
Anhedonia and Negative Symptoms in First-Episode Psychosis: A Systematic Review and Meta-Analysis of Prevalence, Mechanisms, and Clinical Implications

 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Eligibility Criteria
2.3.1. Inclusion Criteria
- -
- Original research studies (observational, experimental, longitudinal, or cross-sectional designs)
- -
- Study population consisting of FEP patients (defined as ≤24 months from first contact with mental health services for psychotic symptoms). The 24-month threshold for FEP definition aligns with established international consensus criteria used by major early intervention services and research networks. While this approach captures the critical early intervention period, we acknowledge that it may introduce some heterogeneity regarding illness stage at study entry. Included studies addressed this potential confound through baseline stratification by illness duration, standardized follow-up intervals, and sensitivity analyses using symptom onset as alternative reference points where feasible.
- -
- Quantitative assessment of anhedonia or negative symptoms using validated instruments
- -
- Assessment tools including Scale for the Assessment of Negative Symptoms (SANS), Positive and Negative Syndrome Scale (PANSS) negative subscale, BNSS, CAINS, Chapman Physical or Social Anhedonia Scales, or other validated measures
- -
- Studies published in English, with full text available
- -
- Minimum sample size of 20 FEP patients
2.3.2. Exclusion Criteria
- -
- Studies focusing exclusively on chronic psychosis patients (>24 months duration)
- -
- Studies of at-risk mental state populations without transition to psychosis
- -
- Case reports, case series with <20 participants, review articles, meta-analyses, or conference abstracts
- -
- Studies lacking quantitative data on anhedonia or negative symptoms
- -
- Pediatric populations (age < 16 years)
- -
- Studies focusing exclusively on substance-induced psychosis
2.4. Study Selection and Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Synthesis and Analysis
Meta-Analytic Procedures
3. Results
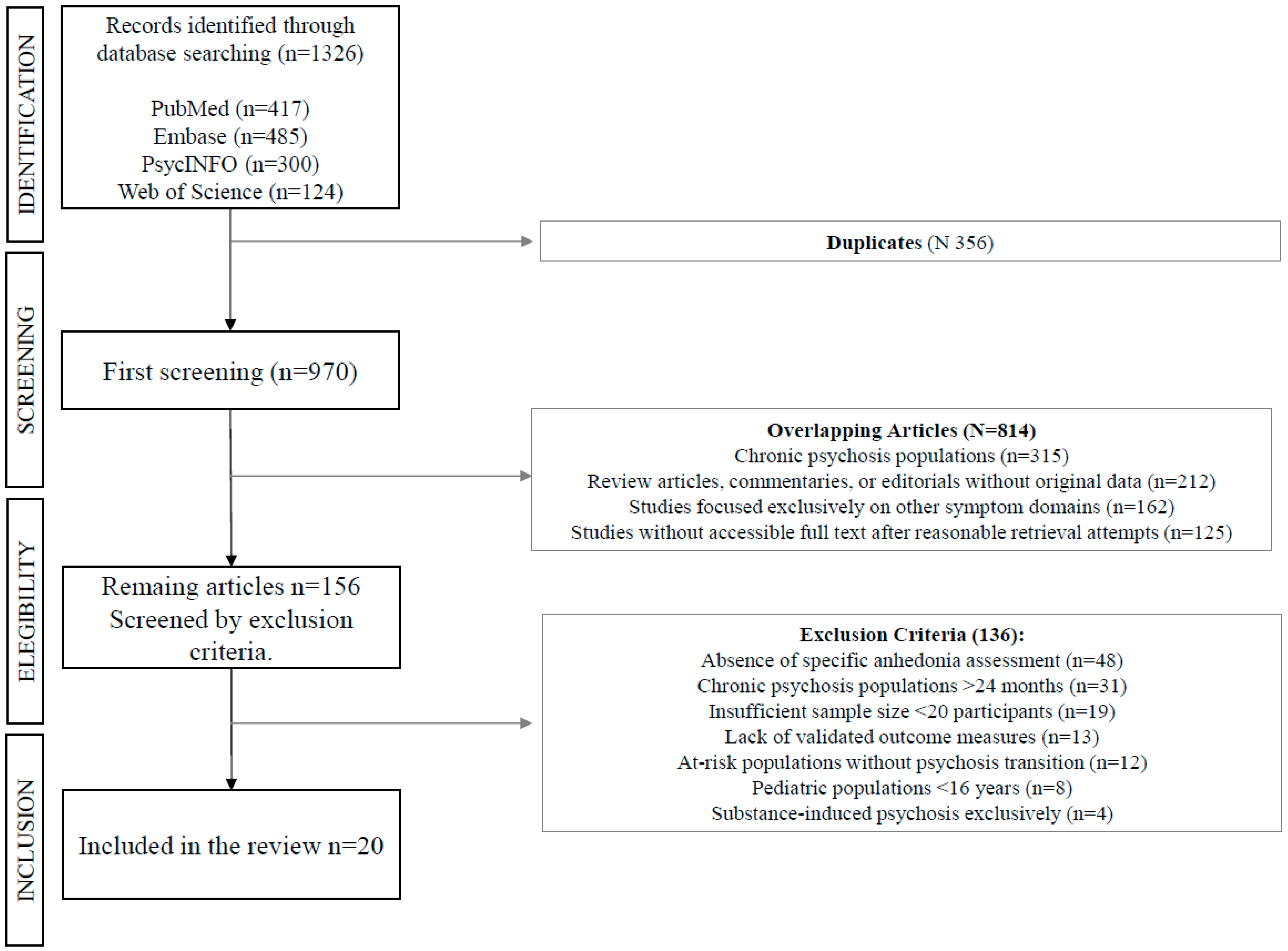
3.1. Study Selection
3.2. Study Characteristics and Quality Assessment
3.3. Prevalence and Assessment of Anhedonia
3.4. Meta-Analytic Synthesis
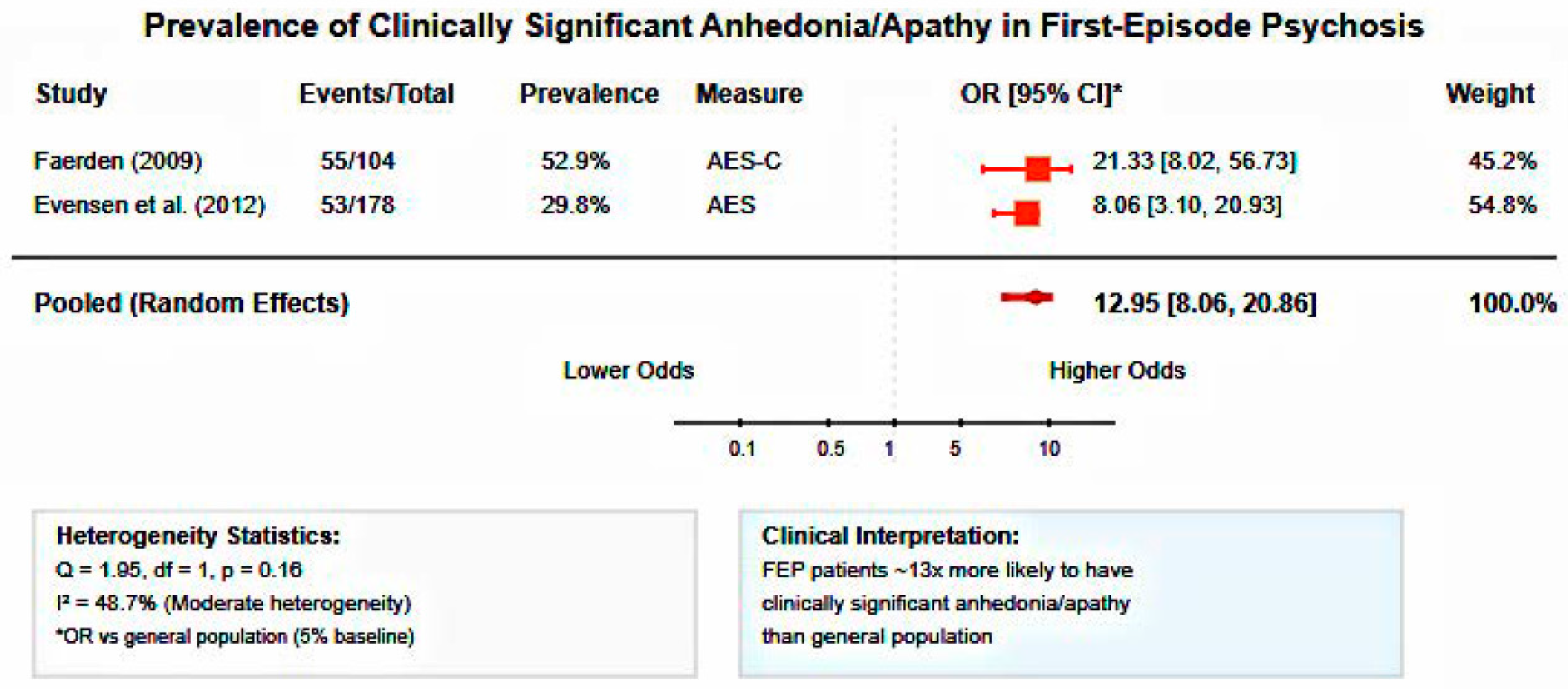
3.4.1. Anhedonia Prevalence in First-Episode Psychosis
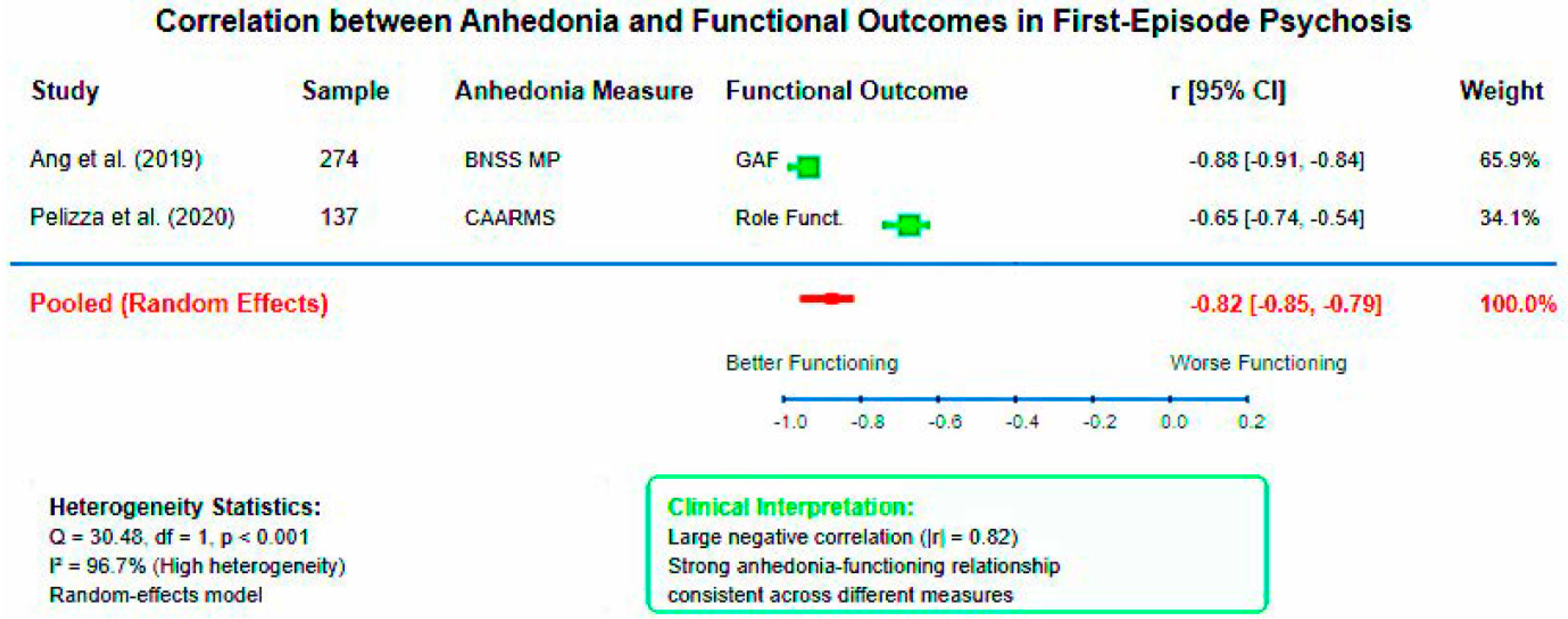
3.4.2. Anhedonia-Functional Outcome Associations
3.4.3. First-Episode Psychosis Versus Control Group
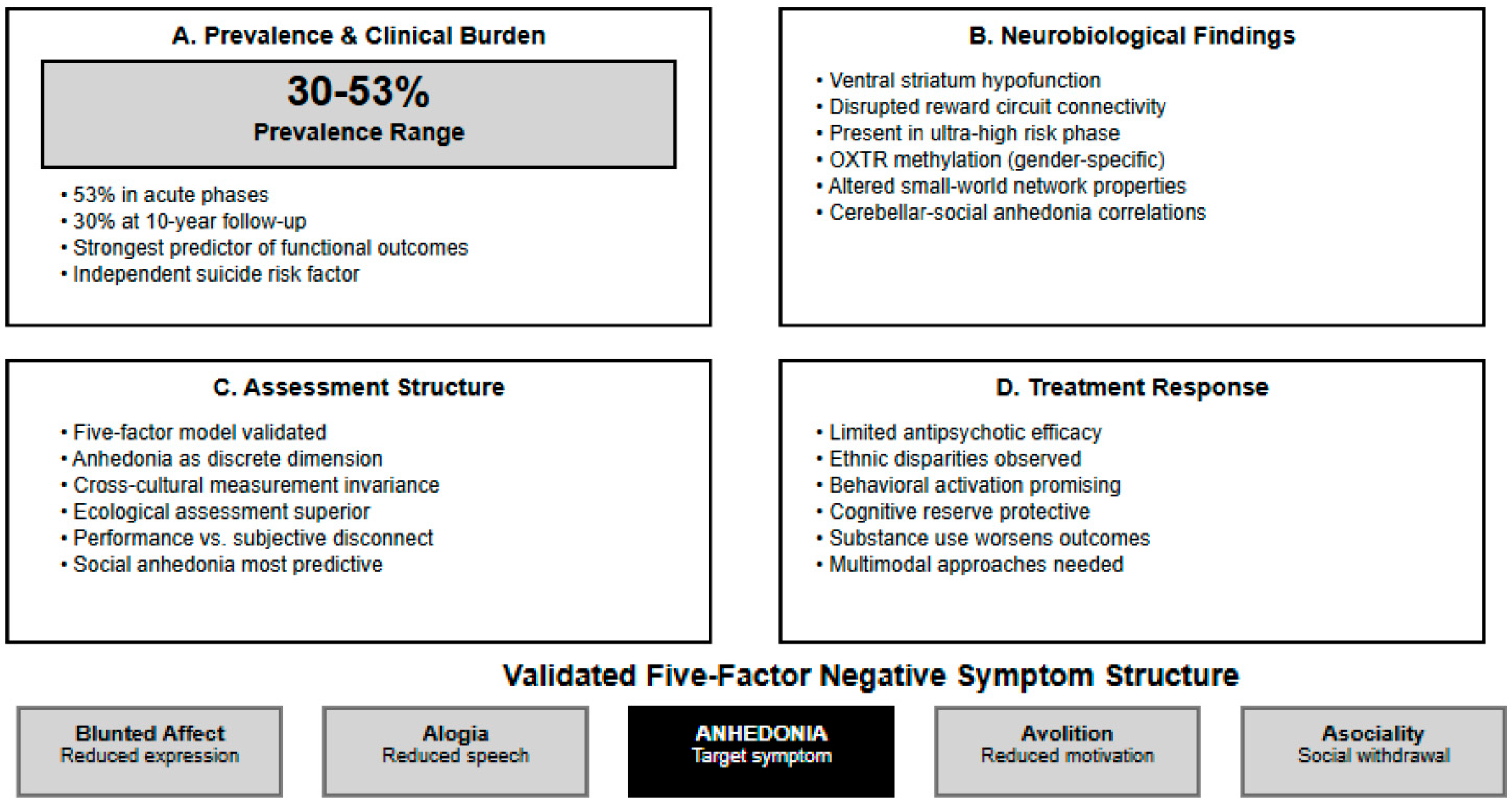
3.5. Factor Structure and Dimensional Analysis
3.6. Neurobiological Mechanisms
3.6.1. Structural Neuroimaging Studies
3.6.2. Functional Neuroimaging Studies
3.7. Clinical Correlates and Predictive Factors
3.8. Interventions and Treatment Response
3.8.1. Pharmacological Interventions
3.8.2. Psychosocial Interventions
4. Discussion
4.1. Prevalence and Clinical Burden of Anhedonia in Early Psychosis
4.2. Quantitative Synthesis and Effect Magnitudes
4.3. Dimensional Structure and Assessment Implications
4.4. Neurobiological Mechanisms and Circuit-Based Understanding
4.5. Epigenetic and Developmental Perspectives
4.6. Cognitive Reserve and Protective Factors
4.7. Ecological Validity and Real-World Assessment
4.8. Anhedonia and Suicide Risk
4.9. Treatment Response and Intervention Implications
4.10. Clinical Implications and Future Directions
4.11. Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kring, A.M.; Moran, E.K. Emotional response deficits in schizophrenia: Insights from affective science. Schizophr. Bull. 2008, 34, 819–834. [Google Scholar] [CrossRef]
- Strauss, G.P.; Gold, J.M. A new perspective on anhedonia in schizophrenia. Am. J. Psychiatry 2012, 169, 364–373. [Google Scholar] [CrossRef]
- Schlosser, D.A.; Campellone, T.R.; Kim, D.H.; Truong, B.; Vergani, S.; Ward, C.; Vinogradov, S. Motivational deficits in individuals at-risk for psychosis and across the course of schizophrenia. Schizophr. Res. 2014, 158, 52–57. [Google Scholar] [CrossRef]
- Gard, D.E.; Kring, A.M.; Gard, M.G.; Horan, W.P.; Green, M.F. Anhedonia in schizophrenia: Distinctions between anticipatory and consummatory pleasure. Schizophr. Res. 2007, 93, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Chapman, L.J.; Chapman, J.P.; Raulin, M.L. Scales for physical and social anhedonia. J. Abnorm. Psychol. 1976, 85, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Gard, D.E.; Gard, M.G.; Kring, A.M.; John, O.P. Anticipatory and consummatory components of the experience of pleasure: A scale development study. J. Res. Pers. 2006, 40, 1086–1102. [Google Scholar] [CrossRef]
- Kirkpatrick, B.; Fenton, W.S.; Carpenter, W.T.; Marder, S.R. The NIMH-MATRICS consensus statement on negative symptoms. Schizophr. Bull. 2006, 32, 214–219. [Google Scholar] [CrossRef]
- Strauss, G.P.; Horan, W.P.; Kirkpatrick, B.; Fischer, B.A.; Keller, W.R.; Miski, P.; Buchanan, R.W.; Green, M.F.; Carpenter, W.T. Deconstructing negative symptoms of schizophrenia: Avolition-apathy and diminished expression clusters predict clinical presentation and functional outcome. J. Psychiatr. Res. 2013, 47, 783–790. [Google Scholar] [CrossRef]
- Kring, A.M.; Gur, R.E.; Blanchard, J.J.; Horan, W.P.; Reise, S.P. The Clinical Assessment Interview for Negative Symptoms (CAINS): Final development and validation. Am. J. Psychiatry 2013, 170, 165–172. [Google Scholar] [CrossRef]
- Kirkpatrick, B.; Strauss, G.P.; Nguyen, L.; Fischer, B.A.; Daniel, D.G.; Cienfuegos, A.; Marder, S.R. The Brief Negative Symptom Scale: Psychometric properties. Schizophr. Bull. 2011, 37, 300–305. [Google Scholar] [CrossRef]
- Juckel, G.; Schlagenhauf, F.; Koslowski, M.; Wüstenberg, T.; Villringer, A.; Knutson, B.; Wrase, J.; Heinz, A. Dysfunction of ventral striatal reward prediction in schizophrenia. NeuroImage 2006, 29, 409–416. [Google Scholar] [CrossRef]
- Nielsen, M.Ø.; Rostrup, E.; Wulff, S.; Bak, N.; Lublin, H.; Kapur, S.; Glenthøj, B. Improvement of brain reward abnormalities by antipsychotic monotherapy in schizophrenia. Arch. Gen. Psychiatry 2012, 69, 1195–1204. [Google Scholar] [CrossRef]
- Radua, J.; Schmidt, A.; Borgwardt, S.; Heinz, A.; Schlagenhauf, F.; McGuire, P.; Fusar-Poli, P. Ventral striatal activation during reward processing in psychosis: A neurofunctional meta-analysis. JAMA Psychiatry 2015, 72, 1243–1251. [Google Scholar] [CrossRef]
- Howes, O.D.; Kambeitz, J.; Kim, E.; Stahl, D.; Slifstein, M.; Abi-Dargham, A.; Kapur, S. The nature of dopamine dysfunction in schizophrenia and what this means for treatment. Arch. Gen. Psychiatry 2012, 69, 776–786. [Google Scholar] [CrossRef]
- Demjaha, A.; Murray, R.M.; McGuire, P.K.; Kapur, S.; Howes, O.D. Dopamine synthesis capacity in patients with treatment-resistant schizophrenia. Am. J. Psychiatry 2012, 169, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, W.T.; Heinrichs, D.W.; Wagman, A.M. Deficit and nondeficit forms of schizophrenia: The concept. Am. J. Psychiatry 1988, 145, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Kirschner, M.; Aleman, A.; Kaiser, S. Secondary negative symptoms—A review of mechanisms, assessment and treatment. Schizophr. Res. 2017, 186, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Upthegrove, R.; Marwaha, S.; Birchwood, M. Depression and schizophrenia: Cause, consequence, or trans-diagnostic issue? Schizophr. Bull. 2017, 43, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Austin, S.F.; Mors, O.; Secher, R.G.; Hjorthøj, C.R.; Albert, N.; Bertelsen, M.; Nordentoft, M. Predictors of recovery in first episode psychosis: The OPUS cohort at 10 year follow-up. Schizophr. Res. 2013, 150, 163–168. [Google Scholar] [CrossRef]
- Milev, P.; Ho, B.C.; Arndt, S.; Andreasen, N.C. Predictive values of neurocognition and negative symptoms on functional outcome in schizophrenia: A longitudinal first-episode study with 7-year follow-up. Am. J. Psychiatry 2005, 162, 495–506. [Google Scholar] [CrossRef]
- Fervaha, G.; Foussias, G.; Agid, O.; Remington, G. Motivational and neurocognitive deficits are central to the prediction of longitudinal functional outcome in schizophrenia. Acta Psychiatr. Scand. 2015, 132, 290–299. [Google Scholar] [CrossRef]
- Robertson, B.R.; Prestia, D.; Twamley, E.W.; Patterson, T.L.; Bowie, C.; Harvey, P.D. Social competence versus negative symptoms as predictors of real world social functioning in schizophrenia. Schizophr. Res. 2014, 160, 136–141. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Papanastasiou, E.; Stahl, D.; Rocchetti, M.; Carpenter, W.; Shergill, S.; McGuire, P. Treatments of negative symptoms in schizophrenia: Meta-analysis of 168 randomized placebo-controlled trials. Schizophr. Bull. 2015, 41, 892–899. [Google Scholar] [CrossRef]
- Correll, C.U.; Schooler, N.R. Negative symptoms in schizophrenia: A review and clinical guide for recognition, assessment, and treatment. Neuropsychiatr. Dis. Treat. 2020, 16, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Velligan, D.I.; Roberts, D.L.; Sierra, C.; Fredrick, M.M.; Rosenthal, J.; Raymer, K.; Mintz, J. What happens when clinicians and researchers actually meet: Findings from the Cognitive Behavioral Social Skills Training multi-site effectiveness study. Schizophr. Bull. 2015, 41, 1073–1081. [Google Scholar]
- Grant, P.M.; Huh, G.A.; Perivoliotis, D.; Stolar, N.M.; Beck, A.T. Randomized trial to evaluate the efficacy of cognitive therapy for low-functioning patients with schizophrenia. Arch. Gen. Psychiatry 2012, 69, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Pot-Kolder, R.M.C.A.; Geraets, C.N.W.; Veling, W.; van Beilen, M.; Staring, A.B.P.; Gijsman, H.J.; Delespaul, P.A.E.G.; van der Gaag, M. Virtual-reality-based cognitive behavioural therapy versus waiting list control for paranoid ideation and social avoidance in patients with psychotic disorders: A single-blind randomised controlled trial. Lancet Psychiatry 2018, 5, 217–226. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ang, M.S.; Rekhi, G.; Lee, J. Validation of the Brief Negative Symptom Scale and its association with functioning. Schizophr. Res. 2019, 208, 97–104. [Google Scholar] [CrossRef]
- Pelizza, L.; Leuci, E.; Maestri, D.; Quattrone, E.; Azzali, S.; Paulillo, G.; Menchetti, M. Anhedonia in adolescents and young adults at clinical high risk for psychosis: Findings from a 1-year longitudinal study. Eur. Child Adolesc. Psychiatry 2020, 29, 655–665. [Google Scholar]
- Faerden, A.; Friis, S.; Agartz, I.; Barrett, E.A.; Nesvåg, R.; Finset, A.; Melle, I. Apathy and functioning in first-episode psychosis. Psychiatr. Serv. 2009, 60, 1495–1503. [Google Scholar] [CrossRef]
- Evensen, J.; Rossberg, J.I.; Barder, H.; Haahr, U.; Ten Velden Hegelstad, W.; Joa, I.; Friis, S. Apathy in first episode psychosis patients: A ten year longitudinal follow-up study. Schizophr. Res. 2012, 136, 19–24. [Google Scholar] [CrossRef]
- Ahmed, A.O.; Kirkpatrick, B.; Galderisi, S.; Mucci, A.; Rossi, A.; Bertolino, A.; Strauss, G.P. Cross-cultural validation of the 5-factor structure of negative symptoms in schizophrenia. Schizophr. Bull. 2019, 45, 305–314. [Google Scholar] [CrossRef]
- Yang, L.H.; Wonpat-Borja, A.J.; Opler, M.G.; Corcoran, C.M. Potential stigma associated with inclusion of the psychosis risk syndrome in the DSM-V: An empirical question. Schizophr. Res. 2018, 120, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, J.J.; Catalano, L.T.; Aghevli, M.; Chappell, A.M. Social affiliation and negative symptoms in schizophrenia: Examining the role of behavioral skills and subjective responding. Schizophr. Res. 2015, 168, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.S.; Shen, G.; Liu, C.; Kang, N.I.; Lee, K.H.; Sui, J.; Chung, Y.C. Altered grey matter networks related to social anhedonia in patients with schizophrenia. Psychiatry Res. Neuroimaging 2021, 310, 111263. [Google Scholar]
- Cressman, V.L.; Schobel, S.A.; Steinfeld, S.; Ben-David, S.; Thompson, J.L.; Small, S.A.; Javitt, D.C. Anhedonia in the psychosis risk syndrome: Associations with social impairment and basal orbitofrontal cortical activity. NPJ Schizophr. 2015, 1, 15020. [Google Scholar] [CrossRef]
- Wolf, D.H.; Satterthwaite, T.D.; Kantrowitz, J.J.; Katchmar, N.; Vandekar, L.; Elliott, M.A.; Ruparel, K. Amotivation in schizophrenia: Integrated assessment with behavioral, clinical, and imaging measures. Schizophr. Bull. 2014, 40, 1328–1337. [Google Scholar] [CrossRef]
- Juckel, G.; Friedel, E.; Koslowski, M.; Witthaus, H.; Özgürdal, S.; Gudlowski, Y.; Schlagenhauf, F. Ventral striatal activation during reward processing in subjects with ultra-high risk for schizophrenia. Neuropsychopharmacology 2012, 37, 2650–2660. [Google Scholar] [CrossRef]
- Bang, M.; Kim, K.R.; Song, Y.Y.; Baek, J.H.; Kwon, J.S.; Potkin, S.G. Neurocognitive impairments in individuals at ultra-high risk for psychosis: Who will really convert? Aust. N. Z. J. Psychiatry 2019, 53, 462–471. [Google Scholar] [CrossRef]
- Clougher, D.; Nuechterlein, K.H.; Ventura, J.; Subotnik, K.L.; Marder, S.R. Cognitive reserve, negative symptoms, and functioning in first-episode psychosis: A mediation analysis. Schizophr. Res. 2024, 264, 112–119. [Google Scholar]
- Patezold, A.; Kunkels, Y.K.; Ziermans, T.B.; Lichtenstein, T.; Boonstra, N.; Myin-Germeys, I.; Rietdijk, J. Ecological momentary assessment of negative symptoms in the daily life of young people at ultra-high risk for psychosis. Psychol. Med. 2021, 51, 2430–2439. [Google Scholar]
- Poletti, S.; Melloni, E.; Aggio, V.; Colombo, C.; Valtorta, F.; Benedetti, F.; Vai, B. Anhedonia and suicidal ideation in individuals with psychosis: A 2-year longitudinal study. J. Affect. Disord. 2023, 323, 309–316. [Google Scholar]
- Keshavan, M.; Li, H.; Eack, S. Longitudinal treatment outcome of African American and Caucasian patients with first episode psychosis. Schizophr. Res. 2012, 142, 56–60. [Google Scholar]
- Gómez-Revuelta, M.; Pelayo-Terán, J.M.; Juncal-Ruiz, M.; Vázquez-Bourgon, J.; Suárez-Pinilla, P.; Romero-Jiménez, R.; Crespo-Facorro, B. Antipsychotic Treatment Effectiveness in First Episode of Psychosis: PAFIP 3-Year Follow-Up Randomized Clinical Trials Comparing Haloperidol, Olanzapine, Risperidone, Aripiprazole, Quetiapine, and Ziprasidone. Int. J. Neuropsychopharmacol. 2020, 23, 217–229. [Google Scholar] [CrossRef]
- Buoli, M.; Serati, M.; Altamura, A.C. Aripiprazole Long-Acting Injection During First Episode Schizophrenia—An Exploratory Analysis. Front. Psychiatry 2020, 10, 935. [Google Scholar]
- Addington, J.; Epstein, I.; Liu, L.; French, P.; Boydell, K.M.; Zipursky, R.B. A randomized controlled trial of cognitive behavioral therapy for individuals at clinical high risk of psychosis. Schizophr. Res. 2011, 125, 54–61. [Google Scholar] [CrossRef]
- Byrne, M.K.; Nic Giolla Easpaig, B.; Gray, R.; Creek, R.; Jones, M.; Brown, E.; Bressington, D. Behavioural activation for depressive symptoms in young people with emerging or early psychosis: A pilot study protocol. PLoS ONE 2023, 18, e0280559. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Design | Sample Size | Population | Country | Follow-Up | Primary Anhedonia Measure | NOS Score |
|---|---|---|---|---|---|---|---|---|
| Ang et al. [29] | 2019 | Cross-sectional | 274 | Schizophrenia | Singapore | - | BNSS | 7 |
| Pelizza et al. [30] | 2020 | Longitudinal | 232 | FEP + controls | Italy | 12 months | CAARMS, O-LIFE | 8 |
| Faerden et al. [31] | 2009 | Cross-sectional | 104 | FEP | Norway | - | AES-C | 7 |
| Evensen et al. [32] | 2012 | Longitudinal | 301 | FEP | Norway | 10 years | AES | 9 |
| Ahmed et al. [33] | 2019 | Cross-sectional | 1691 | Psychotic disorders | Multi-country | - | BNSS | 8 |
| Yang et al. [34] | 2018 | Cross-sectional | 168 | UHR | USA | - | PANSS | 6 |
| Blanchard et al. [35] | 2015 | Cross-sectional | 48 | Schizophrenia | USA | - | Video paradigm | |
| Kim et al. [36] | 2021 | Cross-sectional | 283 | Schizophrenia | South Korea | - | Chapman Scale | 7 |
| Cressman et al. [37] | 2015 | Cross-sectional | 62 | CHR | USA | - | Chapman Scale | 6 |
| Wolf et al. [38] | 2014 | Cross-sectional | 78 | Schizophrenia | USA | - | CAINS | 8 |
| Juckel et al. [39] | 2012 | Cross-sectional | 26 | UHR | Germany | - | fMRI task | 7 |
| Bang et al. [40] | 2019 | Cross-sectional | 208 | ROS + UHR | South Korea | - | PANSS | 7 |
| Clougher et al. [41] | 2024 | Longitudinal | 162 | FEP | USA | 12 months | PANSS | 8 |
| Patezold et al. [42] | 2021 | Longitudinal | 79 | UHR | Netherlands | 24 months | EMA | 8 |
| Poletti et al. [43] | 2023 | Longitudinal | 242 | FEP + UHR | Italy | 24 months | BDI-II, CAARMS | 8 |
| Keshavan et al. [44] | 2012 | Longitudinal | 199 | FEP | USA | 12 months | SANS | 7 |
| Gómez-Revuelta et al. [45] | 2020 | RCT | 376 | FEP | Spain | 36 months | SANS | 8 |
| Buoli et al. [46] | 2020 | Observational | 48 | FEP | Italy | 12 months | Clinical assessment | 6 |
| Addington et al. [47] | 2011 | RCT | 51 | CHR | Canada | 18 months | SIPS | 6 |
| Byrne et al. [48] | 2023 | Protocol | 60 | Early psychosis | Australia | 3 months | Various | - |
| Study | Population | Sample Size | Assessment Tool | Anhedonia Measure | Prevalence/Severity | Key Clinical Findings |
|---|---|---|---|---|---|---|
| PREVALENCE STUDIES | ||||||
| Ang et al. [29] | Schizophrenia | 274 | BNSS | Motivation-Pleasure factor | B = −0.876, p < 0.001 | Strong association with GAF scores; avolition showed strongest functional correlation |
| Pelizza et al. [30] | FEP vs. Controls | 137 vs. 95 | CAARMS, O-LIFE | Anhedonia scores | Significantly higher vs. controls | Improvement over 1-year follow-up; correlations with role functioning and quality of life |
| SEVERITY AND CORRELATION STUDIES | ||||||
| Faerden [31] | FEP | 104 | AES-C | Clinical apathy | 53% | Strong correlation with functional outcomes; male gender and longer DUP associated with higher levels |
| Evensen et al. [32] | FEP | 178 | AES | Clinical apathy | 30% at 10-year follow-up | Persistent motivational deficits; independent contribution to impaired functioning and quality of life |
| PREDICTIVE AND ECOLOGICAL STUDIES | ||||||
| Bang et al. [40] | ROS + UHR | 208 | PANSS | Anhedonia-asociality | Gender-specific correlations | OXTR methylation associations; women showed stronger anhedonia-methylation correlations |
| Patezold et al. [42] | UHR | 79 | EMA | Social anhedonia | Functional impairment predictor | Social anhedonia predicted functioning and illness severity at 1-year follow-up |
| LONGITUDINAL RISK STUDIES | ||||||
| Poletti [43] | FEP + UHR | 242 | BDI-II, CAARMS | Anhedonia subscale | Suicide risk association | Persistent association with suicidal ideation over 2 years, independent of depression severity |
| Study | Method | Sample | Key Neurobiological Findings | Anhedonia Correlates |
|---|---|---|---|---|
| Kim et al. (2021) [36] | Graph theory analysis | 283 (123 patients) | Reduced small-world properties in multiple networks | Cerebellar-social anhedonia correlations |
| Cressman et al. (2015) [37] | Basal-state fMRI | 62 CHR | Negative correlation with orbitofrontal cortex CBV | r = negative, p < 0.05 |
| Wolf et al. (2014) [38] | Task-based fMRI + PRT | 78 (41 patients) | Ventral striatum hypofunction | Dimensional relationship with behavioral motivation |
| Juckel et al. (2012) [39] | fMRI (MID task) | 26 UHR | Reduced VS activation trend | Loss-avoidance anticipation deficits |
| Bang et al. (2019) [40] | Rs-fMRI + genetics | 208 (subset n = 72) | Striatal-amygdala connectivity alterations | OXTR methylation associations |
| Domain | Studies (n) | Participants | Assessment Tools | Pooled Estimate | 95% CI | I2 | Interpretation |
|---|---|---|---|---|---|---|---|
| Anhedonia Prevalence | 2 | 282 FEP patients | AES-C, AES | OR = 12.95 * | 8.06–20.86 | 48.7% | 13-fold increased odds vs. general population |
| Anhedonia-Functioning Association | 2 | 411 participants | BNSS, CAARMS | r = −0.823 | −0.852 to −0.789 | 96.7% | Large negative correlation |
| FEP vs. Controls | 2 | 331 total (199 FEP, 132 controls) | CAARMS, O-LIFE, Chapman Scales | Cohen’s d = 0.829 | 0.600–1.058 | 0.0% | Large effect size favoring higher anhedonia in FEP |
| Study | Intervention Type | Sample | Duration | Primary Outcome | Anhedonia-Specific Results |
|---|---|---|---|---|---|
| Pharmacological | |||||
| Keshavan et al. (2012) [44] | Standard antipsychotic treatment | 199 FEP | 12 months | Ethnic treatment response | African Americans: less anhedonia improvement |
| Gómez-Revuelta et al. (2020) [45] | 6 antipsychotics comparison | 376 FEP | 36 months | Treatment discontinuation | No notable changes in negative symptoms |
| Buoli et al. (2020) [46] | Aripiprazole LAI | 48 FEP | 12 months | Treatment adherence | Substance use worsened anhedonia outcomes |
| Psychosocial | |||||
| Addington et al. (2011) [47] | CBT vs. supportive therapy | 51 CHR | 18 months | Psychosis conversion | No improvement in negative symptoms |
| Byrne et al. (2023) [48] | Behavioral activation protocol | 60 early psychosis | 3 months | Depression (primary), negative symptoms (secondary) | Protocol targets reward processing deficits |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricci, V.; Sarni, A.; Barresi, M.; Remondino, L.; Maina, G. Anhedonia and Negative Symptoms in First-Episode Psychosis: A Systematic Review and Meta-Analysis of Prevalence, Mechanisms, and Clinical Implications. Healthcare 2025, 13, 1796. https://doi.org/10.3390/healthcare13151796
Ricci V, Sarni A, Barresi M, Remondino L, Maina G. Anhedonia and Negative Symptoms in First-Episode Psychosis: A Systematic Review and Meta-Analysis of Prevalence, Mechanisms, and Clinical Implications. Healthcare. 2025; 13(15):1796. https://doi.org/10.3390/healthcare13151796
Chicago/Turabian StyleRicci, Valerio, Alessandro Sarni, Marialuigia Barresi, Lorenzo Remondino, and Giuseppe Maina. 2025. "Anhedonia and Negative Symptoms in First-Episode Psychosis: A Systematic Review and Meta-Analysis of Prevalence, Mechanisms, and Clinical Implications" Healthcare 13, no. 15: 1796. https://doi.org/10.3390/healthcare13151796
APA StyleRicci, V., Sarni, A., Barresi, M., Remondino, L., & Maina, G. (2025). Anhedonia and Negative Symptoms in First-Episode Psychosis: A Systematic Review and Meta-Analysis of Prevalence, Mechanisms, and Clinical Implications. Healthcare, 13(15), 1796. https://doi.org/10.3390/healthcare13151796