
Psychological Assessment and Psychosocial Outcomes in Bariatric Surgery Candidates: A Retrospective Study

 ,
,  ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Inclusion and Exclusion Criteria
2.4. Instruments
2.5. Statistical Analysis
3. Results
3.1. Descriptive Analysis
3.2. Psychological and Functional Assessment
3.3. Correlation
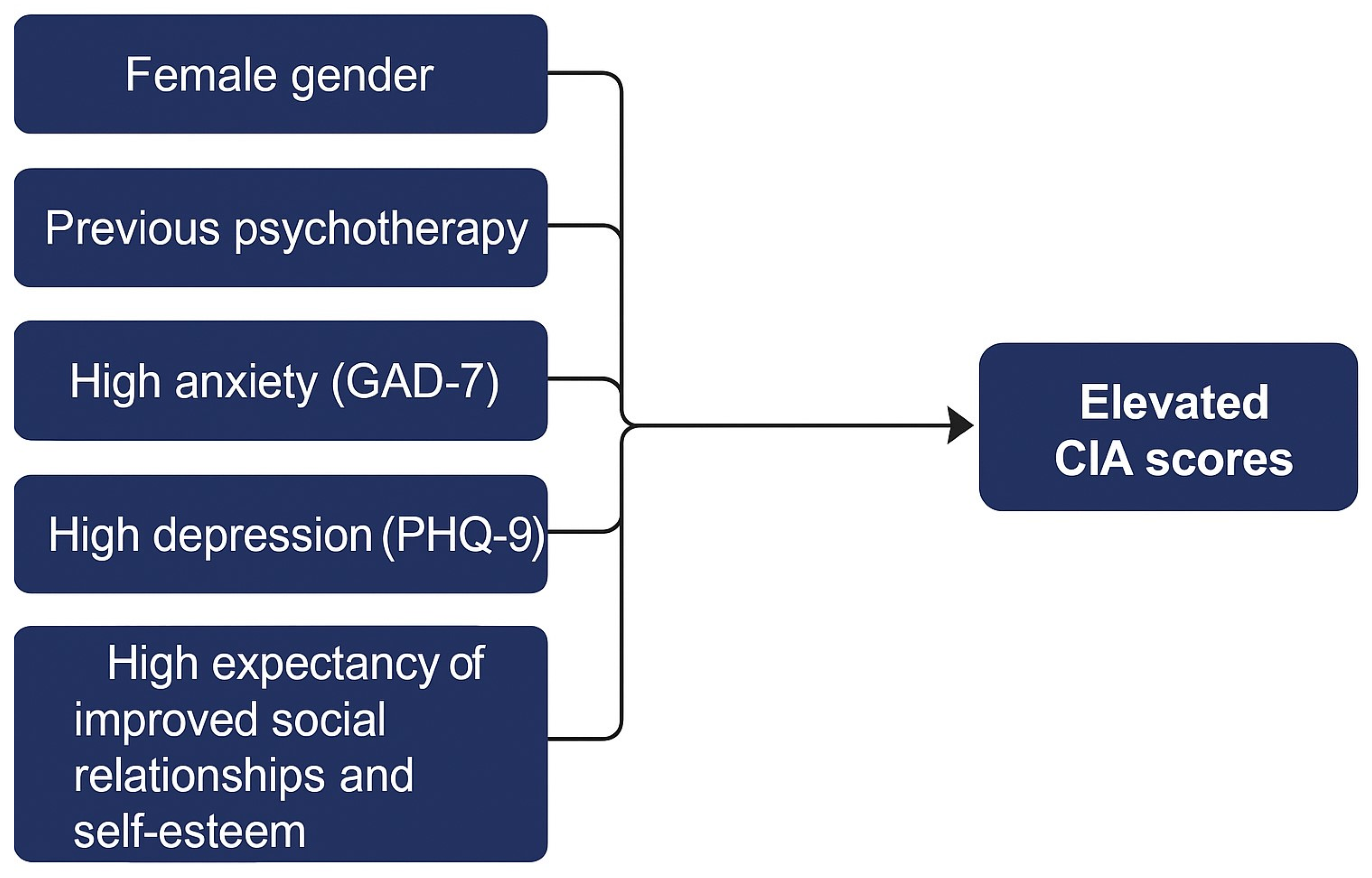
3.4. Factors Associated with CIA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| EWLR | expectations regarding weight loss |
| CIA | Clinical Impairment Assessment |
| PHQ-9 | Patient Health Questionnaire-9 |
| GAD-7 | Generalized Anxiety Disorder Questionnaire-7 |
| IQR | interquartile range |
| OLS | ordinary least squares |
| BIC | Bayesian Information Criterion |
| LRT | likelihood ratio test |
References
- Sarwer, D.B.; Heinberg, L.J. A Review of the Psychosocial Aspects of Clinically Severe Obesity and Bariatric Surgery. Am. Psychol. 2020, 75, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Aoki, Y.; Ogden, C.L. Differences in Obesity Prevalence by Demographic Characteristics and Urbanization Level Among Adults in the United States, 2013–2016. JAMA 2018, 319, 2419–2429. [Google Scholar] [CrossRef] [PubMed]
- Deledda, A.; Pintus, S.; Loviselli, A.; Fosci, M.; Fantola, G.; Velluzzi, F. Nutritional Management in Bariatric Surgery Patients. Int. J. Environ. Res. Public Health 2021, 18, 12049. [Google Scholar] [CrossRef]
- van Hout, G.C.M.; van Oudheusden, I.; van Heck, G.L. Psychological Profile of the Morbidly Obese. Obes. Surg. 2004, 14, 579–588. [Google Scholar] [CrossRef]
- Courcoulas, A.P.; King, W.C.; Belle, S.H.; Berk, P.; Flum, D.R.; Garcia, L.; Gourash, W.; Horlick, M.; Mitchell, J.E.; Pomp, A.; et al. Seven-Year Weight Trajectories and Health Outcomes in the Longitudinal Assessment of Bariatric Surgery (LABS) Study. JAMA Surg. 2018, 153, 427–434. [Google Scholar] [CrossRef]
- Martinelli, V.; Chiappedi, M. Bariatric Surgery: Psychosocial Aspects and Quality of Life. Int. J. Environ. Res. Public Health 2022, 19, 16516. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Allison, K.C.; Bailer, B.; Faulconbridge, L.F.; Wadden, T.A. Bariatric Surgery. In Presurgical Psychological Screening: Understanding Patients, Improving Outcomes; American Psychological Association: Washington, DC, USA, 2013; pp. 61–83. ISBN 978-1-4338-1242-2. [Google Scholar]
- Maraldo, T.M.; Fewell, L.; Vander Wal, J.S. Factor Structure and Psychometric Properties of the Clinical Impairment Assessment 3.0 (CIA) in a Clinical Eating Disorder Sample. Eat. Behav. 2021, 40, 101469. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Polonsky, H.M. The Psychosocial Burden of Obesity. Endocrinol. Metab. Clin. N. Am. 2016, 45, 677–688. [Google Scholar] [CrossRef]
- Heinberg, L.J.; Ashton, K.; Windover, A. Moving beyond Dichotomous Psychological Evaluation: The Cleveland Clinic Behavioral Rating System for Weight Loss Surgery. Surg. Obes. Relat. Dis. 2010, 6, 185–190. [Google Scholar] [CrossRef]
- Marek, R.J.; Heinberg, L.J.; Lavery, M.; Merrell Rish, J.; Ashton, K. A Review of Psychological Assessment Instruments for Use in Bariatric Surgery Evaluations. Psychol. Assess. 2016, 28, 1142–1157. [Google Scholar] [CrossRef]
- De Luca, M.; Angrisani, L.; Himpens, J.; Busetto, L.; Scopinaro, N.; Weiner, R.; Sartori, A.; Stier, C.; Lakdawala, M.; Bhasker, A.G.; et al. Indications for Surgery for Obesity and Weight-Related Diseases: Position Statements from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Obes. Surg. 2016, 26, 1659–1696. [Google Scholar] [CrossRef] [PubMed]
- Presurgical Psychological Screening: Understanding Patients, Improving Outcomes; American Psychological Association: Washington, DC, USA, 2013; pp. xii, 296. ISBN 978-1-4338-1242-2.
- Handbook of Obesity Treatment, 2nd ed.; The Guilford Press: New York, NY, USA, 2018; pp. xx, 716. ISBN 978-1-4625-3556-9.
- Sogg, S.; Lauretti, J.; West-Smith, L. Recommendations for the Presurgical Psychosocial Evaluation of Bariatric Surgery Patients. Surg. Obes. Relat. Dis. 2016, 12, 731–749. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Youdim, A.; Jones, D.B.; Garvey, W.T.; Hurley, D.L.; McMahon, M.M.; Heinberg, L.J.; Kushner, R.; Adams, T.D.; Shikora, S.; et al. Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient—2013 Update: Cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Endocr. Pract. 2013, 19, 337–372. [Google Scholar] [CrossRef]
- Puhl, R.M.; Heuer, C.A. The Stigma of Obesity: A Review and Update. Obesity 2009, 17, 941–964. [Google Scholar] [CrossRef]
- Puhl, R.M.; Heuer, C.A. Obesity Stigma: Important Considerations for Public Health. Am. J. Public Health 2010, 100, 1019–1028. [Google Scholar] [CrossRef]
- Calugi, S.; Sartirana, M.; Milanese, C.; El Ghoch, M.; Riolfi, F.; Dalle Grave, R. The Clinical Impairment Assessment Questionnaire: Validation in Italian Patients with Eating Disorders. Eat. Weight. Disord. 2018, 23, 685–694. [Google Scholar] [CrossRef]
- Weiss, F.; Barbuti, M.; Carignani, G.; Calderone, A.; Santini, F.; Maremmani, I.; Perugi, G. Psychiatric Aspects of Obesity: A Narrative Review of Pathophysiology and Psychopathology. J. Clin. Med. 2020, 9, 2344. [Google Scholar] [CrossRef]
- Bohn, K.; Doll, H.A.; Cooper, Z.; O’Connor, M.; Palmer, R.L.; Fairburn, C.G. The Measurement of Impairment Due to Eating Disorder Psychopathology. Behav. Res. Ther. 2008, 46, 1105–1110. [Google Scholar] [CrossRef]
- Jenkins, P.E. Psychometric Validation of the Clinical Impairment Assessment in a UK Eating Disorder Service. Eat. Behav. 2013, 14, 241–243. [Google Scholar] [CrossRef]
- Dahlgren, C.L.; Stedal, K.; Rø, Ø. Eating Disorder Examination Questionnaire (EDE-Q) and Clinical Impairment Assessment (CIA): Clinical Norms and Functional Impairment in Male and Female Adults with Eating Disorders. Nord. J. Psychiatry 2017, 71, 256–261. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and Utility of a Self-Report Version of PRIME-MD: The PHQ Primary Care Study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and Standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the General Population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, D.L.; White, K.S. Understanding the Complexity of Biopsychosocial Factors in the Public Health Epidemic of Overweight and Obesity. Health Psychol. Open 2016, 3, 2055102916634364. [Google Scholar] [CrossRef]
- Kyrou, I.; Tsigos, C. Stress Mechanisms and Metabolic Complications. Horm. Metab. Res. 2007, 39, 430–438. [Google Scholar] [CrossRef]
- Pyykkö, J.E.; Aydin, Ö.; Gerdes, V.E.A.; Acherman, Y.I.Z.; Groen, A.K.; van de Laar, A.W.; Nieuwdorp, M.; Sanderman, R.; Hagedoorn, M. Psychological Functioning and Well-Being before and after Bariatric Surgery; What Is the Benefit of Being Self-Compassionate? Br. J. Health Psychol. 2022, 27, 96–115. [Google Scholar] [CrossRef]
- Puhl, R.; Suh, Y. Health Consequences of Weight Stigma: Implications for Obesity Prevention and Treatment. Curr. Obes. Rep. 2015, 4, 182–190. [Google Scholar] [CrossRef]
- Gonçalves, I.d.S.A.; Filgueiras, M.D.S.; Moreira, T.R.; Thomé, M.S.; Paiva, G.L.D.; Almeida, G.P.d.; Cotta, R.M.M.; Campos, T.d.N.; Freitas, D.M.d.O.; Novaes, J.F.d.; et al. Interrelation of Stress, Eating Behavior, and Body Adiposity in Women with Obesity: Do Emotions Matter? Nutrients 2024, 16, 4133. [Google Scholar] [CrossRef]
- Causes of Emotional Eating and Matched Treatment of Obesity-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/29696418/ (accessed on 27 April 2025).
- Simon, G.E.; Von Korff, M.; Saunders, K.; Miglioretti, D.L.; Crane, P.K.; van Belle, G.; Kessler, R.C. Association between Obesity and Psychiatric Disorders in the US Adult Population. Arch. Gen. Psychiatry 2006, 63, 824–830. [Google Scholar] [CrossRef]
- Balantekin, K.N.; Grammer, A.C.; Fitzsimmons-Craft, E.E.; Eichen, D.E.; Graham, A.K.; Monterubio, G.E.; Firebaugh, M.-L.; Karam, A.M.; Sadeh-Sharvit, S.; Goel, N.J.; et al. Overweight and Obesity Are Associated with Increased Eating Disorder Correlates and General Psychopathology in University Women with Eating Disorders. Eat. Behav. 2021, 41, 101482. [Google Scholar] [CrossRef]
- van Hout, G.C.M.; Boekestein, P.; Fortuin, F.A.M.; Pelle, A.J.M.; van Heck, G.L. Psychosocial Functioning Following Bariatric Surgery. Obes. Surg. 2006, 16, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Wingo, B.C.; Desmond, R.A.; Brantley, P.; Appel, L.; Svetkey, L.; Stevens, V.J.; Ard, J.D. Self-Efficacy as a Predictor of Weight Change and Behavior Change in the PREMIER Trial. J. Nutr. Educ. Behav. 2013, 45, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.K.; Rai, M.; Rehkopf, D.H.; Abrams, B. Educational Attainment and Obesity: A Systematic Review. Obes. Rev. 2013, 14, 989–1005. [Google Scholar] [CrossRef] [PubMed]
- Patsalos, O.; Keeler, J.; Schmidt, U.; Penninx, B.W.J.H.; Young, A.H.; Himmerich, H. Diet, Obesity, and Depression: A Systematic Review. J. Pers. Med. 2021, 11, 176. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Frequency | Percentage | |
|---|---|---|---|
| Gender | Male | 184 | 29.73 |
| Female | 435 | 70.27 | |
| Marital status | Single | 189 | 30.53 |
| Separated | 67 | 10.82 | |
| Married/cohabiting | 357 | 57.67 | |
| Widowed | 6 | 0.97 | |
| Educational level | First school | 4 | 0.65 |
| Bachelor’s degree | 114 | 18.42 | |
| Middle School | 149 | 24.07 | |
| High school | 352 | 56.87 | |
| Employment status | No | 192 | 31.02 |
| Yes | 427 | 68.98 | |
| Variable | Frequency | Percentage | |
|---|---|---|---|
| Onset of weight issues | Teenaging | 203 | BMI (kg/m2) 32.79 |
| Adult | 252 | BMI (kg/m2) 41.11 | |
| Infant | 164 | BMI (kg/m2) 26.49 | |
| Past dietary regimens | No | 35 | 5.65 |
| Yes | 584 | 94.35 | |
| Weight loss treatments | No | 507 | 81.91 |
| Yes | 112 | 18.09 | |
| Family history of obesity | No | 258 | 41.68 |
| Yes | 361 | 58.32 | |
| Smoking status | No | 453 | 73.18 |
| Yes | 166 | 26.82 | |
| Psychotherapy | No | 377 | 60.90 |
| Yes | 242 | 39.10 | |
| Current psychotropic drugs | No | 532 | 85.95 |
| Yes | 87 | 14.05 | |
| Weight loss expectations—social relationships | No | 373 | 60.26 |
| Yes | 246 | 39.74 | |
| Weight loss expectations—self-esteem | No | 263 | 42.49 |
| Yes | 356 | 57.51 | |
| Weight loss expectations—work | No | 520 | 84.01 |
| Yes | 99 | 15.99 | |
| Physical activity | No | 476 | 76.90 |
| Yes | 143 | 23.10 | |
| Reason for treatment initiation—health | No | 1 | 0.16 |
| Yes | 618 | 99.84 | |
| Reason for treatment initiation—aesthetics | No | 233 | 37.64 |
| Yes | 386 | 62.36 | |
| Category | GAD-7 Score (n, %) | PHQ-9 Score (n, %) |
|---|---|---|
| Absent | 258 (41.68%) | 212 (30.8%) |
| Mild | 213 (34.41%) | 288 (41.9%) |
| Moderate | 98 (15.83%) | 132 (19.2%) |
| Severe | 50 (8.08%) | 54 (7.85%) |
| Variable | Beta | SE | t-Value | p-Value |
|---|---|---|---|---|
| Intercept | −2.578 | 1.821 | −1.415 | 0.166 |
| Gender (female) | 1.075 | 0.571 | 1.882 | 0.029 |
| Past dietary regimens (yes) | 2.421 | 1.103 | 2.194 | 0.091 |
| Weight loss treatments (yes) | −1.085 | 0.666 | −1.629 | 0.124 |
| Psychotherapy (yes) | 1.183 | 0.567 | 2.085 | 0.044 |
| Current psychotropic drugs (yes) | 1.245 | 0.786 | 1.592 | 0.156 |
| Weight loss expectations improve social relationships (yes) | 1.976 | 0.596 | 3.311 | 0.002 |
| Weight loss expectations improve self-esteem (yes) | 2.114 | 0.592 | 3.56 | 0.001 |
| Physical activity (yes) | −1.228 | 0.607 | −2.021 | 0.050 |
| Reason for treatment initiation aesthetics (yes) | 0.920 | 0.553 | 1.664 | 0.120 |
| EWLR | 0.312 | 0.153 | 2.037 | 0.024 |
| GAD-7 (moderate anxiety) | 3.853 | 0.910 | 4.233 | 0.000 |
| GAD-7 (severe anxiety) | 3.135 | 1.210 | 2.591 | 0.035 |
| GAD-7 (mild anxiety) | 1.466 | 0.662 | 2.212 | 0.035 |
| PHQ-9 (mild) | 3.727 | 0.680 | 5.479 | <0.001 |
| PHQ-9 (moderate) | 8.754 | 0.925 | 9.461 | <0.001 |
| PHQ-9 (severe) | 16.673 | 1.323 | 12.601 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magurano, M.R.; Napolitano, D.; Bozzetti, M.; Lo Cascio, A.; Oppo, L.; Fernandez Tayupanta, L.A.; Ferrazzoli, S.; Lopasso, L.; Rellini, E.; Raffaelli, M.; et al. Psychological Assessment and Psychosocial Outcomes in Bariatric Surgery Candidates: A Retrospective Study. Healthcare 2025, 13, 1294. https://doi.org/10.3390/healthcare13111294
Magurano MR, Napolitano D, Bozzetti M, Lo Cascio A, Oppo L, Fernandez Tayupanta LA, Ferrazzoli S, Lopasso L, Rellini E, Raffaelli M, et al. Psychological Assessment and Psychosocial Outcomes in Bariatric Surgery Candidates: A Retrospective Study. Healthcare. 2025; 13(11):1294. https://doi.org/10.3390/healthcare13111294
Chicago/Turabian StyleMagurano, Maria Rosaria, Daniele Napolitano, Mattia Bozzetti, Alessio Lo Cascio, Lorenzo Oppo, Laura Antonella Fernandez Tayupanta, Serena Ferrazzoli, Lucia Lopasso, Emanuela Rellini, Marco Raffaelli, and et al. 2025. "Psychological Assessment and Psychosocial Outcomes in Bariatric Surgery Candidates: A Retrospective Study" Healthcare 13, no. 11: 1294. https://doi.org/10.3390/healthcare13111294
APA StyleMagurano, M. R., Napolitano, D., Bozzetti, M., Lo Cascio, A., Oppo, L., Fernandez Tayupanta, L. A., Ferrazzoli, S., Lopasso, L., Rellini, E., Raffaelli, M., & Chieffo, D. P. R. (2025). Psychological Assessment and Psychosocial Outcomes in Bariatric Surgery Candidates: A Retrospective Study. Healthcare, 13(11), 1294. https://doi.org/10.3390/healthcare13111294