
Social Support’s Dual Mechanisms in the Loneliness–Frailty Link Among Older Adults with Diabetes in Beijing: A Cross-Sectional Study of Mediation and Moderation


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection Procedures
2.3. Statistical Analysis Framework
2.4. Disclosure of Generative Artificial Intelligence Usage in Manuscript Preparation
3. Results
3.1. Participant Characteristics and Distribution of Core Variables
3.2. Correlations Among Loneliness, Social Support, and Frailty
3.3. Multivariate Regression Analysis of Frailty Predictors
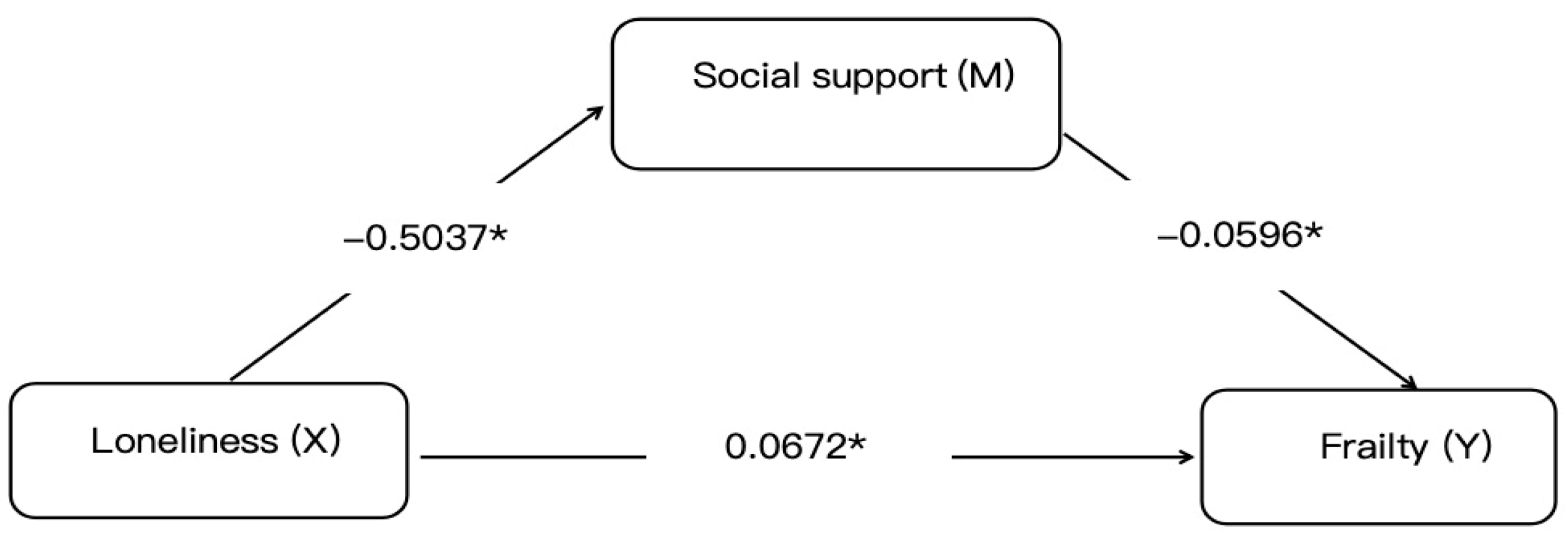
3.4. Mediation Analysis of Social Support
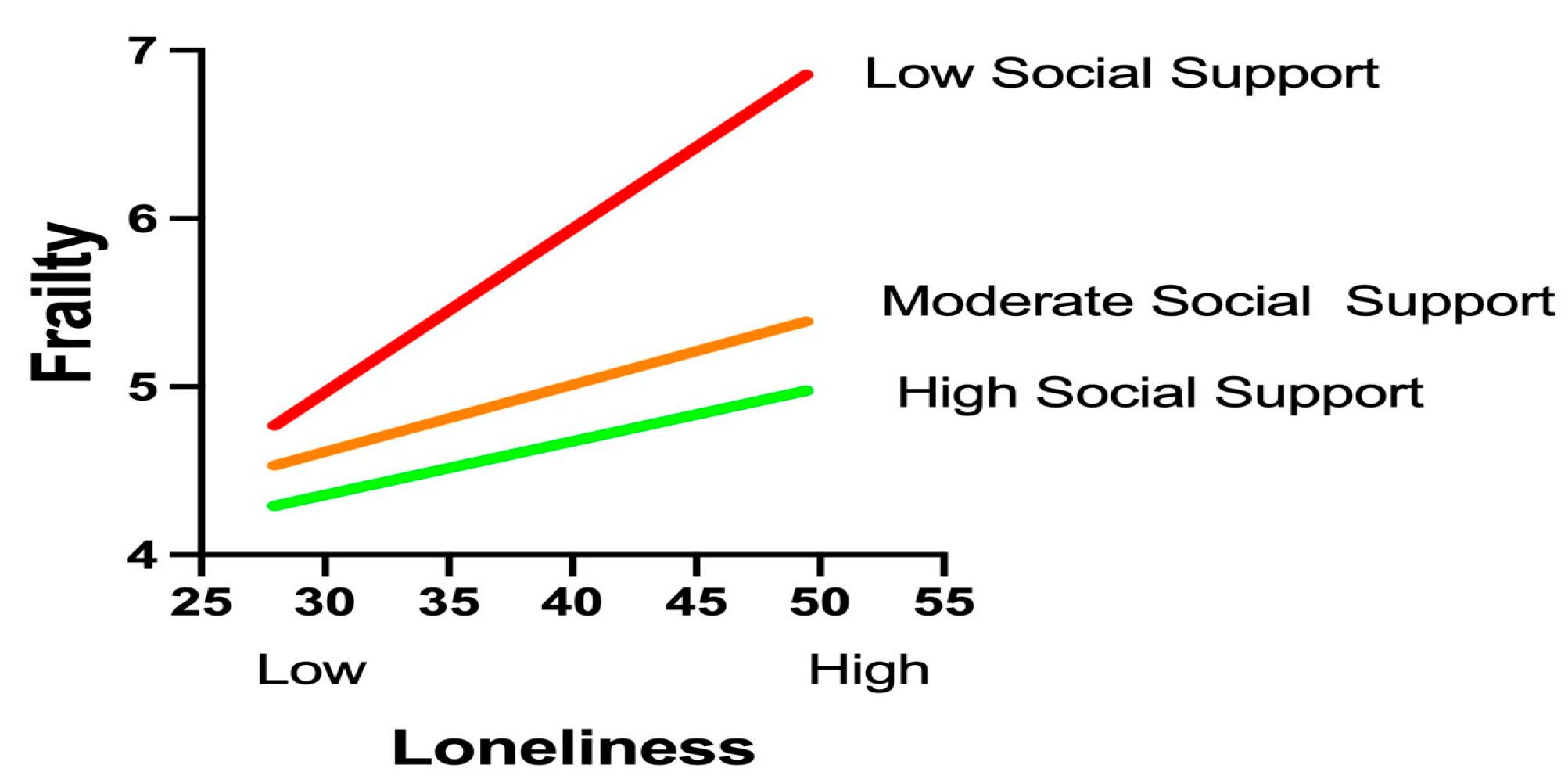
3.5. Role of Social Support in the Loneliness–Frailty Association
3.6. Subgroup Differences in Demographic Characteristics
3.7. Identification of High-Risk Subgroups
4. Discussion
4.1. Theoretical Framework and Dual Mechanisms
4.2. Clinical Translation: Nurse-Led Implementation Framework
4.3. Technological Integration and Objective Monitoring
4.4. Limitations and Future Research Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Liu, Z.; Liu, Z.; Wang, J.; Sun, H.; Xia, Y.; Wu, Y.; Li, H.; Zhang, Y.; Chen, H.; Zhang, J.; et al. Social Isolation in Chinese Older Adults. Lancet Reg. Health West. Pac. 2022, 23, 100458. [Google Scholar]
- National Bureau of Statistics of China. Seventh National Population Census Bulletin; National Bureau of Statistics: Beijing, China, 2021.
- Wicaksana, A.L.; Apriliyasari, R.W.; Tsai, P.S. Prevalence and risk factors for loneliness among individuals with diabetes: A systematic review and meta-analysis. Syst. Rev. 2025, 14, 96. [Google Scholar] [CrossRef] [PubMed]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness Matters: A Theoretical and Empirical Review of Consequences and Mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; McBurnie, M.A. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Hackett, R.A.; Steptoe, A. Psychosocial Stress and Mitochondrial Function in Cardiometabolic Disorders. Psychosom. Med. 2021, 83, 515–526. [Google Scholar]
- Petersen, M.C.; Shulman, G.I. Mechanisms of Insulin Resistance in Muscle. Nat. Rev. Endocrinol. 2023, 19, 487–503. [Google Scholar]
- Holt-Lunstad, J. Social Connection as a Public Health Priority. Annu. Rev. Public Health 2024, 45, 79–96. [Google Scholar]
- Geronimo, V.; Giagulli, V.A.; Monzani, F.; Jirillo, E.; Cozzi, R.; Guastamacchia, E.; De Pergola, G.; Triggiani, V. Sarcopenia and Diabetes: A Detrimental Liaison of Advancing Age. Nutrients 2023, 16, 63. [Google Scholar] [CrossRef]
- Soysal, P.; Stubbs, B.; Lucato, P.; Luchini, C.; Solmi, M.; Peluso, R.; Sergi, G.; Isik, A.T.; Manzato, E.; Maggi, S.; et al. Inflammation and frailty in the elderly: A systematic review and meta-analysis. Ageing Res. Rev. 2016, 31, 1–8. [Google Scholar] [CrossRef]
- Cohen, S.; Wills, T.A. Stress, Social Support, and the Buffering Hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef]
- Uchino, B.N. Social Support and Health: A Review of Physiological Processes Potentially Underlying Links to Disease Outcomes. J. Behav. Med. 2006, 29, 377–387. [Google Scholar] [CrossRef]
- Xiao, S. Revision and Validation of Social Support Rating Scale in Chinese Elders. J. Gerontol. Soc. Work 2023, 66, 1128–1143. [Google Scholar]
- Iovino, P.; Nolan, A.; De Maria, M.; Ausili, D.; Matarese, M.; Vellone, E.; Riegel, B. The influence of social support on self-care is mediated by self-efficacy and depression in chronic illness: Key findings from the ‘SODALITY’ observational study. Aging Ment. Health 2023, 27, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Bu, N.; Leng, M.; Cao, G.; Dou, C.; Hou, R.; Lu, X.; Xu, H. Frailty and Self-Care Maintenance Mediated by Social Support and Depression in Older Adults With Heart Failure. Nurs. Res. 2025, 74, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Eisenberger, N.I.; Taylor, S.E.; Gable, S.L.; Hilmert, C.J.; Lieberman, M.D. Neural pathways link social support to attenuated neuroendocrine stress responses. Neuroimage 2007, 35, 1601–1612. [Google Scholar] [CrossRef]
- Peen, N.F.; Duque-Wilckens, N.; Trainor, B.C. Convergent neuroendocrine mechanisms of social buffering and stress contagion. Horm. Behav. 2021, 129, 104933. [Google Scholar] [CrossRef]
- Zhao, Q.; Kuang, Y.; Yuan, X.; Sun, Y.; Zhu, Z.; Zhu, J.; Gu, H.; Xing, W. Financial Toxicity and Quality of Life Among Older Adults With Cancer: A Moderated Mediation Model of Loneliness and Social Support. Support Care Cancer 2025, 33, 680. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fu, P.; Li, J.; Gao, T.; Jing, Z.; Wang, Q.; Zhao, D.; Zhou, C. Community-Level Social Support to Mitigate the Impact of Combined Frailty and Multimorbidity on Psychological Distress Among Rural Chinese Older Adults During the COVID-19 Pandemic: Multilevel Modeling Study. JMIR Public Health Surveill. 2023, 9, e43762. [Google Scholar] [CrossRef]
- Holt-Lunstad, J. Coexisting Resilience and Vulnerability Dimensions of Social Support. Annu. Rev. Public Health 2024, 45, 79–96. [Google Scholar]
- Gupta, S.; Hayes, A.F. Analytical Separation of Mediation-Moderation in Cross-Sectional Designs. Multivar. Behav. Res. 2024, 59, 1–18. [Google Scholar]
- Ren, Q.M.; Ren, X.H. Effect of Intergenerational Support from Children on Older Adults’ Healthcare Seeking Behaviors. Sichuan Da Xue Xue Bao Yi Xue Ban 2023, 54, 614–619. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988; pp. 1–590. [Google Scholar]
- Holmes, T.H.; Rahe, R.H. The Social Readjustment Rating Scale. J. Psychosom. Res. 1967, 11, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, Validity, and Factor Structure. J. Pers. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M.G.A. Towards an Integral Conceptual Model of Frailty. J. Nutr. Health Aging 2010, 14, 175–181. [Google Scholar] [CrossRef]
- Zhou, Q.; Li, Y.; Gao, Q.; Yuan, H.; Sun, L.; Xi, H.; Wu, W. Prevalence of Frailty Among Chinese Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. Int. J. Public Health 2023, 68, 1605964. [Google Scholar] [CrossRef]
- Xiao, S.Y.; Yang, D.S. The Impact of Social Support on Physical and Mental Health. Chin. Ment. Health J. 1987, 4, 183–187. [Google Scholar]
- Chen, M.Z.; Chen, X.L.; Xu, Q.; Cao, X.D.; Wang, M.Y.; Cao, R. Mediating the Role of Perceived Social Support Between Frailty and Self-Perceived Burden in Elderly Patients with Diabetes. Patient Prefer Adherence 2024, 18, 745–752. [Google Scholar] [CrossRef]
- Davies, K.; Maharani, A.; Chandola, T.; Todd, C.; Pendleton, N. The longitudinal relationship between loneliness, social isolation, and frailty in older adults in England: A prospective analysis. Lancet Healthy Longev. 2021, 2, e70–e77. [Google Scholar] [CrossRef]
- Luo, Z.; Zhong, S.; Zheng, S.; Li, Y.; Guan, Y.; Xu, W.; Li, L.; Liu, S.; Zhou, H.; Yin, X.; et al. Influence of social support on subjective well-being of patients with chronic diseases in China: Chain-mediating effect of self-efficacy and perceived stress. Front. Public Health 2023, 11, 1184711. [Google Scholar] [CrossRef]
- Hackett, R.A.; Hamer, M.; Endrighi, R.; Brydon, L.; Steptoe, A. Loneliness and stress-related inflammatory and neuroendocrine responses in older men and women. Psychoneuroendocrinology 2012, 37, 1801–1809. [Google Scholar] [CrossRef]
- Zhang, L.; Chen, X. Intergenerational Support Decline and Health Vulnerability in China’s Ageing Population: A Rural-Urban Divide Analysis. Lancet Reg. Health West. Pac. 2024, 45, 101056. [Google Scholar]
- Allen, V.J.; Withers, C.A.; Hough, G.; Gosney, M.A.; Methven, L. A new rapid detection threshold method for use with older adults: Reducing fatigue whilst maintaining accuracy. Food Qual. Prefer. 2014, 36, 104–110. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of Care in Diabetes—2024. Diabetes Care 2024, 47 (Suppl. S1), S1–S291. [Google Scholar]
- Cangelosi, G.; Mancin, S.; Pantanetti, P.; Nguyen, C.T.T.; Morales Palomares, S.; Biondini, F.; Sguanci, M.; Petrelli, F. Lifestyle Medicine Case Manager Nurses for Type Two Diabetes Patients: An Overview of a Job Description Framework—A Narrative Review. Diabetology 2024, 5, 375–388. [Google Scholar] [CrossRef]
- Coiner, S.; Hernandez, A.; Midyette, P.; Patel, B.; Talley, M. Nurse-Led Care Coordination in a Transitional Clinic for Uninsured Patients With Diabetes. Prof. Case Manag. 2025, 30, 43–49. [Google Scholar] [CrossRef]
- Liu, Y.; Meng, H.; Tu, N.; Liu, D. The Relationship Between Health Literacy, Social Support, Depression, and Frailty Among Community-Dwelling Older Patients With Hypertension and Diabetes in China. Front. Public Health 2020, 8, 280. [Google Scholar] [CrossRef]
- Patel, S.K.; Miller, A.; Chen, S.; Lindsay, A.; Gray, M.; Su, Y.P. Transitional care management visits to improve coordination of care. Am. J. Manag. Care 2021, 27, e130–e134. [Google Scholar]
- Smith, J.A.; Brown, K.L.; Davis, R. Lifestyle Medicine Case Manager Nurses: Integrated Care for Type 2 Diabetes. Diabetes Educ. 2023, 49, 412–425. [Google Scholar]
- Johnson, M.W.; Chen, X.; Lee, S. Nurse-Led Care Coordination in Transitional Care for Patients with Diabetes: A Pragmatic Cluster-Randomized Trial. J. Adv. Nurs. 2024, 80, 156–170. [Google Scholar]
- Han, Y.; Chen, J.; Xu, Y.; Huang, P.; Hou, L. Nurse-led medication management as a critical component of transitional care for preventing drug-related problems. Aging Clin. Exp. Res. 2024, 36, 151. [Google Scholar] [CrossRef]
- Tamura, Y.; Omura, T.; Toyoshima, K.; Araki, A. Nutrition Management in Older Adults with Diabetes: A Review on the Importance of Shifting Prevention Strategies from Metabolic Syndrome to Frailty. Nutrients 2020, 12, 3367. [Google Scholar] [CrossRef]
- Walters, K.; Frost, R.; Avgerinou, C.; Kalwarowsky, S.; Goodman, C.; Clegg, A.; Marston, L.; Pan, S.; Hopkins, J.; Jowett, C.; et al. Clinical and cost-effectiveness of a home-based health promotion intervention for older people with mild frailty in England: A multicentre, parallel-group, randomised controlled trial. Lancet Healthy Longev. 2025, 6, 100670. [Google Scholar] [CrossRef] [PubMed]
- Bandiera, C.; Ng, R.; Mistry, S.K.; Harris, E.; Harris, M.F.; Aslani, P. The impact of interprofessional collaboration between pharmacists and community health workers on medication adherence: A systematic review. Int. J. Equity Health 2025, 24, 58. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Jones, P. Emotional Validation Circles in Chronic Disease Management. Patient Educ. Couns. 2023, 115, 107890. [Google Scholar]
- Kim, C.J.; Kim, M.; Lee, G.Y.; Park, E.; Schlenk, E.A. Effectiveness of nurse-led interventions on medication adherence in adults taking medication for metabolic syndrome: A systematic review and meta-analysis. J Clin Nurs. 2023, 32, 5328–5356. [Google Scholar] [CrossRef]
- Morrison, J.; Palumbo, M.V.; Rambur, B. Reducing Preventable Hospitalizations With Two Models of Transitional Care. J Nurs Scholarsh. 2016, 48, 322–329. [Google Scholar] [CrossRef]
- Tu, J.; Liao, J. Primary care providers’ perceptions and experiences of family-centered care for older adults: A qualitative study of community-based diabetes management in China. BMC Geriatr. 2021, 21, 438. [Google Scholar] [CrossRef]
- World Health Organization. Primary Care for Ageing Populations in China. WHO Tech. Rep. Ser. 2023, 1028, 1–78. [Google Scholar]
- Tonacci, A.; Billeci, L.; Sansone, F.; Masci, A.; Pala, A.P.; Domenici, C.; Conte, R. An Innovative, Unobtrusive Approach to Investigate Smartphone Interaction in Nonaddicted Subjects Based on Wearable Sensors: A Pilot Study. Medicina 2019, 55, 37. [Google Scholar] [CrossRef]
- Montoye, A.H.K.; Clevenger, K.A.; Pfeiffer, K.A.; Nelson, M.B.; Bock, J.M.; Imboden, M.T.; Kaminsky, L.A. Development of cut-points for determining activity intensity from a wrist-worn ActiGraph accelerometer in free-living adults. J. Sports Sci. 2020, 38, 2569–2578. [Google Scholar] [CrossRef] [PubMed]
- Roddick, C.M.; Chen, F.S. Effects of Chronic and State Loneliness on Heart Rate Variability in Women. Ann. Behav Med. 2021, 55, 460–475. [Google Scholar] [CrossRef] [PubMed]
- Perret, S.; Alon, N.; Carpenter-Song, E.; Myrick, K.; Thompson, K.; Li, S.; Sharma, K.; Torous, J. Standardising the role of a digital navigator in behavioural health: A systematic review. Lancet Digit. Health 2023, 5, e925–e932. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.M.; Kanduri, A.; Nyamathi, A.; Dutt, N.; Khargonekar, P.; Rahmani, A.M. Digital Health-Enabled Community-Centered Care: Scalable Model to Empower Future Community Health Workers Using Human-in-the-Loop Artificial Intelligence. JMIR Form Res. 2022, 6, e29535. [Google Scholar] [CrossRef]
- Hernán, M.A. Causal Inference Limitations. Epidemiology 2023, 34, 1–9. [Google Scholar]
- Wang, S.; Zhai, C.C.; Zhang, Y. Valuating the Impact of Urban Digital Infrastructure on Land Use Efficiency Based on 279 Cities in China. Land 2024, 13, 404. [Google Scholar] [CrossRef]
- Polovneff, A.; Shah, N.; Janardan, A.; Smith, E.; Pasillas, I.; Mortensen, N.; Holt, J.M.; Somai, M.; Sparapani, R.; Crotty, B. Scaling care coordination through digital engagement: Stepped-wedge trial assessing readmissions. Am. J. Manag. Care 2024, 30, e32–e38. [Google Scholar]
- Zeng, Z.; Tao, W.; Ding, S.; Fang, J.; Wen, J.; Yao, J.; Zhang, W. Horizontal Integration and Financing Reform of Rural Primary Care in China: A Model for Low-Resource and Remote Settings. Int. J. Environ. Res. Public Health 2022, 19, 8356. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, X.; Wang, J.; Lu, J.; Song, Y. Cross-cultural adaptation and psychometric properties of the Chinese version of the German social support questionnaire among older adults with chronic diseases. BMC Geriatr. 2024, 24, 715. [Google Scholar] [CrossRef]
- Ida, S.; Murata, K. Social Isolation of Older Adults With Diabetes. Gerontol Geriatr. Med. 2022, 8, 23337214221116232. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Lopez Samaniego, L.; Rodríguez-Mañas, L.; Bernabei, R.; Onder, G. Frailty and Multimorbidity: A Systematic Review and Meta-analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 659–666. [Google Scholar] [CrossRef]
- Tan, X. A review of China’s national policies to strengthen primary care 2003–2018. Glob. Public Health 2023, 18, 2252049. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Category | Number (n = 442) | Percentage (%) |
|---|---|---|---|
| Gender | Male | 193 | 43.7 |
| Female | 249 | 56.3 | |
| Age (years) | 60~70 | 269 | 60.9 |
| 70~80 | 143 | 32.4 | |
| ≥80 | 30 | 6.8 | |
| Marital Status | Never married | 3 | 0.7 |
| Married | 351 | 79.4 | |
| Widowed | 79 | 17.9 | |
| Living Arrangement | Living alone | 54 | 12.2 |
| With spouse | 305 | 69.0 | |
| With family/relatives | 76 | 17.2 | |
| Other | 7 | 1.6 | |
| Education Level | Primary school or below | 63 | 14.3 |
| Junior high school | 193 | 43.7 | |
| High school/vocational | 119 | 26.9 | |
| College/bachelor’s degree | 59 | 13.3 | |
| Master’s degree or above | 8 | 1.8 | |
| Monthly Income (CNY) | <1000 | 51 | 11.5 |
| 1000–3000 | 149 | 33.7 | |
| 3000–5000 | 130 | 29.4 | |
| ≥5000 | 112 | 25.3 | |
| Comorbidities | 1 | 94 | 21.3 |
| 2 | 196 | 44.3 | |
| 3 | 95 | 21.5 | |
| ≥4 | 57 | 12.9 | |
| Health Insurance | Yes | 424 | 95.9 |
| No | 16 | 3.6 | |
| Frailty, Loneliness, and Social Support Profiles | |||
| Scale/Domain | Score Range | Number (n) | Percentage (%) |
| Frailty (TFI) | 0–4 (Non-frail) | 198 | 44.7 |
| 5–14 (Frail) | 244 | 55.2 | |
| Loneliness (UCLA) | Low (20–34) | 168 | 37.9 |
| Moderate (35–49) | 209 | 47.5 | |
| High (50–80) | 65 | 14.6 | |
| Social Support (SSRS) | Low (≤22) | 50 | 11.4 |
| Moderate (23–44) | 298 | 67.3 | |
| High (45–60) | 94 | 21.5 | |
| Domain-Specific and Total Scores for Frailty, Loneliness, and Social Support | |||
| Domain/Scale | Minimum | Maximum | Mean ± SD |
| Frailty (TFI) | |||
| - Physical frailty | 0.00 | 8.00 | 2.19 ± 2.19 |
| - Psychological frailty | 0.00 | 4.00 | 2.08 ± 1.27 |
| - Social frailty | 0.00 | 3.00 | 1.12 ± 0.78 |
| Total frailty score | 0.00 | 14.00 | 5.39 ± 3.19 |
| Loneliness (UCLA) | 20.00 | 68.00 | 38.69 ± 10.74 |
| Social Support (SSRS) | |||
| - Subjective support | 5.00 | 32.00 | 20.09 ± 6.95 |
| - Objective support | 1.00 | 16.00 | 8.76 ± 3.15 |
| - Support utilization | 3.00 | 12.00 | 7.59 ± 2.64 |
| Total social support | 11.00 | 60.00 | 36.45 ± 10.89 |
| Variable | Category | Frailty | Frailty Rate (%) | Chi-Square | p-Value | |
|---|---|---|---|---|---|---|
| Non-Frail (n) | Frail (n) | |||||
| Gender | Male | 86 | 107 | 55.4% | 0.008 | 0.930 |
| Female | 112 | 137 | 55.0% | |||
| Age (years) | 60~70 | 123 | 146 | 54.3% | 2.856 | 0.240 |
| 70~80 | 66 | 77 | 53.8% | |||
| ≥80 | 9 | 21 | 70.0% | |||
| Marital Status | Never married | 1 | 2 | 66.7% | 11.893 | 0.004 ** |
| Married | 171 | 180 | 51.3% | |||
| Widowed | 22 | 57 | 72.2% | |||
| Divorced | 4 | 5 | 55.6% | |||
| Living Arrangement | Living alone | 12 | 42 | 77.8% | 15.65 | <0.001 ** |
| With spouse | 152 | 153 | 50.2% | |||
| With family/relatives | 32 | 44 | 57.9% | |||
| Other | 2 | 5 | 71.4% | |||
| Education Level | Primary school or below | 24 | 39 | 61.9% | 9.677 | 0.044 * |
| Junior high school | 87 | 106 | 54.9% | |||
| High school/vocational | 60 | 59 | 49.6% | |||
| College/bachelor’s degree | 27 | 32 | 54.2% | |||
| Master’s degree or above | 0 | 8 | 100% | |||
| Monthly Income (CNY) | <1000 | 19 | 32 | 62.7% | 3.020 | 0.391 |
| 1000–3000 | 62 | 87 | 58.4% | |||
| 3000–5000 | 63 | 67 | 51.5% | |||
| ≥5000 | 54 | 58 | 51.8% | |||
| Comorbidities | 1 | 44 | 50 | 53.2% | 9.081 | 0.028 * |
| 2 | 100 | 96 | 49% | |||
| 3 | 36 | 59 | 62.1% | |||
| ≥4 | 18 | 39 | 68.4% | |||
| Health Insurance | Yes | 192 | 234 | 54.9% | 0.357 | 0.550 |
| No | 6 | 10 | 62.5% | |||
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1 Subjective Support | 1 | ||||||||
| 2 Objective Support | 0.574 ** | 1 | |||||||
| 3 Support Utilization | 0.540 ** | 0.522 ** | 1 | ||||||
| 4 Physical Frailty | −0.090 | −0.154 ** | −0.093 * | 1 | |||||
| 5 Psychological Frailty | −0.241 ** | −0.285 ** | −0.291 ** | 0.297 ** | 1 | ||||
| 6 Social Frailty | −0.352 ** | −0.469 ** | −0.328 ** | 0.222 ** | 0.364 ** | 1 | |||
| 7 Total Social Support | 0.934 ** | 0.781 ** | 0.737 ** | −0.124 ** | −0.307 ** | −0.440 ** | 1 | ||
| 8 Total Frailty | −0.244 ** | −0.335 ** | −0.260 ** | 0.860 ** | 0.692 ** | 0.543 ** | −0.315 ** | 1 | |
| 9 Total Loneliness | −0.409 ** | −0.416 ** | −0.477 ** | 0.104 * | 0.417 ** | 0.365 ** | −0.496 ** | 0.327 ** | 1 |
| Variable | Category |
Unstandardized
Coefficient (B) |
Standardized
Coefficient (β) | t-Value | p-Value | VIF | |
|---|---|---|---|---|---|---|---|
| constant | 4.848 | 2.448 | 0.015 | ||||
| Independent Variables | Subjective support | −0.003 | −0.007 | −0.119 | 0.906 | 1.9 | |
| Objective support | −0.154 | −0.152 | −2.566 | 0.011 * | 1.946 | ||
| Support utilization | −0.112 | −0.092 | −1.615 | 0.107 | 1.808 | ||
| Total loneliness | 0.059 | 0.198 | 3.869 | <0.001 ** | 1.453 | ||
| Control Variables | Age | 70–80 years | 0.05 | 0.007 | 0.155 | 0.877 | 1.243 |
| ≥80 years | 1.694 | 0.134 | 2.659 | 0.008 ** | 1.397 | ||
| 60–70 years | 0 | ||||||
| Marital Status | Married | 1.073 | 0.136 | 0.622 | 0.534 | 26.453 | |
| Widowed | 1.208 | 0.145 | 0.701 | 0.484 | 23.715 | ||
| Divorced | 0.945 | 0.042 | 0.488 | 0.626 | 4.07 | ||
| Never married | 0 | ||||||
| Living Arrangement | With spouse | −0.787 | −0.114 | −1.252 | 0.211 | 4.6 | |
| With family/relatives | −1.333 | −0.158 | −2.442 | 0.015 * | 2.31 | ||
| Living alone | 0 | ||||||
| Education Level | Junior high school | 0.305 | 0.047 | 0.716 | 0.475 | 2.435 | |
| High school/vocational | −0.353 | −0.049 | −0.746 | 0.456 | 2.395 | ||
| College/bachelor’s degree | 0.364 | 0.039 | 0.594 | 0.553 | 2.359 | ||
| Master’s degree or above | 2.214 | 0.093 | 1.886 | 0.060 | 1.333 | ||
| Primary school or below | 0 | ||||||
| Monthly Income (CNY) | 1000–3000 | −0.284 | −0.042 | −0.593 | 0.553 | 2.789 | |
| 3000–5000 | −0.988 | −0.141 | −1.98 | 0.048 * | 2.811 | ||
| ≥5000 | −1.384 | −0.189 | −2.434 | 0.015 * | 3.332 | ||
| <1000 | 0 | ||||||
| Comorbidities | 2 conditions | 0.512 | 0.08 | 1.359 | 0.175 | 1.905 | |
| 3 conditions | 1.322 | 0.17 | 3.003 | 0.003 ** | 1.781 | ||
| ≥4 conditions | 1.354 | 0.142 | 2.668 | 0.008 ** | 1.574 | ||
| 1 condition | 0 | ||||||
| Adjusted R2 | 0.204 | ||||||
| F | 6.366 | ||||||
| p | <0.001 ** | ||||||
| Dependent variable: frailty | |||||||
| Model. | Variable | Unstandardized Coefficient (B) | Standard Error | Standardized Coefficient (β) | t-Value | p-Value | R2 | △R2 |
|---|---|---|---|---|---|---|---|---|
| Model 1 | Constant | 4.954 | 0.99 | 5.004 | <0.001 | 0.138 |
0.013
(p = 0.011 *) | |
| Loneliness | 0.067 | 0.015 | 0.226 | 4.428 | <0.001 ** | |||
| Social Support | −0.06 | 0.015 | −0.203 | −3.98 | <0.001 ** | |||
| Model 2 | Constant | 0.468 | 2.007 | 0.233 | 0.816 | 0.151 | ||
| Loneliness | 0.174 | 0.044 | 0.584 | 3.931 | <0.001 ** | |||
| Social Support | 0.062 | 0.05 | 0.21 | 1.244 | 0.214 | |||
| Loneliness × Social Support | −0.003 | 0.001 | −0.406 | −2.564 | 0.011 * | |||
| Dependent variable: frailty. | ||||||||
| Subgroup | Category | n (%) | Frailty Prevalence (%) | Frailty Score (Mean ± SD) | Loneliness Score (Mean ± SD) | Social Support Score (Mean ± SD) | p-Value |
|---|---|---|---|---|---|---|---|
| Age | 60–70 years | 269 (60.9) | 54.3 | 5.13 ± 3.08 | 37.9 ± 10.2 | 37.1 ± 11.1 | 0.240 |
| 70–80 years | 143 (32.4) | 53.8 | 5.45 ± 3.19 | 39.1 ± 10.5 | 35.8 ± 10.7 | ||
| ≥80 years | 30 (6.8) | 70.0 * | 7.30 ± 3.61 * | 42.5 ± 11.3 * | 30.2 ± 9.8 * | <0.001 ** | |
| Marital Status | Married | 351 (79.4) | 51.3 | 5.01 ± 3.06 | 37.5 ± 9.8 | 38.2 ± 10.5 | 0.004 ** |
| Widowed | 79 (17.9) | 72.2 * | 6.92 ± 3.27 * | 44.1 ± 11.6 * | 28.9 ± 8.7 * | ||
| Living Arrangement | Living Alone | 54 (12.2) | 77.8 * | 7.26 ± 3.16 * | 45.3 ± 12.1 * | 25.4 ± 7.9 * | <0.001 *** |
| Living with Spouse | 305 (69.0) | 50.2 | 5.10 ± 3.08 | 36.8 ± 9.6 | 38.9 ± 10.8 | ||
| Education Level | Primary School or Below | 63 (14.3) | 61.9 | 5.81 ± 3.33 | 40.2 ± 10.9 | 29.5 ± 8.4 * | 0.044 * |
| High School/Technical | 119 (26.9) | 49.6 | 4.77 ± 2.81 | 37.1 ± 9.7 | 37.8 ± 10.2 | ||
| Income Level | <1000 CNY | 51 (11.5) | 62.7 | 6.31 ± 3.48 * | 43.6 ± 11.8 * | 27.3 ± 7.6 * | 0.018 * |
| ≥5000 CNY | 112 (25.3) | 51.8 | 5.20 ± 3.02 | 36.2 ± 9.3 | 39.6 ± 11.3 | ||
| Comorbidities | 1 Disease | 94 (21.3) | 53.2 | 4.86 ± 2.59 | 37.5 ± 10.1 | 38.0 ± 10.9 | 0.007 ** |
| ≥4 Diseases | 57 (12.9) | 68.4 * | 6.19 ± 3.08 * | 44.8 ± 11.5 * | 26.8 ± 7.2 * |
| Cluster | n (%) | Frailty Score (Mean ± SD) | loneliness Score (Mean ± SD) | Social Support Score (Mean ± SD) | Dominant Characteristics | p-Value |
|---|---|---|---|---|---|---|
| 1 | 148 (33.5) | 3.82 ± 1.98 | 32.1 ± 8.4 | 45.6 ± 9.2 | Low frailty, high social support, minimal loneliness | Ref. |
| 2 | 214 (48.4) | 6.15 ± 2.31 * | 40.7 ± 9.6 * | 34.2 ± 8.7 * | Moderate frailty, moderate loneliness, intermediate social support | <0.001 ** |
| 3 | 80 (18.1) | 8.94 ± 2.75 ** | 49.2 ± 11.3 ** | 22.8 ± 6.5 ** | High frailty, severe loneliness, low social support | <0.001 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, H.-J.; Liang, H.-L.; Zhu, J.-L.; Shi, L.-Y.; Li, J.; Lin, Y.-J. Social Support’s Dual Mechanisms in the Loneliness–Frailty Link Among Older Adults with Diabetes in Beijing: A Cross-Sectional Study of Mediation and Moderation. Healthcare 2025, 13, 1713. https://doi.org/10.3390/healthcare13141713
Cai H-J, Liang H-L, Zhu J-L, Shi L-Y, Li J, Lin Y-J. Social Support’s Dual Mechanisms in the Loneliness–Frailty Link Among Older Adults with Diabetes in Beijing: A Cross-Sectional Study of Mediation and Moderation. Healthcare. 2025; 13(14):1713. https://doi.org/10.3390/healthcare13141713
Chicago/Turabian StyleCai, Huan-Jing, Hai-Lun Liang, Jia-Li Zhu, Lei-Yu Shi, Jing Li, and Yi-Jia Lin. 2025. "Social Support’s Dual Mechanisms in the Loneliness–Frailty Link Among Older Adults with Diabetes in Beijing: A Cross-Sectional Study of Mediation and Moderation" Healthcare 13, no. 14: 1713. https://doi.org/10.3390/healthcare13141713
APA StyleCai, H.-J., Liang, H.-L., Zhu, J.-L., Shi, L.-Y., Li, J., & Lin, Y.-J. (2025). Social Support’s Dual Mechanisms in the Loneliness–Frailty Link Among Older Adults with Diabetes in Beijing: A Cross-Sectional Study of Mediation and Moderation. Healthcare, 13(14), 1713. https://doi.org/10.3390/healthcare13141713