


Status and Barriers of Physical Activity and Exercise in Community-Dwelling Stroke Patients in South Korea: A Survey-Based Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Survey
2.2.1. EuroQol-5D (EQ-5D)
- Mobility (M): ‘Slight’ issues were assigned a value of M2 = 1, and ‘severe’ issues, M3 = 1.
- Self-Care (SC): For ‘slight’ and ‘severe’ issues, values of SC2 = 1 and SC3 = 1 were respectively applied.
- Usual Activities (UA): ‘Slight’ and ‘severe’ difficulties received scores of UA2 = 1 and UA3 = 1, respectively.
- Pain/Discomfort (PD): PD2 = 1 was allocated for ‘slight’ discomfort, and PD3 = 1 for ‘severe’.
- Anxiety/Depression (AD): ‘Slight’ issues were quantified as AD2 = 1, and ‘severe’ as AD3 = 1.
- No. of severe problem (N): If there is at least one dimension in which severe problems are reported, N3 = 1 is applied.
2.2.2. Reintegration to Normal Living Index (RNLI)
2.3. Statistical Analyses
3. Results
3.1. Participant Characteristics
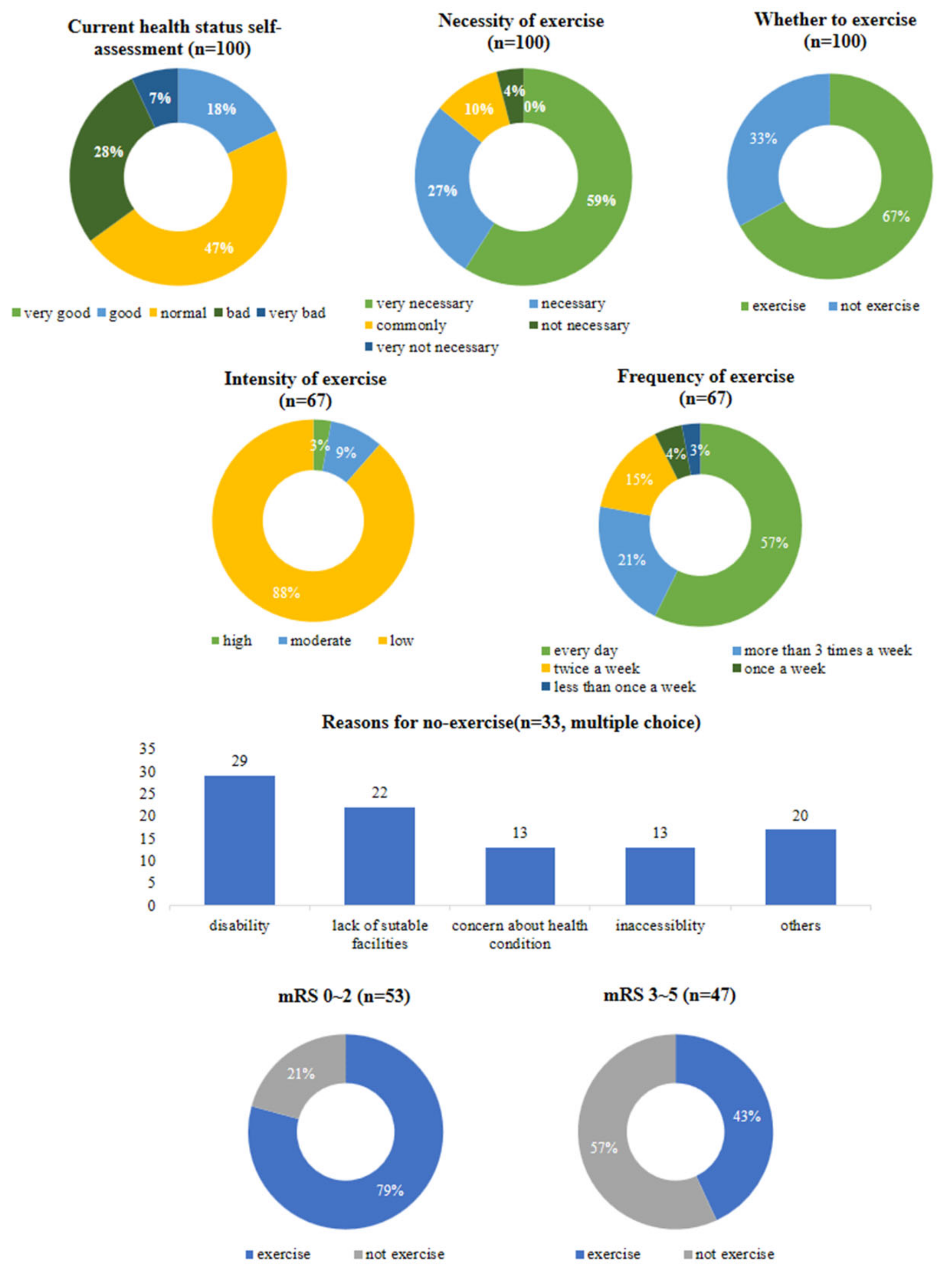
3.2. Self-Assessment of Health Status and Physical Activity Status after Discharge from Hospital
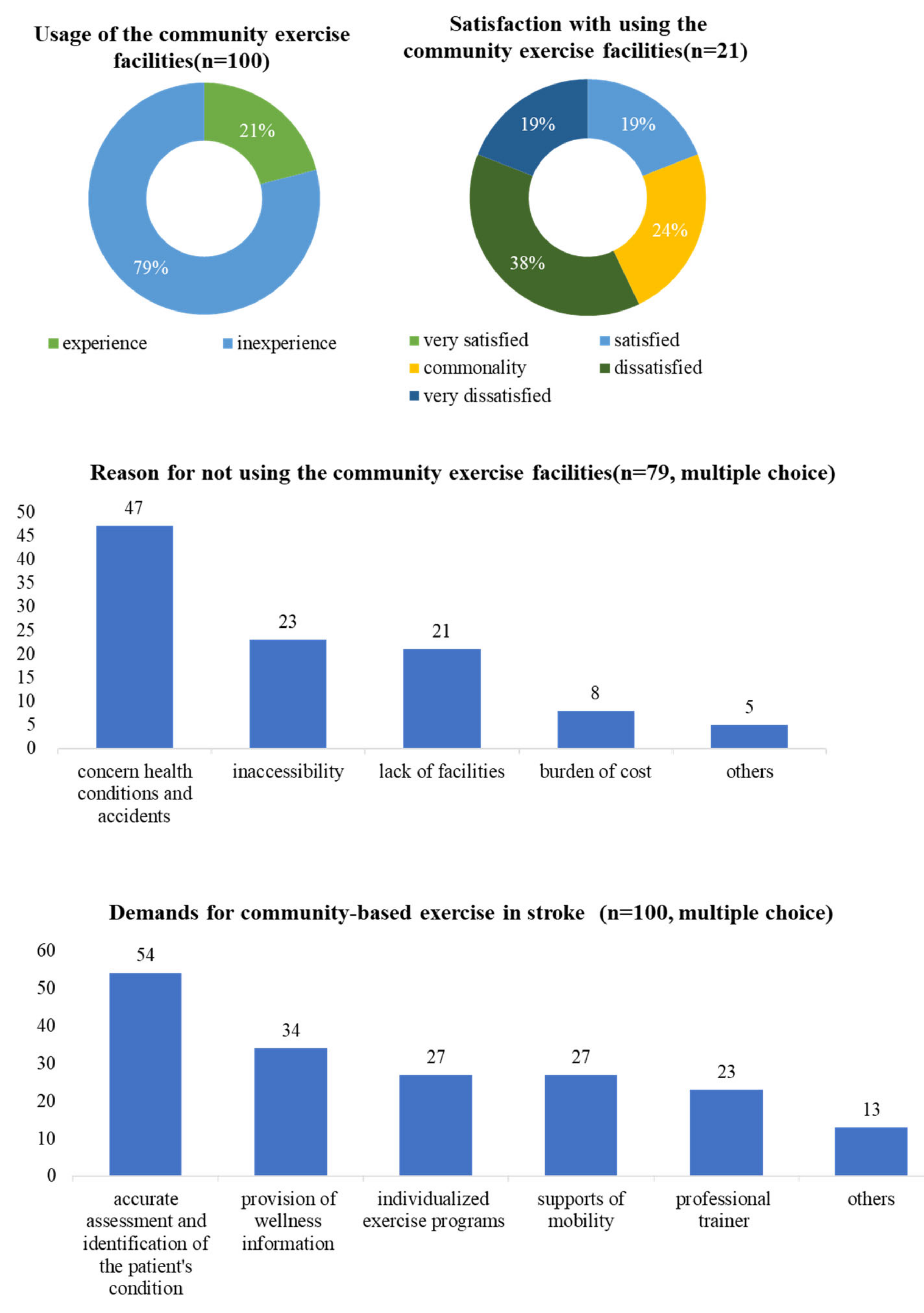
3.3. Demands for Community-Based Exercise after Discharge
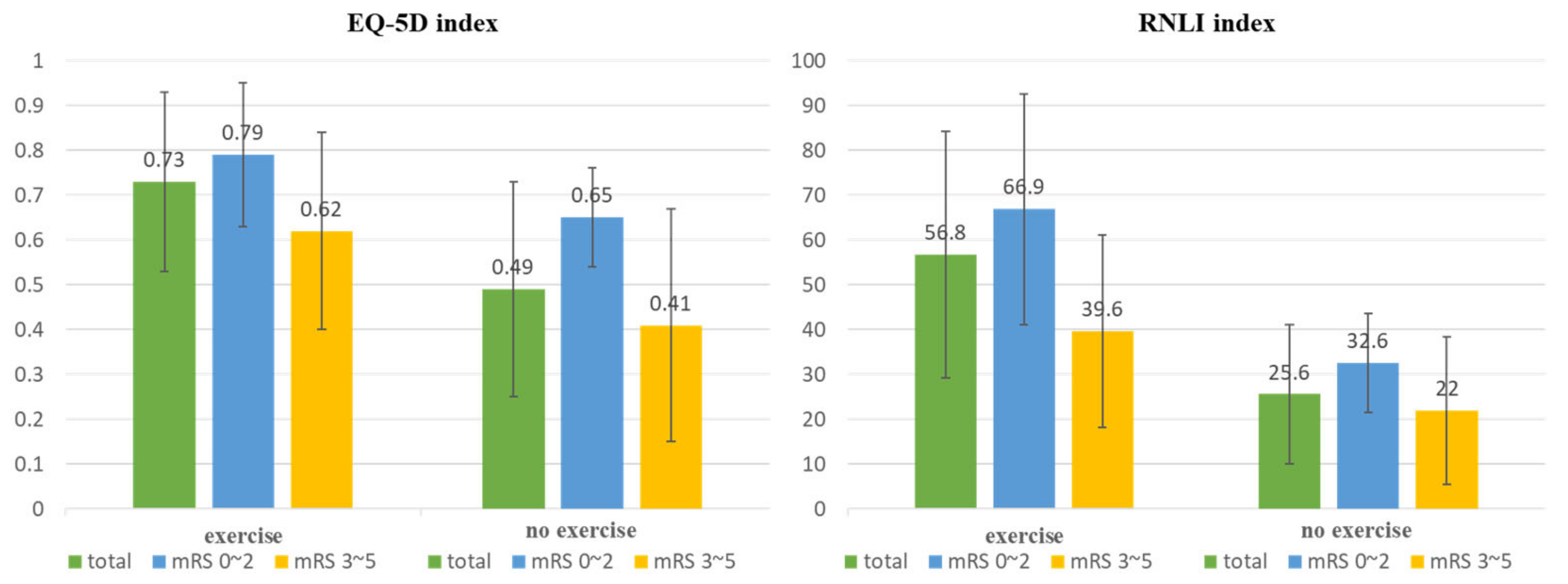
3.4. QoL and Social Participation According to Exercise after Discharge
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Statistics Korea. 2021 Annual Report on the Causes of Death Statistics. Available online: https://kostat.go.kr/board.es?mid=a10301060200&bid=218&act=view&list_no=420715 (accessed on 27 November 2022).
- Wheatley, C. Evaluation and treatment of cognitive dysfunction. In Occupational Therapy: Practice Skills for Physical Dysfunction; Lorraine Williams Pedretti: Mosby, MI, USA, 2001; pp. 456–491. [Google Scholar]
- Baek, S.; Park, E.; Cho, M.; Kim, H. Analysis of the burden factors influencing quality of life of stroke patients caregivers. J. Korea Entertain. Ind. Assoc. 2016, 10, 227–234. [Google Scholar] [CrossRef]
- Lee, J.; Stone, A.J. Combined aerobic and resistance training for cardiorespiratory fitness, muscle strength, and walking capacity after stroke: A systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 2020, 29, 104498. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Park, J.; Deok, E.S. Development and Effectiveness of Combined Exercise Based on Rehabilitation Sports Program for Stroke in the Community: A Randomized Pilot Study. J. Korean Soc. Rhythmic. Exerc. 2022, 15, 21–32. [Google Scholar]
- Chen, M.D.; Rimmer, J.H. Effects of exercise on quality of life in stroke survivors: A meta-analysis. Stroke 2011, 42, 832–837. [Google Scholar] [CrossRef]
- Joundi, R.A.; Patten, S.B.; Lukmanji, A.; Williams, J.V.A.; Smith, E.E. Association Between Physical Activity and Mortality Among Community-Dwelling Stroke Survivors. Neurology 2021, 97, e1182–e1191. [Google Scholar] [CrossRef]
- Kang, S.-M.; Kim, S.-H.; Han, K.-D.; Paik, N.-J.; Kim, W.-S. Physical activity after ischemic stroke and its association with adverse outcomes: A nationwide population-based cohort study. Top Stroke Rehabil. 2021, 28, 170–180. [Google Scholar] [CrossRef]
- Ju, E.-S.; Bang, Y.-S. The Effects of Multimodal Activity Program on Physical Function, Cognitive Function and Depression of the Elderly. Stroke J. Korea Entertain. Ind. Assoc. 2018, 12, 317–328. [Google Scholar] [CrossRef]
- Park, Y.-J.; Lee, C.-Y. Effects of a group self exercise program on quality of life and motor functions after stroke. J. Korean Acad. Univ. Trained Phys. Ther. 2008, 15, 20–29. [Google Scholar]
- Kang, D.-H.; Park, J.; Deok, E.S. Effects of community-based group exercise program on the motor function and quality of life for patients with stroke—A randomized controlled pilot study. Technol. Manag. 2022, 7, 101–123. [Google Scholar]
- Vahlberg, B.; Cederholm, T.; Lindmark, B.; Zetterberg, L.; Hellstrom, K. Short-term and long-term effects of a progressive resistance and balance exercise program in individuals with chronic stroke: A randomized controlled trial. Disabil. Rehabil. 2017, 39, 1615–1622. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, L.T.; Nadeau, S.; Britto, R.R.; Teixeira-Salmela, L.F.; Martins, J.C.; de Morais Faria, C.D.C. Effects of aerobic training on physical activity in people with stroke: Protocol for a randomized controlled trial. Trials 2018, 19, 1–8. [Google Scholar] [CrossRef]
- Yoo, S.D. Secondary Prevention as Integral Part of Stroke Rehabilitation. Brain NeuroRehabilitation 2014, 60, 86–92. [Google Scholar] [CrossRef]
- Choi, Y.-A.; Lee, J.S.; Park, J.H.; Kim, Y.H. Patterns of physical activity and sedentary behavior and their associated factors among nondisabled stroke survivors. Maturitas 2022, 158, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Butler, E.N.; Evenson, K.R. Prevalence of physical activity and sedentary behavior among stroke survivors in the United States. Top Stroke Rehabil. 2014, 21, 246–255. [Google Scholar] [CrossRef] [PubMed]
- English, C.; Manns, P.J.; Tucak, C.; Bernhardt, J. Physical Activity and Sedentary Behaviors in People With Stroke Living in the Community: A Systematic Review. Phys. Ther. 2014, 94, 185–196. [Google Scholar] [CrossRef]
- Fini, N.A.; Holland, A.E.; Keating, J.; Simek, J.; Bernhardt, J. How physically active are people following stroke? Systematic review and quantitative synthesis. Phys. Ther. 2017, 97, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Craig, C.L.; Brown, W.J.; Clemes, S.A.; De Cocker, K.; Giles-Corti, B.; Hatano, Y.; Inoue, S.; Matsudo, S.M.; Mutrie, N.; et al. How many steps/day are enough? For adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Craig, C.L.; Aoyagi, Y.; Bell, R.C.; Croteau, K.A.; De Bourdeaudhuij, I.; Ewald, B.; Gardner, A.W.; Hatano, Y.; Lutes, L.D.; et al. How many steps/day are enough? For older adults and special populations. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–19. [Google Scholar] [CrossRef]
- Nicholson, S.; Sniehotta, F.F.; Van Wijck, F.; Greig, C.A.; Johnston, M.; McMurdo, M.E.; Dennis, M.; Mead, G.E. A systematic review of perceived barriers and motivators to physical activity after stroke. Int. J. Stroke 2013, 8, 357–364. [Google Scholar] [CrossRef]
- EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Jeon, G.S.; Park, S.J.; Jang, S.N. The Relationship between Frailty and Health-Related Quality of Life among Korean Elderly. J. Korean Geriatr. Soc. 2012, 16, 175–183. [Google Scholar] [CrossRef]
- Feng, Y.S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2021, 30, 647–673. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, I.; Janssen, M.F.; Kohlmann, T.; Feng, Y.S. A Systematic Review of Studies Comapring the Measurement Properties of the Three-Level and Five-Level Versions of the EQ-5D. Pharmacoeconomics 2018, 36, 645–661. [Google Scholar] [CrossRef] [PubMed]
- Wood-Dauphinee, S.; Williams, J.I. Reintegration to normal living as a proxy to quality of life. J. Chronic Dis. 1987, 40, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Merz, Z.C.; Van Patten, R.; Mulhauser, K.; Fucetola, R. Exploratory factor analysis of the reintegration to normal living index in a stroke population. Top. Stroke Rehabil. 2017, 24, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Bourget, N.; Deblock-Bellamy, A.; Blanchette, A.K.; Batcho, C.S. Use and psychometric properties of the Reintergration to Normal Living Index in rehabilitation: A systematic review. Ann. Phys. Rehabil. Med. 2018, 61, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.-S.; Yu, K.-H.; Rha, J.-H.; Kim, H.Y.; Koo, J.; Park, J.-M.; Seo, D.-H.; Park, I.S.; Cho, K.-H.; Jung, K.-H.; et al. Review of Evidences and Updates of the Korean Clinical Practice Guidelines for Stroke in 2013. Korean Soc. NeuroRehabilitation 2013, 31, 143–157. [Google Scholar]
- Kim, D.Y.; Ryu, B.; Oh, B.M.; Kim, D.Y.; Kim, D.S.; Kim, D.Y.; Kim, D.K.; Kim, E.J.; Lee, H.Y.; Choi, H.; et al. Clinical Practice Guideline for Stroke Rehabilitation in Korea-Part 1: Rehabilitation for Motor Function (2022). Brain Neurorehabil. 2023, 16, e18. [Google Scholar] [CrossRef]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef]
- Meschia, J.F.; Bushnell, C.; Boden-Albala, B.; Braun, L.T.; Bravata, D.M.; Chaturvedi, S.; Creager, M.A.; Eckel, R.H.; Elkind, M.S.; Fornage, M.; et al. Guidelines for the primary prevention of stroke: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 3754–3832. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, T.; You, L.; Li, K. Barriers to activity and participation for stroke survivors in rural China. Arch. Phys. Med. Rehabil. 2015, 96, 1222–1228. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, M.A.; Batcho, C.S.; Best, K.L. A description of physical activity behaviors, barriers, and motivators in stroke survivors in Quebec. Disabil. Health J. 2022, 15, 101265. [Google Scholar] [CrossRef] [PubMed]
- Teo, R.; Thilarajah, S.; Jiale, L.; Yu, F.L.F.; Khim, K.L. Barriers to physical activity of stroke survivors in Singapore: A face-to-face cross-sectional survey. Proc. Singap. Healthc. 2023, 32, 20101058231184953. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Questions | Answers | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Current health status self-assessment | Very good | Good | Normal | Bad | Very bad | |||||
| 2. Necessity of exercise | Very necessary | Necessary | Common | Not necessary | Very not necessary | |||||
| 3. Whether to exercise | Exercise | Not exercise | ||||||||
| 3.1.1. Intensity of exercise | High | Moderate | Low | |||||||
| 3.1.2. Frequency of exercise | Every day | Three or more times a week | Twice a week | Once a week | Less than once a week | |||||
| 3.2. Reasons for no exercise (multiple choice) | Disability | Lack of suitable facilities | Concern about health conditions | Inadequate accessibility | Others | |||||
| 4. Usage of the community exercise facilities | Experience | Inexperience | ||||||||
| 4.1. Satisfaction with using the community exercise facilities | Very satisfied | Satisfied | Commonality | Dissatisfied | Very dissatisfied | |||||
| 4.2. Reason for not using the community exercise facilities | Concern about health conditions and accidents | Difficult mobility and inadequate accessibility | Lack of time or suitable facilities | Burden of cost | Others | |||||
| 5. Essential factors needed for community-based exercise (multiple choice) | Accurate assessment and identification of the patient’s condition | Providing and linking to welfare | Individual exercise program | Supports of mobility and accessibility | Qualified exercise trainers | Others | ||||
| Characteristics | (n = 100) |
|---|---|
| Age (years) | |
| <40 | 5 |
| 40–59 | 37 |
| 60–69 | 34 |
| ≥70 | 24 |
| Sex | |
| Male | 56 |
| Female | 44 |
| Type of stroke | |
| Infarction | 43 |
| Hemorrhage | 57 |
| Time since stroke (months) | |
| <12 | 15 |
| 12–59 | 38 |
| 60–120 | 31 |
| ≥120 | 13 |
| Modified Rankin Scale score | |
| 0–2 | 53 |
| 3–5 | 47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-L.; Kim, Y.; Huh, S.; Shin, Y.-I.; Ko, S.-H. Status and Barriers of Physical Activity and Exercise in Community-Dwelling Stroke Patients in South Korea: A Survey-Based Study. Healthcare 2024, 12, 697. https://doi.org/10.3390/healthcare12060697
Lee J-L, Kim Y, Huh S, Shin Y-I, Ko S-H. Status and Barriers of Physical Activity and Exercise in Community-Dwelling Stroke Patients in South Korea: A Survey-Based Study. Healthcare. 2024; 12(6):697. https://doi.org/10.3390/healthcare12060697
Chicago/Turabian StyleLee, Jung-Lim, Yuna Kim, Sungchul Huh, Yong-Il Shin, and Sung-Hwa Ko. 2024. "Status and Barriers of Physical Activity and Exercise in Community-Dwelling Stroke Patients in South Korea: A Survey-Based Study" Healthcare 12, no. 6: 697. https://doi.org/10.3390/healthcare12060697
APA StyleLee, J.-L., Kim, Y., Huh, S., Shin, Y.-I., & Ko, S.-H. (2024). Status and Barriers of Physical Activity and Exercise in Community-Dwelling Stroke Patients in South Korea: A Survey-Based Study. Healthcare, 12(6), 697. https://doi.org/10.3390/healthcare12060697