Abstract
Background/Objectives: Smoking during pregnancy endangers maternal and infant health outcomes, posing significant risks such as preterm birth and developmental complications. Applying the Three Delays Framework, this study examines how smoking behaviors impact maternal health in Alabama, focusing on barriers to prenatal care. Methods: This cross-sectional study utilized PRAMS Phase 8 data collected from 2016 to 2021, comprising 533 observations from the Alabama Department of Public Health. Prenatal care barriers were categorized into three domains: seeking, reaching, and receiving care. Analyses included descriptive statistics, hierarchical clustering of barrier items, derivation of an informational barrier latent score using item-response theory (θ_info), and multivariable logistic regression adjusted for age, race/ethnicity, income, and BMI. Results: Multivariable logistic regression analysis revealed that informational barriers (OR = 2.42, p < 0.001) and system-level barriers (OR = 1.77, p = 0.047) were significant predictors of adverse maternal health outcomes. In the baseline model, which included sociodemographic covariates, prenatal smoking was not significantly associated with poor maternal health (OR = 0.83, 95% CI [0.58, 1.17]). After adjusting for informational, structural, and system barriers, the association further attenuated and remained non-significant (adjusted OR = 0.72, 95% CI [0.50, 1.03]). Conclusions: While smoking during pregnancy remains a modifiable health behavior, informational and system barriers emerged as the more immediate determinants of poor maternal outcomes in this cohort. Addressing these barriers through targeted prenatal education initiatives and system-level improvements can enhance care utilization and improve maternal and infant health outcomes, even among pregnant smokers.
1. Introduction
Smoking during pregnancy poses substantial risks to maternal and neonatal health, contributing to adverse outcomes such as stillbirth, preterm birth, birth defects, and low birth weight [1]. Despite efforts to address this issue, maternal mortality and morbidity rates in Alabama continue to exceed national benchmarks, driven in part by high smoking prevalence among reproductive-age women and barriers to accessing prenatal care [2]. According to the Alabama Maternal Mortality Review Committee, pregnancy-related mortality and near-miss events remain alarmingly high despite declines at the national level, highlighting the need for a localized understanding of delayed or suboptimal care [3]. More crucially, regional studies have documented significant barriers impeding timely prenatal care utilization, such as transportation deficits, appointment delays, and stigma-driven informational gaps [2,3,4]. These barriers collectively exacerbate the challenges faced by pregnant women, particularly smokers, in accessing essential healthcare services.
Historically, U.S. policy has alternated between punitive measures, such as criminalizing prenatal substance use, and public health-focused interventions aimed at providing support [5]. In states like Alabama, the chemical endangerment law categorizes prenatal substance use as child endangerment, deterring some women from seeking care due to fear of legal repercussions [6,7]. In addition, the burden of disease and disability associated with smoking during pregnancy is continually changing. Therefore, it is essential to prioritize and update our understanding of the structural and social factors that contribute to this public health challenge to improve outcomes for those affected by this issue. Furthermore, long-term maternal outcomes, such as postpartum morbidity and mental health challenges, remain insufficiently addressed, particularly in settings where substance use stigma is prevalent [8,9].
While significant efforts have been made over the past decades to lessen the risks associated with smoking during pregnancy among women of reproductive age, substantial gaps remain in contextualizing the psychosocial factors that contribute to this problem and how to galvanize community action to address this ongoing health issue [10]. Interestingly, past research has shown that psychosocial and behavioral interventions, like contingency management, motivational support, and cognitive behavioral therapies, are crucial to addressing substance use during pregnancy [11]. Notwithstanding, establishing and implementing innovative, sustained strategies that can help identify at-risk pregnant women early and connect them to treatment remains a significant challenge in resource-constrained settings, underscoring the critical importance of information-seeking during the prenatal period.
Moreover, geographic factors and cultural nuances play a critical role in shaping the burden and disability associated with smoking during pregnancy, varying significantly across diverse care settings. The prevailing perspective suggests that culture significantly shapes behavior and communication, with its intricate nuances influencing beliefs and perceptions regarding substance and alcohol use [12]. This insight underscores the importance of uncovering the multifaceted dynamics and interconnected factors that drive pregnant women affected by substance use to seek, access, and successfully receive care.
Against this backdrop, the Three Delays Model provides a structured framework to categorize and address multifaceted barriers at critical points in the prenatal care continuum [13]. This framework identifies delays in seeking care, reaching healthcare facilities, and receiving adequate care, allowing for a comprehensive understanding of the obstacles that impact maternal and infant health outcomes. Delays in seeking care are often related to various factors, including informational barriers, insufficient awareness about pregnancy signs, and hesitancy in recognizing the importance of prenatal care. Systemic factors, such as transportation difficulties or clinic access issues, contribute to delays in reaching care [2,9], and delays in receiving care reflect structural barriers, such as long wait times and unsupportive clinic environments.
In the context of Alabama, these barriers are amplified by stigma and systemic challenges, making it crucial to employ frameworks like the Three Delays Model to improve maternal health outcomes. This study applies the Three Delays Model to assess whether informational, structural, and system barriers confound and thereby attenuate the crude association between prenatal smoking and maternal health.
Accordingly, the study tests two hypotheses:
- Higher levels of prenatal care barriers, especially informational and system domains, are associated with poorer self-reported maternal health;
- Adjusting for these barrier domains will substantially weaken or eliminate the crude association between prenatal smoking and poor maternal health.
Conceptual Framework and Study Aims
The Three Delays Model lists or delineates three stages at which barriers can impede prenatal care [13]:
- I.
- Delay 1 (Decision to Seek Care): This domain or phase focuses on informational/sociocultural barriers. It touches on issues like a lack of pregnancy awareness, fear of legal repercussions, or stigma that discourages the initial decision to seek care;
- II.
- Delay 2 (Reaching Care): This phase or domain focuses on structural barriers, including transportation problems, work/school conflicts, childcare responsibilities, or out-of-pocket costs that obstruct travel to a facility;
- III.
- Delay 3 (Receiving Care): This phase or domain highlights system barriers, including appointment availability, insurance restrictions, or provider delays that hinder the timely receipt of services once a facility is reached.
In this study, prenatal smoking serves as the exposure, while self-reported maternal health is the outcome. The three delay-domain barriers are evaluated as potential confounders that may attenuate the crude smoking health association. Because some barriers, such as stigma-related informational deficits, can both influence smoking behavior and directly impact health, treating them as confounders aligns with current causal-inference guidance [14,15]. Accordingly, the study addresses two aims:
- Estimate the independent associations between each delay-domain barrier and maternal health status;
- Determine whether adjusting for informational, structural, and system barriers reduces or eliminates the crude association between prenatal smoking and poor maternal health, after controlling for age, race/ethnicity, income, and BMI.
2. Materials and Methods
This cross-sectional study utilized secondary de-identified data from the Pregnancy Risk Assessment Monitoring System (PRAMS) Phase 8 survey (2016–2021; N = 533) provided by the Alabama Department of Public Health. PRAMS is administered to women who have recently delivered a live infant and captures maternal behaviors and attitudes during pregnancy and the early postpartum period, typically 2–4 months after birth. The population of interest comprised women who experienced live births in Alabama from 2016 to 2021. The initial PRAMS Phase 8 data set used for analysis comprised 596 observations, deliberately selected based on key variables essential to addressing the research question, study aims, and the relevance of the Three Delays Model or framework. A total of 63 records missing any key variables were excluded, with listwise deletion applied across all analyses.
2.1. Measures
The study variables were conceptualized using the Three Delays Model. The outcome, maternal health status, was derived from PRAMS Qn22 items and dichotomized as good vs. poor based on self-report. Although PRAMS captures multiple substances, cigarette items showed the highest response reliability; prenatal smoking was measured with Qn42_CigaretteCategory (“In the last 3 months of your pregnancy, how many cigarettes on an average day?”) and recoded 0 = non-smoker, 1 = any smoking.
Delay-domain confounders
- Delay 1—Informational barriers: latent trait θ_info from IRT modelling of Qn21i (I didn’t know I was pregnant), Qn21j (I didn’t want anyone else to know), and Qn21k (I didn’t want prenatal care), capturing stigma-related knowledge deficits;
- Delay 2—Structural barriers: sum of Qn21b (financial constraints) + Qn21f (work/school conflicts) + Qn21h (no childcare);
- Delay 3—System barriers: sum of Qn21a (appointment availability) + Qn21d (insurance/plan delays).
The covariates were age group (15–19, 20–24, 25–29, 30–34, 35–39, and ≥40 y), race/ethnicity (Non-Hispanic White, Non-Hispanic Black, and Hispanic), household income (Qn79 categories), and BMI category (underweight, healthy, and overweight, obese). Table 1 provides operational definitions, coding schemes, and the Qn21 mapping to delay domains; Appendix A (Table A2) lists full PRAMS wording for each barrier item.

Table 1.
Operational definitions and measurement of study variables.
Factors that influence substance use and smoking during pregnancy among women of reproductive age are multifaceted [16,17,18]. Addressing this intractable public health crisis requires the application of an appropriate theoretical framework coupled with a steadfast commitment to sustainable resource allocation. This study employs the Three Delays Framework to provide critical insights into the multifaceted challenges women experience when seeking prenatal care services during pregnancy [13]. By capturing the interplay of individual, community, and health system factors, this framework offers a structured approach to identifying modifiable barriers and their linkages, offering opportunities for effective policy realignment and addressing implementation gaps.
2.2. Statistical Analysis
Descriptive statistics were generated to summarize sample characteristics and variable distributions. Multidimensional scaling (MDS) and hierarchical clustering techniques were used to assess the grouping of prenatal care barrier items. Internal consistency was evaluated using Cronbach’s alpha (α) and McDonald’s omega (ω). Despite the low reliability estimates (ω = 0.11, 0.07, 0.14), the composites were retained because the items represent theoretically coherent domains within the Three Delays framework, and the study is intentionally exploratory. Item response theory (IRT) modeling was then applied to derive the latent informational barrier trait (θ_info), accounting for item difficulty and discrimination.
Age categories were collapsed into three groups (15–24, 25–34, and ≥35 years), while household income was categorized as ≤USD 20k, USD 20–40k, and >USD 40k to ensure adequate cell sizes. Multivariable logistic regression was the sole inferential technique employed. The baseline model included smoking status and sociodemographic covariates (age band, race/ethnicity, income band, and BMI). A second model incorporated informational, structural, and system barriers as confounders. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported, and model fit was assessed using the Hosmer–Lemeshow test and variance-inflation diagnostics, with no multicollinearity detected.
The adjusted model was specified as follows:
logit[P(Y = poor)] = β0 + β1(smoker_status) + β2(structural_barriers) + β3(system_barriers) + β4(θ_info) + β5(AgeBand3) + β6(Race/Ethnicity) + β7(IncBand3) + β8(BMI_Category)
All analyses were conducted in R 4.4.2 using the following packages: dplyr, tidyr, psych, and broom.
3. Results
The initial PRAMS Phase 8 data set comprised 596 observations. After excluding 63 records with missing key variables (listwise deletion), 533 remained for analysis.
3.1. Sample Characteristics
Table 2 displays frequencies and percentages for all key study variables (maternal health status, smoking status, income, BMI, age group, and race/ethnicity), except for the Qn21 barrier item frequencies, which are moved to Table A1 for ease of reading. For example, 53.8% of respondents were classified as having good maternal health, while 46.2% had poor maternal health. In addition, 60.2% were categorized as non-smokers, and 39.8% were smokers.
Table 2.
Sociodemographic and health characteristics of participants (Complete-Case Analytic Sample, N = 533).
3.2. IRT-Derived Informational Barriers
Figure 1 shows the two-dimensional MDS plot, where items cluster in patterns suggestive of distinct barrier domains. Items associated with financial or scheduling constraints, like I didn’t have enough money or insurance to pay for my visit (Qn21b) and I couldn’t get an appointment (Qn21a), appeared in one region, and items reflecting knowledge or secrecy barriers, like I didn’t know that I was pregnant (Qn21i), and I didn’t want anyone else to know I was pregnant (Qn21j), appeared in another. These patterns provide initial evidence that these items may capture multiple underlying dimensions of prenatal care barriers, aligning partially with the Three Delays Model. For a full list of the Qn21 items and their corresponding barrier domains, please refer to Table A2 (Appendix A).
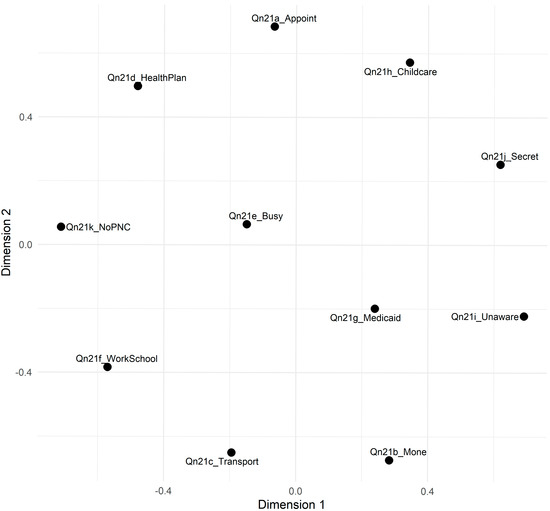
Figure 1.
Multidimensional scaling of Qn21 items. Note: Distances represent the dissimilarity among items (-1|correlation|). Items closer together in the two-dimensional space share stronger correlations, suggesting they may reflect similar underlying barriers to prenatal care.
To assess the relationship between different types of delays (seeking, reaching, and receiving care) and maternal health status, bivariate analyses were conducted using chi-square tests. The results indicated that the Delay Seeking factor was significantly associated with maternal health status (χ2(3) = 23.11, p < 0.001). In contrast, the Delay Reaching (χ2(1) = 2.59, p = 0.462) and Delay Receiving (χ2(1) = 4.42, p = 0.229) factors showed no significant associations. These findings suggest that, at the bivariate level, variations in Delay Seeking are the only factor significantly linked to differences in maternal health outcomes.
Expanding on these bivariate findings, it is noteworthy that although the Delay in Seeking barrier showed a significant bivariate association with maternal outcomes (χ2(3) = 23.11, p < 0.001), this effect was not retained in the multivariable models, suggesting that its impact is confounded or mediated by other barriers.
3.3. Multivariable Logistic Regression
Baseline results, which included smoking status and sociodemographic covariates, showed no significant association between prenatal smoking and poor maternal health (OR = 0.83, 95% CI [0.58, 1.17]). After adjusting for informational, structural, and system barriers as confounders, the association further attenuated and remained non-significant (adjusted OR = 0.72, 95% CI [0.50, 1.03]). Informational barriers (OR = 2.42, p < 0.001) and system-level barriers (OR = 1.77, p = 0.047) were the only factors that significantly increased the odds of poor maternal health, whereas structural barriers were not statistically significant. Model calibration was adequate (Hosmer–Lemeshow p = 0.61), and variance-inflation factors were ≤1.7, indicating no multicollinearity. Table 3 provides the full model estimates, while the baseline versus adjusted smoking odds ratio is listed in Appendix B, Table A3.
Table 3.
Multivariable logistic regression results predicting maternal health status.
As shown in Table 3, after controlling for sociodemographic factors and the three delay domains, informational and system barriers, rather than smoking status, emerge as the strongest determinants of poor maternal health.
3.4. Hierarchical Clustering Analysis
A hierarchical clustering analysis was performed to identify distinct groups of prenatal care barriers. This method shows how specific barriers cluster together, offering insights into their relationships and guiding targeted perinatal interventions. Figure 2 depicts the hierarchical clustering dendrogram for the Qn21 items, which were hypothesized as representing different domains of prenatal care barriers. Several notable clusters emerged.
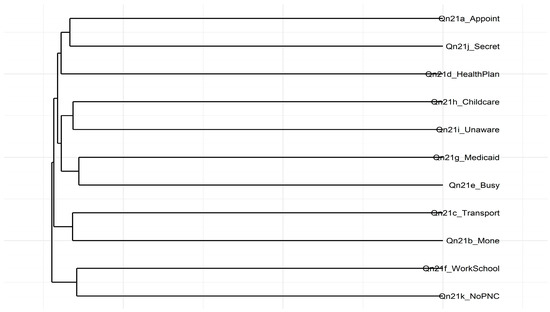
Figure 2.
Hierarchical clustering dendrogram of Qn21 items. Note: The dendrogram was created using an average linkage method and a dissimilarity matrix derived from 1 − ∣r∣. Items that fuse at lower heights share stronger correlations, showing they measure similar or overlapping barriers to prenatal care.
For instance, I didn’t have enough money or insurance to pay for my visit (Qn21b), and I couldn’t take time off from work or school (Qn21f) are grouped, showing a potential overlap in financial and work-related constraints. Similarly, I didn’t have my Medicaid card (Qn21g), I had too many other things going on (Qn21e), and I didn’t know that I was pregnant (Qn21i) formed another cluster, revealing a set of logistical or knowledge-related barriers. Conversely, I didn’t want anyone else to know I was pregnant (Qn21j), and I didn’t want prenatal care (Qn21k) appeared as a distinct pair, potentially capturing personal or privacy concerns associated with pregnant women not seeking prenatal care.
These groupings largely align with the patterns observed in the Multidimensional Scaling (MDS) analysis shown in Figure 1. However, the dendrogram does not wholly separate the items into three discrete clusters corresponding to the Three Delays Model. Instead, the results suggest that some barriers, like money and work constraints, may cut across multiple theoretical domains. Composite scores for each cluster were created to understand their relationship to maternal health outcomes. Further steps involve refining these item groupings and examining how they relate to maternal health outcomes.
3.5. Item Characteristics Curves
Figure 3 illustrates the item characteristic curves (ICCs) for the informational barriers’ items, underscoring their discriminative properties under a two-parameter logistic (2PL) IRT model. For instance, I didn’t know that I was pregnant (Qn21i) portrays a relatively flat slope, indicating low discrimination. In contrast, I didn’t want anyone else to know I was pregnant (Qn21j) shows a sharply declining curve, consistent with its strong discrimination and high negative loading, and I didn’t want prenatal care (Qn21k) demonstrates a steep slope, reflecting moderate-to-high discrimination.
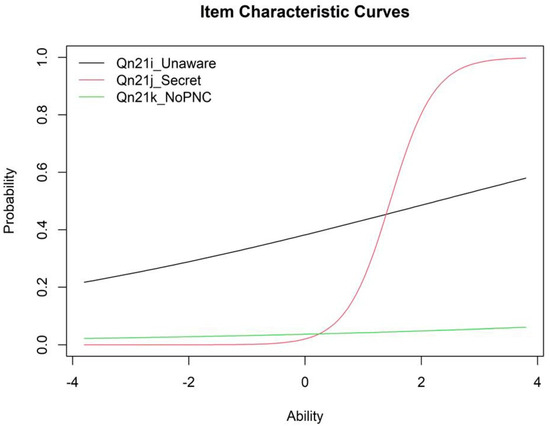
Figure 3.
Item characteristic curves for informational barriers.
These patterns show that I didn’t want anyone else to know I was pregnant (Qn21j) and I didn’t want prenatal care (Qn21k) are particularly effective in differentiating respondents along the latent trait of informational barriers, while I didn’t know that I was pregnant (Qn21i) contributes less to differentiation. Despite the limited discrimination of I didn’t know that I was pregnant (Qn21i), the items collectively capture a meaningful latent construct of informational barriers to prenatal care.
The ICCs visually highlight how each item differentiates across levels of the latent trait, further emphasizing the critical role of informational barriers in understanding maternal health outcomes. Although I didn’t know that I was pregnant (Qn21i) demonstrated low discrimination, it was retained to preserve theoretical completeness. Future studies may consider excluding this item.
4. Discussion
This cross-sectional study is the first to extend the Three Delays Model to prenatal smoking, identifying system and informational barriers, rather than structural constraints or smoking itself, as the primary factors associated with poor maternal health. Fear of mandatory reporting and its related stigma likely exacerbate Delay 1, discouraging pregnant smokers from seeking timely care [6,7,19]. Although the Three Delays Model is widely applied in maternal health research [13,20,21], its use in examining smoking during pregnancy remains limited. The study findings indicate that informational and system barriers independently predict adverse maternal outcomes and substantially attenuate the crude smoking health association, emphasizing the need for tailored educational campaigns that enhance awareness and navigation of prenatal services among high-risk populations.
To align with the Three Delays framework, prenatal care barriers were categorized into structural, informational, and system domains. Consistent with previous PRAMS analyses in Alabama [2], Georgia [3], and Mississippi [4], as well as national maternal health reports [22,23,24,25,26,27,28], informational and system barriers remained significant even after adjusting for age, race/ethnicity, income, and BMI. These barriers align with broader frameworks addressing substance use during pregnancy, such as contextual models of opioid crises [22]. Additionally, polysubstance use, combining smoking with alcohol or opioids, worsens prenatal health disparities [23], reinforcing the importance of maternal healthcare strategies designed to address worsening outcomes [24,25]. Global maternal health guidelines stress the need for equitable access to care, highlighting targeted prenatal outreach for high-risk populations [26].
Since the barrier domains act as confounders rather than mediators in the adjusted multivariable logistic regression model, the exploratory mediation and SEM outputs remain available in Appendix B (Table A3 and Table A4) for readers interested in alternative causal specifications. However, these supplementary analyses do not alter the primary conclusion that informational and system barriers are the predominant contributors to poor maternal health in this cohort. Structural equation modeling (SEM) was employed to assess mediation pathways, following methodological best practices for response shift detection and item response theory applications [27,28]. Findings from Tennessee PRAMS further reinforce these patterns, highlighting persistent disparities in maternal health access [29]. These results suggest that interventions addressing informational deficits, such as culturally tailored prenatal education modules, and system frictions, including appointment availability and insurance navigation, may yield greater improvements in maternal health than smoking-cessation messaging alone.
4.1. Implications for Theory and Practice
The study findings highlight the value of the Three Delays Model for analyzing barriers to prenatal care and their influence on maternal outcomes. System and informational barriers emerged as the most vital obstacles for pregnant smokers: inadequate appointment availability, insurance hurdles, and limited knowledge about prenatal services compound the challenges of navigating care.
Low maternal health literacy has long been linked to sub-optimal maternal and child health outcomes, including reduced access to essential services [30]. Likewise, language barriers and health communication anxiety among linguistic minorities can exacerbate disparities [31], while cultural norms and health-seeking behaviors shape service use in rural or diverse communities [32].
Importantly, disparities in postpartum care reinforce the need for equitable approaches. Interrante et al. [33] showed that race, geography, and insurance type affect receipt of recommended postpartum visits, underscoring the interconnected social and structural determinants of health. Shang et al. [9] demonstrated that early, targeted postpartum interventions reduce depression and anxiety among women with pregnancy complications, and Pacho et al. [34] found that substance use during pregnancy increases the risk of postpartum depression. Culturally tailored health education materials have been shown to improve patient engagement and health outcomes, especially among underserved populations [35].
Practical recommendations include establishing integrated antenatal substance counselling clinics and adopting a “no wrong door” referral system so that patients receive needed services regardless of entry point. Routine postpartum follow-ups are also essential to maintain continuity of care. In Alabama, interventions should prioritize easy-to-understand, culturally tailored prenatal care information and community support referrals, complemented by case management services to sustain health gains. Addressing systemic issues, such as appointment scheduling, transportation, and insurance barriers, should be a policy priority. Investments in telehealth and mobile clinics could further reduce geographic inequities.
Because informational and system barriers confound the smoking health association, tackling these domains may yield substantial improvements in maternal health beyond smoking cessation messaging alone.
4.2. Study Limitations
This study has several limitations that merit consideration. First, it focuses exclusively on smoking as a substance use behavior. This tobacco-only focus may overlook broader substance use patterns, such as alcohol or opioid use, that also influence maternal health outcomes. Future PRAMS modules should expand their scope to capture the full spectrum of substance use during pregnancy.
Second, the study findings are specific to Alabama and may not generalize to other states or regions. PRAMS incorporates state-specific core questions and sampling methods, which may limit cross-state comparability. Notwithstanding, this geographic specificity is also a strength, as it provides actionable insights for policymakers and practitioners in Alabama’s unique demographic and healthcare context.
Third, several additional sociodemographic and reproductive variables like maternal education level, marital status, parity (number of children), and pregnancy intendedness, align with the Three Delays framework as potential influences on the decision to seek care (Delay 1) or the ability to reach care (Delay 2). For instance, maternal education shapes health literacy and recognition of prenatal needs, and marital status and household structure provide social support for transportation and childcare. Parity affects caregiving responsibilities, and pregnancy intendedness reflects motivation to engage in care.
However, a substantial portion of the complete-case sample had missing information on one or more of these variables, and including them in multivariable models would have markedly reduced the analytic sample and risked biased estimates. Although conceptually relevant, these factors were excluded to preserve analytic validity. Future research with more complete data should examine their specific roles within the prenatal care continuum.
Fourth, the cross-sectional design precludes causal inferences, and associations observed cannot establish temporal ordering or definitively confirm mediation versus confounding. Fifth, some composite measures exhibited low internal consistency, requiring advanced techniques such as item response theory (IRT) to derive latent traits. While IRT addresses reliability concerns, it may obscure item-level nuances. Qualitative studies or longitudinal designs could complement these findings by providing richer, context-specific insights into prenatal care barriers and their impact on maternal health.
5. Conclusions
In this cross-sectional analysis of PRAMS Phase 8 data from Alabama, the Three Delays Model was applied to examine how barriers to prenatal care influence maternal health among pregnant smokers. After adjusting for age, race/ethnicity, income, and BMI, smoking status was not significantly associated with poor maternal health (adjusted OR = 0.72, 95% CI [0.50, 1.03]). Instead, informational barriers (OR = 2.42, p < 0.001) and system-level barriers (OR = 1.77, p = 0.047) emerged as the strongest predictors.
These findings underscore that, although smoking remains a vital public health target, the most immediate opportunities for improving maternal health lie in addressing modifiable obstacles to care, such as increasing awareness of prenatal services and streamlining appointment and insurance processes. Mediation and SEM results have been moved to Appendix B to ensure transparency while maintaining focus on the primary message that enhancing prenatal care utilization through targeted education campaigns and system-level reforms may yield greater improvements in maternal health than focusing exclusively on smoking cessation.
Future research should employ longitudinal designs, incorporate a broader set of sociodemographic and psychosocial covariates, and evaluate barrier-reduction strategies across diverse settings to confirm and extend these findings.
Funding
This study did not receive funding from government, commercial, or non-profit organizations.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. It utilized de-identified, anonymized data, and new approval was unnecessary or not applicable. The PRAMS Phase 8 dataset was approved previously for use by Auburn University IRB under protocol number 24-831, with an approval date of 11 July 2024.
Informed Consent Statement
Informed consent was not required for this research study.
Data Availability Statement
Due to the existing data use agreement with the state of Alabama, the entire dataset cannot be shared. However, data supporting the study findings can be made available upon reasonable request.
Acknowledgments
Special thanks to the Alabama PRAMS Work Group and the Centers for Disease Control and Prevention for providing quantitative data for this study.
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
| ACME | Average Causal Mediation Effect |
| ADE | Average Direct Effect |
| ADPH | Alabama Department of Public Health |
| BMI | Body Mass Index |
| CFI | Comparative Fit Index |
| CI | Confidence Interval |
| IRB | Institutional Review Board |
| IRT | Item Response Theory |
| MDS | Multidimensional Scaling |
| PNC | Prenatal Care |
| PRAMS | Pregnancy Risk Assessment Monitoring System |
| Qn21a | Alabama PRAMS Phase 8 Questionnaire #21a |
| Qn21b | Alabama PRAMS Phase 8 Questionnaire #21b |
| Qn21c | Alabama PRAMS Phase 8 Questionnaire #21c |
| Qn21d | Alabama PRAMS Phase 8 Questionnaire #21d |
| Qn21e | Alabama PRAMS Phase 8 Questionnaire #21e |
| Qn21f | Alabama PRAMS Phase 8 Questionnaire #21f |
| Qn21g | Alabama PRAMS Phase 8 Questionnaire #21g |
| Qn21h | Alabama PRAMS Phase 8 Questionnaire #21h |
| Qn21i | Alabama PRAMS Phase 8 Questionnaire #21i |
| Qn21j | Alabama PRAMS Phase 8 Questionnaire #21j |
| Qn21k | Alabama PRAMS Phase 8 Questionnaire #21k |
| RMSEA | Root Mean Square Error of Approximation |
| SE | Standard Error |
| SEM | Structural Equation Model |
| TLI | Tucker—Lewis Index |
Appendix A
Table A1.
Qn21 Prenatal-care barrier items (frequencies and percentages).
Table A1.
Qn21 Prenatal-care barrier items (frequencies and percentages).
| PRAMS Item (Qn21) | No | Yes | % Yes |
|---|---|---|---|
| Couldn’t get an appointment (a) | 304 | 229 | 43.0 |
| Didn’t have enough money/insurance (b) | 356 | 177 | 33.2 |
| No transportation (c) | 468 | 65 | 12.2 |
| Insurance/plan would not start care early (d) | 403 | 130 | 24.4 |
| Too many other things going on (e) | 441 | 92 | 17.3 |
| Couldn’t take time off work/school (f) | 482 | 51 | 9.6 |
| No Medicaid card (g) | 387 | 146 | 27.4 |
| No childcare (h) | 500 | 33 | 6.2 |
| Didn’t know I was pregnant (i) | 371 | 162 | 30.4 |
| Didn’t want anyone to know I was pregnant (j) | 480 | 53 | 9.9 |
| Didn’t want prenatal care (k) | 512 | 21 | 3.9 |
Note: Percentages reflect the same N = 533 analytic sample.
Table A2.
Fully labeled Qn21 items in Table 1.
Table A2.
Fully labeled Qn21 items in Table 1.
| Barrier Domain | PRAMS Item Code | Question Text |
|---|---|---|
| Delay 1: Informational | Qn21i_Unaware | I didn’t know that I was pregnant |
| Qn21j_Secret | I didn’t want anyone else to know I was pregnant | |
| Qn21k_NoPNC | I didn’t want prenatal care | |
| Delay 2: Structural | Qn21b_Mone | I didn’t have enough money or insurance to pay for my visit |
| Qn21c_Transport | I didn’t have any transportation to get to the clinic or doctor’s office | |
| Qn21e_Busy | I had too many other things going on | |
| Qn21f_WorkSchool | I couldn’t take time off from work or school | |
| Qn21h_Childcare | I didn’t have anyone to take care of my children | |
| Delay 3: System | Qn21a_Appoint | I couldn’t get an appointment when I wanted one |
| Qn21d_HealthPlan | The doctor or my health insurance plan would not start care as early as I wanted | |
| Qn21g_Medicaid | I didn’t have my Medicaid card |
Note: Qn21 items were derived from the PRAMS Phase 8 dataset provided by the Alabama Department of Public Health. These items represent barriers to prenatal care categorized into structural, informational, and system domains based on the Three Delays Framework. Items were labeled for interpretability and linked directly to the survey questions.
Appendix B
Table A3.
Baseline versus adjusted odds ratio for prenatal smoking.
Table A3.
Baseline versus adjusted odds ratio for prenatal smoking.
| Model | OR | 95% CI | p |
|---|---|---|---|
| Baseline + | 0.83 | [0.58, 1.17] | 0.28 |
| Adjusted ‡ | 0.72 | [0.50, 1.03] | 0.07 |
Note: Baseline model (marked with +) includes smoking status plus age band, race/ethnicity, income band, and BMI. Adjusted model (marked with ‡) additionally includes informational, structural, and system barrier scores. OR = odds ratio; CI = confidence interval.
Table A4.
Exploratory mediation analysis (indirect effect of smoking via informational barriers).
Table A4.
Exploratory mediation analysis (indirect effect of smoking via informational barriers).
| Effect | Estimate | 95% CI | p-Value |
|---|---|---|---|
| ACME (Average) | 0.03 | [0.01, 0.05] | 0.006 *** |
| ADE (Average) | −0.08 | [−0.16, 0.00] | 0.056 |
| Total Effect | −0.05 | [−0.13, 0.04] | 0.232 |
| Prop. Mediated (Average) | −0.44 | [−4.62, 4.34] | 0.238 |
Note. ACME = Average Causal Mediation Effect; ADE = Average Direct Effect. Asterisks indicate significance levels: *** p < 0.001.
Table A5.
Exploratory structural-equation model.
Table A5.
Exploratory structural-equation model.
| Parameter | Estimate | Std. Error | z-Value | p-Value | 95% CI |
|---|---|---|---|---|---|
| Mediator Equation | |||||
| Smoker_status (a) | 0.143 | 0.058 | 2.453 | 0.014 | [0.029, 0.257] |
| Outcome Equation | |||||
| Theta_info (d) | 0.530 | 0.079 | 6.683 | <0.001 | [0.375, 0.685] |
| Smoker_status (c′) | –0.199 | 0.111 | –1.797 | 0.072 | [–0.417, 0.019] |
| Defined Effects | |||||
| Indirect Effect (a*d) | 0.076 | 0.032 | 2.363 | 0.018 | [0.013, 0.139] |
| Total Effect | –0.123 | 0.112 | –1.106 | 0.269 | [–0.343, 0.097] |
Note. Confidence intervals are computed as Estimate ± 1.96 × Std. Error. ACME = Average Causal Mediation Effect (indirect effect); ADE = Average Direct Effect. Smoker_status (a) represents the effect of smoking status on the mediator (informational barriers). Theta_info (d) represents the effect of informational barriers on maternal health. Indirect Effect (a*d) represents the mediated effect of smoking status on maternal health through informational barriers. Smoker_status (c′) represents the direct effect of smoking status on maternal health, controlling for informational barriers as mediating factors. The SEM demonstrated an excellent fit (CFI 0.972, TLI 0.965, RMSEA 0.038 [90% CI 0.032–0.044]).
References
- National Institute on Drug Abuse. Substance Use While Pregnant and Breastfeeding. National Institute on Drug Abuse: 2020. Available online: https://nida.nih.gov/publications/research-reports/substance-use-in-women/substance-use-while-pregnant-breastfeeding (accessed on 15 May 2025).
- Alabama Department of Public Health. Pregnancy Risk Assessment Monitoring System (PRAMS) Report; Alabama Department of Public Health: Montgomery, AL, USA, 2025. Available online: https://www.alabamapublichealth.gov/prams/ (accessed on 15 May 2025).
- Georgia Department of Public Health. Georgia Pregnancy Risk Assessment Monitoring System (PRAMS); Georgia Department of Public Health: Atlanta, GA, USA, 2025. Available online: https://dph.georgia.gov/PRAMS (accessed on 15 May 2025).
- Mississippi State Department of Health. Mississippi PRAMS Surveillance Report 2020; Mississippi State Department of Health: Jackson, MS, USA, 2020. Available online: https://msdh.ms.gov/page/resources/20345.pdf (accessed on 15 May 2025).
- Goodman, D.; Whalen, B.; Hodder, L.C. It’s Time to Support, Rather Than Punish, Pregnant Women with Substance Use Disorder. JAMA Netw. Open 2019, 2, e1914135. [Google Scholar] [CrossRef] [PubMed]
- Alabama Code § 26-15-3.2. Chemical Endangerment of Exposing a Child to an Environment in Which Controlled Substances Are Produced or Distributed. Code of Alabama. 2020. Available online: https://law.justia.com/codes/alabama/2020/title-26/chapter-15/section-26-15-3-2/ (accessed on 15 May 2025).
- Shah, S.K.; Perez-Cardona, L.; Helner, K.; Massey, S.H.; Premkumar, A.; Edwards, R.; Norton, E.S.; Rogers, C.E.; Miller, E.S.; Smyser, C.D.; et al. How penalizing substance use in pregnancy affects treatment and research: A qualitative examination of researchers’ perspectives. J. Law Biosci. 2023, 10, lsad019. [Google Scholar] [CrossRef] [PubMed]
- Sultan, P.; Ando, K.; Elkhateb, R.; George, R.B.; Lim, G.; Carvalho, B.; Chitneni, A.; Kawai, R.; Tulipan, T.; Blake, L.; et al. Assessment of Patient-Reported Outcome Measures for Maternal Postpartum Depression Using the Consensus-Based Standards for the Selection of Health Measurement Instruments Guideline. JAMA Netw. Open 2022, 5, e2214885. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.; Dolikun, N.; Tao, X.; Zhang, P.; Woodward, M.; Hackett, M.L.; Henry, A. The effectiveness of postpartum interventions aimed at improving women’s mental health after medical complications of pregnancy: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2022, 22, 809. [Google Scholar] [CrossRef] [PubMed]
- Substance Use During Pregnancy. Maternal Infant Health. 2024. Available online: https://www.cdc.gov/maternal-infant-health/pregnancy-substance-abuse/index.html (accessed on 15 May 2025).
- Brandon, A.R. Psychosocial Interventions for Substance Use During Pregnancy. J. Perinat. Neonatal Nurs. 2014, 28, 169–177. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Des Marais, S. Cultural Differences in Substance Use. Psych Central. 2022. Available online: https://psychcentral.com/addictions/cultural-context-and-influences-on-substance-abuse (accessed on 15 May 2025).
- Thaddeus, S.; Maine, D. Too far to walk: Maternal mortality in context. Soc. Sci. Med. 1994, 38, 1091–1110. [Google Scholar] [CrossRef] [PubMed]
- Hernán, M.A.; Robins, J.M. Causal Inference: What If; Chapman & Hall/CRC: Boca Raton, FL, USA, 2020. [Google Scholar]
- VanderWeele, T.J. Explanation in Causal Inference: Methods for Mediation and Interaction; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Wilson, C.A.; Finch, E.; Kerr, C.; Shakespeare, J. Alcohol, smoking, and other substance use in the perinatal period. BMJ 2020, 369, m1627. [Google Scholar] [CrossRef]
- Pomar, E.G.; Berryhill, J.; Bhattacharyya, S. Evaluating maternal drug use disparities, risk factors and outcomes in Northeast Arkansas: A pre, during, and post-COVID-19 pandemic analysis. BMC Public Health 2025, 25, 509. [Google Scholar] [CrossRef] [PubMed]
- Pielage, M.; El Marroun, H.; Odendaal, H.J.; Willemsen, S.P.; Hillegers, M.H.; Steegers, E.A.; Rousian, M. Alcohol exposure before and during pregnancy is associated with reduced fetal growth: The Safe Passage Study. BMC Med. 2023, 21, 318. [Google Scholar] [CrossRef]
- Yu, C. Policies Affecting Pregnant Women with Substance Use Disorder. Voices Bioeth. 2023, 9. [Google Scholar] [CrossRef]
- Keating, E.M.; Sakita, F.; Mmbaga, B.T.; Amiri, I.; Nkini, G.; Rent, S.; Fino, N.; Young, B.; Staton, C.A.; Watt, M.H. Three delays model applied to pediatric injury care seeking in Northern Tanzania: A mixed methods study. PLOS Glob. Public Health 2022, 2, e0000657. [Google Scholar] [CrossRef] [PubMed]
- Save the Children. Applying the Three Delays Model: Improving Access to Care for Newborns with Danger Signs. 2013. Available online: https://www.healthynewbornnetwork.org/hnn-content/uploads/Applying-the-three-delays-model_Final.pdf (accessed on 15 May 2025).
- Jalali, M.S.; Botticelli, M.; Hwang, R.C.; Koh, H.K.; McHugh, R.K. The opioid crisis: A contextual, social-ecological framework. Health Res. Policy Syst. 2020, 18, 87. [Google Scholar] [CrossRef] [PubMed]
- CDC. Polysubstance Use During Pregnancy. Pregnancy. 2024. Available online: https://www.cdc.gov/pregnancy/during/polysubstance-use.html (accessed on 15 May 2025).
- Office USGA. Maternal Health: HHS Should Improve Assessment of Efforts to Address Worsening Outcomes. U.S. GAO. 2024. Available online: https://www.gao.gov/products/gao-24-106271 (accessed on 15 May 2025).
- Office on Women’s Health. Maternal Health. Office on Women’s Health. OASH. Office on Women’s Health. 2022. Available online: https://womenshealth.gov/maternalhealth (accessed on 15 May 2025).
- World Health Organization. Maternal Health. Who.int. World Health Organization. 2019. Available online: https://www.who.int/health-topics/maternal-health#tab=tab_1 (accessed on 15 May 2025).
- Blanchin, M.; Guilleux, A.; Hardouin, J.B.; Sébille, V. Comparison of structural equation modelling, item response theory and Rasch measurement theory-based methods for response shift detection at item level: A simulation study. Stat. Methods Med. Res. 2019, 29, 096228021988457. [Google Scholar] [CrossRef]
- Lu, I.R.R.; Thomas, D.R.; Zumbo, B.D. Embedding IRT in Structural Equation Models: A Comparison With Regression Based on IRT Scores. Struct. Equ. Model. Multidiscip. J. 2005, 12, 263–277. [Google Scholar] [CrossRef]
- Tennessee Department of Health. Tennessee PRAMS Annual Summary Report 2020; Tennessee Department of Health: Nashville, TN, USA, 2020. Available online: https://www.tn.gov/content/dam/tn/health/documents/PRAMS-Summary-Report-2020.pdf (accessed on 15 May 2025).
- Phommachanh, S.; Essink, D.R.; Wright, P.E.; Broerse, J.E.W.; Mayxay, M. Maternal health literacy on mother and child health care: A community cluster survey in two southern provinces in Laos. PLoS ONE 2021, 16, e0244181. [Google Scholar] [CrossRef]
- Zhao, Y.; Segalowitz, N.; Voloshyn, A.; Chamoux, E.; Ryder, A.G. Language barriers to healthcare for linguistic minorities: The case of second language-specific health communication anxiety. Health Commun. 2019, 36, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Yadav, R.; Zaman, K.; Mishra, A.; Reddy, M.M.; Shankar, P.; Yadav, P.; Kumar, K.; Kant, R. Health Seeking Behaviour and Healthcare Utilization in a Rural Cohort of North India. Healthcare 2022, 10, 757. [Google Scholar] [CrossRef] [PubMed]
- Interrante, J.D.; Admon, L.K.; Carroll, C.; Henning-Smith, C.; Chastain, P.; Kozhimannil, K.B. Association of Health Insurance, Geography, and Race and Ethnicity With Disparities in Receipt of Recommended Postpartum Care in the US. JAMA Health Forum 2022, 3, e223292. [Google Scholar] [CrossRef] [PubMed]
- Pacho, M.; Aymerich, C.; Pedruzo, B.; Salazar de Pablo, G.; Sesma, E.; Bordenave, M.; Dieguez, R.; Lopez-Zorroza, I.; Herrero, J.; Laborda, M.; et al. Substance use during pregnancy and risk of postpartum depression: A systematic review and meta-analysis. Front. Psychiatry 2023, 14, 1264998. [Google Scholar] [CrossRef] [PubMed]
- Harvey, I.; O’Brien, M. Addressing Health Disparities Through Patient Education: The Development of Culturally-Tailored Health Education Materials at Puentes de Salud. J. Community Health Nurs. 2011, 28, 181–189. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).