
Knowledge, Adherence, and Barriers to Gluten-Free Diet Among Adults with Celiac Disease in Saudi Arabia: A Pilot Study at a Tertiary Hospital in Madinah, Saudi Arabia
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Validation of Tools Used
2.4. Assessment of Knowledge Related to Support Program and Gluten-Free Diet
2.5. Assessment of Adherence to a Gluten-Free Diet
2.6. Assessment of Barriers to Adhering to a Gluten-Free Diet
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Sample of Celiac Disease Patients
3.2. Factors Related to the Health and Lifestyle of Celiac Disease Patients
3.3. Knowledge Related to a Gluten-Free Diet
3.4. Associations with Adherence to and Barriers to Adherence to a Gluten-Free Diet
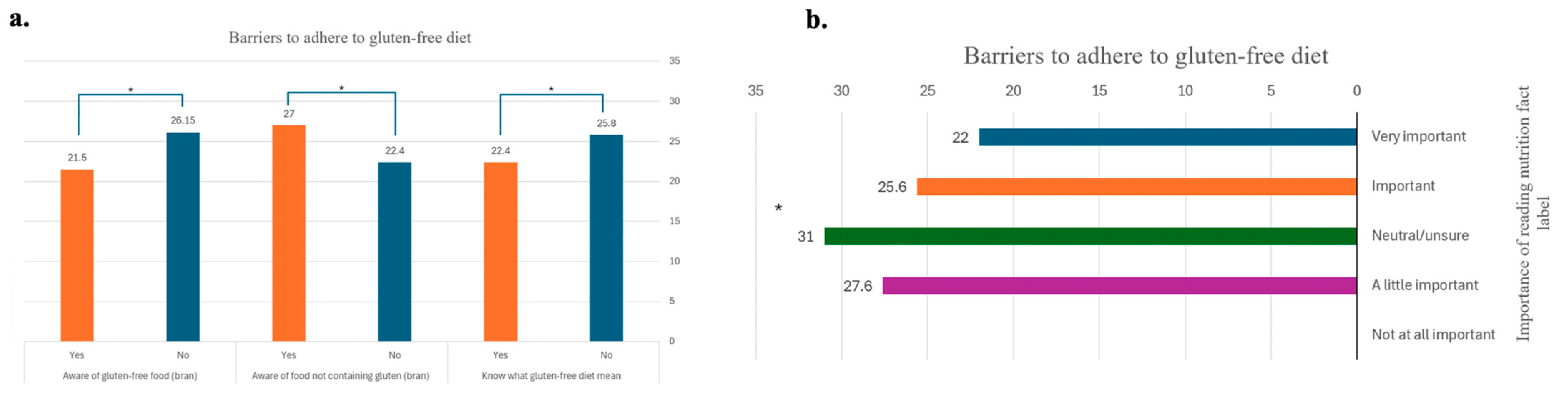
3.5. Knowledge Related to the Support Program and a Gluten-Free Diet in Relation to Adherence to and Barriers to Adherence to Gluten-Free Diet
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CD | Celiac disease |
| GFD | Gluten-free diet |
| GF | Gluten-free |
| TTG-IgA | Tissue Transglutaminase IgA |
References
- King, J.A.; Jeong, J.; Underwood, F.E.; Quan, J.; Panaccione, N.; Windsor, J.W.; Coward, S.; Debruyn, J.; Ronksley, P.E.; Shaheen, A.-A.; et al. Incidence of Celiac Disease Is Increasing Over Time: A Systematic Review and Meta-analysis. Am. J. Gastroenterol. 2020, 115, 507–525. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836.e2. [Google Scholar] [CrossRef] [PubMed]
- Allowaymi, S.S.; Binobead, M.A.; Alshammari, G.M.; Alrasheed, A.; Mohammed, M.A.; Yahya, M.A. Nutritional Status of Saudi Children with Celiac Disease Following the Ministry of Health’s Gluten-Free Diet Program. Nutrients 2022, 14, 2792. [Google Scholar] [CrossRef]
- Al Hatlani, M.M. Prevalence of celiac disease among symptom-free children from the Eastern Province of Saudi Arabia. Saudi J. Gastroenterol. 2015, 21, 367–371. [Google Scholar] [CrossRef]
- Kreutz, J.M.; Adriaanse, M.P.M.; van der Ploeg, E.M.C.; Vreugdenhil, A.C.E. Narrative Review: Nutrient Deficiencies in Adults and Children with Treated and Untreated Celiac Disease. Nutrients 2020, 12, 500. [Google Scholar] [CrossRef] [PubMed]
- Itzlinger, A.; Branchi, F.; Elli, L.; Schumann, M. Gluten-Free Diet in Celiac Disease-Forever and for All? Nutrients 2018, 10, 1796. [Google Scholar] [CrossRef]
- Newnham, E.D.; Shepherd, S.J.; Strauss, B.J.; Hosking, P.; Gibson, P.R. Adherence to the gluten-free diet can achieve the therapeutic goals in almost all patients with coeliac disease: A 5-year longitudinal study from diagnosis. J. Gastroenterol. Hepatol. 2016, 31, 342–349. [Google Scholar] [CrossRef]
- Muhammad, H.; Reeves, S.; Jeanes, Y.M. Identifying and improving adherence to the gluten-free diet in people with coeliac disease. Proc. Nutr. Soc. 2019, 78, 418–425. [Google Scholar] [CrossRef]
- Abu-Janb, N.; Jaana, M. Facilitators and barriers to adherence to gluten-free diet among adults with celiac disease: A systematic review. J. Hum. Nutr. Diet. 2020, 33, 786–810. [Google Scholar] [CrossRef]
- Hall, N.J.; Rubin, G.; Charnock, A. Systematic review: Adherence to a gluten-free diet in adult patients with coeliac disease. Aliment. Pharmacol. Ther. 2009, 30, 315–330. [Google Scholar] [CrossRef]
- Health Mo. Gluten-Free-Food-Program 2019. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/Ads/Documents/Gluten-Free-Food-Program.pdf (accessed on 19 May 2025).
- Safi, M.A. Celiac disease among at-risk individuals in Saudi Arabia. Saudi Med. J. 2019, 40, 9–18. [Google Scholar] [CrossRef]
- Hulley, S.B.; Cummings, S.R.; Browner, W.S.; Grady, D.G.; Newman, T.B. Designing Clinical Research, 4th ed.; Wolters Kluwer: Alfen am Rhine, The Netherlands, 2013. [Google Scholar]
- Leffler, D.A.; Dennis, M.; Edwards George, J.B.; Jamma, S.; Magge, S.; Cook, E.F.; Schuppan, D.; Kelly, C.P. A simple validated gluten-free diet adherence survey for adults with celiac disease. Clin. Gastroenterol. Hepatol. 2009, 7, 530–536.e2. [Google Scholar] [CrossRef]
- Muhammad, H.; Reeves, S.; Ishaq, S.; Mayberry, J.; Jeanes, Y.M. Adherence to a Gluten Free Diet Is Associated with Receiving Gluten Free Foods on Prescription and Understanding Food Labelling. Nutrients 2017, 9, 705. [Google Scholar] [CrossRef] [PubMed]
- Bathrellou, E.; Georgopoulou, A.; Kontogianni, M. Perceived barriers to gluten-free diet adherence by people with celiac disease in Greece. Ann. Gastroenterol. 2023, 36, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Wieser, H.; Ruiz-Carnicer, A.; Segura, V.; Comino, I.; Sousa, C. Challenges of Monitoring the Gluten-Free Diet Adherence in the Management and Follow-Up of Patients with Celiac Disease. Nutrients 2021, 13, 2274. [Google Scholar] [CrossRef]
- Villafuerte-Galvez, J.; Vanga, R.R.; Dennis, M.; Hansen, J.; Leffler, D.A.; Kelly, C.P.; Mukherjee, R. Factors governing long-term adherence to a gluten-free diet in adult patients with coeliac disease. Aliment. Pharmacol. Ther. 2015, 42, 753–760. [Google Scholar] [CrossRef]
- Qashqari, L.; Shakweer, D.; Alzaben, A.S.; Hanbazaza, M.A. Investigation of cost and availability of gluten-free food in Jeddah, KSA. J. Taibah Univ. Med. Sci. 2024, 19, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Al-Barqi, R.; Al-Salem, Y.; Mahrous, L.; Abat, E.; Al-Quraishi, R.; Benajiba, N. Understanding barriers towards the use of food labels among Saudi female college students. Malays. J. Nutr. 2020, 26, 19–30. [Google Scholar] [CrossRef]
- Verma, A.K. Nutritional Deficiencies in Celiac Disease: Current Perspectives. Nutrients 2021, 13, 4476. [Google Scholar] [CrossRef]
- Ullah, M.I.; Alsrhani, A.; Atif, M.; Shaukat, I.; Hussain, S.; Ejaz, H. Estimation of serum iron, serum lipids and serum liver enzymes in celiac disease patients of Saudi Arabia. Pak. J. Med. Sci. 2022, 38, 2101–2106. [Google Scholar]
- Perez-Junkera, G.; Simon, E.; Calvo, A.E.; Garcia Casales, Z.; Oliver Goicolea, P.; Serrano-Vela, J.I.; Larretxi, I.; Lasa, A. Importance of an Ongoing Nutritional Counselling Intervention on Eating Habits of Newly Diagnosed Children with Celiac Disease. Nutrients 2024, 16, 2418. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Escobar, P.; Vazquez-Polo, M.; van der Hofstadt, M.; Nunez, C.; Montoro-Huguet, M.A.; Churruca, I.; Simón, E. Knowledge Gaps in Gluten-Free Diet Awareness among Patients and Healthcare Professionals: A Call for Enhanced Nutritional Education. Nutrients 2024, 16, 2512. [Google Scholar] [CrossRef] [PubMed]
- Gladys, K.; Dardzinska, J.; Guzek, M.; Adrych, K.; Kochan, Z.; Malgorzewicz, S. Expanded Role of a Dietitian in Monitoring a Gluten-Free Diet in Patients with Celiac Disease: Implications for Clinical Practice. Nutrients 2021, 13, 1859. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cheng, Z. Cross-Sectional Studies: Strengths, Weaknesses, and Recommendations. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef]
- National Institutes of Health. Pilot Studies: Common Uses and Misuses. 2025. Available online: https://www.nccih.nih.gov/grants/pilot-studies-common-uses-and-misuses (accessed on 19 May 2025).


{kind=link}
{kind=link}
| Variable | n | % |
|---|---|---|
| Gender | ||
| Male | 9 | 25.0 |
| Female | 27 | 75.0 |
| Age group | ||
| 19–30 years | 11 | 30.6 |
| 31–40 years | 11 | 30.6 |
| 41–50 years | 9 | 25.0 |
| >50 years | 5 | 13.9 |
| Marital status | ||
| Single | 13 | 36.1 |
| Married | 23 | 63.9 |
| Family monthly income | ||
| <SAR 6000 | 16 | 44.4 |
| SAR 6000–10,999 | 10 | 27.8 |
| SAR 11,000–15,999 | 2 | 5.56 |
| ≥SAR 16,000 | 8 | 22.2 |
| Education level | ||
| <High-school | 4 | 11.1 |
| High-school/Diploma | 11 | 30.6 |
| Undergraduate degree | 18 | 50.0 |
| Postgraduate degree | 3 | 8.33 |
| Work status | ||
| Student | 4 | 11.1 |
| Employed | 12 | 33.3 |
| Unemployed/Retired/Other | 20 | 55.5 |
| Place of residency | ||
| Madinah | 32 | 88.9 |
| Other cities in Madinah province | 4 | 11.1 |
| Variable | n | % |
|---|---|---|
| Sleeping hours per day | ||
| <7 h | 15 | 41.7 |
| ≥7 h | 21 | 58.3 |
| Weight status | ||
| Underweight (<18.5 kg/m2) | 7 | 19.4 |
| Healthy weight (18.5–24.9 kg/m2) | 17 | 47.2 |
| Overweight (25–29.9 kg/m2) | 6 | 16.7 |
| Obesity (≥30 kg/m2) | 6 | 16.7 |
| Visited dietitian | ||
| No | 21 | 58.3 |
| Yes | 15 | 41.7 |
| Frequency of visiting dietitian | ||
| Never | 21 | 58.3 |
| Once | 8 | 22.2 |
| More than once | 7 | 19.4 |
| Supplement use | ||
| No | 12 | 33.3 |
| Yes | 24 | 66.7 |
| Other chronic diseases | ||
| No | 6 | 16.7 |
| Yes | 30 | 83.3 |
| Diabetes, yes | 8 | 26.6 |
| Hypertension, yes | 3 | 10.0 |
| Renal disease, yes | 3 | 10.0 |
| Other autoimmune diseases | ||
| No | 21 | 58.3 |
| Yes | 15 | 41.7 |
| Thyroid diseases, yes | 11 | 30.6 |
| Arthritis, yes | 4 | 11.1 |
| Crohn’s disease, yes | 1 | 2.78 |
| Variable | Adherence to Gluten-Free Diet Score Out of 35 | Barriers to Adhere to Gluten-Free Diet Score Out of 35 |
|---|---|---|
| Sleeping hours per day | ||
| <7 h | 25.6 ± 4.03 | 21.7 ± 4.13 |
| ≥7 h | 24.5 ± 5.17 | 24.2 ± 3.49 |
| p-value | 0.506 | 0.053 |
| Weight status | ||
| Underweight (BMI < 18.5 kg/m2) | 23.2 ± 4.15 | 22.4 ± 4.99 |
| Healthy weight (BMI 18.5–24.9 kg/m2) | 26.8 ± 3.79 | 23.5 ± 3.34 |
| Overweight (BMI 25–29.9 kg/m2) | 22.6 ± 5.64 | 23.0 ± 4.42 |
| Obese (BMI ≥ 30 kg/m2) | 24.5 ± 6.09 | 23.1 ± 4.70 |
| p-value | 0.194 | 0.952 |
| Visited dietitian | ||
| No | 24.1 ± 5.05 | 24.0 ± 3.49 |
| Yes | 26.2 ± 3.98 | 22.1 ± 4.35 |
| p-value | 0.189 | 0.163 |
| Frequency of visiting dietitian | ||
| Never | 24.1 ± 5.05 | 24.0 ± 3.49 |
| Once | 25.3 ± 3.62 | 21.3 ± 3.37 |
| More than once | 27.1 ± 4.45 | 23.0 ± 5.41 |
| p-value | 0.328 | 0.278 |
| Supplement use | ||
| No | 23.7 ± 4.55 | 24.3 ± 4.29 |
| Yes | 25.5 ± 4.74 | 22.6 ± 3.70 |
| p-value | 0.276 | 0.235 |
| Other chronic diseases | ||
| No | 26.0 ± 4.73 | 21.1 ± 4.26 |
| Yes | 24.7 ± 4.74 | 23.6 ± 3.80 |
| p-value | 0.565 | 0.163 |
| Diabetes | ||
| No | 25.0 ± 4.81 | 22.5 ± 3.69 |
| Yes | 24.8 ± 4.58 | 25.6 ± 3.99 |
| p-value | 0.948 | 0.048 |
| Hypertension | ||
| No | 24.6 ± 4.78 | 23.3 ± 3.95 |
| Yes | 28.3 ± 1.52 | 21.6 ± 4.04 |
| p-value | 0.200 | 0.482 |
| Renal disease | ||
| No | 25.2 ± 4.64 | 23.2 ± 4.05 |
| Yes | 22.3 ± 5.50 | 23.0 ± 2.64 |
| p-value | 0.317 | 0.920 |
| Other autoimmune diseases (thyroid diseases, arthritis, Crohn’s disease) | ||
| No | 24.9 ± 5.50 | 24.1 ± 3.30 |
| Yes | 25.0 ± 3.45 | 21.9 ± 4.46 |
| p-value | 0.921 | 0.097 |
| Thyroid diseases | ||
| No | 25.0 ± 5.37 | 23.8 ± 3.72 |
| Yes | 24.8 ± 2.82 | 21.7 ± 4.14 |
| p-value | 0.898 | 0.132 |
| Arthritis | ||
| No | 24.6 ± 4.81 | 23.5 ± 3.81 |
| Yes | 27.5 ± 3.00 | 20.2 ± 4.03 |
| p-value | 0.260 | 0.110 |
| Crohn’s disease | ||
| No | 25.1 ± 4.65 | 23.0 ± 3.85 |
| Yes | 19.0 ± 0.00 | 29.0 ± 0.00 |
| p-value | 0.202 | 0.138 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsayb, M.A.; Alharbi, S.A.; Alloqmani, R.H.; Madkli, G.A.; Basharahil, R.A.; Alhejaili, M.I.; Mumena, W.A. Knowledge, Adherence, and Barriers to Gluten-Free Diet Among Adults with Celiac Disease in Saudi Arabia: A Pilot Study at a Tertiary Hospital in Madinah, Saudi Arabia. Healthcare 2025, 13, 1208. https://doi.org/10.3390/healthcare13101208
Alsayb MA, Alharbi SA, Alloqmani RH, Madkli GA, Basharahil RA, Alhejaili MI, Mumena WA. Knowledge, Adherence, and Barriers to Gluten-Free Diet Among Adults with Celiac Disease in Saudi Arabia: A Pilot Study at a Tertiary Hospital in Madinah, Saudi Arabia. Healthcare. 2025; 13(10):1208. https://doi.org/10.3390/healthcare13101208
Chicago/Turabian StyleAlsayb, May A., Suliman A. Alharbi, Renad H. Alloqmani, Ghaida A. Madkli, Rahaf A. Basharahil, Marah I. Alhejaili, and Walaa A. Mumena. 2025. "Knowledge, Adherence, and Barriers to Gluten-Free Diet Among Adults with Celiac Disease in Saudi Arabia: A Pilot Study at a Tertiary Hospital in Madinah, Saudi Arabia" Healthcare 13, no. 10: 1208. https://doi.org/10.3390/healthcare13101208
APA StyleAlsayb, M. A., Alharbi, S. A., Alloqmani, R. H., Madkli, G. A., Basharahil, R. A., Alhejaili, M. I., & Mumena, W. A. (2025). Knowledge, Adherence, and Barriers to Gluten-Free Diet Among Adults with Celiac Disease in Saudi Arabia: A Pilot Study at a Tertiary Hospital in Madinah, Saudi Arabia. Healthcare, 13(10), 1208. https://doi.org/10.3390/healthcare13101208