

Psychological Factors Influencing Attitudes towards Euthanasia, Assisted Suicide and Palliative Care among Medical Students and Doctors in Training
 , , ,
, , ,
Abstract
1. Introduction
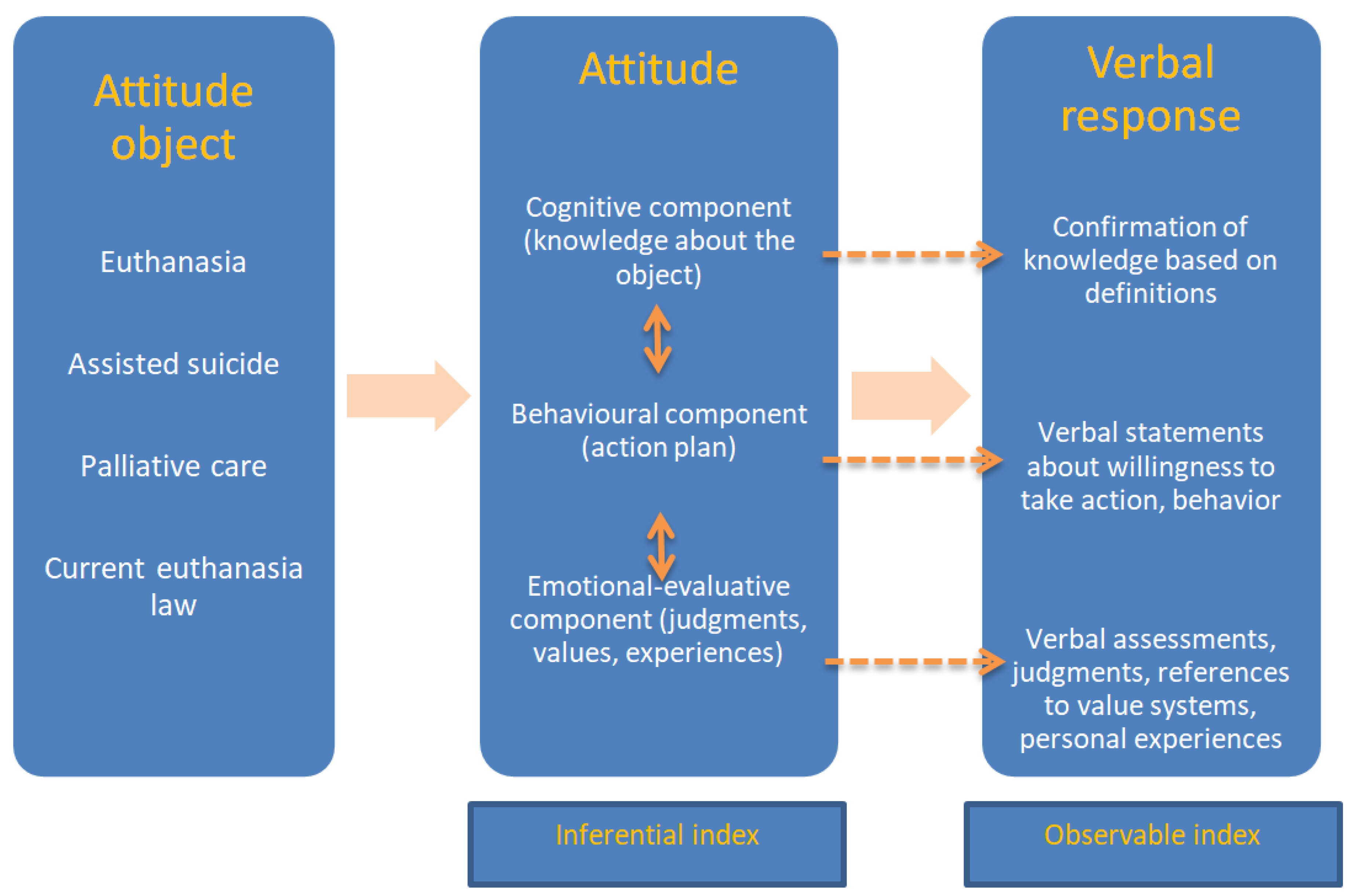
- Does more knowledge about the object of attitude (euthanasia, assisted suicide and palliative care) impact these attitudes?
- Does the perspective of potentially deciding about euthanasia or potentially committing euthanasia or assisted suicide impact these attitudes?
- Do experience of own disease or disease of a close person or value system have an impact on these attitudes?
2. Material and Methods
3. Results
3.1. Attitudes towards Euthanasia and Assisted Suicide and Palliative Care and Sociodemographic Differences
3.2. Cognitive Component: Respondents’ Knowledge of Attitude Objects
3.3. Behavioural Component: Readiness to Euthanise
3.4. Behavioural Component: Willingness to Undergo Euthanasia in Case of One’s Own Illness
3.5. Emotional Component: Experiences, Values and Judgements Influencing Attitudes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Materstvedt, L.J.; Clark, D.; Ellershaw, J.; Førde, R.; Gravgaard, A.-M.B.; Mu, H.C.; Sales, J.P.I.; Rapin, C.-H. EAPC Ethics Task Force. Euthanasia and physician-assisted suicide: A view from an EAPC Ethics Task Force. Palliat. Med. 2003, 17, 97–101; discussion 102–179. [Google Scholar] [CrossRef]
- Radbruch, L.; Leget, C.; Bahr, P.; Müller-Busch, C.; Ellershaw, J.; de Conno, F.; Vanden Berghe, P.; Board Members of EAPC. Euthanasia and physician-assisted suicide: A white paper from the European Association for Palliative Care. Palliat. Med. 2016, 30, 104–116. [Google Scholar] [CrossRef]
- Ustawa z dnia 6 czerwca 1997 r., Kodeks karny (Dz.U. z 2016 r., poz. 2138). (Polish Criminal Proceeding Code). Available online: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU19970880553/O/D19970553.pdf (accessed on 23 March 2024).
- De Lima, L.; Woodruff, R.; Pettus, K.; Downing, J.; Buitrago, R.; Munyoro, E.; Venkateswaran, C.; Bhatnagar, S.; Radbruch, L. International Association for Hospice and Palliative Care Position Statement: Euthanasia and Physician-Assisted Suicide. J. Palliat. Med. 2017, 20, 8–14. [Google Scholar] [CrossRef]
- Van den Berg, V.; van Thiel, G.; Zomers, M.; Hartog, I.; Leget, C.; Sachs, A.; Uiterwaal, C.; van Wijngaarden, E. Euthanasia and Physician–Assisted Suicide in Patients with Multiple Geriatric Syndromes. JAMA Intern. Med. 2021, 181, 245–250. [Google Scholar] [CrossRef]
- Grassi, L.; Folesani, F.; Marella, M.; Tiberto, E.; Riba, M.B.; Bortolotti, L.; Toffanin, T.; Palagini, L.; Murri, M.B.; Biancosino, B.; et al. Debating Euthanasia and Physician-Assisted Death in People with Psychiatric Disorders. Curr. Psychiatry Rep. 2022, 24, 325–335. [Google Scholar] [CrossRef]
- Aries, P. Man and Death; Państwowy Instytut Wydawniczy: Warszawa, Poland, 1989. [Google Scholar]
- Giddens, A. Modernity and self–identity. In Self and Society in the Late Modern Age; Polity Press: Cambridge, UK, 2008. [Google Scholar]
- Emanuel, E.J. Attitudes and desires related to euthanasia and physician–assisted suicide among terminally ill patients and their caregivers. JAMA 2000, 284, 2460–2468. [Google Scholar] [CrossRef]
- Morita, T.S. Desire for death and requests to hasten death of Japanese terminally ill cancer patients receiving specialized inpatient palliative care. J. Pain. Symptom Manag. 2004, 27, 44–52. [Google Scholar] [CrossRef]
- Gutierrez-Castillo, A.; Gutierrez-Castillo, J.; Guadarrama-Conzuelo, F.; Jimenez-Ruiz, A.; Ruiz-Sandoval, J.L. Euthanasia and physician-assisted suicide: A systematic review of medical students’ attitudes in the last 10 years. J. Med. Ethic-Hist. Med. 2020, 13, 22. [Google Scholar] [CrossRef]
- Schioldborg, P. Studenters holdninger til aktiv dødshjelp, assistert suicid og foreslått lovendring [Students’ attitudes toward active euthanasia, assisted suicide and proposed amendments to the penal code]. Tidsskr. Nor. Laegeforen 2000, 120, 2283–2288. [Google Scholar]
- Ramírez-Rivera, J.; Cruz, J.; Jaume-Anselmi, F. Euthanasia, assisted suicide and end-of-life care: Attitudes of students, residents and attending physicians. P. R. Health Sci. J. 2006, 25, 325–329. [Google Scholar]
- Kontaxakis, V.; Paplos, K.G.; Havaki-Kontaxaki, B.J.; Ferentinos, P.; Kontaxaki, M.-I.V.; Kollias, C.T.; Lykouras, E. Attitudes on euthanasia and physician-assisted suicide among medical students in Athens. Psychiatriki 2009, 20, 305–311. [Google Scholar] [PubMed]
- Lau, A.M.; Wong, E.L. Attitude towards Euthanasia among Medical Students: A Cross-Sectional Study in Hong Kong. Int. J. Environ. Res. Public Health 2022, 19, 7697. [Google Scholar] [CrossRef] [PubMed]
- Anneser, J.; Jox, R.J.; Thurn, T.; Borasio, G.D. Physician-assisted suicide, euthanasia and palliative sedation: Attitudes and knowledge of medical students. GMS J. Med. Educ. 2016, 33, Doc11. [Google Scholar] [PubMed]
- Roelands, M.; Van den Block, L.; Geurts, S.; Deliens, L.; Cohen, J. Attitudes of belgian students of medicine, philosophy, and law toward euthanasia and the conditions for its acceptance. Death Stud. 2015, 39, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Bator, E.X.; Philpott, B.; Costa, A.P. This moral coil: A cross-sectional survey of Canadian medical student attitudes toward medical assistance in dying. BMC Med. Ethics 2017, 18, 58. [Google Scholar] [CrossRef]
- Pomfret, S.; Mufti, S.; Seale, C. Medical students and end-of-life decisions: The influence of religion. Future Healthc. J. 2018, 5, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Gruber, P.C.; Gomersall, C.D.; Joynt, G.M.; Lee, A.; Tang, P.Y.; Young, A.S.; Yu, N.Y.; Yu, O.T. Changes in medical students’ attitudes towards end-of-life decisions across different years of medical training. J. Gen. Intern. Med. 2008, 23, 1608–1614. [Google Scholar] [CrossRef] [PubMed]
- Akbayram, H.T. Medical Faculty Students’ Views on Euthanasia: Does It Change With Medical Education? Alpha Psychiatry 2021, 22, 113–117. [Google Scholar] [CrossRef]
- Grassi, L.; Agostini, M.; Rossin, P.; Magnani, K. Medical Students’ opinions of euthanasia and physician-assisted suicide in Italy. Arch. Intern. Med. 2000, 160, 2226–2227. [Google Scholar] [CrossRef]
- Forycka, M.; Leppert, W.; Majkowicz, M. Attitudes toward euthanasia among medical students from different countries. Oncol. Clin. Pract. 2022, 18, 275–283. [Google Scholar] [CrossRef]
- Leppert, W.; Gottwald, L.; Majkowicz, M.; Kazmierczak-Lukaszewicz, S.; Forycka, M.; Cialkowska-Rysz, A.; Kotlinska-Lemieszek, A. A comparison of attitudes toward euthanasia among medical students at two Polish universities. J. Cancer Educ. 2013, 28, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Stokłosa, I.; Stokłosa, M.; Więckiewicz, G.; Porwolik, M.; Bugajski, M.; Masarczyk, W.; Męcik-Kronenberg, T.; Piegza, M.; Pudlo, R.; Gorczyca, P. Analysis of Factors Influencing Polish Students’ Opinions on Euthanasia. Int. J. Environ. Res. Public Health 2022, 19, 5019. [Google Scholar] [CrossRef] [PubMed]
- Wojciszke, B. Social Psychology; Scholar: Warszawa, Poland, 2022. [Google Scholar]
- Bohner, G.W.; Wänke, M. Attitudes and Attitude Change; Gdańskie Wydawnictwo Psychologiczne: Gdańsk, Poland, 2004. [Google Scholar]
- Aizen, I. The theory of planned behavior: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar]
- Mordy, M. Theoretical Meaning and Empirical Meaning of the Concept of Attitude; PWN: Warszawa, Poland, 1976. [Google Scholar]
- Breckler, S.J. Empirical validation of affect, behavior, and cognition as distinct components of attitude. J. Pers. Soc. Psychol. 1984, 47, 1191–1205. [Google Scholar] [CrossRef] [PubMed]
- Vishal, J. 3D model of attitude. Intern. J. Adv. Manag. Soc. Sci. 2014, 3, 1–12. [Google Scholar]
- Aronson, E.; Wilson, T.; Alert, R. Social Psychology: Heart and Mind; Zysk i Spółka: Poznań, Poland, 2012. [Google Scholar]
- Oppenheim, A. Questionnaires, Interviews, Measurements of Attitudes; Zysk i Spółka: Poznań, Poland, 2004. [Google Scholar]
- Hassan, W.; Ahmad, F.; Malik, A.; Ali, S. Knowledge and attitude regarding euthanasia among medical students in the public and private medical schools of Karachi. J. Pak. Med. Assoc. 2013, 63, 295–299. [Google Scholar] [PubMed]
- ProCon.org. Euthanasia & Medical Aid in Dying (MAID) around the World. Last Modified on 7 July 2022. Available online: https://euthanasia.procon.org/euthanasia-physician-assisted-suicide-pas-around-the-world/ (accessed on 23 March 2024).
- Le Coz, P. Fin de vie: Il faut distinguer euthanasie et suicide assisté [End of life: We must distinguish between euthanasia and assisted suicide]. Rev. Prat. 2022, 72, 825–828. (In French) [Google Scholar] [PubMed]
- Sprung, C.L.; Maia, P.; Bulow, H.-H.; Ricou, B.; Armaganidis, A.; Baras, M.; Wennberg, E.; Reinhart, K.; Cohen, S.L.; Fries, D.R.; et al. The importance of religious affiliation and culture on end–of–life decisions in European intensive care units. Intensive Care Med. 2007, 33, 1732–1739. [Google Scholar] [CrossRef]
- Gula, R.M. Euthanasia: A Catholic perspective. Health Prog. 1987, 68, 28–42. [Google Scholar]
- Nagi, M.H.; Pugh, M.D.; Lazerine, N.G. Attitudes of Catholic and Protestant clergy on euthanasia and abortion. Pastor. Psychol. 1981, 29, 178–190. [Google Scholar] [CrossRef]
- Nie, L.; Smith–Han, K.; Iosua, E.; Walker, S. New Zealand medical students’ views of euthanasia/assisted dying across different year levels. BMC Med. Educ. 2021, 21, 125. [Google Scholar] [CrossRef] [PubMed]
- Lachowski, S.; Łuszczki, J.; Lachowska, B.; Florek–Łuszczki, M. Euthanasia in opinions of students of medicine. Ann. Agric. Environ. Med. 2023, 30, 148–155. [Google Scholar] [CrossRef]
- Leppert, W.; Gottwald, L.; Kazmierczak–Łukaszewicz, S. Euthanasia and palliative care problems in the views of sixth year medical students. Med. Paliat. 2009, 1, 45–52. (In Polish) [Google Scholar]
- Stronegger, W.J.; Schmölzer, C.; Rásky, E.; Freidl, W. Changing attitudes towards euthanasia among medical students in Austria. J. Med. Ethics 2011, 37, 227–229. [Google Scholar] [CrossRef] [PubMed]
- Nordstrand, M.A.; Nordstrand, S.J.; Materstvedt, L.J.; Nortvedt, P.; Magelssen, M. Medical students’ attitudes towards legalisation of euthanasia and physician–assisted suicide. Tidsskr. Nor. Laegeforening Tidsskr. Prakt. Med. Raekke 2013, 133, 2359–2363. [Google Scholar] [CrossRef] [PubMed]
- Dimovski, D.; Turanjanin, V.; Kolaković–Bojović, M.; Čvorović, D. Euthanasia in Serbia: Attitudes of Students of Law and Medicine. Int. Q. Community Health Educ. 2021, 41, 303–308. [Google Scholar] [CrossRef]
- Poreddi, V.; Reddy, S.s.N.; Pashapu, D.R. Attitudes of Indian Medical and Nursing Students Towards Euthanasia: A Cross–Sectional Survey. Omega 2022, 86, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Van Landeghem, P.; Carpentier, N.; Deliens, L. Different trends in euthanasia acceptance across Europe. A study of 13 western and 10 central and eastern European countries, 1981–2008. Eur. J. Public Health 2013, 23, 378–380. [Google Scholar] [CrossRef]
- World Health Organization. Global Atlas of Palliative Care at the End of Life, 2nd ed.; Worldwide Hospice Palliative Care Alliance: London, UK, 2020. [Google Scholar]
- Arias-Casais, N.; Garralda, E.; Rhee, J.; De Lima, L.; Pons Izquierdo, J.; Clark, D.; Hasselaar, J.; Mosoiu, D.; Ling, J.; Centeno, C. EAPC Atlas of Palliative Care in Europe 2019; EAPC Press: Vilvoorde, Belgium, 2019. [Google Scholar]
- Wilczkowski, K.; Rydzewski, S.J.; Doskocz, J.; Getek, J.; Kaniowski, B.; Korzeniewska, K.; Lebiedziński, F.; Pancewicz, M.; Pawłowski, L. Organisation of hospice and palliative care in Poland according to data from the National Health Fund—Cross-sectional study. Palliat. Med. Pract. 2024, 1–23. [Google Scholar] [CrossRef]
- Bauman, Z. 44 Letters from the Liquid Modern World; Polity Press: Cambridge, UK, 2011. [Google Scholar]


{kind=link}
| Total | Degree Course | ||||
|---|---|---|---|---|---|
| First- to Fourth-Year Medical Students | Fifth- to Sixth-Year Medical Students and Doctors in Training | First- to Fifth-Year Students of Polish and Classical Philology | |||
| (n = 313) | (n = 108) | (n = 98) | (n = 107) | ||
| Number of students (%) | 100% | 34.5% | 31.31% | 34.19% | |
| Age | (mean ± SD) | 23.52 ± 3.26 | 22.49 ± 2.56 | 25.6 ± 1.7 | 22.64 ± 4.02 |
| Range | 18–43 | 19–33 | 23–33 | 18–43 | |
| Gender | Men | 27.2% | 30.6% | 41.8% | 10.3% |
| Women | 71.2% | 68.5% | 57.1% | 86.9% | |
| No answer | 1.6% | 0.9% | 1% | 2.8% | |
| Religion | Roman Catholic | 54% | 54.6% | 65.3% | 43% |
| Orthodox | 0.63% | 0% | 1% | 0.9% | |
| Buddhist | 0.31% | 0% | 0% | 0.9% | |
| Atheist | 30.68% | 25% | 26.5% | 40.2% | |
| Agnostic | 6.39% | 8.3% | 3.1% | 7.5% | |
| Native believer | 2.24% | 1.9% | 0% | 4.7% | |
| Other | 1.6% | 2.9% | 0% | 1.9% | |
| No answer | 4.15% | 7.4% | 4.1% | 0.9% | |
| Place of residence | Rural area | 19.2% | 24.1% | 15.3% | 17.8% |
| Small city with up to 50 k residents | 18.5% | 19.4% | 18.4% | 17.8% | |
| City 51–100 k | 8% | 13.9% | 5.1% | 4.7% | |
| City 101–200 k | 22.4% | 22.2% | 42.9% | 3.7% | |
| Item | Total | First- to Fourth-Year Medical Students | Fifth- to Sixth-Year Medical Students and Intern | First- to Fifth-Year Students of the Polish and Classical Philology | p-Value | |
|---|---|---|---|---|---|---|
| (n = 313) | (n = 108) | (n = 98) | (n = 107) | |||
| Attitudes toward euthanasia | Yes | 68.69% | 65.75% | 65.3% | 74.8% | 0.072 |
| No | 14.69% | 11.1% | 17.35% | 15.9% | ||
| Do not know | 16.61% | 23.15%% | 17.35% | 9.3% | ||
| Attitudes toward assisted suicide | Yes | 35.8% | 38% | 30.6% | 38.3% | 0.398 |
| No | 24.3% | 19.4% | 30.6% | 23.4% | ||
| Do not know | 39.9% | 42.6% | 38.8% | 38.3% | ||
| Attitudes toward palliative care | Yes | 71.88% | 68.5% | 89.8% | 58.9% | <0.001 |
| No | 14.05% | 11.1% | 5.1% | 25.2% | ||
| Do not know | 14.05% | 20.4% | 5.1% | 15.9% | ||
| Yes | No | Attitudes toward Euthanasia | Attitudes toward Assisted Suicide | Attitudes toward Palliative Care | |
|---|---|---|---|---|---|
| % | % | p-Value | p-Value | p-Value | |
| Knowledge of the definition of palliative care (n = 313) | 87.5 | 12.5 | 0.972 | 0.533 | 0.463 |
| Knowledge of the definition of euthanasia (n = 313) | 95.5 | 4.5 | 0.138 | 0.916 | 0.744 |
| Knowledge of the definition of assisted suicide (n = 313) | 57.8 | 42.2 | 0.992 | <0.001 | 0.330 |
| Yes | No | Do Not Know | Attitudes toward Euthanasia | Attitudes toward Assisted Suicide | Attitudes toward Palliative Care | ||
|---|---|---|---|---|---|---|---|
| % | % | % | p-Value | p-Value | p-Value | ||
| Readiness to perform euthanasia (n = 206) | 43.7 | 17.5 | 38.8 | <0.001 | <0.001 | 0.016 | |
| Readiness to perform assisted suicide (n = 206) | 25.7 | 22.8 | 51.5 | <0.001 | <0.001 | 0.015 | |
| Natural death | Euthanasia | Assisted suicide | Persistent therapy | ||||
| % | % | % | % | ||||
| Declared willingness to undergo euthanasia (n = 313) | 41.5 | 42.8 | 9.6 | 6.1 | <0.001 | <0.001 | 0.035 |
| Ethical Norms According to Which One Should Always Respect the Patient’s Life, Even in an Advanced Stage of an Incurable Disease | Absolute Freedom of Choice for the Patient as well as the Possibility of Shortening the Life by the Doctor | Other | Attitudes toward Euthanasia | Attitudes toward Assisted Suicide | Attitudes toward Palliative Care | |
|---|---|---|---|---|---|---|
| % | % | % | p-Value | p-Value | p-Value | |
| The most important value in the doctor–patient relationship (n = 313) | 28.1 | 49.5 | 22.4 | <0.001 | <0.001 | 0.053 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forycka, M.; Liberacka-Dwojak, M.; Leppert, W.; Suchecki, P.; Suchecka, N.; Ast, B. Psychological Factors Influencing Attitudes towards Euthanasia, Assisted Suicide and Palliative Care among Medical Students and Doctors in Training. Healthcare 2024, 12, 833. https://doi.org/10.3390/healthcare12080833
Forycka M, Liberacka-Dwojak M, Leppert W, Suchecki P, Suchecka N, Ast B. Psychological Factors Influencing Attitudes towards Euthanasia, Assisted Suicide and Palliative Care among Medical Students and Doctors in Training. Healthcare. 2024; 12(8):833. https://doi.org/10.3390/healthcare12080833
Chicago/Turabian StyleForycka, Maria, Magdalena Liberacka-Dwojak, Wojciech Leppert, Paweł Suchecki, Natalia Suchecka, and Bartłomiej Ast. 2024. "Psychological Factors Influencing Attitudes towards Euthanasia, Assisted Suicide and Palliative Care among Medical Students and Doctors in Training" Healthcare 12, no. 8: 833. https://doi.org/10.3390/healthcare12080833
APA StyleForycka, M., Liberacka-Dwojak, M., Leppert, W., Suchecki, P., Suchecka, N., & Ast, B. (2024). Psychological Factors Influencing Attitudes towards Euthanasia, Assisted Suicide and Palliative Care among Medical Students and Doctors in Training. Healthcare, 12(8), 833. https://doi.org/10.3390/healthcare12080833