
Suicide and Self-Harming Among Young Women: A Qualitative Exploratory Study in Southern Punjab, Pakistan

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Methodology
2.1. Background and Study Setting
2.2. Participants
2.2.1. Sampling and Inclusion/Exclusion Criteria
2.2.2. Interviews and Data Collection Procedure
2.3. Thematic Analysis Procedure
2.4. Ethical Consideration
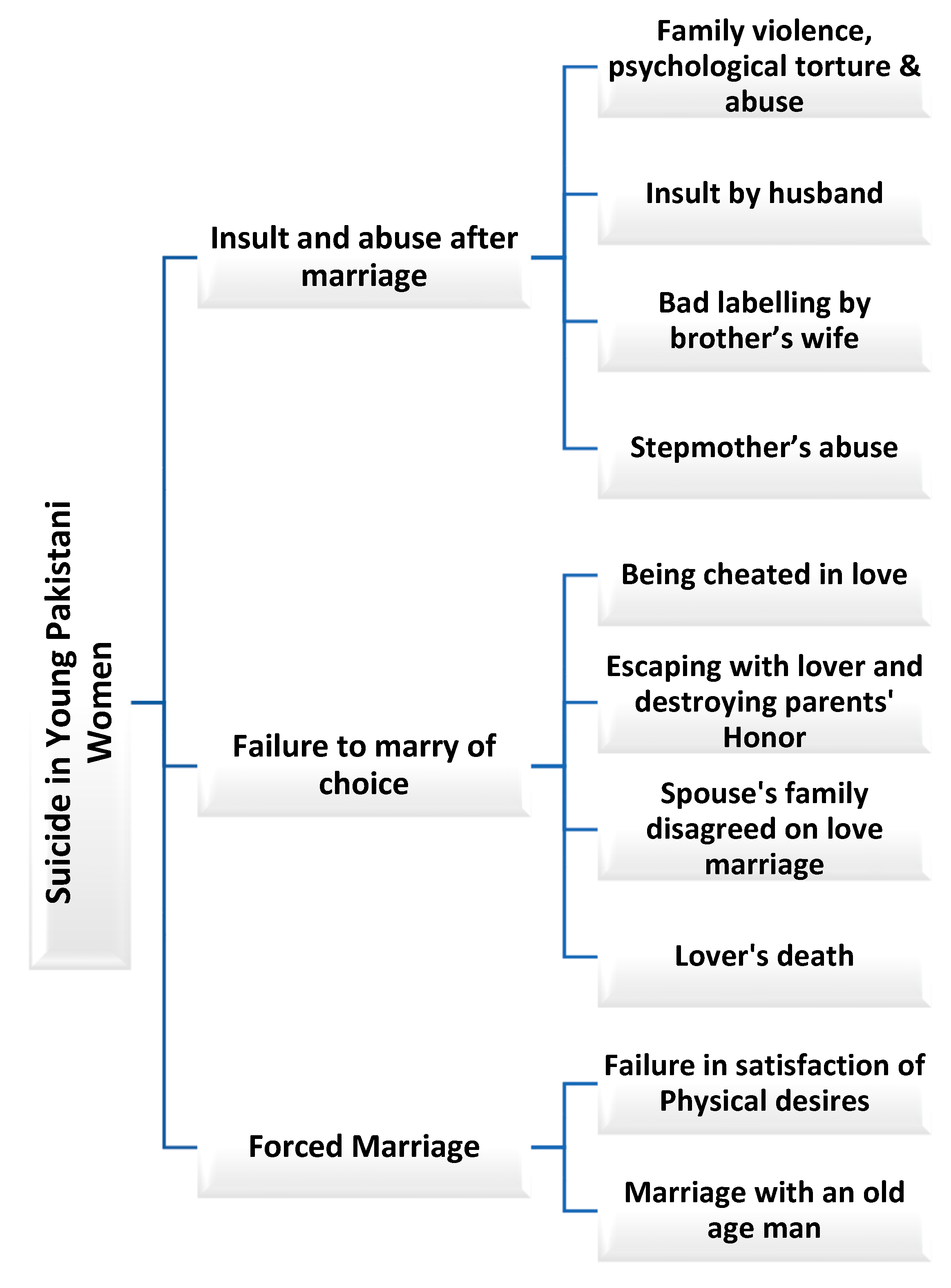
3. Results
3.1. Theme One: Forced Marriages or Marriage Without the Choice of Young Girls
3.1.1. Protest Against the Forced Marriage
“My 70-year-old uncle got married by exchanging her son’s daughter with the groom’s brother. Once I asked, Are you happy with this old uncle? She said, ‘he can’t fulfill my desire. Wealth is not sufficient. Please ask my parents, “I can no longer live with him. Otherwise, I would take my life.” ‘Everyone was aware of her critical situation. One day, in the absence of my uncle, she attempted suicide, but one family member saved her life. She warned, ‘If you don’t divorce me, I will do it again.’ But no one could take it seriously. After some time, she took a black rock and ate it with some juice. This time she succeeded in dying”.
“She did not agree to marry an old man and attempted suicide. When we reached, she had drunk all the nail-polish remover, and her family members were crying. Her stomach was bulging inside her belly, she was not breathing well. She was catching her neck. My husband brought her to the hospital. The doctor told her that her breathing pipe would be disturbed for her whole life”.
3.1.2. Cultural Violence as the Motivating Determinant of Suicide
“The future of women is decided without their consent, by the parents and family elders, and soon after marriages, domestic disputes and unsustainable relationships erupt with husbands, which forces women to commit suicide”.
“My husband disliked that her daughter disobeyed his decision to marry. I failed to convince him, but he deemed his daughter’s confrontation an abuse of the local norms and customs. This controversial marriage made her depressed. My well-educated daughter decided to kill herself soon after she was forced to marry her uneducated cousin. My husband was ready to withdraw from his stance, so our daughter thought it better to lose her life”.
“Kalakali means when a married woman is caught with her boyfriend, the family honor is considered ruined. Women in that case often prefer to die otherwise, they are sold out or murdered. The reasons to commit suicide are many, but the main causes are misbehavior, domestic issues, and violence by husbands and relatives. We did not report the suicide case to the police and kept it secret to evade social stigma”.
3.2. Theme Two: Insulting Behaviors of Relatives and Suicide Among Women
3.2.1. Violence, Stigma, and Depression
“My aunt fell in love; her boyfriend sent his family to propose, but her parents refused, saying that since your elder sisters are still unmarried, how can you marry? After this, her family members used to abuse her verbally and physically. One day, she came in front of the train and was no more”.
“My niece was young, energetic, and talented. Her brother’s wife was strict and cruel; she treated her like a maid. Her mother was a social lady and often used to leave her alone in the house with her brother’s wife. She was asked to wash clothes and utensils and cook food. Even after her work, her brother’s wife was not happy and used to label, stigmatize, and abuse her all the time. One day, she bought a packet of henna with black rock (PPD) and ate it with juice. After some time, her brother’s wife called her to make the loaf, but there was no answer. Her daughter went to check her in the room, but she was vomiting, and later she died”.
“My niece was a young, beautiful, and intelligent girl. But for some time, she was very disturbed and disappointed with her stepmother. She abused her in front of her dad, but her dad never interfered and supported. She came to me and was weeping and said, ‘Aunt (father’s sister), I will not go to my house because my stepmother pains me and labels me.’ The next day, we heard that she had eaten the black rock, which she reportedly brought for dyeing the hair. The main reason was consistent mistreatment of her stepmom with her and often labeling her as a bad character woman”.
3.2.2. Insult in Front of Other Family Members
“It was his habit to insult me before our children. One day, I told him, Now our children are older, please don’t insult me in front of them.” He replied, ‘I don’t care about you and your children, leave me, I will never die without you.’ I was shocked and went to the room, took the pesticide, and drank it. But later, I was saved by the doctors”.
“My husband was bad-tempered and used to insult me in front of my family members. He often put me in a painful situation. Once, I saw a spray bottle of organophosphorus compounds (pesticides) in anger and drank a few sips. But my family members managed to take me to the hospital, and I was saved”.
3.3. Theme Three: Failure in Marriage or Love Due to Unfaithfulness
3.3.1. Failing to Marry Due to Cheating
“My sister loved a boy, but when she insisted on marrying her, he shouted and said No, I have many girlfriends, and I can’t marry all of them. You are not the only one with whom I talk. If you ask me to marry you, I will block your number from my contact list. And he literally did this. My sister was very sensitive; she could not accept this insult and hanged herself. After a few days, the police arrested him, and he agreed that they both quarreled”.
“My classmate from a very ethnically strict family fell in love. People told her not to meet with that guy. He belonged to a very rich family, maybe he will cheat you. She said, ‘Love is blind. I cannot live without him. I know my parents are strict, but this love is not in my control, it’s in my heart.’ Once she escaped with that guy, but unfortunately, the boy left her. After some days, my classmate came to her parents’ house, but they did not want to accept her. They said, ‘You buried our honor, we wish you were buried under this earth.’ She did not accept this treatment from her own parents and committed suicide with the black rock”.
3.3.2. Failure of a Love Marriage
“She was young, beautiful, with long hair, but was looking sad. I tried to investigate what happened. She revealed: ‘I think I will die soon because I often dream, I am dying. One night I dreamed that I died and there was a moringa tree upon my grave.’ I said to her, Don’t feel stressed, just donate some slaughter. It was just a dream. My sister fell in love with my cousin, but the boy’s mom did not agree. One night, my sister used insecticide crushed tablets, which were used for the protection of wheat. In the early morning, she fainted and all family members wanted to save her life, but it was too late”.
“One of my female students fell in love with someone, and the boy was from another caste. She discussed this matter with her brothers, who got angry when she discussed this matter with them. They said, Go and marry, but we will give no piece of land to you. We will not allow them to become rebels like you. After some period, that girl came to me and told me, ‘My love has died due to a medical issue, my brothers also don’t accept me, now I have no reason to live, I want to die. After that, she hanged herself and died”.
4. Discussion
4.1. Socioeconomic and Demographic Factors
4.2. Gendered Vulnerability and Violence
4.3. Marital and Family Dynamics
4.4. Family Honor and Ethnic and Cultural Violence
4.5. Methods and Means of Suicide
4.6. Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Suicide. World Health Organization. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 15 May 2012).
- Shakil, M. A Qualitative Analysis of Suicides Committed by the Students in Pakistan. Pak. J. Med. Res. 2019, 58, 35–40. [Google Scholar]
- World Health Organization. Preventing Suicide: A Global Imperative; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Turecki, G.; Brent, D. Suicide and Suicidal Behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Observatory; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Shah, I.; Khalily, M.T.; Ahmad, I.; Hallahan, B. Impact of Conventional Beliefs and Social Stigma on Attitude Towards Access to Mental Health Services in Pakistan. Community Ment. Health J. 2019, 55, 527–533. [Google Scholar] [CrossRef]
- Tabassum, R. Gender Inequality in Mental Health: A Review from the South Asian Context. Bangladesh J. Med. Sci. 2017, 16, 203–206. [Google Scholar] [CrossRef]
- Kiran, T.; Chaudhry, N.; Bee, P.; Tofique, S.; Farooque, S.; Qureshi, A.; Taylor, A.K.; Husain, N.; Chew-Graham, C.A. Clinicians’ Perspectives on Self-Harm in Pakistan: A Qualitative Study. Front. Psychiatry 2021, 12, 607549. [Google Scholar] [CrossRef]
- Mahmood, S. The Pakistan Penal Code (XLV of 1880); Legal Research Centre: Lahore, Pakistan, 1989; Volume II. [Google Scholar]
- De Leo, D. Can We Rely on Suicide Mortality Data? Crisis 2015, 36, 1–3. [Google Scholar] [CrossRef]
- Dwivedi, Y. (Ed.) The Neurobiological Basis of Suicide; CRC Press: Boca Raton, FL, USA, 2012. [Google Scholar]
- Marecek, J.; Senadheera, C. ‘I Drank It to Put an End to Me’: Narrating Girls’ Suicide and Self-Harm in Sri Lanka. Contrib. Indian Sociol. 2012, 46, 53–82. [Google Scholar] [CrossRef]
- Lester, D. Why Women Kill Themselves; Charles C. Thomas: Springfield, IL, USA, 1988. [Google Scholar]
- Tomlinson, M. Dealing with Suicide; KESS Seminar Series; Stormont Assembly: Belfast, UK, 2013. [Google Scholar]
- Rugkhla, P. Women and Suicide; Gender Impact Assessment; Women’s Health Victoria: Melbourne, Australia, 2011. [Google Scholar]
- Mallon, S.; Galway, K.; Hughes, L.; Rondón-Sulbarán, J.; Leavey, G. An Exploration of Integrated Data on the Social Dynamics of Suicide Among Women. Sociol. Health Illn. 2016, 38, 662–675. [Google Scholar] [CrossRef]
- Ahmed, F.; Malik, N.I.; Bashir, S.; Noureen, N.; Ahmad, J.B.; Tang, K. Political Economy of Maternal Child Malnutrition: Experiences about Water, Food, and Nutrition Policies in Pakistan. Nutrients 2024, 16, 2642. [Google Scholar] [CrossRef]
- Ahmed, F.; Malik, N.I.; Bashir, S.; Noureen, N.; Ullah, S.; Ahmed, J.B.; Mansoor, T. “An obedient wife never says ‘no’ to her virtual god”. High fertility conceptions and barriers to contraceptive use among mothers of Southern Pakistan: A qualitative study. BMC Public Health 2024, 24, 2157. [Google Scholar] [CrossRef]
- Shahid, M.; Ahmed, F.; Ameer, W.; Guo, J.; Raza, S.; Fatima, S.; Qureshi, M.G. Prevalence of child malnutrition and household socioeconomic deprivation: A case study of marginalized district in Punjab, Pakistan. PLoS ONE 2022, 17, e0263470. [Google Scholar] [CrossRef]
- Ahmed, F.; Shahid, M.; Cao, Y.; Qureshi, M.G.; Zia, S.; Fatima, S.; Guo, J. A qualitative exploration in causes of water insecurity experiences, and gender and nutritional consequences in South Punjab, Pakistan. Int. J. Environ. Res. Public Health 2021, 18, 12534. [Google Scholar] [CrossRef]
- Ahmed, F.; Malik, N.I.; Shahzad, M.; Ahmad, M.; Shahid, M.; Feng, X.L.; Guo, J. Determinants of Infant Young Child Feeding Among Mothers of Malnourished Children in South Punjab, Pakistan: A Qualitative Study. Front. Public Health 2022, 10, 834089. [Google Scholar] [CrossRef]
- Ahmed, F.; Malik, N.I.; Zia, S.; Akbar, A.S.; Li, X.; Shahid, M.; Tang, K. Rural mothers’ beliefs and practices about diagnosis, treatment, and management of children health problems: A qualitative study in marginalized Southern Pakistan. Front. Public Health 2023, 10, 1001668. [Google Scholar] [CrossRef]
- Ahmed, F.; Malik, N.I.; Malik, N.; Qureshi, M.G.; Shahzad, M.; Shahid, M.; Zia, S.; Tang, K. Key challenges to optimal therapeutic coverage and maternal utilization of CMAM Program in rural southern Pakistan: A qualitative exploratory study. Nutrients 2022, 14, 2612. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. One Size Fits All? What Counts as Quality Practice in (Reflexive) Thematic Analysis? Qual. Res. Psychol. 2020, 18, 328–352. [Google Scholar] [CrossRef]
- Agnew, R. General Strain Theory: Current Status and Directions for Further Research. In Taking Stock: The Status of Criminological Theory; Cullen, F.T., Wright, J.P., Blevins, K.R., Eds.; Transaction Publishers: New Brunswick, NJ, USA, 2006; pp. 101–123. [Google Scholar]
- Björkenstam, C.; Kosidou, K.; Björkenstam, E. Childhood Adversity and Risk of Suicide: Cohort Study of 548,721 Adolescents and Young Adults in Sweden. BMJ 2017, 357, j1334. [Google Scholar] [CrossRef]
- Skegg, K. Self-Harm. Lancet 2005, 366, 1471–1483. [Google Scholar] [CrossRef]
- Shahid, M.; Khan, M.M.; Saleem Khan, M.; Jamal, Y.; Badshah, A.; Rehmani, R. Deliberate Self-Harm in the Emergency Department: Experience from Karachi, Pakistan. Crisis 2009, 30, 85–89. [Google Scholar] [CrossRef]
- Shekhani, S.S.; Perveen, S.; Hashmi, D.-E.; Akbar, K.; Bachani, S.; Khan, M.M. Suicide and Deliberate Self-Harm in Pakistan: A Scoping Review. BMC Psychiatry 2018, 18, 44. [Google Scholar] [CrossRef]
- Stack, S. Contributing Factors to Suicide: Political, Social, Cultural and Economic. Prev. Med. 2021, 152, 106498. [Google Scholar] [CrossRef]
- Messias, E.; Azasu, E.K.; Nayeem, N.; Lin, P.-I.; Grucza, R. Suicide Deaths by Occupation Skill Level and Educational Attainment in the United States. J. Occup. Health 2025, 67, uiae078. [Google Scholar] [CrossRef] [PubMed]
- Balaji, M.; Mandhare, K.; Nikhare, K.; Shah, A.K.; Kanhere, P.; Panse, S.; Santre, M.; Vijayakumar, L.; Phillips, M.R.; Pathare, S.; et al. Why Young People Attempt Suicide in India: A Qualitative Study of Vulnerability to Action. SSM-Ment. Health 2023, 3, 100216. [Google Scholar] [CrossRef]
- Bilsen, J. Suicide and Youth: Risk Factors. Front. Psychiatry 2018, 9, 540. [Google Scholar] [CrossRef]
- Bagge, C.L.; Lamis, D.A.; Nadorff, M.R.; Osman, A. Relations Between Hopelessness, Depressive Symptoms and Suicidality: Mediation by Reasons for Living. J. Clin. Psychol. 2014, 70, 18–31. [Google Scholar] [CrossRef]
- Ali, T.S.; Krantz, G.; Gul, R.; Asad, N.; Johansson, E.; Mogren, I. Gender Roles and Their Influence on Life Prospects for Women in Urban Karachi, Pakistan: A Qualitative Study. Glob. Health Action 2011, 4, 7448. [Google Scholar] [CrossRef]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.; Selby, E.A.; Joiner, T.E. The Interpersonal Theory of Suicide. Psychol. Rev. 2010, 117, 575–600. [Google Scholar] [CrossRef] [PubMed]
- Kuo, W.H.; Gallo, J.J.; Eaton, W.W. Hopelessness, Depression, Substance Disorder, and Suicidality: A 13-Year Community-Based Study. Soc. Psychiatry Psychiatr. Epidemiol. 2004, 39, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.M.; Alloy, L.B.; Abramson, L.Y. Cognitive Vulnerability to Depression, Rumination, Hopelessness, and Suicidal Ideation: Multiple Pathways to Self-Injurious Thinking. Suicide Life-Threat. Behav. 2006, 36, 443–454. [Google Scholar] [CrossRef]
- Spirito, A.; Esposito-Smythers, C. Attempted and Completed Suicide in Adolescence. Annu. Rev. Clin. Psychol. 2006, 2, 237–266. [Google Scholar] [CrossRef]
- Gilani, A.I.; Gilani, U.I.; Kasi, P.M.; Khan, M.M. Psychiatric Health Laws in Pakistan: From Lunacy to Mental Health. PLoS Med. 2005, 2, e317. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, L.; Hosseini, S.A.; Rassafiani, M.; Najafi, F.; Shakeri, J.; Khankeh, H. Why Self-Immolation? A Qualitative Exploration of the Motives for Attempting Suicide by Self-Immolation. Burns 2014, 40, 319–327. [Google Scholar] [CrossRef]
- Roohafza, H.; Mosharraf, S.; Mousavi, G.; Khani, A.; Andalib, E.; Reihani, M. The Prevalence and Determinants of Suicidal Behaviors in the Central Region of Iran. Int. J. Body Mind Cult. 2014, 1, 142–153. [Google Scholar]
- Pillai, A.; Andrews, T.; Patel, V. Violence, Psychological Distress and the Risk of Suicidal Behavior in Young People in India. Int. J. Epidemiol. 2009, 38, 459–469. [Google Scholar] [CrossRef]
- LeMasters, K.; Bates, L.M.; Chung, E.O.; Gallis, J.A.; Hagaman, A.; Scherer, E.; Sikander, S.; Staley, B.S.; Zalla, L.C.; Zivich, P.N.; et al. Adverse Childhood Experiences and Depression among Women in Rural Pakistan. BMC Public Health 2021, 21, 400. [Google Scholar] [CrossRef]
- Vijaykumar, L. Suicide and Its Prevention: The Urgent Need in India. Indian J. Psychiatry 2007, 49, 81–84. [Google Scholar] [CrossRef]
- Pradhan, A.; Poudel, P.; Thomas, D.; Barnett, S. A Review of the Evidence: Suicide among Women in Nepal; National Health Sector Support Program, Ministry of Health and Population: Kathmandu, Nepal, 2011; Volume 117. [Google Scholar]
- Sajid, I. Suicides Rising Among Women in Northern Pakistan. Anadolu Agency. 2018. Available online: https://www.aa.com.tr/en/asia-pacific/suicides-rising-among-women-in-northern-pakistan/1270469 (accessed on 18 April 2021).
- Ali, T.S.; Mogren, I.; Krantz, G. Intimate Partner Violence and Mental Health Effects: A Population-Based Study Among Married Women in Karachi, Pakistan. Int. J. Behav. Med. 2013, 20, 131–139. [Google Scholar] [CrossRef]
- Campbell, J.C.; Kub, J.; Belknap, R.A.; Templin, T.N. Predictors of Depression in Battered Women. Violence Against Women 1997, 3, 271–293. [Google Scholar] [CrossRef]
- Farooq, U.; Majeed, M.; Bhatti, J.A.; Khan, J.S.; Razzak, J.A.; Khan, M.M. Differences in Reporting of Violence and Deliberate Self-Harm-Related Injuries to Health and Police Authorities, Rawalpindi, Pakistan. PLoS ONE 2010, 5, e9373. [Google Scholar] [CrossRef]
- Pico-Alfonso, M.A.; Garcia-Linares, M.I.; Celda-Navarro, N.; Blasco-Ros, C.; Echeburúa, E.; Martinez, M. The Impact of Physical, Psychological, and Sexual Intimate Male Partner Violence on Women’s Mental Health: Depressive Symptoms, Posttraumatic Stress Disorder, State Anxiety, and Suicide. J. Womens Health 2006, 15, 599–611. [Google Scholar] [CrossRef]
- Khan, M.M. Suicide Prevention and Developing Countries. J. R. Soc. Med. 2005, 98, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Houry, D.; Kemball, R.; Rhodes, K.V.; Kaslow, N.J. Intimate Partner Violence and Mental Health Symptoms in African American Female ED Patients. Am. J. Emerg. Med. 2006, 24, 444–450. [Google Scholar] [CrossRef]
- Hagaman, A.K.; Khadka, S.; Wutich, A.; Lohani, S.; Kohrt, B.A. Suicide in Nepal: Qualitative Findings from a Modified Case-Series Psychological Autopsy Investigation of Suicide Deaths. Cult. Med. Psychiatry 2018, 42, 704–734. [Google Scholar] [CrossRef] [PubMed]
- Geo News. 346 People Committed Suicide in Malakand in Last Eight Months. Geo News. 2018. Available online: https://www.geo.tv/latest/212922 (accessed on 18 April 2021).
- Mathew, A.; Saradamma, R.; Krishnapillai, V.; Muthubeevi, S.B. Exploring the Family Factors Associated with Suicide Attempts among Adolescents and Young Adults: A Qualitative Study. Indian J. Psychol. Med. 2021, 43, 113–118. [Google Scholar] [CrossRef]
- Ikram, N.; Frost, A.; LeMasters, K.; Hagaman, A.; Baranov, V.; Gallis, J.; Sikander, S.; Scherer, E.; Maselko, J. Adverse Childhood Experiences and Implications of Perceived Stress, Anxiety, and Cortisol Among Women in Pakistan. BMJ Open 2021, 12, e052280. [Google Scholar] [CrossRef] [PubMed]
- Kizza, D.; Knizek, B.L.; Kinyanda, E.; Hjelmeland, H. An Escape from Agony: A Qualitative Psychological Autopsy Study of Women’s Suicide in a Post-Conflict Northern Uganda. Int. J. Qual. Stud. Health Well-being 2012, 7, 18463. [Google Scholar] [CrossRef]
- Pascali, M. La Riforma Normativa Sulla Violenza Sulle Donne in Relazione Alla Natura Dei Crimini Perpetrati. Riv. Criminol. Vittimol. Sicurezza 2015, 9, 1–45. [Google Scholar] [CrossRef]
- Ghalambor, A.; Zarei, J.; Pipelzadeh, M.H. Assessment of Personal and Social Characteristics as Risk Factors in Self-Inflicted Burns. Med. Sci. J. 2010, 9, 233–246. [Google Scholar]
- Elmerstig, E.; Wijma, B.; Sandell, K.; Berterö, C. “Sexual Pleasure on Equal Terms”: Young Women’s Ideal Sexual Situations. J. Psychosom. Obstet. Gynecol. 2012, 33, 129–134. [Google Scholar] [CrossRef]
- Law, L.W.S. Child, Early and Forced Marriage: A Multi-Country Study; UN Office of the High Commissioner for Human Rights: Geneva, Switzerland, 2013. [Google Scholar]
- Pridmore, S.; Walter, G. Suicide and Forced Marriage. Malays. J. Med. Sci. 2013, 20, 47–50. [Google Scholar]
- Ahmed, Z.; Nisa, Q.; Yousufzai, A.W.; Khoja, S.; Chaudhry, J. Trends and Patterns of Suicide in People of Chitral, Khyber Pakhtunkhwa, Pakistan. Khyber Med. Univ. J. 2016, 8, 72–77. [Google Scholar]
- Zhang, J.; Wieczorek, W.F.; Conwell, Y.; Tu, X.M. Psychological Strains and Youth Suicide in Rural China. Soc. Sci. Med. 2011, 72, 2003–2010. [Google Scholar] [CrossRef] [PubMed]
- Lasrado, R.A.; Chantler, K.; Jasani, R.; Young, A. Structuring Roles and Gender Identities Within Families Explaining Suicidal Behavior in South India. Crisis 2016, 37, 205–213. [Google Scholar] [CrossRef]
- Hagaman, A.K.; Maharjan, U.; Kohrt, B.A. Suicide Surveillance and Health Systems in Nepal: A Qualitative and Social Network Analysis. Int. J. Ment. Health Syst. 2016, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Hagaman, A.K. Hidden Death and Social Suffering: A Critical Investigation of Suicide, Death Surveillance, and Implications for Addressing a Complex Health Burden in Nepal. Ph.D. Thesis, Arizona State University, Tempe, AZ, USA, 2017. Available online: https://keep.lib.asu.edu/items/155678 (accessed on 25 October 2023).
- Khan, M.M.; Mahmud, S.; Karim, M.S.; Zaman, M.; Prince, M. Case-Control Study of Suicide in Karachi, Pakistan. Br. J. Psychiatry 2008, 193, 402–405. [Google Scholar] [CrossRef]
- Karunarathne, A.; Gunnell, D.; Konradsen, F.; Eddleston, M. How Many Premature Deaths from Pesticide Suicide Have Occurred Since the Agricultural Green Revolution? Clin. Toxicol. 2020, 58, 227–232. [Google Scholar] [CrossRef]
- Lee, Y.Y.; Chisholm, D.; Eddleston, M.; Gunnell, D.; Fleischmann, A.; Konradsen, F.; Bertram, M.Y.; Mihalopoulos, C.; Brown, R.; Santomauro, D.F.; et al. The Cost-Effectiveness of Banning Highly Hazardous Pesticides to Prevent Suicides Due to Pesticide Self-Ingestion across 14 Countries: An Economic Modeling Study. Lancet Glob. Health 2021, 9, e291–e300. [Google Scholar] [CrossRef]

{kind=link}
| Case | Age in Years | Education | Household Income (PKR) | Harm Method | Immediate Cause Behind the Attempt | Underlying Cause |
|---|---|---|---|---|---|---|
| R9 | 18 | Higher Secondary | 20 K | Came under a train | Family violence, psychologically tortured, and abused | Insult |
| A2 | 21 | Middle | 21 K | Black Rock | Mentally tortured and badly labeled by his brother’s wife | Insult |
| H11 | 20 | Illiterate | 10 K | Black Rock | Stepmother’s abuse and insult | Insult |
| R12 | 16 | Illiterate | 12 K | Insecticide | Husband insulted (marital stress), psychologically tortured | Insult |
| T4 | 25 | Illiterate | 15 K | Organophosphorus (pesticides) | Husband insults in front of family members | Insult |
| T10 | 19 | Secondary | 25 K | Hanged | Boyfriend cheats on her | Love Marriage Failure infidelity |
| S13 | 24 | Secondary | 14 K | Black Rock | Escape with boyfriend, destroy parents’ reputation (honor) | Love Marriage Failure |
| N1 | 20 | Secondary | 25 K | Insecticide | Spouse’s family disagreed about love marriage | Love Marriage Failure |
| U7 | 20 | Illiterate | 50 K | Hanged | Violence and boyfriend’s death | Love Marriage Failure |
| K3 | 20 | Primary | 13 K | Black rock | Exchange marriage does not satisfy desire | Forced Marriage |
| E6 | 19 | Middle | 15 K | Nail polish remover | Does not agree to marry an old man | Forced Marriage |
| B6 | 18 | Higher Secondary | 20 K | Firearm | Marriage | Arranged Marriage |
| A7 | 21 | Middle | 21 K | Hanging | Marriage without consent | Forced Marriage |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, F.; Tsang, E.Y.H.; Anjum, R.; Malik, N.I.; Zia, S.; Nawaz, R.; Wilkinson, J.S.; Fang, Y. Suicide and Self-Harming Among Young Women: A Qualitative Exploratory Study in Southern Punjab, Pakistan. Healthcare 2025, 13, 1284. https://doi.org/10.3390/healthcare13111284
Ahmed F, Tsang EYH, Anjum R, Malik NI, Zia S, Nawaz R, Wilkinson JS, Fang Y. Suicide and Self-Harming Among Young Women: A Qualitative Exploratory Study in Southern Punjab, Pakistan. Healthcare. 2025; 13(11):1284. https://doi.org/10.3390/healthcare13111284
Chicago/Turabian StyleAhmed, Farooq, Eileen Yuk Ha Tsang, Razia Anjum, Najma Iqbal Malik, Sidra Zia, Rashed Nawaz, Jeffrey S. Wilkinson, and Yueyao Fang. 2025. "Suicide and Self-Harming Among Young Women: A Qualitative Exploratory Study in Southern Punjab, Pakistan" Healthcare 13, no. 11: 1284. https://doi.org/10.3390/healthcare13111284
APA StyleAhmed, F., Tsang, E. Y. H., Anjum, R., Malik, N. I., Zia, S., Nawaz, R., Wilkinson, J. S., & Fang, Y. (2025). Suicide and Self-Harming Among Young Women: A Qualitative Exploratory Study in Southern Punjab, Pakistan. Healthcare, 13(11), 1284. https://doi.org/10.3390/healthcare13111284