Abstract
Background/Objectives: Pertussis-like syndrome (PLS) presents symptoms similar to whooping cough but without Bordetella pertussis detection. This study assessed the efficacy and safety of combined treatment herbal and Western medicine (HM and WM, respectively) for PLS. Methods: Eleven English, Chinese, Korean, and Japanese databases were searched until 1 December 2024. Randomized clinical trials (RCTs) that compared HM with WM versus WM alone in children with PLS were included. Independent searches and risk-of-bias analyses were conducted. Random-effects and fixed-effects models were utilized. Dichotomous outcomes are presented as the risk ratio (RR) with 95% confidence interval (CI), and continuous outcomes as either the standard mean difference (SMD) or mean difference (MD) with 95% CI. Results: A total of 23 RCTs (performed in China) with 1938 participants were included. The meta-analysis showed that HM with WM is more effective than WM in improving the total effective rate [n = 1888; RR = 1.20; 95% CI: 1.16–1.24; p < 0.001], reducing the disappearance time of main symptoms (especially spastic cough) [n = 815; MD = −3.31; 95% CI: −3.51–−3.11; p < 0.001], shortening the recovery time of routine blood parameters to the normal range [n = 472; MD = −2.79; 95% CI: −3.06–−2.52; p < 0.001], and decreasing hospitalization duration [n = 703; MD = −2.61; 95% CI: −2.85–−2.38; p < 0.001]. Only mild adverse events were reported, with a lower occurrence rate in HM with WM cohorts than in WM cohorts. The quality of evidence ranged from moderate to very low. Conclusions: HM combined with WM is effective and safe for PLS in children, offering a potential alternative for symptom relief.
1. Introduction
Whooping cough (pertussis) is a type of acute respiratory disease induced by Bordetella pertussis (B. pertussis) infection and is among the top 10 fatal infections in children [1]. When pertussis infection is suspected, clinical history and symptoms are evaluated. To confirm the diagnosis, laboratory tests, such as white blood cell count, absolute lymphocyte count, bacterial culture, polymerase chain reaction, and chest X-ray, should be conducted [2]. Pertussis is a global infectious disease that requires reporting of cases to the government. According to the World Health Organization (WHO), global pertussis incidence rates were 4.6–9.9 during 2020–2022. These rates surged to 22.7 and 35.7 per 1,000,000 total population during 2023 and 2024, respectively [3]. In particular, the pertussis resurgence rate in Europe in 2023 was approximately 14 times higher than that in 2022 [3]. The incidence rates were also higher in 2024 than in the same period in 2023 in various countries, including the United States (six times), South Korea (164 times), and China (12 times) [4,5,6].
If clinical signs and test results do not confirm pertussis, the condition is referred to as a pertussis-like syndrome (PLS). PLS is reported at any age but is more prevalent in children. PLS can be particularly challenging for children and their parents because its symptoms often disrupt quality of life and cause sleep disorders [7]. In one study, only 19.8% of children with similar symptoms tested positive for B. pertussis [8]. Consequently, the incidence of pertussis has increased rapidly, indicating that PLS should be treated with caution.
Whooping cough has an incubation period of 5–21 days. The catarrhal stage (1–2 weeks) is characterized by upper respiratory symptoms such as rhinorrhea, excessive tearing, and mild cough. The paroxysmal stage (1–6 weeks) is characterized by severe spastic cough followed by post-tussive vomiting. In the convalescent stage (lasting for 2–4 weeks), paroxysmal cough may recur due to infections [2]. However, B. pertussis infection is not the only cause of these clinical symptoms. Other pathogens, including adenovirus, influenza virus, and Mycoplasma species, can cause similar symptoms, collectively termed PLS, making differential diagnosis challenging due to the lack of distinctive clinical features [9].
In Western medicine (WM), whooping cough (and PLS) is generally treated with antibiotics, such as erythromycin and azithromycin [10]. Erythromycin and azithromycin are also used to treat other respiratory diseases, such as diffuse panbronchiolitis, bronchiectasis, rhinosinusitis, and cystic fibrosis, as inflammation and immunity modulators [11]. The limitation of antibiotic use is that it does not dramatically relieve the clinical symptoms of the illness, such as spastic cough, even though the treatment is effective in eliminating pathogens [12]. This has prompted interest in herbal medicines (HMs) as potential alternatives to WM for symptom relief. Previous studies have demonstrated the efficacy of HM in managing respiratory diseases. For example, a combination of HMs including Glycyrrhizae Radix et Rhizoma and Pinelliae Rhizoma improved lung function in patients with asthma, which is characterized by spastic cough but not an infectious disease, and also reduced the dosage of WMs [13]. HMs (such as Zhisou-san) are effective in decreasing cough severity and recurrence rates in nonspecific chronic coughs, and Glycyrrhizae Radix et Rhizoma, Pinelliae Tuber, Platycodonis Radix, and Armeniacae Semen are frequently used herbs [14]. Since HM use can relieve symptoms of respiratory diseases that are difficult to manage using only WM, a combination of HM and WM in PLS may also be effective.
No meta-analysis or systematic review has addressed the use of HMs for PLS. This study aimed to evaluate the efficacy and safety of the combination of HM and WM for PLS.
2. Materials and Methods
2.1. Protocol and Registration
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [15] (Table S1). The study protocol was registered in PROSPERO (ID: CRD42024561529), and modified to specify the outcome indicators.
2.2. Eligibility Criteria
2.2.1. Types of Studies
RCTs evaluating HM for PLS in children and adolescents were included. Non-RCTs, case reports, animal studies, gray literature, surveys, and review articles were excluded.
2.2.2. Types of Participants
Participants included children and adolescents aged <18 years diagnosed with PLS. Those diagnosed with B. pertussis infection were excluded.
2.2.3. Types of Interventions
The experimental group received oral HM, with no restrictions on the number of herb ingredients, formulations (such as powder, granules, or decoctions), dosages, or duration. Conventional treatments, including WMs, such as azithromycin and erythromycin, were considered only if the control group received identical treatments.
2.2.4. Types of Comparisons
If conventional treatments were administered to the experimental group, equivalent treatments were provided to the control group.
2.2.5. Types of Outcome Measurements
The main outcome was the total effective rate (TER). Secondary outcomes included the disappearance time of primary symptoms, such as spastic cough, the recovery time of blood routine parameters to normal range, hospitalization duration, and adverse events.
2.3. Information Sources and Search Strategy
Eleven databases were searched until 1 December 2024, without limitations on country, language, and publication year. The databases included three English-language sources (PubMed, Excerpta Medica Database, and the Cochrane Central Register of Controlled Trials), three Chinese databases (China National Knowledge Infrastructure, VIP, and Wanfang Database), four Korean databases (Oriental Medicine Advanced Searching Integrated System, Korean Studies Information Service System, Korea Citation Index, and Research Information Sharing Service), and one Japanese database (CiNii). The main terms for searching included “whooping cough”, “pertussis-like syndrome”, and “herbal medicine”, which were tailored to each database’s language requirements. More specific search strategies and results are included (Table S2).
2.4. Study Selection and Data Extraction
2.4.1. Study Selection
Two reviewers (J.U.C. and Y.S.S.) independently screened titles and abstracts, and next then assessed full-text articles based on the inclusion and exclusion criteria. Any disagreements were resolved through discussion, and an additional reviewer (E.J.K.) made the final decision if there was no agreement.
2.4.2. Data Extraction
Two reviewers (J.U.C. and Y.S.S.) independently extracted information from the included studies. Any discrepancies were resolved through discussion among all reviewers. The missing information was resolved by contacting the corresponding author via email. Extracted data included first author, publication year, study location, sample size, duration of disease, total treatment period, participant characteristics, such as gender and age distribution, treatment interventions and comparisons, HM composition, outcome measurements, adverse events, and data for risk of bias assessment.
2.5. Statistical Analysis
Review Manager (RevMan) software (version 5.4, Cochrane Collaboration, London, UK) was used for performing the meta-analysis. Both random-effects and fixed-effects models were used. For dichotomous outcomes, the risk ratio (RR) with 95% confidence intervals (CIs) was applied, whereas for continuous outcomes, either the standard mean difference (SMD) or mean difference (MD) with 95% CIs was applied.
2.5.1. Assessment of Heterogeneity
Heterogeneity among included studies was assessed by using the Higgins I2 index [16]. When I2 was ≥50%, it indicates significant heterogeneity, and a random-effects model was applied. When I2 was <50%, indicating low heterogeneity, a fixed-effects model was applied.
2.5.2. Assessment of Reporting Bias
Publication bias was assessed when >10 studies were included for a specific outcome. Funnel plots were presented to visualize bias. If asymmetry suggested potential bias, Egger’s regression test, trim-and-fill, and Rosenthal fail-safe N method were performed.
2.5.3. Subgroup and Sensitivity Analysis
Due to the variability in HM composition, subgroup analyses were performed based on specific HM formulations. Sensitivity analysis was performed for the outcomes when data from at least 10 studies were available.
2.6. Quality Assessment
Two reviewers (J.U.C. and Y.S.S.) independently assessed the quality of included studies using the Cochrane Risk of Bias (RoB 2) tool, categorizing studies as having low risk of bias, some concerns regarding bias, or high risk of bias [17]. The assessment included five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported results. Any discrepancies between reviewers were resolved through discussions, and if there was no agreement, a third reviewer (E.J.K.) made the final decision.
The quality of evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework (http://gradepro.org (accessed on 1 February 2025)). The evaluation considered risk of bias, inconsistency, indirection, imprecision, and publication bias. The GRADE system categorized the quality of evidence as very low, low, moderate, and high.
3. Results
3.1. Study Selection
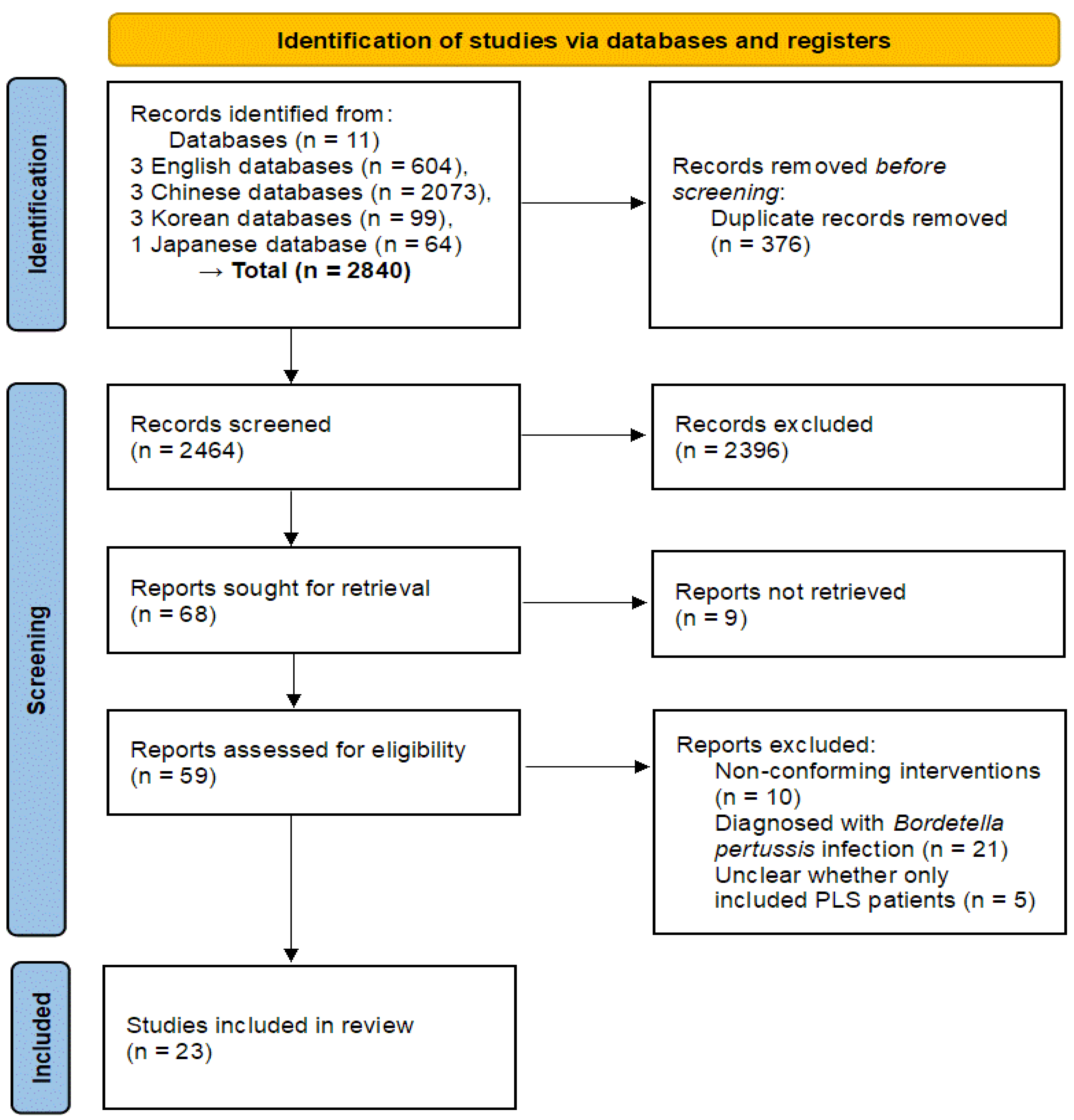
After applying the search strategy to each database, a total of 2840 records were retrieved. These consisted of 604 from English databases, 2073 from Chinese databases, 99 from Korean databases, and 64 from the Japanese database. Following deduplication, 2464 studies were left. After reviewing titles and abstracts, 68 studies were selected for further evaluation; however, 9 studies were inaccessible. All the 59 full-text articles assessed were based on RCTs. However, 10 studies were excluded due to non-conforming interventions. Twenty-one studies involved participants diagnosed with B. pertussis infection and were excluded. In five studies, it was unclear whether only patients with PLS were included. Ultimately, 23 RCTs [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] were selected (Figure 1).
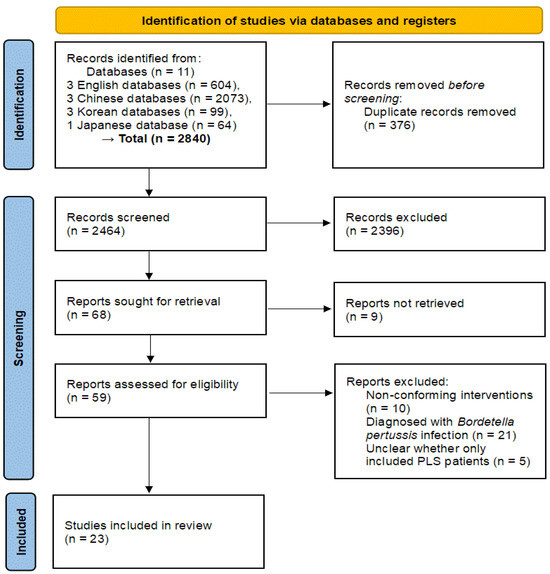
Figure 1.
PRISMA 2020 flow diagram. PLS, pertussis-like syndrome.
3.2. The Characteristics of the Study
All included 23 RCTs were conducted in China (although we did not apply any national restrictions) and published from 2015 to 2024. Sample sizes ranged from 40 to 140 participants, and the total treatment period ranged from 3 days to 2 weeks. The mean age distribution ranged from 9.89 ± 1.53 months to 6.26 ± 1.33 years. The duration of disease ranged from 5.2 ± 1.7 days to 35.71 ± 6.03 days. Most studies maintained identical total treatment durations for both the experimental and control groups (Table 1).

Table 1.
Basic characteristics of the included studies.
3.3. Interventions
Oral HMs were reported in all 23 studies. Twelve types of HM formulations were used, including Sangbaipi (SB) [18,19,20,21,25,34], Jiawei Weijing (WJ) [24,32,38], Chunggan Sapye decoction [28], Sosiho decoction with Sabaek powder [22], Canyu Dunke [23], Zhenhai Jingyan [27], Zhenhai Hwadam prescription [29], Dengtai Ye (DY) [30,35,36,37,40], Baikening [31], Xiaoer Feike granules [39], Lusika [26], and Heron Cough Pill [33]. The details of their compositions, dosages, and frequencies are provided in Table 2.
Table 2.
Herbal medicine information.
Glycyrrhizae Radix et Rhizoma was the most used ingredient, appearing in 16 RCTs, followed by Armeniacae Semen in 13 studies. Mori Cortex Radicis was included in 10 RCTs, whereas Pinelliae Rhizoma and Perillae Fructus were used in 9 RCTs each (Table S3).
In four studies [22,23,30,36], the experimental and control groups received additional treatments. All studies implemented respiratory support measures, such as inhalation therapy, nasal catheter use, and continuous positive airway pressure oxygen therapy. Three studies included antispasmodic treatments [23,30,36], whereas two studies aimed to relieve cough symptoms [30,36] (Table S4).
Western medications were also used for PLS treatment, including erythromycin [19,20,21,22,24,25,26,27,29,30,32,34,35,36,37,38,39,40], azithromycin [18,28], roxithromycin [33], ipratropium bromide [26], albuterol sulfate solution [26], budesonide [26,31], and montelukast [37].
3.4. Outcome Measures
Main outcome measures included TER [18,19,20,21,22,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40], the disappearance time of the main symptoms (mainly spastic cough) [22,23,29,30,32,35,36,37,40], the recovery time of routine blood parameters to normal range [18,19,21,25,34,40], hospitalization time [18,19,20,21,22,25,29,34,36], and adverse events [24,27,28,30,31,35,36,37,38,40].
TER was reported in 22 studies [18,19,20,21,22,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] and demonstrated the objective effects of HM compared to WM alone. The disappearance time of the main symptoms, especially spastic cough, was an important evaluation indicator since spastic cough is a key symptom in diagnosing PLS. Although 15 studies [18,19,20,22,23,25,28,29,30,32,34,35,36,37,40] reported disappearance times for the main symptoms, only 9 studies [22,23,29,30,32,35,36,37,40] specified the exact symptoms analyzed.
The recovery time of routine blood parameters to normal range was included as an evaluation criterion. While many studies reported inflammatory factors in blood routine tests, their variability prevented meaningful analysis. Therefore, only studies assessing recovery to normal levels were included. Six studies [18,19,21,25,34,40] met this criterion, whereas eight studies [22,26,28,29,30,32,33,35] were excluded.
Hospitalization time was considered a relevant evaluation indicator, as effective treatments could shorten hospital stays. Nine studies [18,19,20,21,22,25,29,34,36] reported hospitalization time and were included in the analysis.
Adverse events were reported in 10 studies [24,26,27,30,31,35,36,37,38,40]. One study [26] was excluded because it only reported symptoms of adverse events rather than the number of occurrences. Further details on adverse events are presented in Table S5.
3.5. Meta-Analysis
The meta-analysis was performed to compare the outcomes with HM and WM combined versus WM alone. When significant heterogeneity was observed, subgroup analysis about the type of HM was conducted for further evaluation of outcomes.
3.5.1. TER
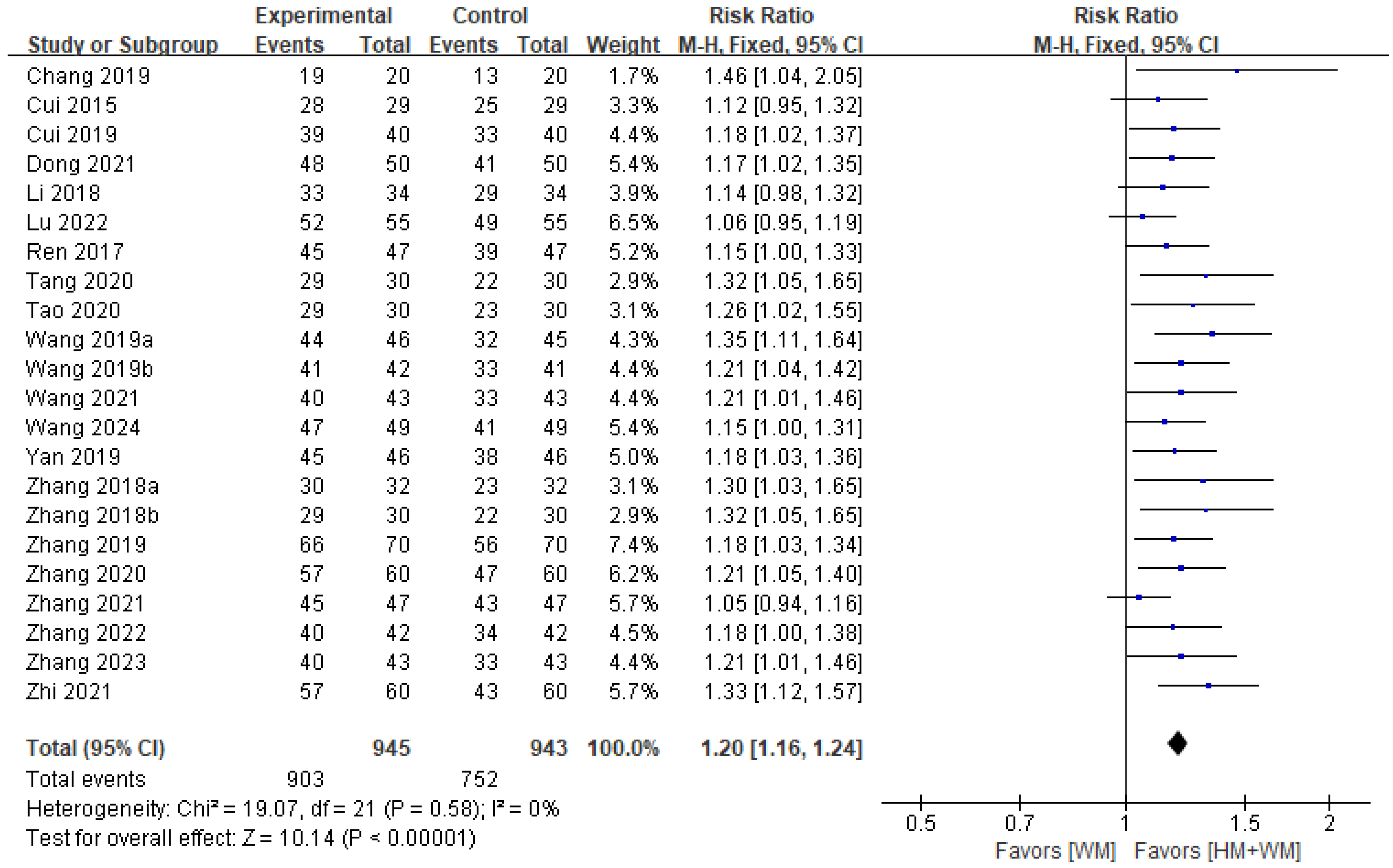
A total of 22 studies [18,19,20,21,22,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40], involving 1888 patients, reported TER and were included in the analysis. The results indicated no significant heterogeneity (p = 0.58, I2 = 0%), and a fixed-effects model was used. The analysis demonstrated that HM with WM was more effective than WM in improving TER (RR = 1.20; 95% CI: 1.16–1.24; p < 0.001, Figure 2). Since there was no heterogeneity and an adequate number of RCTs were included, additional subgroup analysis was not required.
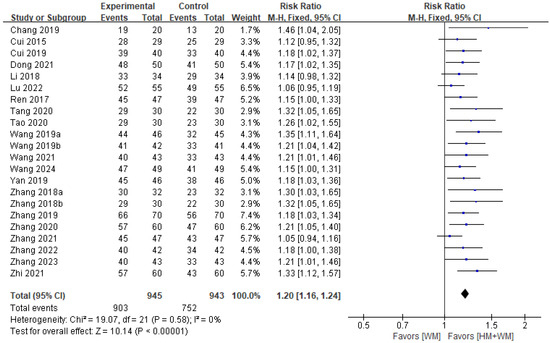
Figure 2.
A forest plot of the total effective rate [18,19,20,21,22,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40].
3.5.2. Disappearance Time of Main Symptoms (Spastic Cough)
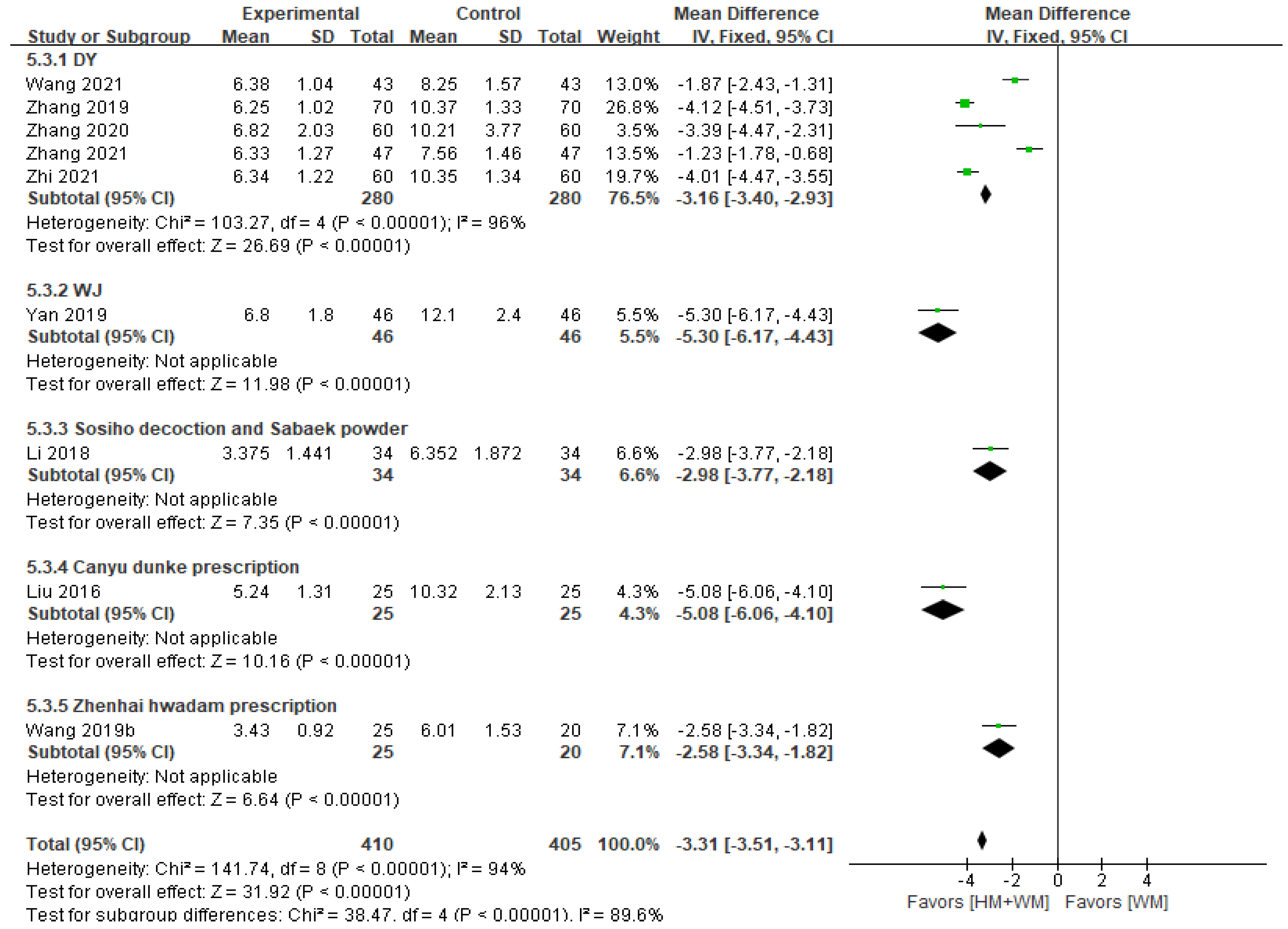
Nine studies [22,23,29,30,32,35,36,37,40], including 815 patients, reported the disappearance time of spastic cough. The meta-analysis showed that HM significantly reduced the disappearance time of spastic cough compared to WM alone (fixed-effects MD = −3.31, 95% CI: −3.51–−3.11, Figure 3). However, substantial heterogeneity was observed (p < 0.001, I2 = 94%). Subgroup analysis indicated that WJ was the most effective in reducing disappearance time (MD = −5.30, 95% CI: −6.17–−4.43).
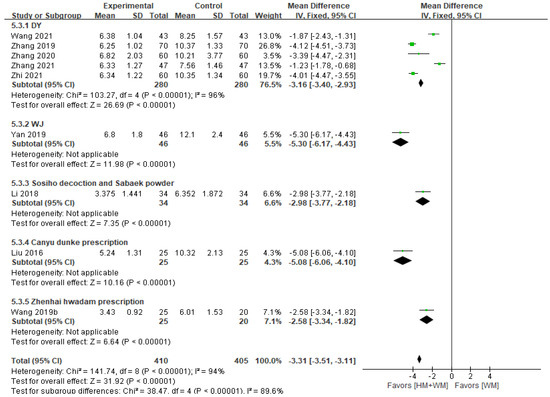
Figure 3.
A forest plot of the disappearance time of main symptoms (spastic cough). DY, Dengtai ye granule; WJ, Jiawei Weijing decoction [22,23,29,30,32,35,36,37,40].
3.5.3. Recovery Time of Blood Routine Parameters to Normal Range
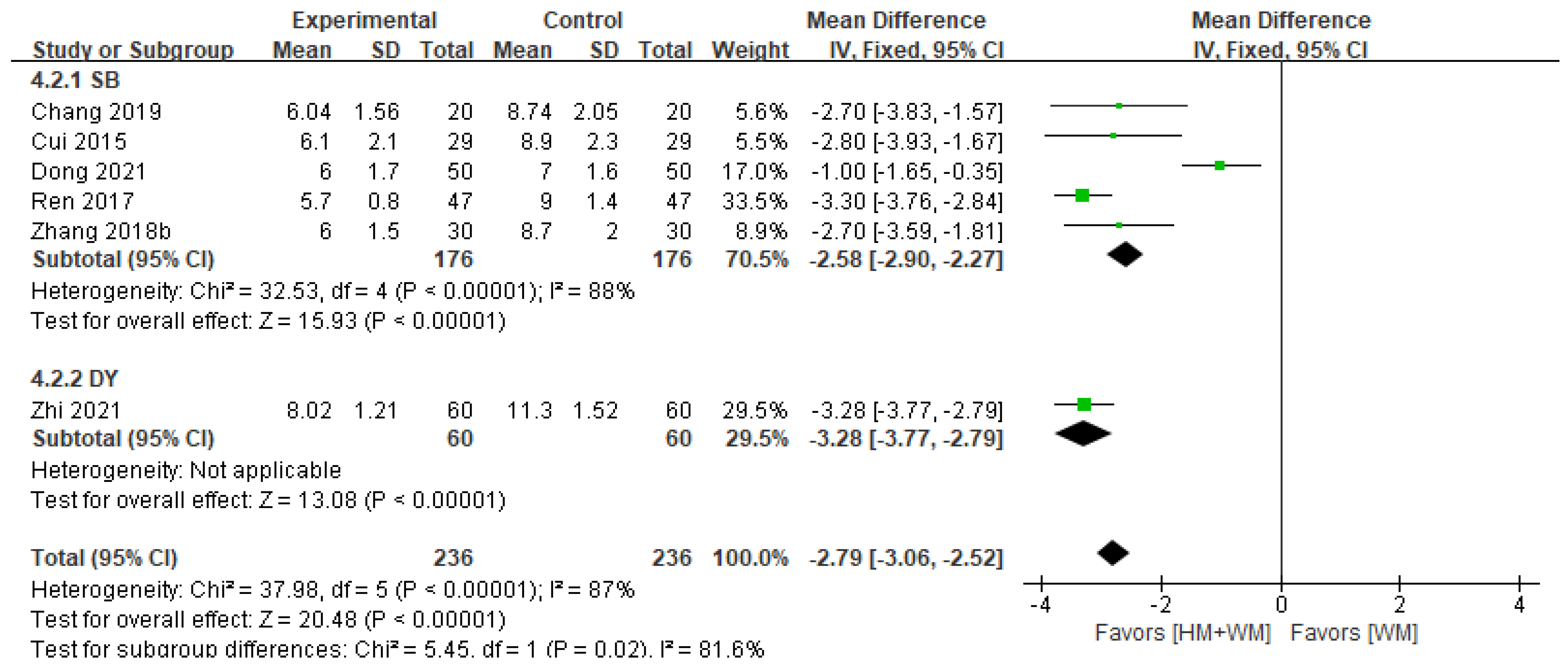
Six studies [18,19,21,25,34,40], involving 472 patients, assessed the recovery time of routine blood parameters to normal levels. HM was more effective than WM alone in accelerating recovery (fixed-effects MD = −2.79, 95% CI: −3.06–−2.52, I2 = 87%, p < 0.001, Figure 4). Subgroup analysis identified SB (MD = −2.58, 95% CI: −2.90–−2.27) and DY (MD = −3.25, 95% CI: −3.77–−2.79) as effective interventions for PLS.
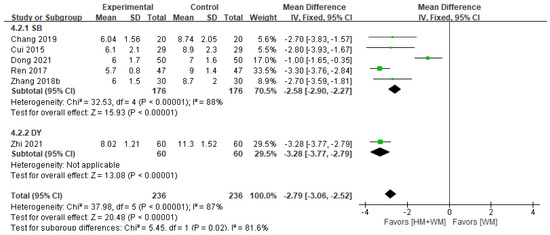
Figure 4.
A forest plot of the recovery time of blood routine to normal range. DY, Dengtai ye granule; SB, Sangbaipi decoction [18,19,21,25,34,40].
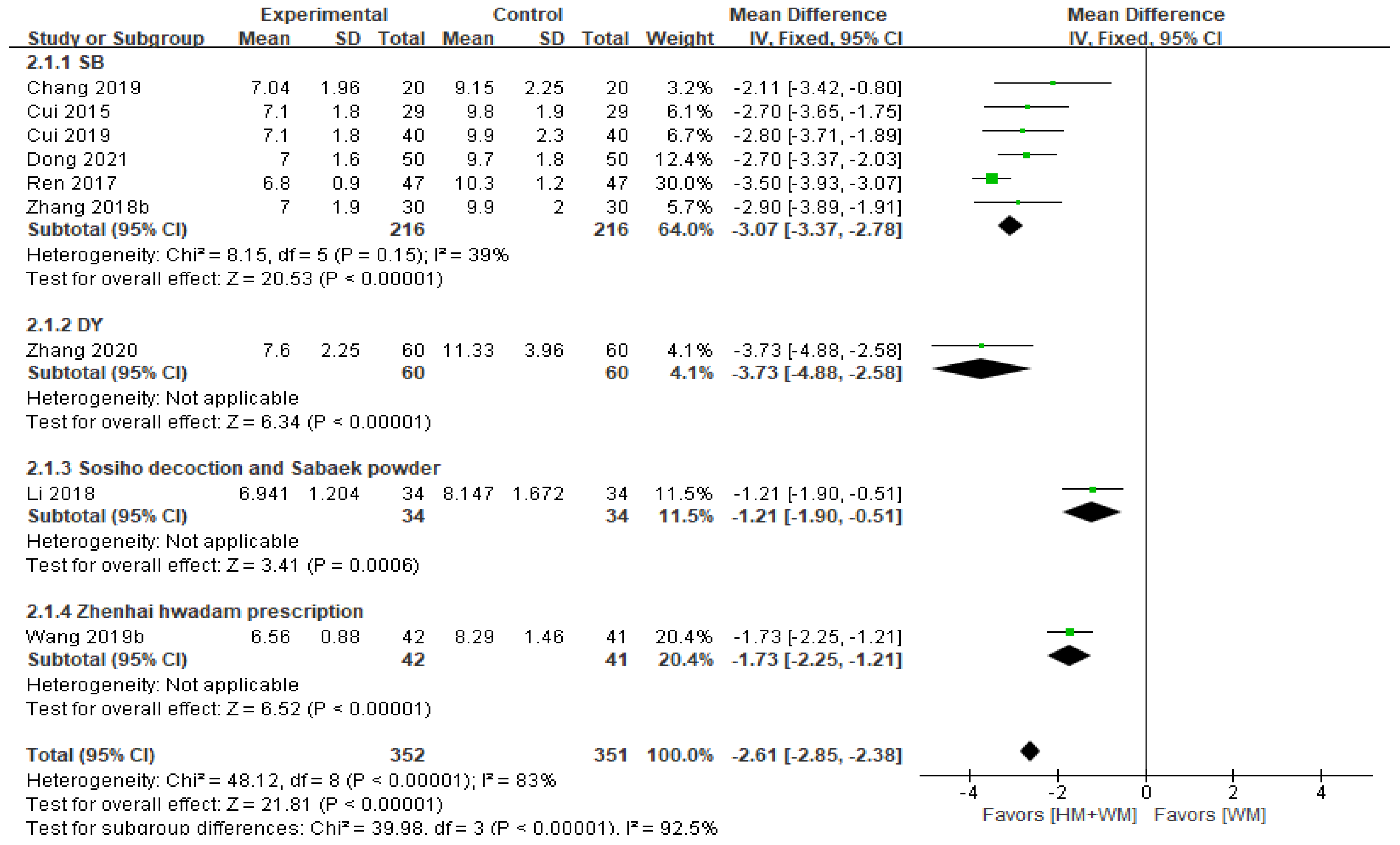
3.5.4. Hospitalization Time
Nine studies [18,19,20,21,22,25,29,34,36], with 703 patients, assessed hospitalization time. The analysis revealed that HM with WM significantly shortened hospitalization time (MD = −2.61, 95% CI: −2.85–−2.38, Figure 5). Subgroup analysis showed that SB (MD = −3.07, 95% CI: −3.37–−2.78) and DY (MD = −3.73, 95% CI: −4.88–−2.58) were more effective in reducing hospitalization time than other herbal formulations.
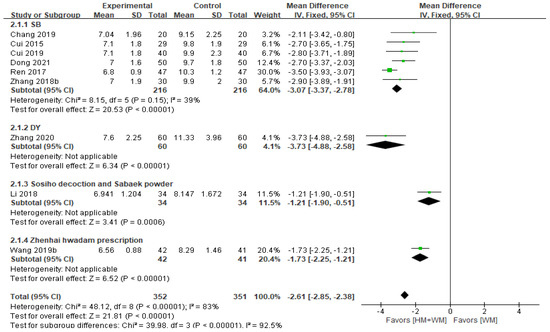
Figure 5.
A forest plot of the hospitalization time. DY, Dengtai ye granule; SB, Sangbaipi decoction [18,19,20,21,22,25,29,34,36].
3.6. Adverse Events
Nine studies [24,27,30,31,35,36,37,38,40] reported adverse events, involving 912 patients (456 each in the HM and WM groups). Only one study [35] reported no adverse events. In the HM with WM group, there were 27 cases of adverse events, whereas the WM group had 40 cases. The most frequently reported adverse events in the HM group included nausea and vomiting (nine cases), diarrhea, abdominal distension, abdominal pain, and increased frequency of defecation (each four cases). The WM group also reported nausea and vomiting (ten cases), diarrhea (seven cases), abdominal pain (five cases), abdominal distension (four cases), increased frequency of defecation, and abdominal discomfort (three cases). Other symptoms, such as rash and constipation, were rarely reported in either group. All adverse events were mild and resolved without additional treatments.
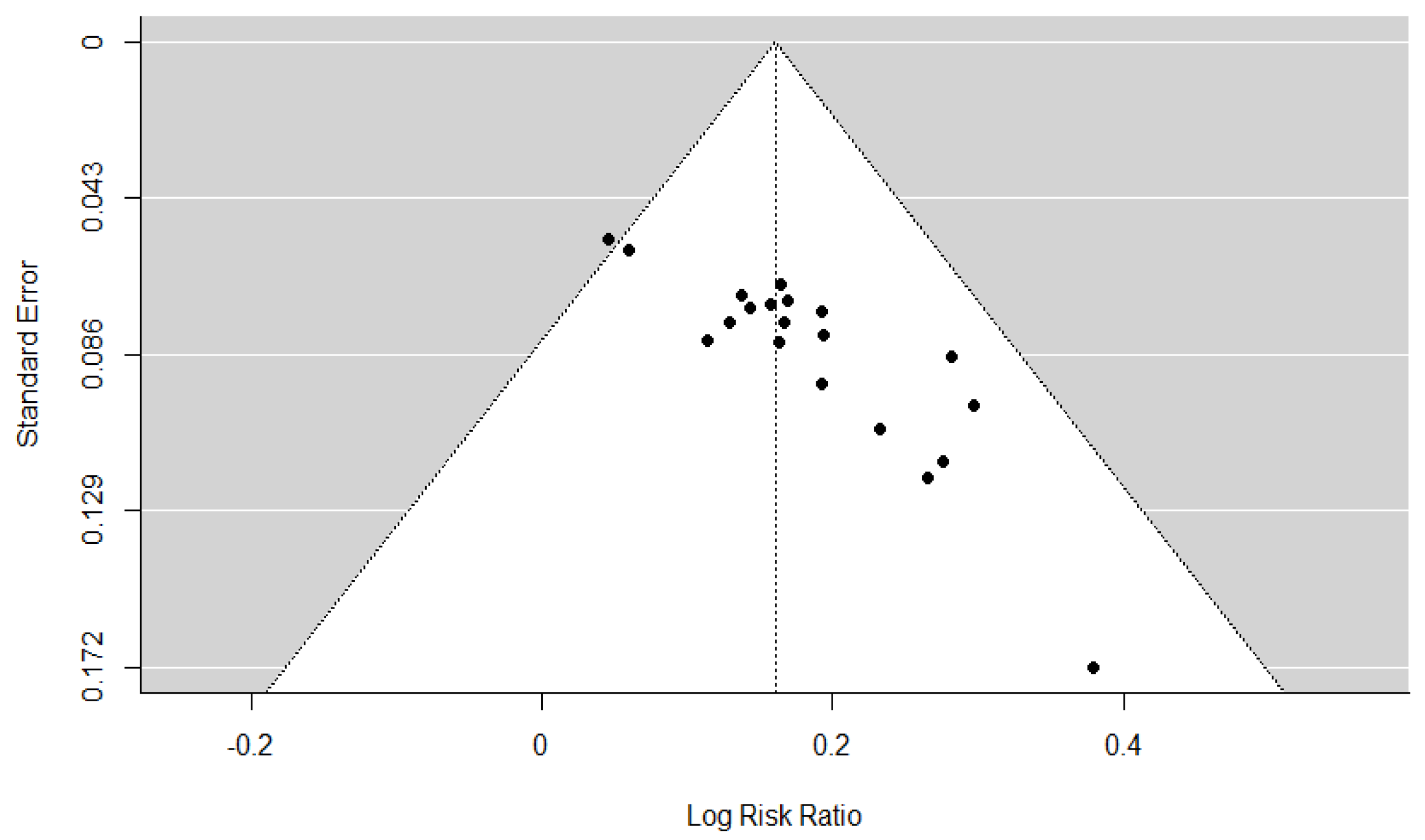
3.7. Assessment of Reporting Bias
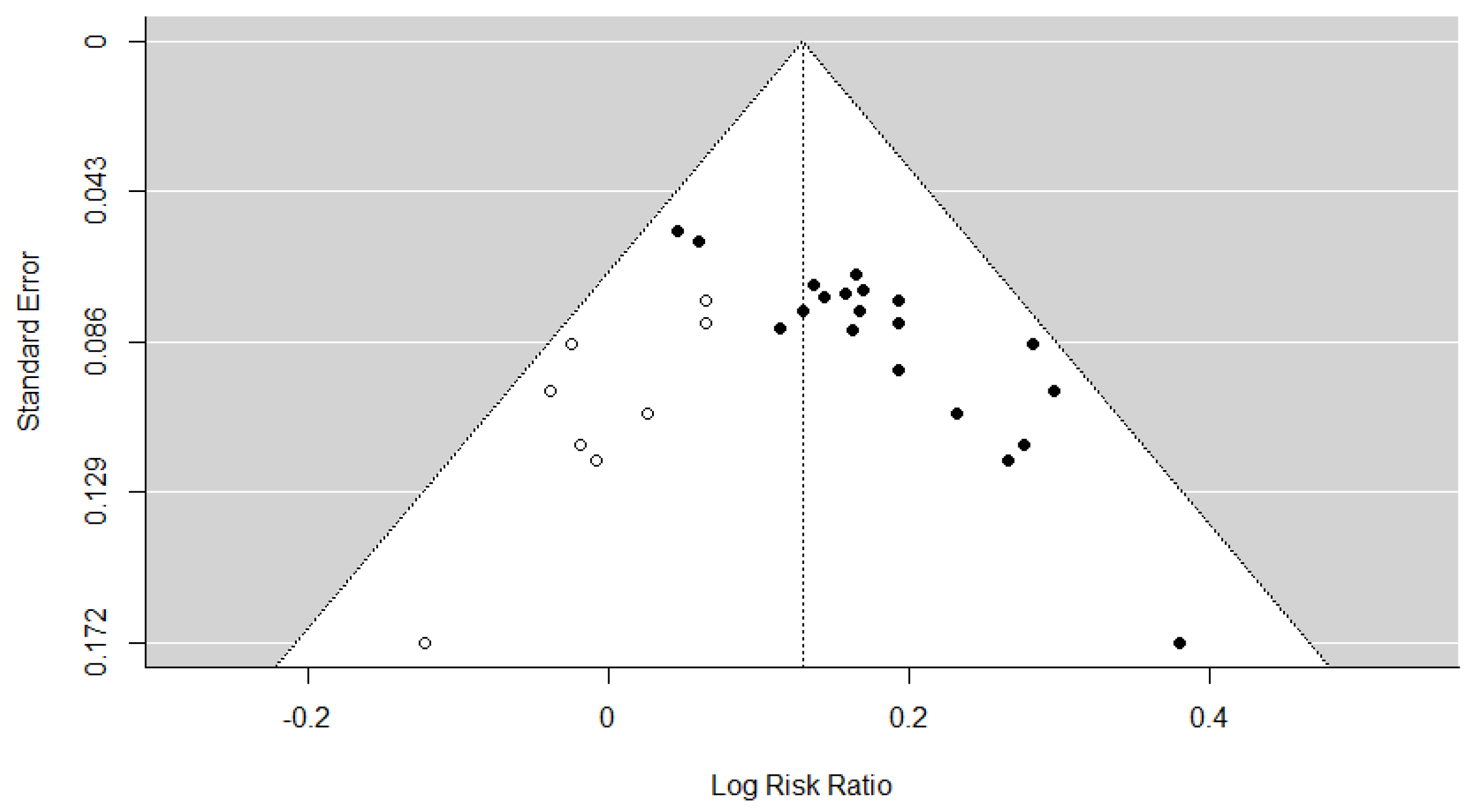
Publication bias for the TER was assessed. Publication bias was not assessed for other outcome measures owing to the inclusion of <10 studies. The assessment of publication bias revealed significant funnel plot asymmetry based on Egger’s regression test (t = 7.4624, p < 0.001; Figure 6), indicating the presence of potential small-study effects. The trim-and-fill method estimated that nine studies might be missing from the left side of the funnel plot (Figure 7), suggesting a possible overestimation of the intervention effect. After adjusting for these potentially missing studies, the pooled effect size was logRR = 0.1287 (95% CI: 0.0989–0.1584, p < 0.001), corresponding to an RR of 1.14 (95% CI: 1.10–1.17). Although slightly attenuated compared with the original estimate of RR = 1.17 (logRR = 0.1603), the result remained statistically significant. Furthermore, the Rosenthal fail-safe N was 786, far exceeding the commonly recommended minimum threshold of 120 (calculated as 5k + 10, where k = 22 is the number of included RCTs), indicating that 786 unpublished null-result studies would be required to negate the observed results. These findings suggest potential publication bias. However, the robustness of the conclusions was maintained.
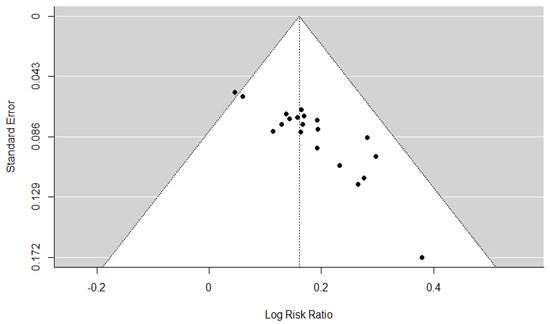
Figure 6.
Funnel plot of the total effective rate.
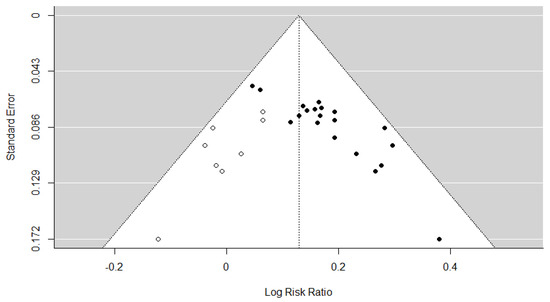
Figure 7.
Adjusted funnel plot (trim and fill) of the total effective rate. The closed dots represent real studies and the open dots represent filled artificial studies.
3.8. Subgroup and Sensitivity Analyses
Subgroup analysis based on specific HM formulations was performed in the meta-analysis. For TER, no additional subgroup analysis was conducted owing to the sufficient number of RCTs. Sensitivity analyses were not performed independently for other outcomes because <10 RCTs were included in each category (Table S6).
3.9. Quality Assessment
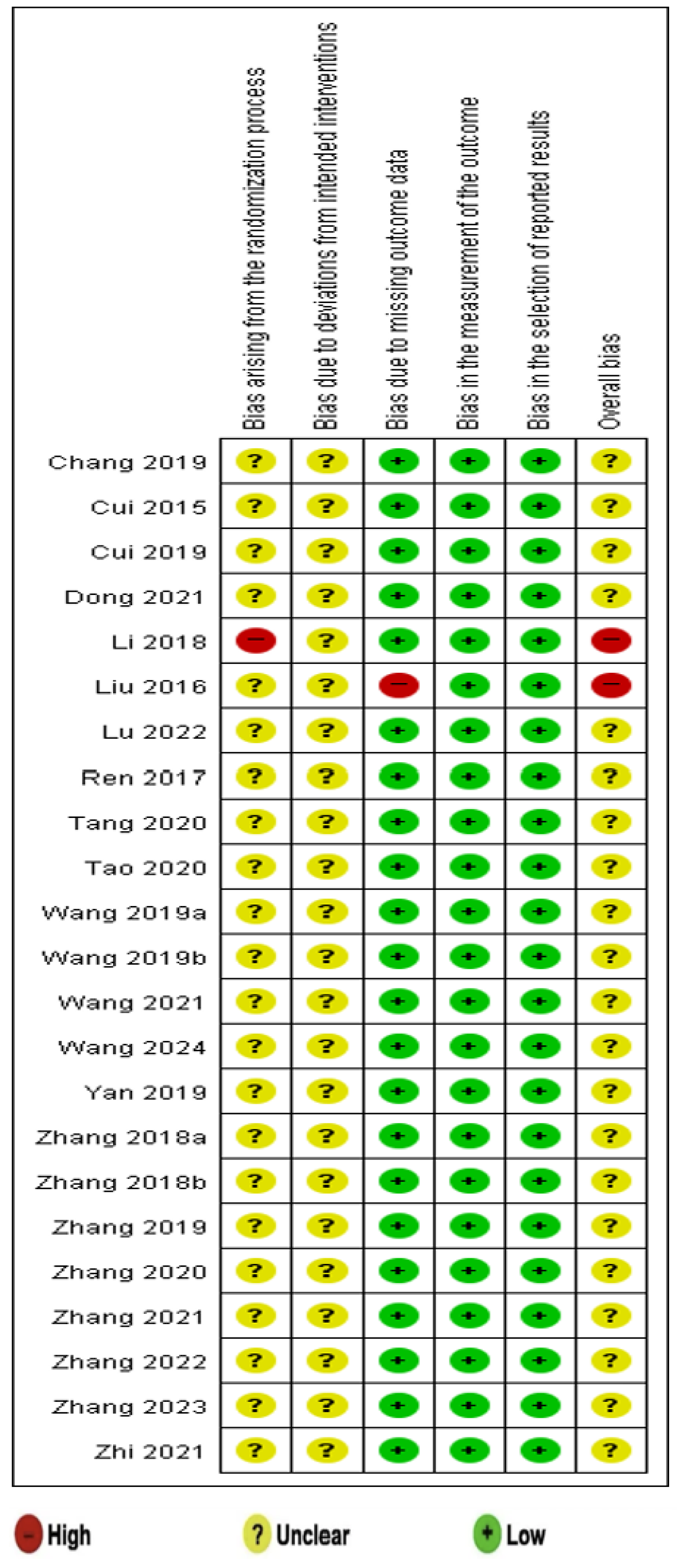
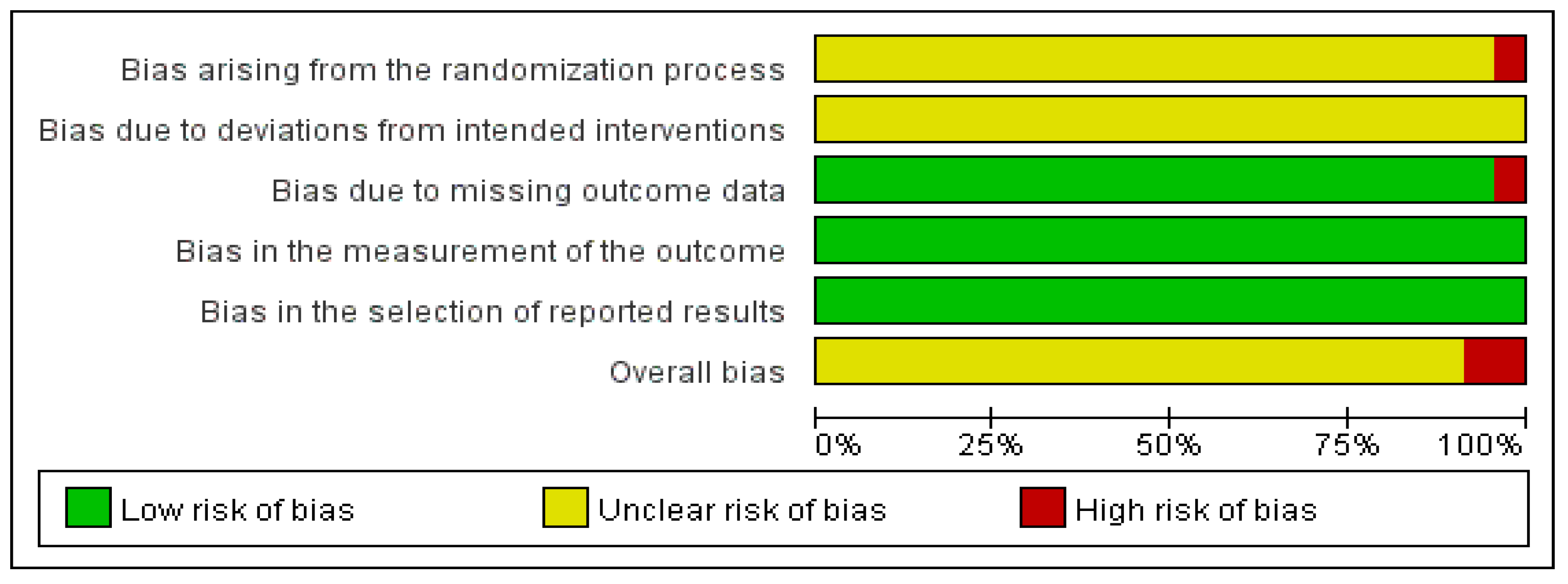
Except for one study [22], concerns regarding bias were raised in the randomization process of the included RCTs. Allocation sequence concealment was not reported in any RCTs, but no baseline imbalances were observed. However, in one study [22], insufficient information regarding the randomization process was reported.
All included studies had some concerns regarding deviations from intended interventions as a result of insufficient relevant information. Most studies were evaluated to have a low risk of bias in outcome measurements, with the exception of one study [23], where differences between the stated methodology and reported results led to a high risk.
Outcome measurements were evaluated using appropriate indicators, leading to a low risk in this category. In terms of the selection of reported results, all studies were rated as having a low risk.
With the exception of two studies [22,23] categorized as “high risk”, all other RCTs were rated as having “some concerns (unclear)” regarding bias. These findings are visualized in Figure 8 and Figure 9.

Figure 8.
Risk of bias assessment [18,19,20,21,22,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40].
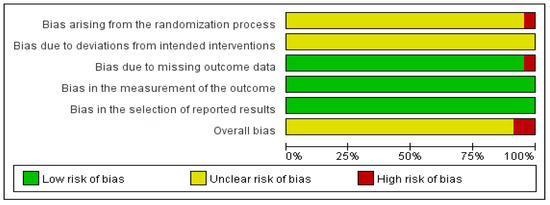
Figure 9.
Risk of bias graph.
3.10. GRADE Certainty of Evidence
The GRADE evidence profile is presented in Table 3. The TER (overall), disappearance time of main symptoms (spastic cough) (overall and DY subgroup), recovery time of routine blood parameters to normal range (overall), and hospitalization time (overall and SB subgroup) were rated as “moderate quality”. Owing to a high risk of bias and imprecision, other outcomes were rated as having a “low” or “very low” quality.
Table 3.
GRADE certainty of evidence.
4. Discussion
4.1. Summary of Findings
The findings of this study indicate that combining HM with WM provides greater therapeutic benefits than WM alone in pediatric PLS. Data from 23 RCTs conducted in China involving 1938 children were analyzed. Children with PLS in these RCTs were divided into the control group if they used WM and the experimental group if they used a combination of HM and WM, and they received the corresponding treatments for less than two weeks. However, a high heterogeneity for all outcomes, except for TER, was observed among the studies because they covered 12 different types of HMs. Accordingly, subgroup analyses were conducted based on specific HM types.
A meta-analysis revealed that HM significantly improved the TER and other clinical outcomes. In the included RCTs, the TER was assessed by reflecting the degree of improvement in spastic cough and the main symptoms of PLS, such as lung rhonchus sounds, wheezing and wet chirping, panting, and shortness of breath. This observation highlights the appropriateness of using TER as the main outcome measure for PLS, where the diagnosis was based on symptoms. These findings suggest that HM in combination with WM can help alleviate PLS symptoms. In particular, JW was effective in reducing the disappearance time of main symptoms, especially spastic cough. Additionally, HM accelerated the recovery of blood routine parameters, with DY showing the greatest efficacy, followed by SB. DY and SB were also more effective in shortening hospitalization time than WM alone.
Across all included studies, digestive symptoms such as nausea (or vomiting), abdominal pain, and diarrhea were the most reported adverse events. However, their occurrence was lower in patients who were treated with HM combined with WM than in patients treated with WM alone. All reported adverse events were mild and resolved without the need for additional treatment.
Regarding risk of bias, most RCTs had “some concerns”, and two RCTs were rated as having a “high” risk of bias. The main issues involved randomization procedures and deviations from intended interventions, with only one RCT having missing outcome data. Due to the lack of number of RCTs per outcome, publication bias could only be evaluated for TER.
This study is significant as it addresses the use of HM in treating PLS, a condition that has symptoms similar to pertussis in children and is often overlooked in clinical practice.
4.2. Clinical Implications
PLS closely resembles whooping cough, presenting with paroxysmal (spastic) cough, facial redness, and often a high-pitched inspiratory “whoop” sound [41]. As with whooping cough, PLS can manifest a variety of respiratory symptoms, with persistent spastic cough being a key diagnostic feature. In severe cases, prolonged coughing may lead to complications, such as vomiting, dehydration, apnea, cyanosis, convulsions, and death in young children [42,43]. Several studies have identified pathogens, such as adenovirus, Mycoplasma pneumoniae, and influenza B virus, as potential causes of PLS [44,45]. However, due to the wide range of possible causative pathogens, treatment generally focuses on symptomatic management rather than pathogen-specific therapy.
Macrolide antibiotics, including erythromycin and azithromycin, are commonly used to treat respiratory infections and are standard treatments for both whooping cough and PLS [46]. However, while antibiotics effectively eliminate pathogens, they do not significantly alleviate persistent clinical symptoms [12]. Moreover, these medications are associated with digestive adverse events, such as nausea (or vomiting), abdominal pain, and diarrhea, with erythromycin having a particularly high likelihood of causing such adverse effects [47]. Azithromycin and roxithromycin are next-generation antibiotics that cause fewer adverse digestive effects than those caused by erythromycin. They are prescribed to children; however, caution is warranted when prescribing these drugs at a high dosage [48,49]. Therefore, it is important to explore whether HM can improve symptoms without exacerbating the gastrointestinal adverse effects when used alongside WM, such as with antibiotics. In addition to antibiotics, WMs generally used to treat respiratory failure in children, such as asthma, were used to treat PLS symptoms in the included RCTs [50]. Ipratropium bromide (an anticholinergic drug), albuterol sulfate (a beta agonist), and montelukast (a leukotriene receptor antagonist) are bronchodilators that improve lung function, control symptoms, and reduce exacerbations of asthma [51]. Budesonide (a corticosteroid) acts as an anti-inflammatory agent and is often used in combination with bronchodilators to achieve maximum efficacy [52]. However, anticholinergic drugs and beta-agonists can cause increased heart rate, tremors, and palpitations [53]. Additionally, whether montelukast causes neuropsychiatric adverse events in children remains debatable [54]. In particular, inhaled corticosteroids are used for long-term symptoms, and there are concerns that they affect children’s growth, adrenal function, and bone density [55]. In this study, it was expected that HMs could play the role of WMs in alleviating symptoms.
This systematic review analyzed 12 types of oral HMs used to treat PLS. Among them, SB, WJ, and DY were evaluated in multiple studies. SB is traditionally administered for respiratory disorders induced by phlegm–heat obstruction and has demonstrated anti-influenza and anti-inflammatory effects [56]. Mori Cortex Radicis, a key ingredient of SB, has strong anti-inflammatory properties [57]. Additionally, it elevates the expression of regulatory T cells and represses Th2 cytokines in asthma and acts as an anti-allergic HM similar to the WMs used in the included RCTs [58]. Similarly, WJ is used to clear phlegm and heat from the lungs, improve lung function, and regulate arterial blood gases. It reportedly reduces the expression of inflammatory markers in respiratory disorders, such as chronic obstructive pulmonary disease (COPD) [59]. Its active compounds—beta-sitosterol, tricin, and stigmasterol—are reportedly beneficial for conditions such as pneumonia and COPD [60]. Folium Wrightiae Laevis, derived from the leaves of Alstonia scholaris (L.) R. Br., is traditionally used for treating lung fever, cough, and phlegm, and DY has been developed for managing respiratory disorders such as chronic bronchitis [61].
Glycyrrhizae Radix et Rhizoma, the most frequent ingredient in included RCTs (present in 16 prescriptions), has anti-inflammatory and antiviral properties and can enhance the efficacy of other herbs [62,63,64]. Particularly, triterpene saponin, the main chemical component, exhibits antimicrobial and antiviral activities against infectious respiratory diseases such as coronavirus, influenza, and COVID-19 [65]. The second most used herb, Armeniacae Semen, has been widely recognized for its benefits in treating lung diseases such as cough and asthma [66]. Notably, its active component, amygdalin, exhibits strong anti-inflammatory and antifibrotic properties [67]. Amygdalin also inhibits cell death and prevents cell damage in lung epithelial cells infected with bacteria [68]. Pinelliae Rhizoma is also a notable herb, and its components, chrysin, DHC, and 7,8-DHF, control the inflammatory response by suppressing the activity of the NLRP3 inflammasome due to acute infection of the lungs [69]. This study found that the HMs (herbs) used in RCTs could play a role similar to that of conventional WMs, without increasing gastrointestinal adverse events.
To support the effects of the above-mentioned HMs, this study analyzed whether the herbs were effective in improving major symptoms of PLS, such as spastic cough, reducing the time for routine blood parameters to recover to normal range, and shortening hospitalization time. The findings suggest that combining HM with WM is more effective in treating PLS symptoms in children than WM alone.
4.3. Limitations and Suggestions
This study has several limitations. First, although databases in four languages were searched without regional restrictions, all the included RCTs were performed in China. However, considering that HMs are widely used in East Asia, particularly China, this geographical concentration alone should not be interpreted as indicative of low methodological quality or substantial heterogeneity among studies. Additionally, if future studies included RCTs from other regions, they could provide a more comprehensive evaluation of the efficacy of HMs.
Second, most RCTs have challenges in blinding participants, leading to a potential risk of bias. Additionally, heterogeneity was observed, and the evidence quality ranged from moderate to very low, suggesting the need for well-designed studies with standardized methodologies.
Third, this study assessed publication bias only with respect to the TER. The funnel plot of TER revealed asymmetry, suggesting potential publication bias. Additional analysis revealed that these results did not affect the overall conclusion. However, it was difficult to assess publication bias for other outcomes that were based on less than 10 RCTs because of insufficient data and diversity among HMs used. These factors contributed to the high heterogeneity in the results of other outcomes. When designing future RCTs on PLS, it is necessary to select consistent outcome indicators for comparison. Additionally, if sufficient RCTs are available, a meta-analysis can be conducted to determine the effectiveness of a specific type of HM in pediatric patients with PLS.
Fourth, inflammatory markers, such as C-reactive protein, interleukins, and immunoglobulins, are important indicators of treatment efficacy. However, non-uniform measurement methods across studies prevented any direct comparisons. Future studies incorporating these biomarkers would provide more objective and reliable evidence.
Finally, only one included study [27] reported the recurrence rate of PLS. Because PLS can recur due to various pathogens, future studies should use recurrence rates as an indicator of the long-term efficacy of HM in managing PLS.
In conclusion, this study statistically showed that a combination of HM and WM is more effective than treatment with WM alone in children with PLS. However, high-quality, well-designed RCTs of PLS need to be conducted globally.
5. Conclusions
This study showed that HM combined with WM is more effective than WM alone for managing PLS in children, and the combination does not lead to serious adverse events. However, the quality of evidence was not high, highlighting the need for well-designed, high-quality RCTs in the future. Additionally, owing to the inconsistency in the types of HMs used, further studies focusing on specific HM formulations are necessary. Despite these limitations, our findings provide valuable insights for clinicians, particularly when managing PLS in children who do not meet the diagnostic criteria for whooping cough.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/healthcare13101131/s1, Table S1: PRISMA 2020 checklist; Table S2: Search strategy for each database; Table S3: Frequency of herb; Table S4: Conventional and basic treatments; Table S5: Outcome measurement and result (p-value); Table S6: Sensitivity analysis of TER.
Author Contributions
Conceptualization and design: J.-U.C., Y.-S.S., E.-J.K. and S.Y.M.; data curation and formal analysis: J.-U.C., Y.-S.S. and E.-J.K.; investigation: J.-U.C., Y.-S.S., E.-J.K. and S.Y.M.; methodology: J.-U.C., Y.-S.S. and E.-J.K.; project administration and supervision: S.Y.M.; visualization: J.-U.C. and Y.-S.S.; writing—original draft: J.-U.C. and Y.-S.S.; writing—review and editing: J.-U.C., Y.-S.S., E.-J.K. and S.Y.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data analyzed in this study are included in this published article and Supplementary Materials.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CI | confidence interval |
| DY | Dengtai ye granule |
| GRADE | Grading of Recommendations Assessment, Development, and Evaluation |
| HM | herbal medicine |
| MD | mean difference |
| PLS | pertussis-like syndrome |
| RCTs | randomized clinical trials |
| ROB | risk of bias |
| RR | risk ratio |
| SB | Sangbaipi decoction |
| SMD | standardized mean difference |
| TER | total effective rate |
| WJ | Weijing decoction |
| WM | Western medicine |
References
- Nguyen, V.T.N.; Simon, L. Pertussis: The whooping cough. Prim. Care 2018, 45, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Kline, J.M.; Smith, E.A.; Zavala, A. Pertussis: Common questions and answers. Am. Fam. Physician 2021, 104, 186–192. [Google Scholar] [PubMed]
- World Health Organization. Pertussis Reported Cases and Incidence. Available online: https://immunizationdata.who.int/global/wiise-detail-page/pertussis-reported-cases-and-incidence (accessed on 24 April 2025).
- Centers for Disease Control and Prevention (CDC). Pertussis Surveillance and Trends. Available online: https://www.cdc.gov/pertussis/php/surveillance/index.html (accessed on 24 April 2025).
- Dportal of Korea Disease Control and Prevention Agency (KDCA). Infectious Disease Reporting. Available online: https://dportal.kdca.go.kr/pot/is/summaryEDW.do (accessed on 24 April 2025).
- National Disease Control and Prevention Administration (NDCPA). Epidemic Information. Available online: https://www.ndcpa.gov.cn/jbkzzx/c100016/second/list.html (accessed on 24 April 2025).
- Gu, W.; Wang, K.; Zhang, X.; Hao, C.; Lu, Y.; Wu, M.; Chen, S.; He, Y.; Xu, J.; Shao, X.; et al. Pathogen analysis of pertussis-like syndrome in children. BMC Infect. Dis. 2020, 20, 353. [Google Scholar] [CrossRef]
- Hu, Y.; Shi, W.; Meng, Q.; Yuan, L.; Gao, W.; Wang, L.; Yao, K. Detection of Bordetella spp. in children with pertussis-like illness from 2018 to 2024 in China. J. Infect. 2024, 89, 106222. [Google Scholar] [CrossRef]
- Saiki-Macedo, S.; Valverde-Ezeta, J.; Cornejo-Tapia, A.; Castillo, M.E.; Petrozzi-Helasvuo, V.; Aguilar-Luis, M.A.; Del Valle, L.J.; Cieza-Mora, E.; Bada, C.; Del Aguila, O.; et al. Identification of viral and bacterial etiologic agents of the pertussis-like syndrome in children under 5 years old hospitalized. BMC Infect. Dis. 2019, 19, 75. [Google Scholar] [CrossRef] [PubMed]
- Langley, J.M.; Halperin, S.A.; Boucher, F.D.; Smith, B. Pediatric Investigators Collaborative Network on Infections in Canada (PICNIC). Azithromycin is as effective as and better tolerated than erythromycin estolate for the treatment of pertussis. Pediatrics 2004, 114, e96–e101. [Google Scholar] [CrossRef]
- Kanoh, S.; Rubin, B.K. Mechanisms of action and clinical application of macrolides as immunomodulatory medications. Clin. Microbiol. Rev. 2010, 23, 590–615. [Google Scholar] [CrossRef]
- Altunaiji, S.; Kukuruzovic, R.; Curtis, N.; Massie, J. Antibiotics for whooping cough (pertussis). Cochrane Database Syst. Rev. 2007, 3, CD004404. [Google Scholar] [CrossRef]
- Shergis, J.L.; Wu, L.; Zhang, A.L.; Guo, X.; Lu, C.; Xue, C.C. Herbal medicine for adults with asthma: A systematic review. J. Asthma 2016, 53, 650–659. [Google Scholar] [CrossRef]
- Lee, B.; Kwon, C.Y.; Suh, H.W.; Kim, Y.J.; Kim, K.I.; Lee, B.J.; Lee, J.H. Herbal medicine for the treatment of chronic cough: A systematic review and meta-analysis. Front. Pharmacol. 2023, 14, 1230604. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Rennie, D.; Meade, M.; Cook, D. Users’ Guides to the Medical Literature: Essentials of Evidence Based Clinical Practice, 3rd ed.; McGraw-Hill Education: New York, NY, USA, 2015. [Google Scholar]
- National Heart, Lung, and Blood Institute (NHLBI). Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 1 January 2025).
- Mai, Y.C.; Lin, Q. Analysis of the curative effect of modified Sangbaipi decoction on pertussis-like syndrome in children. Chin. Pediatr. Integr. Tradit. West Med. 2021, 4, 362–365. [Google Scholar]
- Cui, J.; Wang, X.X. Clinical observation of modified Sangbai Pi decoction in treating pediatric pertussis syndrome in 29 cases. Chin. J. Ethnomed. Ethnopharm. 2015, 24, 98–99. [Google Scholar]
- Cui, Y.C. Clinical analysis of the effectiveness of Sangbai Pi decoction in treating pediatric pertussis syndrome. Pract. Clin. J. Integr. Tradit. Chin. West Med. 2019, 19, 97–98. [Google Scholar]
- Dong, C.H. Exploring the clinical efficacy of modified Sangbai Pi decoction in treating pediatric pertussis syndrome. Diabetes World 2021, 18, 32. [Google Scholar]
- Li, Q.Q.; Ge, G.L.; Han, X. Clinical observation of Xiao Chai Hu decoction combined with Xie Bai San in treating pediatric pertussis syndrome. Guangming J. Chin. Med. 2018, 20, 3027–3028. [Google Scholar]
- Liu, Y.H.; Xiang, H.J.; Fan, S.H. 25 cases of pediatric pertussis syndrome treated with a combination of Gan Yu Dun cough formulas and conventional Western medicine. Tradit. Chin. Med. Res. 2016, 29, 22–24. [Google Scholar]
- Lu, F.; Li, A.M.; Xu, S.S. The efficacy of modified reed stem decoction combined with Western medicine in treating whooping cough syndrome in children and its impact on moisture respiration lung function. Sichuan Tradit. Chin. Med. 2022, 40, 79–82. [Google Scholar]
- Ren, R.Y. Clinical experience with modified Sangbai Pi decoction in treating patients with pertussis-cough stage pertussis. Women’s Health Res 2017, 10, 52–53. [Google Scholar]
- Tang, Q.Q.; Li, L.F.; Guan, L.F.; Guan, M.C.; Hang, J.G. Observation of the effectiveness of Lvguo pills in auxiliary treatment for pediatric pertussis syndrome. Chin. J. Rural. Med. Pharm. 2020, 17, 17–18. [Google Scholar]
- Tao, M.M. Observation of clinical efficacy in treating whooping cough syndrome (phlegm-heat gel block syndrome). Anhui Univ. Tradit. Chin. Med. 2020, 10369, 1–57. [Google Scholar]
- Wang, X.S. Clinical observation of combined traditional Chinese and Western medicine in treating whooping cough syndrome. Pract. J. Tradit. Chin. Med. 2019, 35, 1090–1091. [Google Scholar]
- Wang, S.Y. Observation of the effectiveness of a self-drafted cough suppression and phlegm transformation formula in whoop ing cough syndrome. Guangxi Tradit. Chin. Med. 2019, 42, 15–17. [Google Scholar]
- Wang, F.; Jin, X.H.; Zhang, Y.H. Clinical observation of lampshade leaf granules combined with cycloerythromycin in treating pediatric pertussis syndrome. Pract. J. Tradit. Chin. Med. 2021, 37, 227–228. [Google Scholar]
- Wang, H.; Zhang, T.T.; Duan, C.C.; Zhen, L.; Zhang, Z.P. Clinical study of Baikening granules combined with budesonide in treatment of pertussis syndrome in children. Drugs Clin. 2024, 39, 382–386. [Google Scholar]
- Yan, W.; Song, J.P.; Zhao, C.J. Clinical observation on 46 cases of pediatric pertussis syndrome with stage of spasmodic cough treated by modified Weijing Tang combined with erythromycin. J. Pediatr. Tradit. Chin. Med. 2019, 15, 52–55. [Google Scholar]
- Zhang, X.F. Analysis of the clinical characteristics and treatment of children with whooping cough syndrome. China Contin. Med. Educ. 2018, 10, 91–93. [Google Scholar]
- Zhang, B.F. Clinical observation of 60 cases of pertussis syndrome in children treated with mulberry pica. Contemp. Med. 2018, 24, 25–27. [Google Scholar]
- Zhang, X.F.; Jin, X.H.; Lu, F.X.; Li, H.J.; Zhang, Z.Y.; Feng, Y.; Deng, P.P.; Gao, X.H.; Yang, J.L. 70 children with pertussis treated with lampstand leaf granules in combination with Western medicine. Res. Integr. Tradit. Chin. West. Med. 2019, 4, 213–214. [Google Scholar]
- Zhang, Z.Y.; Jin, X.H.; Zhang, X.N.; Zhang, X.F. Clinical study of Dengtaiye Granules combined with cycloester erythromycin in treatment of pertussis-like syndrome. Drugs Clin. 2020, 12, 2365–2369. [Google Scholar]
- Zhang, X.F.; Lu, F.X.; Li, H.J.; Zhang, Z.Y.; Deng, P.P.; Gao, X.H.; Jin, X.H. Clinical study on treatment of pertussis-like synd rome with Dengtaiye Granules. Res. Integr. Tradit. Chin. West. Med. 2021, 1, 8–10. [Google Scholar]
- Zhang, H.G.; Zhu, S.; Zhu, Z.P.; Wang, X.L.; Tian, X.L.; Zhao, W.J. Effects of Jiawei Weijing Decoction on tidal breathing lung function and inflammatory factors in child patients with pertussis syndrome. Pharmacol. Clin. Chin. Mater. Med. 2022, 2, 199–202. [Google Scholar]
- Zhang, X.F.; Yu, Y.J.; Zhang, X.N. Effect of Xiao’er Feike Granules combined with erythromycin cyclocarbonate on pulmonary function status and cellular immunity in children with pertussis-like syndrome. Chin. Foreign Med. Res. 2023, 9, 1–4. [Google Scholar]
- Zhi, Y.L. Clinical observation on Dengtaiye Granule combined with Western medicine in the treatment of 60 children with pertussis-like syndrome. Chin. J. Ethnomed. Ethnopharm. 2021, 7, 91–93. [Google Scholar]
- Liu, Y.; Ai, T.; Fan, Y.; Xie, C.; Lou, R.; Zeng, X.; Wang, L.; Peng, Y.; Chen, M. Etiological distribution of pertussis-like syndro me in 756 children in Chengdu. Transl. Pediatr. 2021, 10, 984–989. [Google Scholar] [CrossRef]
- Wang, K.; Bettiol, S.; Thompson, M.J.; Roberts, N.W.; Perera, R.; Heneghan, C.J.; Harnden, A. Symptomatic treatment of the cough in whooping cough. Cochrane Database Syst. Rev. 2014, 9, CD003257. [Google Scholar] [CrossRef] [PubMed]
- Mattoo, S.; Cherry, J.D. Molecular pathogenesis, epidemiology, and clinical manifestations of respiratory infections due to Bordetella pertussis and other Bordetella subspecies. Clin. Microbiol. Rev. 2005, 18, 326–382. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, A.; Calicó, I.; Manresa, J.M.; Andreu, A.; Moraga, F.; Valle, I. Microorganisms isolated in cases of pertussis-like synd rome. Enferm. Infecc. Microbiol. Clin. 2000, 18, 433–438. [Google Scholar]
- Mahmoudi, S.; Banar, M.; Pourakbari, B.; Alavi, H.S.; Eshaghi, H.; Ahari, A.A.; Mamishi, S. Identification of etiologic agents of the pertussis-like syndrome in children by real-time PCR method. Prague Med. Rep. 2018, 119, 61–69. [Google Scholar] [CrossRef]
- Amsden, G.W. Erythromycin, clarithromycin, and azithromycin: Are the differences real? Clin. Ther. 1996, 18, 56–72. [Google Scholar] [CrossRef]
- Carter, B.L.; Woodhead, J.C.; Cole, K.J.; Milavetz, G. Gastrointestinal side effects with erythromycin preparations. Drug Intell. Clin. Pharm. 1987, 21, 734–738. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Wang, Y. Safety of azithromycin in pediatric infectious diseases: A clinical systematic review and meta-analysis. Transl. Pediatr. 2021, 10, 2594–2601. [Google Scholar] [CrossRef]
- Hansen, M.P.; Scott, A.M.; McCullough, A.; Thorning, S.; Aronson, J.K.; Beller, E.M.; Glasziou, P.P.; Hoffmann, T.C.; Clark, J.; Del Mar, C.B. Adverse events in people taking macrolide antibiotics versus placebo for any indication. Cochrane Database Syst. Rev. 2019, 1, CD011825. [Google Scholar] [CrossRef]
- Hon, K.L.E.; Leung, A.K.C. Medications and Recent Patents for Status Asthmaticus in Children. Recent. Pat. Inflamm. Allergy Drug Discov. 2017, 11, 12–21. [Google Scholar] [PubMed]
- Aryani, T.; Rahmawat, R.K.; Cintyadewi, N.P.; Puspitasari, A.D.; Rasyid, A.N.; Samirah. Patterns of bronchodilator therapy in asthmatic outpatients. J. Public. Health Afr. 2023, 14, 2533. [Google Scholar] [CrossRef]
- Koziol-White, C.; Johnstone, T.B.; Corpuz, M.L.; Cao, G.; Orfanos, S.; Parikh, V.; Deeney, B.; Tliba, O.; Ostrom, R.S.; Dainty, I.; et al. Budesonide enhances agonist-induced bronchodilation in human small airways by increasing cAMP production in airway smooth muscle. Am. J. Physiol. Lung Cell. Mol. Physiol. 2020, 318, L345–L355. [Google Scholar] [CrossRef]
- Akhtar, A.; Abbas, S.A.; Zaidi, S.H.M.; Sohail, A.; Alam, M.I.; Raza, L. The Acute Effects of the Use of Salbutamol and Ipratropium on the Heart Rates of Patients With Obstructive Airway Disease. Cureus 2023, 15, e46409. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, M.; Seo, M.S.; Shin, J.Y. Risk of neuropsychiatric adverse events associated with montelukast use in children and adolescents: A population-based case-crossover study. BMJ Paediatr. Open 2024, 8, e002483. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.B. Effects of inhaled steroids on growth, bone metabolism, and adrenal function. Adv. Pediatr. 2006, 53, 101–110. [Google Scholar] [CrossRef]
- Shi, T.; Lin, J.; Liang, S.; Song, Y.; Zhao, X.; Xiao, M.; Ti, H. Sangbaipi decoction exerted in vitro and in vivo anti-influenza effect through inhibiting viral proteins. J. Ethnopharmacol. 2024, 331, 118258. [Google Scholar] [CrossRef]
- Seo, C.S.; Lim, H.S.; Jeong, S.J.; Ha, H.; Shin, H.K. HPLC-PDA analysis and anti-inflammatory effects of Mori Cortex Radicis. Nat. Prod. Commun. 2013, 8, 1443–1446. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, H.J.; Jeong, S.J.; Lee, H.J.; Kim, S.H.; Park, E.J. Cortex Mori Radicis extract exerts antiasthmatic effects via enhancement of CD4+CD25+Foxp3+ regulatory T cells and inhibition of Th2 cytokines in a mouse asthma model. J. Ethnopharmacol. 2011, 138, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Shergis, J.; Chen, X.; Yu, X.; Guo, X.; Zhang, A.L.; Lu, C.; Xue, C.C. Chinese herbal medicine (Weijing Decoction) combined with pharmacotherapy for the treatment of acute exacerbations of chronic obstructive pulmonary disease. Evid. Based Complement. Alternat Med. 2014, 2014, 257012. [Google Scholar] [CrossRef] [PubMed]
- Li, J.X.; Han, Z.X.; Cheng, X.; Zhang, F.L.; Zhang, J.Y.; Su, Z.J.; Li, B.P.; Jiang, Z.R.; Li, R.Z.; Xie, Y.; et al. Combinational study with network pharmacology, molecular docking, and preliminary experiments on exploring common mechanisms underlying the effects of Weijing Decoction on various pulmonary diseases. Heliyon 2023, 9, e15631. [Google Scholar] [CrossRef]
- Rao, K.S.; Sun, Y.; Hui, T.T.; Gong, Y.Q.; Zhu, L.P.; Guo, W. Research on the HPLC method for determining alkaline content induck feet leaf granules. J. Yunnan Univ. Tradit. Chin. Med. 2008, 3, 9–12. [Google Scholar]
- Yang, R.; Yuan, B.C.; Ma, Y.S.; Zhou, S.; Liu, Y. The anti-inflammatory activity of licorice, a widely used Chinese herb. Pharm. Biol. 2016, 55, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yang, R.; Yuan, B.; Liu, Y.; Liu, C. The antiviral and antimicrobial activities of licorice, a widely used Chinese herb. Acta Pharm. Sin. B 2015, 5, 310–315. [Google Scholar] [CrossRef]
- Zhao, F.Q.; Wang, G.F.; Xu, D.; Zhang, H.Y.; Cui, Y.L.; Wang, Q.S. Glycyrrhizin-mediated liver-targeted alginate nanogels delivers quercetin to relieve acute liver failure. Int. J. Biol. Macromol. 2021, 168, 93–104. [Google Scholar] [CrossRef]
- Li, F.; Liu, B.; Li, T.; Wu, Q.; Xu, Z.; Gu, Y.; Li, W.; Wang, P.; Ma, T.; Lei, H. Review of Constituents and Biological Activities of Triterpene Saponins from Glycyrrhizae radix et Rhizoma and Its Solubilization Characteristics. Molecules 2020, 25, 3904. [Google Scholar] [CrossRef]
- Wei, Y.; Li, Y.; Wang, S.; Xiang, Z.; Li, X.; Wang, Q.; Dong, W.; Gao, P.; Dai, L. Phytochemistry and pharmacology of Armeniacae semen Amarum: A review. J. Ethnopharmacol. 2023, 8, 116265. [Google Scholar] [CrossRef]
- Wang, Y.; Gu, W.; Kui, F.; Gao, F.; Niu, Y.; Li, W.; Zhang, Y.; Guo, Z.; Du, G. The mechanism and active compounds of Semen Armeniacae Amarum treating coronavirus disease 2019 based on network pharmacology and molecular docking. Food Nutr. Res. 2021, 65, 5623. [Google Scholar] [CrossRef] [PubMed]
- Si, Z.; Zhang, B. Amygdalin Attenuates Airway Epithelium Apoptosis, Inflammation, and Epithelial-Mesenchymal Transition through Restraining the TLR4/NF-κB Signaling Pathway on LPS-Treated BEAS-2B Bronchial Epithelial Cells. Int. Arch. Allergy Immunol. 2021, 182, 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.N.; Zhang, X.X.; Shen, P.; Huang, C.S.; Deng, H.F.; Zhou, L.; Yue, L.X.; Shen, B.Y.; Zhou, W.; Gao, Y. Pinelliae rhizoma alleviated acute lung injury induced by lipopolysaccharide via suppressing endoplasmic reticulum stress-mediated NLRP3 inflammasome. Front. Pharmacol. 2022, 13, 883865. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).