
The Effects of the Mamanet Cachibol League Intervention Program on Perceived Health Status, Mental Health, and Healthy Lifestyle Among Arab Women

 , , ,
, , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Description of the Mamanet Cachibol League Intervention Program (MCLIP)
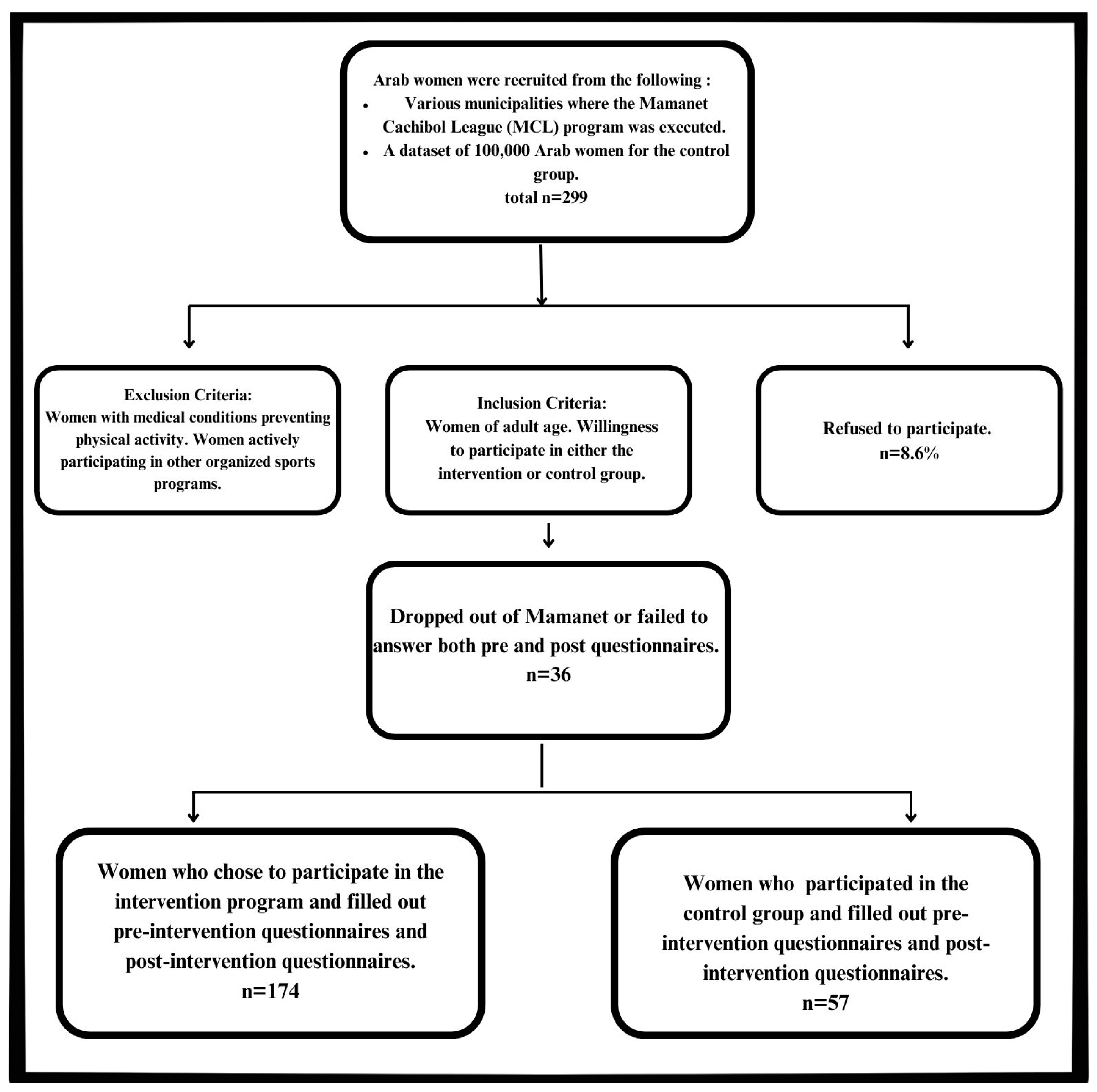
2.2. Research Design
2.3. Measures and Instruments
2.3.1. Sociodemographic Characteristics
2.3.2. Health Status
2.3.3. Mental Health
2.3.4. Healthy Lifestyle
2.4. Data Analysis
2.4.1. Sociodemographic Characteristics of Study Participants
2.4.2. Between- and Within-Group Differences and Changes in Health and Healthy Lifestyle Characteristics in the Intervention Group vs. the Control Group
2.4.3. Health and Lifestyle Differences Among Intervention Group Participants Based on Sociodemographic Characteristics
2.4.4. Pre-to-Post-Test Changes in Health and Lifestyle by Sociodemographic Characteristics—Intervention Group
3. Results
3.1. Sociodemographic Characteristics of the Study Participants
3.2. Comparisons Between Groups
3.3. Health Outcomes in the Intervention and Control Groups
3.4. Differences in Health and Healthy Lifestyle Between Participants with Different Sociodemographic Characteristics—Intervention Group
3.5. Changes in Health and Healthy Lifestyle According to Sociodemographic Characteristics—Intervention Group
4. Discussion
5. Practical Implications and Future Research
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sunarti, V.; Rahman, M.A.; Handrianto, C.; Syuraini, S.; Putri, L.D.; Azizah, Z.; Azhar, N.F. Understanding women’s empowerment through exercise: Insights from a study on physical activity and self-efficacy. Retos Nuevas Tend. Educ. Física Deporte Recreación 2024, 58, 227–237. [Google Scholar] [CrossRef]
- Eather, N.; Wade, L.; Pankowiak, A.; Eime, R. The impact of sports participation on mental health and social outcomes in adults: A systematic review and the ‘Mental Health through Sport’ conceptual model. Syst. Rev. 2023, 12, 102. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Physical Activity 2022; WHO: Geneva, Switzerland, 2023. [Google Scholar]
- Mansuri, S.; Daniel, M.N.; Westrick, J.C.; Buchholz, S.W. Physical activity behavior and measurement in Arab American women: An integrative review. J. Prev. 2023, 44, 749–776. [Google Scholar] [CrossRef] [PubMed]
- Alruwaili, M.D. A leadership-based framework for improving Saudi Arabian female participation in sports. Front. Sports Act. Living 2023, 5, 1283842. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, B.F.; Baker, P.; Pavey, T.; Alharbi, M.F. Investigating the beliefs of Saudi females regarding physical activity: A qualitative exploration. Int. J. Qual. Stud. Health Well-Being 2024, 19, 2296696. [Google Scholar] [CrossRef]
- World Health Organization Eastern Mediterranean Regional Office. Physical Activity Fact Sheet 2023: Focus on Women’s Health; WHO EMRO: Cairo, Egypt, 2023. [Google Scholar]
- Musaiger, A.O.; Hassan, A.S.; Obeid, O. The paradox of nutrition-related diseases in the Arab countries: The need for action. Int. J. Environ. Res. Public Health 2011, 8, 3637–3671. [Google Scholar] [CrossRef]
- Nikoloski, Z. Obesity in middle east. In Metabolic Syndrome: A Comprehensive Textbook; Springer International Publishing: Cham, Switzerland, 2024; pp. 65–80. [Google Scholar]
- World Health Organization. Obesity in the Middle East and North Africa. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 December 2022).
- Alhyas, L.; McKay, A.; Balasanthiran, A.; Majeed, A. Prevalences of overweight, obesity, hyperglycaemia, hypertension and dyslipidaemia in the Gulf: Systematic review. JRSM Short Rep. 2011, 2, 55. [Google Scholar] [CrossRef]
- Meernik, C.; Eilat-Adar, S.; Leonard, D.; Barlow, C.E.; Gerber, Y.; Tesler, R.; Byker Shanks, C.; Pettee Gabriel, K.; Pavlovic, A.; DeFina, L.F.; et al. Dietary patterns and cardiorespiratory fitness in midlife and subsequent all-cause dementia: Findings from the cooper center longitudinal study. Int. J. Behav. Nutr. Phys. Act. 2024, 21, 109. [Google Scholar] [CrossRef]
- Balatoni, I.; Szépné, H.V.; Kiss, T.; Adamu, U.G.; Szulc, A.M.; Csernoch, L. The importance of physical activity in preventing fatigue and burnout in healthcare workers. Healthcare 2023, 11, 1915. [Google Scholar] [CrossRef] [PubMed]
- Kahan, D. Physical Inactivity Prevalence in the Islamic World: An Updated Analysis of 47 Countries. J. Phys. Act. Health 2023, 20, 1133–1142. [Google Scholar] [CrossRef]
- Benajiba, N.; Mahrous, L.; Janah, K.; Alqabbani, S.F.; Chavarria, E.A.; Aboul-Enein, B.H. Physical activity interventions promoted in the Arabic-speaking region: A review of the current literature. Obes. Rev. 2020, 21, e13032. [Google Scholar] [CrossRef]
- Shao, T.; Verma, H.K.; Pande, B.; Costanzo, V.; Ye, W.; Cai, Y.; Bhaskar, L.V. Physical activity and nutritional influence on immune function: An important strategy to improve immunity and health status. Front. Physiol. 2021, 12, 751374. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.J.; Campbell, J.P.; Gleeson, M.; Krüger, K.; Nieman, D.C.; Pyne, D.B.; Turner, J.E.; Walsh, N.P. Can exercise affect immune function to increase susceptibility to infection? Exerc. Immunol. Rev. 2020, 26, 8–22. [Google Scholar] [PubMed]
- Wong, M.Y.; Fung, H.W.; Yuan, G.F. The association between physical activity, self-compassion, and mental well-being after COVID-19: In the exercise and self-esteem model revised with self-compassion (EXSEM-SC) perspective. Healthcare 2023, 11, 233. [Google Scholar] [CrossRef] [PubMed]
- Peng, B.; Ng, J.Y.; Ha, A.S. Barriers and facilitators to physical activity for young adult women: A systematic review and thematic synthesis of qualitative literature. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Vershinina, N.; Phillips, N.; McAdam, M. Online communities and entrepreneuring mothers: Practices of building, being and belonging. Entrep. Reg. Dev. 2022, 34, 742–764. [Google Scholar] [CrossRef]
- Donnelly, T.T.; Al-Thani, A.A.; Benjamin, K.; Al-Khater, A.H.; Fung, T.S.; Ahmedna, M.; Welch, A. Arab female and male perceptions of factors facilitating and inhibiting their physical activity: Findings from a qualitative study in the Middle East. PLoS ONE 2018, 13, e0199336. [Google Scholar] [CrossRef]
- Samara, A.; Nistrup, A.; Al-Rammah, T.Y.; Aro, A.R. Lack of facilities rather than sociocultural factors as the primary barrier to physical activity among female Saudi university students. Int. J. Women’s Health 2015, 7, 279–286. [Google Scholar] [CrossRef]
- Chaabane, S.; Chaabna, K.; Doraiswamy, S.; Mamtani, R.; Cheema, S. Barriers and facilitators associated with physical activity in the Middle East and North Africa region: A systematic overview. Int. J. Environ. Res. Public Health 2021, 18, 1647. [Google Scholar] [CrossRef] [PubMed]
- Sofian, M.; Omar-Fauzee, U.P.; Abd-Latif, R. The perspective of Arabic Muslim women toward sport participation. J. Asia Pac. Stud. 2010, 1, 364–377. [Google Scholar]
- Kay, T. Daughters of Islam: Family influences on Muslim young women’s participation in sport. Int. Rev. Sociol. Sport 2006, 41, 357–373. [Google Scholar] [CrossRef]
- Alanazi, H.M. The role of leisure activities in enhancing well-being in Saudi’s retired community: A mixed methods study. Humanit. Soc. Sci. Commun. 2024, 11, 604. [Google Scholar] [CrossRef]
- Parvez, Z. The FIFA World Cup 2022, National Identity, and the Politics of Women’s Sports Participation in Qatar. Asian J. Sport Hist. Cult. 2024, 3, 154–179. [Google Scholar] [CrossRef]
- Paldi, Y.; Moran, D.S.; Baron-Epel, O.; Bord, S.; Tesler, R. Ethnic disparities in social capital and health among Jewish and Arab participants in the Israeli Mamanet Cachibol League. Int. J. Environ. Res. Public Health 2021, 18, 295. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.K.; Yancey, A.K.; Spring, B.; Figueroa-Moseley, C.; Mohr, D.C.; Mustian, K.M.; Sprod, L.K.; Purnell, J.Q.; Fiscella, K. What are successful recruitment and retention strategies for underserved populations? Examining physical activity interventions in primary care and community settings. Transl. Behav. Med. 2011, 1, 234–251. [Google Scholar] [CrossRef]
- Baron-Epel, O.; Paldi, Y.; Bord, S.; Kadish, D.; Guttman, E.; Moran, D.S.; Tesler, R. Social capital and health among participants in the cachibol league in Israel. Int. Rev. Sociol. Sport 2021, 56, 877–896. [Google Scholar] [CrossRef]
- Eines, K.; Hochwald, I.H.; Green, G.; Dolev, A.; Bord, S.; Paldi, Y.; Shmueli, L.; Levi, S.; Tesler, R. The Effect of the Mamanet Cachibol League on Psychosomatic Symptoms, Healthy Eating, and Social Support Among Arab Women: A Mixed-Methods Study. J. Phys. Act. Health 2024, 21, 1208–1215. [Google Scholar] [CrossRef]
- Tesler, R.; Ng, K.; Gelber, D.; Hytönen-Ng, E. Mamanet: Empowering Mothers Towards Sport. In The Routledge Handbook of Gender Politics in Sport and Physical Activity; Routledge: Oxfordshire, UK, 2022; pp. 334–343. [Google Scholar]
- Molnar, G.; Bullingham, R. (Eds.) . The Routledge Handbook of Gender Politics in Sport and Physical Activity; Routledge: Oxfordshire, UK, 2022. [Google Scholar]
- Sleed, M.; Slade, A.; Fonagy, P. Reflective Functioning on the Parent Development Interview: Validity and reliability in relation to socio-demographic factors. Attach. Hum. Dev. 2020, 22, 310–331. [Google Scholar] [CrossRef] [PubMed]
- Almaleki, D.A. The Psychometric Properties of Distance-Digital Subjective Happiness Scale. Int. J. Comput. Sci. Netw. Secur. 2021, 21, 211–216. [Google Scholar]
- Cheung, R.Y. Patient Health Questionnaire-9 (PHQ-9). In Handbook of Assessment in Mindfulness Research; Springer International Publishing: Cham, Switzerland, 2024; pp. 1–12. [Google Scholar]
- Kyne, D.; Aldrich, D.P. Capturing bonding, bridging, and linking social capital through publicly available data. Risk Hazards Crisis Public Policy 2020, 11, 61–86. [Google Scholar] [CrossRef]
- Joseph, K.L.; Dagfinrud, H.; Christie, A.; Hagen, K.B.; Tveter, A.T. Criterion validity of The International Physical Activity Questionnaire-Short Form (IPAQ-SF) for use in clinical practice in patients with osteoarthritis. BMC Musculoskelet. Disord. 2021, 22, 232. [Google Scholar] [CrossRef]
- García-Conesa, M.T.; Philippou, E.; Pafilas, C.; Massaro, M.; Quarta, S.; Andrade, V.; Jorge, R.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; et al. Exploring the validity of the 14-item mediterranean diet adherence screener (Medas): A cross-national study in seven european countries around the mediterranean region. Nutrients 2020, 12, 2960. [Google Scholar] [CrossRef]
- Aharon, S.B.; Regev, O.; Tesler, R.; Barak, S.; Shapira, Y.; Weiss, Y.; Shtainmetz, N.; Vaknin, Y.; Goldstein, L.; Ben-Zvi, K.; et al. Assessment of nutritional status and health perception among male inmates in Israeli Prisons. Nutrients 2023, 15, 2255. [Google Scholar] [CrossRef]
- Morris, S.B.; DeShon, R.P. Combining effect size estimates in meta-analysis with repeated measures and independent-groups designs. Psychol. Methods 2002, 7, 105. [Google Scholar] [CrossRef] [PubMed]
- Welch, W.A.; Groth, C.P.; Phillips, S.M.; Spring, B.; Siddique, J. Comparing Accelerometer and Self-Reported Treatment Effects in a Technology-Supported Physical Activity Intervention. Health Educ. Behav. 2021, 48, 34–41. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; Sage Publications Limited: Los Angeles, CA, USA, 2024. [Google Scholar]
- Hume, P.; Marfell-Jones, M. The importance of accurate site location for skinfold measurement. J. Sports Sci. 2008, 26, 1333–1340. [Google Scholar] [CrossRef]
- Andersen, M.H.; Ottesen, L.; Thing, L.F. The social and psychological health outcomes of team sport participation in adults: An integrative review of research. Scand. J. Public Health 2019, 47, 832–850. [Google Scholar] [CrossRef] [PubMed]
- Martín-Rodríguez, A.; Gostian-Ropotin, L.A.; Beltrán-Velasco, A.I.; Belando-Pedreño, N.; Simón, J.A.; López-Mora, C.; Navarro-Jiménez, E.; Tornero-Aguilera, J.F.; Clemente-Suárez, V.J. Sporting Mind: The Interplay of Physical Activity and Psychological Health. Sports 2024, 12, 37. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Pardo, P.J.; Espeso-García, A.; Vaquero-Cristóbal, R.; Abelleira-Lamela, T.; González-Gálvez, N. The Effect of Resistance Training with Outdoor Fitness Equipment on the Body Composition, Physical Fitness, and Physical Health of Middle-Aged and Older Adults: A Randomized Controlled Trial. Healthcare 2024, 12, 726. [Google Scholar] [CrossRef]
- Alkhatry, M.; Hamadi, H.M.; Alwahedi, A.; Al Muzaki, Z.; Ahmed, F.; Almasri, B.; Housen, F.; Bataweel, M.; Alabar, E. Redefining Health through Multidisciplinary Obesity Prevention and Treatment in the United Arab Emirates. Med. Res. Arch. 2024, 12. [Google Scholar] [CrossRef]
- Ritondo, T.; Trussell, D.E. Resistance and mothers’ experiences in postnatal team sport: “Didn’t you just have a kid?”. Leis. Sci. 2023. [Google Scholar] [CrossRef]
- Liddelow, C. Exploring a mother’s engagement in team sport: An application of an extended theory of planned behaviour. J. Sci. Med. Sport 2024, 27, 786–792. [Google Scholar] [CrossRef]
- Batey, J.; Owton, H. Team Mums: Team sport experiences of athletic mothers. Women Sport Phys. Act. J. 2014, 22, 30–36. [Google Scholar] [CrossRef]
- Khalaf, S.B. Arabic Women’s Participation in Sport: Barriers and Motivation Among Egyptian and Kuwaiti Athletes. Ph.D. Thesis, Bangor University (United Kingdom), Bangor, UK, 2014. [Google Scholar]
- DeChano-Cook, L.M.; Shelley, F.M. Gender Equality and Sport Around the World. In Geography of Time, Place, Movement and Networks; Volume 5: Mapping Women and Family Journeys; Springer Nature: Cham, Switzerland, 2024; pp. 41–52. [Google Scholar]
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for adults: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 135. [Google Scholar] [CrossRef]
- Al-Eisa, E.S.; Al-Sobayel, H.I. Physical activity and health beliefs among Saudi women. J. Nutr. Metab. 2012, 2012, 642187. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Intervention Group (n = 174) | Control Group (n = 57) | Between-Group Differences: t Score (p-Value) or Chi-Square (p-Value) | |
|---|---|---|---|---|
| Age, years: mean (SD) | 43.1 (5.7) | 40.1 (5.9) | 0.001 | |
| Family status: n (%) | Single | 14.0 (8.0) | 8.0 (14.0) | 0.18 |
| In a relationship | 150.0 (86.2) | 47.0 (82.5) | 0.46 | |
| Divorced | 3.0 (1.7) | 1.0 (1.8) | 0.95 | |
| Widow | 7.0 (4.0) | 1.0 (1.8) | 0.43 | |
| Children, number: mean (SD) | 3.1 (1.2) | 2.5 (1.0) | 0.001 | |
| Education: n (%) | High school | 49.0 (28.1) | 8.0 (14.0) | 0.03 |
| Professional certificate | 56.0 (32.2) | 11.0 (19.3) | 0.06 | |
| Bachelor’s degree | 34.0 (19.5) | 29.0 (50.9) | <0.001 | |
| Graduate degree | 35.0 (20.1) | 9.0 (15.8) | 0.47 | |
| Religion: n (%) | Arab—Christian | 36.0 (20.6) | 11.0 (19.3) | 0.83 |
| Arab—Muslim | 131.0 (75.3) | 34.0 (59.6) | 0.02 | |
| Druze | 3.0 (1.7) | 11.0 (19.3) | <0.001 | |
| Other | 5.0 (2.8) | 1.0 (1.8) | 0.67 | |
| Religiosity level: n (%) | Secular | 56.0 (32.1) | 12.0 (21.1) | 0.11 |
| Traditional | 34.0 (19.5) | 29.0 (50.9) | <0.001 | |
| Religious | 54.0 (31.0) | 14.0 (24.6) | 0.35 | |
| Orthodox | 12.0 (6.9) | - | 0.04 | |
| Refuse or unknown | 18.0 (10.3) | 2.0 (3.5) | 0.11 | |
| Employment status: n (%) | Employee | 94.0 (54.0) | 43.0 (75.4) | 0.004 |
| Self-employed | 30.0 (17.2) | 4.0 (7.0) | 0.05 | |
| Unemployed | 4.0 (2.3) | 1.0 (1.8) | 0.82 | |
| Housewife | 28.0 (16.1) | 3.0 (5.3) | 0.03 | |
| Other | 18.0 (10.3) | 6.0 (10.5) | 0.96 | |
| Assessment Domain | Scale’s Name | Intervention Group (n = 174) | Control Group (n = 57) | Between-Group Differences | |||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-Test: Mean (SD) | Post-Test: Mean (SD) | Within-Group Changes: t (p-Value) [ES] | Pre-Test: Mean (SD) | Post-Test: Mean (SD) | Within-Group Changes: t (p-Value) [ES] | Pre-Test: t (p-Value) | Post-Test: t (p-Value) | ||
| Mental health | Subjective Happiness Scale, mean score | 5.0 (1.2) | 5.6 (0.8) | <0.01 | 4.6 (1.1) | 4.5 (1.1) | 0.06 | −2.40 (0.01) | <0.01 |
| Depression, sum score | 5.0 (4.4) | 4.0 (4.0) | −2.35 (0.01) [−0.22] | 8.4 (5.3) | 9.3 (3.9) | 2.30 (0.02) [0.15] | 4.40 (<0.01) | 8.75 (<0.001) | |
| Social capital, sum scores | 50.00 (13.7) | 52.5 (14.4) | 3.66 (<0.001) [0.11] | 45.0 (11.4) | 45.2 (10.7) | 0.56 (0.57) [0.01] | −3.21 (<0.001) | −4.06 (<0.001) | |
| Healthy lifestyle characteristics | Physical activity, weekly minutes in moderate and vigorous aerobic physical activity | 221.3 (437.2) | 248.2 (438.3) | 3.73 (<0.001) [0.06] | 206.5 (128.6) | 204.0 (191.0) | −0.32 (0.74) [−0.05] | −0.39 (0.69) | −1.03 (0.30) |
| Nutrition, IMED sum score | 8.0 (1.3) | 8.4 (1.4) | 3.92 (<0.001) [0.25] | 7.2 (1.7) | 7.4 (1.6) | 0.83 (0.40) [0.07] | −3.06 (0.003) | −3.96 (<0.001) | |
| Health | Happiness | Depression | Social Capital | Physical Activity | Nutrition | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| Not in a relationship (n = 24) | 4.6 (1.0) | 5.0 (0.8) | 4.8 (1.0) | 5.6 (0.8) | 5.0 (6.2) | 3.0 (3.0) | 55.2 (14.0) | 56.9 (14.7) | 196.6 (184.4) | 191.2 (173.5) | 8.0 (1.4) | 8.1 (1.8) |
| Relationship (n = 149) | 4.6 (1.08) | 5.2 (0.7) | 5.1 (1.2) | 5.6 (0.8) | 5.0 (4.0) | 4.1 (4.1) | 50.3 (13.5) | 51.8 (14.3) | 225.2 (465.4) * | 257.3 (466.7) * | 8.0 (1.3) | 8.4 (1.4) |
| High school (n = 47) a | 4.3 (1.0) | 5.2 (0.7) | 5.1 (1.2) | 5.8 (0.7) | 5.4 (4.4) | 2.9 (3.3) | 45.8 (15.1) b,c,d | 47.1 (16.3) c | 323.9 (796.9) | 344.6 (799.1) | 7.8 (1.2) | 8.3 (1.6) |
| Professional certificate (n = 56) b | 4.6 (1.0) | 5.2 (0.7) | 4.9 (1.2) | 5.5 (0.9) | 5.4 (5.1) | 4.1 (3.8) | 50.9 (12.8) a | 52.3 (13.3) | 202.9 (175.6) | 218.8 (174.7) | 8.1 (1.3) | 8.7 (1.3) |
| Bachelor’s degree (n = 33) c | 4.6 (1.0) | 5.3 (0.6) | 5.2 (1.0) | 5.7 (0.7) | 3.1 (3.0) | 4.6 (3.9) | 54.4 (13.0) a | 57.5 (13.7) a | 161.6 (131.4) | 227.4 (148.7) | 8.3 (1.2) | 8.2 (1.5) |
| Graduate degree (n = 35) d | 4.8 (1.1) | 5.2 (0.7) | 5.0 (1.1) | 5.4 (0.9) | 5.4 (4.0) | 4.6 (4.6) | 54.4 (12.0) a | 54.9 (12.1) | 181.7 (144.9) | 198.3 (150.9) | 7.8 (1.4) | 8.0 (1.5) |
| Not Muslim (n = 39) | 4.7 (1.3) | 5.2 (0.6) | 5.6 (0.7) | 5.8 (0.7) | 4.7 (3.8) | 4.0 (3.9) | 55.1 (11.7) | 55.7 (11.2) | 155.3 (151.5) | 170.7 (151.8) | 8.1 (1.1) | 8.4 (1.1) |
| Muslim (n = 130) | 4.2 (1.2) * | 5.2 (0.7) | 5.2 (1.1) * | 5.5 (0.9) | 4.7 (3.8) | 3.9 (4.0) | 47.9 (13.7) | 52.2 (14.6) | 194.6 (109.7) | 274.4 (495.6) | 7.3 (1.0) | 8.3 (1.5) |
| Secular (n = 56) | 4.8 (0.9) | 5.3 (0.7) | 5.1 (1.1) | 5.9 (0.7) | 4.8 (5.1) | 4.3 (4.2) | 52.8 (13.1) | 54.6 (14.4) | 283.5 (736.4) | 317.2 (730.8) | 8.3 (1.1) | 8.6 (1.5) |
| Traditional (n = 34) | 4.6 (1.1) | 5.2 (0.7) | 4.9 (1.1) | 5.4 (0.8) | 5.0 (4.3) | 4.7 (5.0) | 50.1 (15.8) | 52.0 (17.0) | 199.9 (153.5) | 214.5 (149.9) | 8.0 (1.4) | 8.2 (1.5) |
| Religious (n = 53) | 4.5 (0.9) | 5.2 (0.6) | 5.0 (1.3) | 5.4 (1.0) | 4.9 (4.0) | 3.4 (3.4) | 51.5 (13.7) | 52.4 (13.7) | 183.0 (169.8) | 211.0 (201.2) | 8.0 (1.4) | 8.2 (1.3) |
| Orthodox (n = 12) | 4.4 (1.0) | 4.7 (0.7) | 5.3 (0.9) | 5.8 (0.8) | 6.1 (3.7) | 4.5 (4.1) | 46.3 (8.7) | 49.5 (8.5) | 204.08 (183.4) | 230.0 (185.9) | 7.9 (1.3) | 8.5 (1.2) |
| Refuse (n = 18) | 4.2 (1.2) | 5.11 (0.7) | 5.2 (1.1) | 5.6 (0.7) | 4.7 (3.8) | 2.7 (2.0) | 47.9 (13.7) | 49.3 (14.7) | 194.6 (109.7_ | 220.5 (111.6) | 7.3 (1.0) | 8.1 (15) |
| Employee (n = 94) e | 4.7 (1.0) | 5.2 (0.6) | 5.1 (1.0) | 5.6 (0.8) | 4.7 (4.1) | 4.5 (4.6) | 51.5 (12.8) g | 53.1 (13.7) g | 214.3 (174.5) | 238.9 (170.3) | 8.0 (1.3) | 8.2 (1.4) |
| Self-employed (n = 29) f | 4.5 (1.0) | 5.4 (0.6) | 5.1 (1.0) | 5.5 (0.8) | 4.3 (4.8) | 2.9 (2.9) | 56.7 (9.7) g | 57.7 (10.1) g | 132.7 (126.5) | 182.1 (153.8) | 8.1 (1.3) | 8.6 (1.4) |
| Unemployed (n = 32) g | 4.6 (0.9) | 5.2 (0.7) | 5.0 (1.5) | 5.7 (1.0) | 5.9 (4.8) | 4.0 (3.3) | 43.7 (15.7) e,f,h | 44.9 (16.9) e,f,h | 332.6 (964.9) | 352.0 (968.7) | 8.1 (1.2) | 8.4 (1.4) |
| Other (n = 18) h | 4.2 (1.1) | 4.8 (0.8) | 5.0 (1.2) | 5.7 (0.7) | 5.8 (4.4) | 3.0 (2.5) | 51.5 (15.3) g | 54.4 (15.1)g | 207.3 (123.3) | 221.9 (123.7) | 7.7 (1.2) | 8.6 (1.6) |
| Sociodemographic Characteristics | Health Perception: Effect Size | Subjective Happiness: Effect Size | Depression: Effect Size | Social Capital: Effect Size | Physical Activity: Effect Size | Nutrition: Effect Size | |
|---|---|---|---|---|---|---|---|
| Family status | Not in a relationship (n = 24) | 0.37 * | 0.76 * | −0.31 * | 0.12 * | −0.02 | 0.08 |
| In a relationship (n = 149) | 0.60 * | 0.41 * | −0.20 * | 0.11 * | 0.06 | 0.28 * | |
| Education | High school (n = 47) | 0.85 * | 0.48 * | −0.55 * | 0.08 | 0.02 | 0.36 * |
| Professional certificate (n = 56) | 0.56 * | 0.50 * | −0.26 * | 0.11 * | 0.09 | 0.40 * | |
| Bachelor’s degree (n = 33) | 0.65 * | 0.50 * | 0.47 * | 0.24 * | 0.50 * | −0.04 | |
| Graduate degree (n = 35 | 0.27 * | 0.32 * | −0.19 * | 0.04 | 0.11 * | 0.16 * | |
| Religion | Not Muslim (n = 39) | 0.35 * | 0.26 * | −0.19 * | 0.05 | 0.10 * | 0.26 * |
| Muslim (n = 130) | 0.65 * | 0.45 * | −0.19 * | 0.13 * | 0.06 | 0.25 * | |
| Religiosity level | Secular (n = 56) | 0.59 * | 0.69 * | −0.09 | 0.13 * | 0.04 | 0.29 * |
| Traditional (n = 34) | 0.44 * | 0.46 * | −0.06 | 0.11 * | 0.09 | 0.14 * | |
| Religious (n = 53) | 0.69 * | 0.27 * | −0.37 * | 0.06 | 0.16 * | 0.15 * | |
| Orthodox (n = 12) | 0.30 * | 0.46 * | −0.44 * | 0.37 * | 0.14 * | 0.42 * | |
| Refuse/unknown (n = 18) | 0.67 * | 0.35 * | −0.52 * | 0.10 * | 0.23 * | 0.69 * | |
| Employment status | Employee (n = 94) | 0.48 * | 0.46 * | −0.05 | 0.12 * | 0.14 * | 0.14 * |
| Self-employed (n = 29) | 0.80 * | 0.33 * | −0.28 * | 0.09 | 0.39 * | 0.35 * | |
| Unemployed/housewife (n = 32) | 0.69 * | 0.43 * | −0.40 * | 0.07 | 0.02 | 0.25 * | |
| Other (n = 18) | 0.52 * | 0.63 * | −0.64 * | 0.19 * | 0.11 * | 0.70 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eines, K.; Tesler, R.; Birk, R.; Giladi, A.; Dunsky, A.; Alian, N.; Gonen, L.; Barak, S. The Effects of the Mamanet Cachibol League Intervention Program on Perceived Health Status, Mental Health, and Healthy Lifestyle Among Arab Women. Healthcare 2025, 13, 169. https://doi.org/10.3390/healthcare13020169
Eines K, Tesler R, Birk R, Giladi A, Dunsky A, Alian N, Gonen L, Barak S. The Effects of the Mamanet Cachibol League Intervention Program on Perceived Health Status, Mental Health, and Healthy Lifestyle Among Arab Women. Healthcare. 2025; 13(2):169. https://doi.org/10.3390/healthcare13020169
Chicago/Turabian StyleEines, Karin, Riki Tesler, Ruth Birk, Ariela Giladi, Ayelet Dunsky, Nada Alian, Limor Gonen, and Sharon Barak. 2025. "The Effects of the Mamanet Cachibol League Intervention Program on Perceived Health Status, Mental Health, and Healthy Lifestyle Among Arab Women" Healthcare 13, no. 2: 169. https://doi.org/10.3390/healthcare13020169
APA StyleEines, K., Tesler, R., Birk, R., Giladi, A., Dunsky, A., Alian, N., Gonen, L., & Barak, S. (2025). The Effects of the Mamanet Cachibol League Intervention Program on Perceived Health Status, Mental Health, and Healthy Lifestyle Among Arab Women. Healthcare, 13(2), 169. https://doi.org/10.3390/healthcare13020169