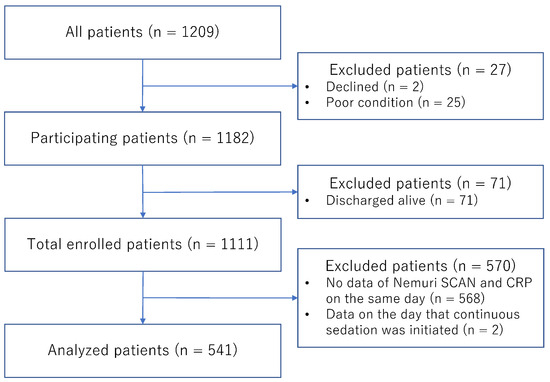
Figure 1.
Study diagram. CRP, C-reactive protein.
Patient characteristics are presented in Table 1. The median age was 75 years old. The proportion of males was 55.8%. The top three sites of primary cancer were the upper and lower gastrointestinal tracts (24.8%), liver, biliary system, and pancreas (21.8%), and lung (21.1%). Furthermore, 42.0% of the patients had lung metastases, and 37.2% had liver metastases.

Table 1.
Patient Characteristics (n = 541).
According to their serum CRP levels, the 541 patients were categorized as low (n = 66), moderate (n = 290), and high (n = 185). Relationships between CRP levels, symptoms, and other variables in all patients are shown in Table 2. Higher CRP levels were significantly associated with more severe pain and more opioid use (p = 0.014 and p < 0.001, respectively). Moreover, relationships between CRP levels and Nemuri SCAN parameters in all patients are shown in Table 3. The higher the CRP levels, the longer the sleeping time and the lower the activity scores appeared to be, but no significant differences were found. However, higher CRP levels were correlated with significantly higher heart rates (p < 0.001).
Table 2.
Relationships between CRP levels and symptoms, including other variables.
Table 3.
Relationships between CRP levels and Nemuri SCAN parameters.
The relationship between the number of patients and sleeping time, and the relationship between the number of patients and activity scores in all patients are illustrated in Figure 2 and Figure 3, respectively. As the sleeping time decreased, the number of patients decreased. Furthermore, as the activity scores increased, the number of patients decreased.
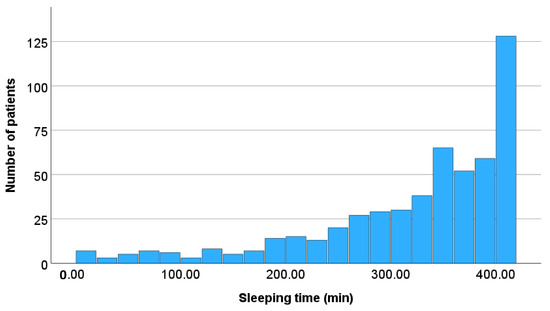
Figure 2.
Relationship between the number of patients and daily sleeping time. As the sleeping time decreased, the number of patients decreased.
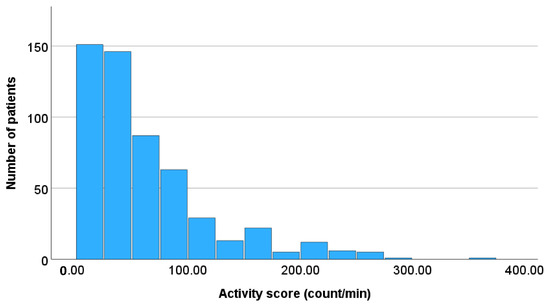
Figure 3.
Relationship between the number of patients and daily activity scores. As the activity scores increased, the number of patients decreased.
Results of the multivariate logistic regression analysis are presented in Table 4, showing the associations between CRP levels and sleeping time in the long-survival group (n = 273) and short-survival group (n = 262). Patients with high CRP levels (≥10 mg/dL) had significantly longer night sleeping time than those with low CRP levels (<1 mg/dL) in patients who survived more than 11 days (OR 2.81, 95% CI 1.19–6.65, p-value 0.019). However, there were no significant correlations in patients who survived less than 10 days.
Table 4.
Association between CRP levels and total sleeping time.
Results of the multivariate logistic regression analysis are also presented in Table 5, showing the associations between CRP levels and activity scores in the long-survival group (n = 273) and short-survival group (n = 262). Patients with high CRP levels (≥10 mg/dL) tended to have less activity at night than those with low CRP levels (<1 mg/dL) in patients who survived more than 11 days (OR 0.46, 95% CI 0.20–1.08, p-value 0.076). However, there were no significant correlations in patients who survived less than 10 days.
Table 5.
Association between CRP levels and activity scores.
4. Discussion
To date, there is limited evidence on the negative impacts of systemic inflammation on the status of night sleep in patients with advanced cancer. We determined the association of serum CRP levels with night sleep, considering survival time among terminally ill patients with cancer admitted to a palliative care unit. Our results showed that a higher CRP level (≥10 mg/dL) was significantly associated with longer sleeping time during the night in patients with longer survival time (≥11 days), but it was not significant for activity score during the night. Furthermore, there were no associations between CRP levels and sleeping time or activity scores in patients with shorter survival time (≤10 days). The findings implied that patients with non-imminent death were likely to be simply and highly affected by systemic inflammation, and that patients with impending death were bedridden regardless of systemic inflammation or delirious and restless due to factors other than systemic inflammation. However, these need to be verified in the future.
A previous study conducted on patients with advanced cancer admitted to palliative care units reported a significant association between a higher CRP level (≥10 mg/dL) and the occurrence of delirium [19], suggesting that patients with systemic inflammation tend to have restlessness due to delirium. Moreover, a prior study revealed that the activity scores reflecting restlessness measured using the Nemuri SCAN were significantly and positively associated with the levels of terminal agitation, or delirium [27]. Against our expectations, however, there was no association between CRP levels and activity scores in patients with impending death in this study. A secondary analysis of two randomized clinical trials conducted in palliative care units showed that cancer patients with end-of-life delirium were more restless between 15:00 and 23:00 [38], while this study used data obtained between 23:00 and 6:00. This may be one of the reasons why no associations were observed between CRP levels, sleeping time, and activity levels in patients in the dying phase.
Sickness behavior is considered a symptom cluster (e.g., fever, fatigue, drowsiness, nausea, anorexia, depression, anxiety, and cognitive impairment) caused by CNS inflammation, which is followed by systemic inflammation in animals [39]. CNS inflammation is directly induced by inflammatory mediators, such as pro-inflammatory cytokines, in individuals with sickness, and the CNS/HPA axis controls behavioral changes (e.g., decline in motivation, sleep disturbance, and cognitive impairment) through the immune system and the CNS in animals and humans [40]. Other phenotypes (e.g., increased catabolism, weight loss, and circadian rhythm disorders) are also related to sickness behavior through an integrated response of CNS inflammation and systemic inflammation [39,40]. Accordingly, there are many overlapping features between cancer cachexia and sickness behavior, and such phenomena are sustained and exacerbated by persistent CNS inflammation and systemic inflammation in patients with advanced cancer and those with infectious diseases. Hence, cancer cachexia may be understood in the context of sickness behavior, although there is limited evidence concerning the relationship between them. Clarifying this may be essential for explaining what cancer cachexia is and why we suffer from it [12]. In summary, there is an urgent need for further research to understand the underlying pathophysiology of systemic inflammation and its impact on the CNS/HPA axis and to develop effective treatments for physical and psychological symptoms, including anorexia, sleep disturbance, and delirium, among cachectic patients with cancer.
The present study has several strengths and limitations. The dataset was obtained from a large single-center prospective observational study, which contained robust clinical information and enabled an accurate analysis. However, this study was based on a secondary analysis, and approximately 50% of the original cohort was excluded. The main reason for this was that blood tests were not frequently performed in palliative care units. In addition, a database for this study was created to pair the blood test results with Nemuri SCAN data on the same day. Moreover, the findings of this study demonstrated that higher CRP levels were significantly associated with longer night sleeping time in patients with non-imminent death. However, the association can be reverse causal, or even bidirectional. This study did not examine the causes of elevated CRP levels, but it investigated the association of serum CRP levels with sleep disturbance. A serum CRP level is not a specific marker, but the clinical significance of CRP remains unchanged regardless of the reason for elevated CRP levels. According to previous studies, elevated CRP levels are undoubtedly a poor prognostic factor, regardless of their cause [15,19,21,22,23,24,25,26]. The causes are often complex and coexist (e.g., cancer cachexia, acute infection, chronic heart failure, and obesity), and it is difficult to detect a single factor in clinical practice. Additionally, it was impossible to assess other factors that may influence the associations between CRP and sleeping time or activities because potential confounders could not be identified. To investigate the causal mechanisms of serum CRP levels and sleep disturbance, it is necessary to stratify by CRP levels and adjust for potential confounders, including acute infection and chronic heart failure, in clinical studies. Changes in CRP levels are also very important in clinical practice. The survival cutoff value of 11 days has not been validated, but dividing patients receiving palliative care into two groups using ≥11 days and ≤10 days seems to be clinically acceptable. Furthermore, it was difficult to differentiate between a participant who was truly sleeping and one who was under some level of sedation induced by medication, including morphine, benzodiazepines, and psychotropic drugs, using the sleeping time and activity scores measured using just a sheet-type non-wearable sensor. The effectiveness of anti-inflammatory drugs and pain and symptom management in improving sleep status must be examined in the future. The results obtained should be confirmed in prospectively derived data on the patient cohort of interest who have complained of sleep disturbance, with appropriate outcomes assessed using objective and subjective parameters to translate research findings into clinical practice.
5. Conclusions
A higher CRP level was significantly associated with longer sleeping time during the night in patients whose death was less imminent, but it was not significant for activity score during the night. Furthermore, there were no correlations in patients whose death was imminent. The clinical implications of serum CRP levels appear to vary with life expectancy in terminally ill patients with cancer. Further research is necessary to verify the present findings and clarify their relevance in clinical assessment and management of sleep-related symptoms in palliative care practice.
Author Contributions
Conceptualization: K.A., K.I. and T.M.; Data curation: K.I., S.T., T.Y., S.M., M.Y., S.O. and S.I.; Formal analysis: K.A.; Funding acquisition: K.A., T.K. and T.M.; Investigation: K.A.; Methodology: K.A.; Project administration: T.K. and T.M.; Supervision: T.K. and T.M.; Visualization: K.A.; Writing—original draft: K.A.; Writing—review and editing: All authors. All authors have read and agreed to the published version of the manuscript.
Funding
The present study was supported by Paramount Bed Co., Ltd., which covered the costs of the Nemuri SCAN, data storage, wireless networks, and related construction. This study was also supported by JSPS KAKENHI Grant Number 22K11839.
Institutional Review Board Statement
The present study was performed following the ethical standards of the Helsinki Declaration and the ethical guidelines for medical and health research involving human subjects presented by the Ministry of Health, Labor, and Welfare in Japan [41]. The present study was approved by the local Institutional Review Board at Seirei Mikatahara Hospital on 22 December 2022 (approval number 22-53), and the requirement for written informed consent was waived based on national ethical guidelines.
Informed Consent Statement
An opt-out method was employed in the present study. All patients received detailed written information on this study from physicians and/or nurses. Patients declined participation at their discretion. A substitute decision-maker acted on the patient’s behalf when the patient was unable to decide.
Data Availability Statement
The datasets generated and analyzed in the present study are not publicly available because sharing is not explicitly covered by patient consent.
Acknowledgments
We are grateful to Satomi Okamura for her advice on the statistical analysis of this study and help in the preparation of the manuscript.
Conflicts of Interest
Authors Saori Toyota and Takamasa Kogure were employed by the Paramount Bed Co., Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Lippitz, B.E. Cytokine patterns in patients with cancer: A systematic review. Lancet Oncol. 2013, 14, 218–228. [Google Scholar] [CrossRef]
- Candido, J.; Hagemann, T. Cancer-related inflammation. J. Clin. Immunol. 2013, 33 (Suppl. S1), 79–84. [Google Scholar] [CrossRef]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Baracos, V.E.; Martin, L.; Korc, M.; Guttridge, D.C.; Fearon, K.C.H. Cancer-associated cachexia. Nat. Rev. Dis. Primers 2018, 4, 17105. [Google Scholar] [CrossRef] [PubMed]
- Olson, B.; Diba, P.; Korzun, T.; Marks, D.L. Neural Mechanisms of Cancer Cachexia. Cancers 2021, 13, 3990. [Google Scholar] [CrossRef]
- Stagikas, D.; Simos, Y.V.; Lakkas, L.; Filis, P.; Peschos, D.; Tsamis, K.I. The role of the hypothalamus in the development of cancer cachexia. Physiol. Behav. 2025, 295, 114909. [Google Scholar] [CrossRef]
- Simoes, E.; Uchida, R.; Nucci, M.P.; Duran, F.L.S.; Lima, J.D.C.C.; Gama, L.R.; Costa, N.A.; Otaduy, M.C.G.; Bin, F.C.; Otoch, J.P.; et al. Cachexia Alters Central Nervous System Morphology and Functionality in Cancer Patients. J. Cachexia Sarcopenia Muscle 2025, 16, e13742. [Google Scholar] [CrossRef]
- Zhu, X.A.; Starosta, S.; Ferrer, M.; Hou, J.; Chevy, Q.; Lucantonio, F.; Muñoz-Castañeda, R.; Zhang, F.; Zang, K.; Zhao, X.; et al. A neuroimmune circuit mediates cancer cachexia-associated apathy. Science 2025, 388, eadm8857. [Google Scholar] [CrossRef]
- Greenlund, I.M.; Carter, J.R. Sympathetic neural responses to sleep disorders and insufficiencies. Am. J. Physiol. Heart Circ. Physiol. 2022, 322, H337–H349. [Google Scholar] [CrossRef] [PubMed]
- Amano, K.; Hopkinson, J.; Baracos, V. Psychological symptoms of illness and emotional distress in advanced cancer cachexia. Curr. Opin. Clin. Nutr. Metab. Care 2022, 25, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Laird, B.J.A.; Scott, A.C.; Colvin, L.A.; McKeon, A.L.; Murray, G.D.; Fearon, K.C.H.; Fallon, M.T. Cancer pain and its relationship to systemic inflammation: An exploratory study. Pain 2011, 152, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Laird, B.J.; McMillan, D.C.; Fayers, P.; Fearon, K.; Kaasa, S.; Fallon, M.T.; Klepstad, P. The systemic inflammatory response and its relationship to pain and other symptoms in advanced cancer. Oncologist 2013, 18, 1050–1055. [Google Scholar] [CrossRef]
- Amano, K.; Maeda, I.; Morita, T.; Miura, T.; Inoue, S.; Ikenaga, M.; Matsumoto, Y.; Baba, M.; Sekine, R.; Yamaguchi, T.; et al. Clinical implications of C-reactive protein as a prognostic marker in advanced cancer patients in palliative care settings. J. Pain. Symptom Manag. 2016, 51, 860–867. [Google Scholar] [CrossRef]
- Paulsen, Ø.; Laird, B.; Aass, N.; Lea, T.; Fayers, P.; Kaasa, S.; Klepstad, P. The relationship between proinflammatory cytokines and pain, appetite and fatigue in patients with advanced cancer. PLoS ONE 2017, 12, e0177620. [Google Scholar] [CrossRef]
- Kwekkeboom, K.L.; Tostrud, L.; Costanzo, E.; Coe, C.L.; Serlin, R.C.; Ward, S.E.; Zhang, Y. The role of inflammation in the pain, fatigue, and sleep disturbance symptom cluster in advanced cancer. J. Pain. Symptom Manag. 2018, 55, 1286–1295. [Google Scholar] [CrossRef]
- Miranda, D.O.; Anatriello, E.; Azevedo, L.R.; Cordeiro, J.F.C.; Peria, F.M.; Flória-Santos, M.; Pereira-da-Silva, G. Elevated serum levels of proinflammatory cytokines potentially correlate with depression and anxiety in colorectal cancer patients in different stages of the antitumor therapy. Cytokine 2018, 104, 72–77. [Google Scholar] [CrossRef]
- Amano, K.; Hatano, Y.; Matsuda, Y.; Maeda, I.; Ishiki, H.; Miura, T.; Imai, K.; Hori, T.; Funaki, H.; Suzuki, K.; et al. C-reactive protein, delirium, and other psychological symptoms among patients with advanced cancer. JCSM Clin. Rep. 2020, 5, 42–51. [Google Scholar] [CrossRef]
- Yule, M.S.; Brown, L.R.; Skipworth, R.J.E.; Laird, B.J.A. Central neural mechanisms of cancer cachexia. Curr. Opin. Support. Palliat. Care 2024, 18, 138–144. [Google Scholar] [CrossRef]
- Kieler, M.; Kössler, P.; Milovic, M.; Meyer, E.; Križanová, K.; Kum, L.; Friedrich, A.; Masel, E.; Bauer, R.; Unseld, M. C-reactive protein and white blood cell count are adverse prognostic markers for patients with advanced cancer on parenteral nutrition in a palliative care unit setting: A retrospective cohort study. Palliat. Med. 2022, 36, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Westgaard, A.; Pirnat, A.; Hjermstad, M.J.; Aass, N.; Kaasa, S.; Dajani, O.F. Prognostic Value of Performance Status, Albumin, and CRP in Last-Line Chemotherapy for Pancreatic vs. Other Gastrointestinal Cancers-Simple Tools Matter. Curr. Oncol. 2024, 31, 5462–5471. [Google Scholar] [CrossRef] [PubMed]
- McGovern, J.; O’ROurke, F.; Will, S.; Nguyen, H.T.N.; Cranfield, E.; Maseland, C.; MacLeod, N.; Maclay, J.D.; Laird, B.J.; Dolan, R.D.; et al. The prevalence and prognostic value of systemic inflammation in good performance status patients with advanced, inoperable non-small cell lung cancer receiving palliative radiotherapy: Comparison of composite ratios and cumulative scores. Cancer Med. 2024, 13, e70139. [Google Scholar] [CrossRef] [PubMed]
- Yule, M.S.; Machado, A.M.; Brown, L.R.; Rocha, B.M.; Patton, R.; Sayers, J.; Munro, I.; Baxter, J.; McLuskie, A.; Lajolo, P.P.; et al. Dissecting the global leadership initiative on malnutrition criteria in advanced cancer: Reduced intake vs. inflammation. Clin. Nutr. ESPEN 2025, 67, 114–121. [Google Scholar] [CrossRef]
- Pumtako, C.; Dolan, R.D.; Fallon, M.; Sullivan, E.S.; Simmons, C.P.; Ryan, A.M.; McGovern, J.; Power, D.G.; Laird, B.J.; McMillan, D.C. The Global Leadership Initiative on Malnutrition (GLIM) inflammation criteria to predict survival in patients with advanced cancer: A prospective cohort study. Clin. Nutr. ESPEN 2025, 67, 344–352. [Google Scholar] [CrossRef]
- Vagnildhaug, O.M.; Habberstad, R.H.; Salvesen, Ø.; Balstad, T.R.; Bye, A.; Dajani, O.; Kaasa, S.; Klepstad, P.; Solheim, T.S. A comparison of inflammatory markers’ potential to predict weight loss in advanced cancer: A prospective observational study. J. Circ. Biomark. 2025, 14, 12–20. [Google Scholar] [CrossRef]
- Otani, H.; Yokomichi, N.; Imai, K.; Toyota, S.; Yamauchi, T.; Miwa, S.; Yuasa, M.; Okamoto, S.; Kogure, T.; Inoue, S.; et al. A Novel Objective Measure for Terminal Delirium: Activity Scores Measured by a Sheet-Type Sensor. J. Pain. Symptom Manag. 2024, 68, 246–254. [Google Scholar] [CrossRef]
- Kogure, T.; Shirakawa, S.; Shimokawa, M.; Masato, S.; Hosokawa, Y. Automatic sleep/wake scoring from body motion in bed: Validation of a newly developed sensor placed under a mattress. J. Physiol. Anthropol. 2011, 30, 103–109. [Google Scholar] [CrossRef]
- Collins, E.S.; Witt, J.; Bausewein, C.; Daveson, B.A.; Higginson, I.J.; Murtagh, F.E. A Systematic Review of the Use of the Palliative Care Outcome Scale and the Support Team Assessment Schedule in Palliative Care. J. Pain. Symptom Manag. 2015, 50, 842–853. [Google Scholar] [CrossRef]
- Schildmann, E.K.; Groeneveld, E.I.; Denzel, J.; Brown, A.; Bernhardt, F.; Bailey, K.; Guo, P.; Ramsenthaler, C.; Lovell, N.; Higginson, I.J.; et al. Discovering the hidden benefits of cognitive interviewing in two languages: The first phase of a validation study of the Integrated Palliative care Outcome Scale. Palliat. Med. 2016, 30, 599–610. [Google Scholar] [CrossRef]
- Mawatari, H.; Shinjo, T.; Morita, T.; Kohara, H.; Yomiya, K. Revision of Pharmacological Treatment Recommendations for Cancer Pain: Clinical Guidelines from the Japanese Society of Palliative Medicine. J. Palliat. Med. 2022, 25, 1095–1114. [Google Scholar] [CrossRef]
- Ely, E.W.; Truman, B.; Shintani, A.; Thomason, J.W.; Wheeler, A.P.; Gordon, S.; Francis, J.; Speroff, T.; Gautam, S.; Margolin, R.; et al. Monitoring sedation status over time in ICU patients: Reliability and validity of the Richmond Agitation-Sedation Scale (RASS). JAMA 2003, 289, 2983–2991. [Google Scholar] [CrossRef] [PubMed]
- Benítez-Rosario, M.A.; Castillo-Padrós, M.; Garrido-Bernet, B.; González-Guillermo, T.; Martínez-Castillo, L.P.; González, A. Appropriateness and reliability testing of the modified Richmond Agitation-Sedation Scale in Spanish patients with advanced cancer. J. Pain. Symptom Manag. 2013, 45, 1112–1119. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, H.; Miyashita, M.; Imai, K.; Miyamoto, S.; Otani, H.; Oishi, A.; Kizawa, Y.; Matsushima, E. Validation of the Integrated Palliative care Outcome Scale (IPOS)—Japanese Version. Jpn. J. Clin. Oncol. 2019, 49, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Morita, T.; Mori, M.; Yokomichi, N.; Fukuta, K. Development and linguistic validation of the Japanese version of the modified Richmond Agitation-Sedation Scale. Palliat. Care Res. 2016, 11, 331–336. (In Japanese) [Google Scholar] [CrossRef]
- Morley, J.J.; Kushner, I. Serum C-reactive protein levels in disease. Ann. N. Y. Acad. Sci. 1982, 389, 406–418. [Google Scholar] [CrossRef]
- Merker, M.; Felder, M.; Gueissaz, L.; Bolliger, R.; Tribolet, P.; Kägi-Braun, N.; Gomes, F.; Hoess, C.; Pavlicek, V.; Bilz, S.; et al. Association of Baseline Inflammation With Effectiveness of Nutritional Support Among Patients With Disease-Related Malnutrition: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e200663. [Google Scholar] [CrossRef]
- Admane, S.; Pasyar, S.; Bassett RJr Bruera, E.; Hui, D. Circadian rhythm in end-of-life delirium: A secondary analysis of two randomized controlled trials. J. Pain. Symptom Manag. 2025, 70, 131–139.e2. [Google Scholar] [CrossRef]
- Shakhar, K.; Shakhar, G. Why Do We Feel Sick When Infected—Can Altruism Play a Role? PLoS Biol. 2015, 13, e1002276. [Google Scholar] [CrossRef]
- Kelley, K.W.; Kent, S. The Legacy of Sickness Behaviors. Front. Psychiatry 2020, 11, 607269. [Google Scholar] [CrossRef]
- Eba, J.; Nakamura, K. Overview of the ethical guidelines for medical and biological research involving human subjects in Japan. Jpn. J. Clin. Oncol. 2022, 52, 539–544. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).