
The Effectiveness and Usability of a Rehabilitation Program Using the Nintendo Switch to Promote Healthy Aging in Older People with Cognitive Impairment: A Randomized Clinical Trial
 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
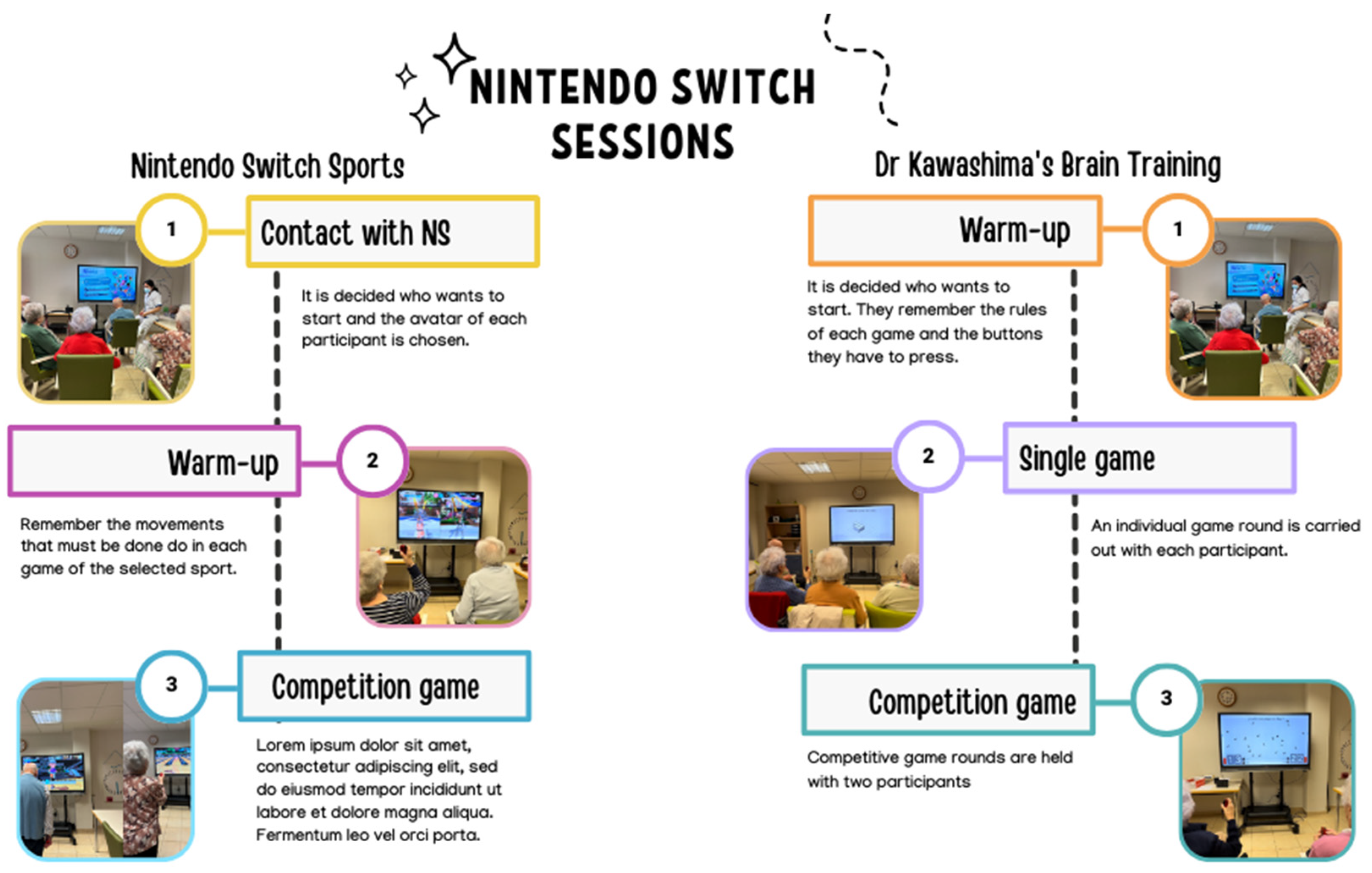
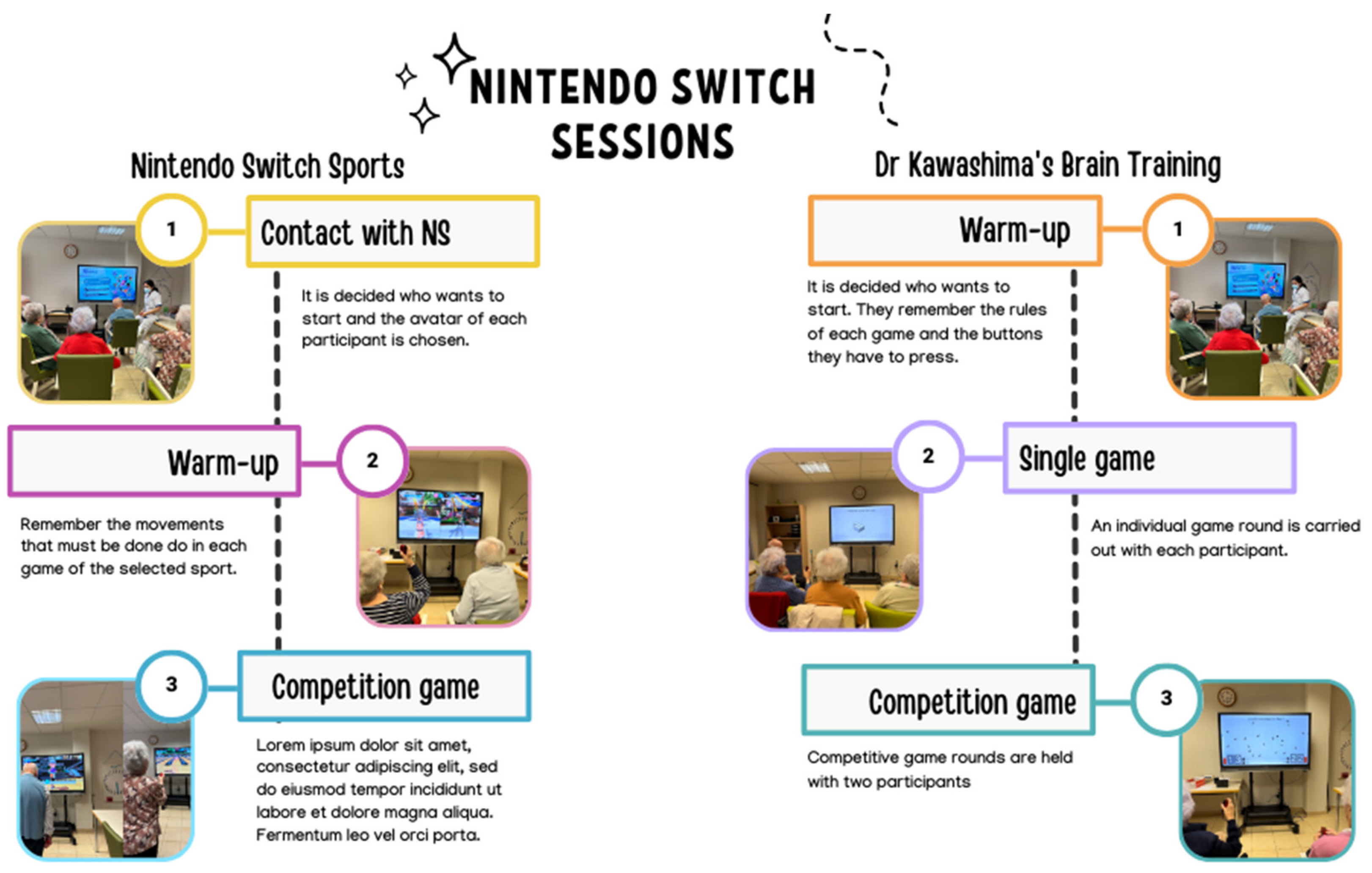
2.3. Intervention
- Nintendo Switch Sports:
- Golf: requires the player to stand upright, perform block movements with both upper limbs and slight wrist movements, as well as requiring trunk and shoulder stability.
- Tennis: requires the player to perform upper limb movements, such as flexion-extension, abduction and adduction of the shoulder, flexion-extension of the elbow, and pronation-supination of the forearm, as well as testing strength and the player’s reflexes.
- Bowling: requires shoulder flexion-extension, elbow flexion-extension, and cylindrical palm pressing in order to press a button with the second finger until releasing it to throw.
- Chambara: consists of performing movements of flexion-extension, abduction and adduction of the shoulder, elbow flexion-extension, and the palmar pressure of the hand in order to defeat the opponent.
- 2.
- Dr Kawashima’s Brain Training for Nintendo Switch
- Rock, paper, and scissors: the player must analyse what result they are asked for and perform the gesture of stone (closed fist), paper (open hand), or scissors (extension of the second and third fingers and the opposition of the first finger to the fourth and fifth fingers). With the other hand, the player needs to hold the other controller horizontally, so that the camera picks up the movement.
- Fingerprinting: consists of performing simple mental calculations and representing the result with the fingers of the hand (right or left), which can be one, two, three, four, five, or zero.
- Finger gymnastics: This consists of performing different hand gestures (right or left) in the shortest possible time. These gestures engage the opposition of the fingers to the palm and the extension of one or more fingers.
- Bird Counter: Two participants must count the birds that appear on the screen and enter the correct number before the opponent (by pressing the buttons with their thumb).
- Flags: Two participants must memorize the correct order of the raised flags and imitate it following the sequence shown. The movements involved in this game are flexion, extension, abduction, and shoulder adduction.
- Box counter: Two participants must memorize the number of boxes that appear on the screen before they disappear. Each player must enter the correct number of boxes (by pressing the buttons with their thumb) as quickly as possible before their opponent.
2.4. Measures
- General Medical Information
- 2.
- Examination of Cognitive Status
- 3.
- Examination of Functional Independence
- 4.
- Examination of the Upper Limb Function
- 5.
- Examination of quality of life
- 6.
- Examination of satisfaction with the treatment received
2.5. Statiscal Analysis
3. Results
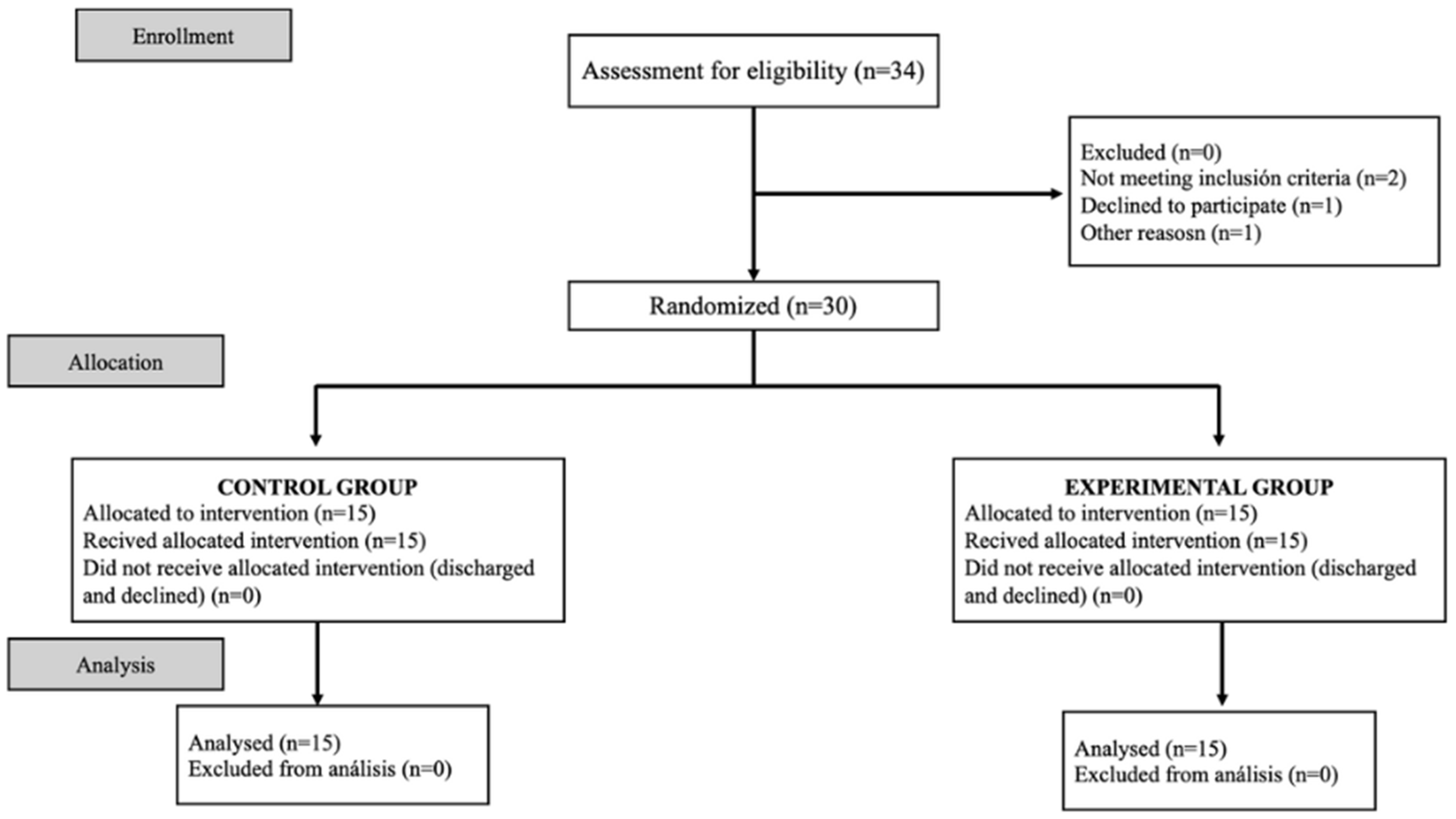
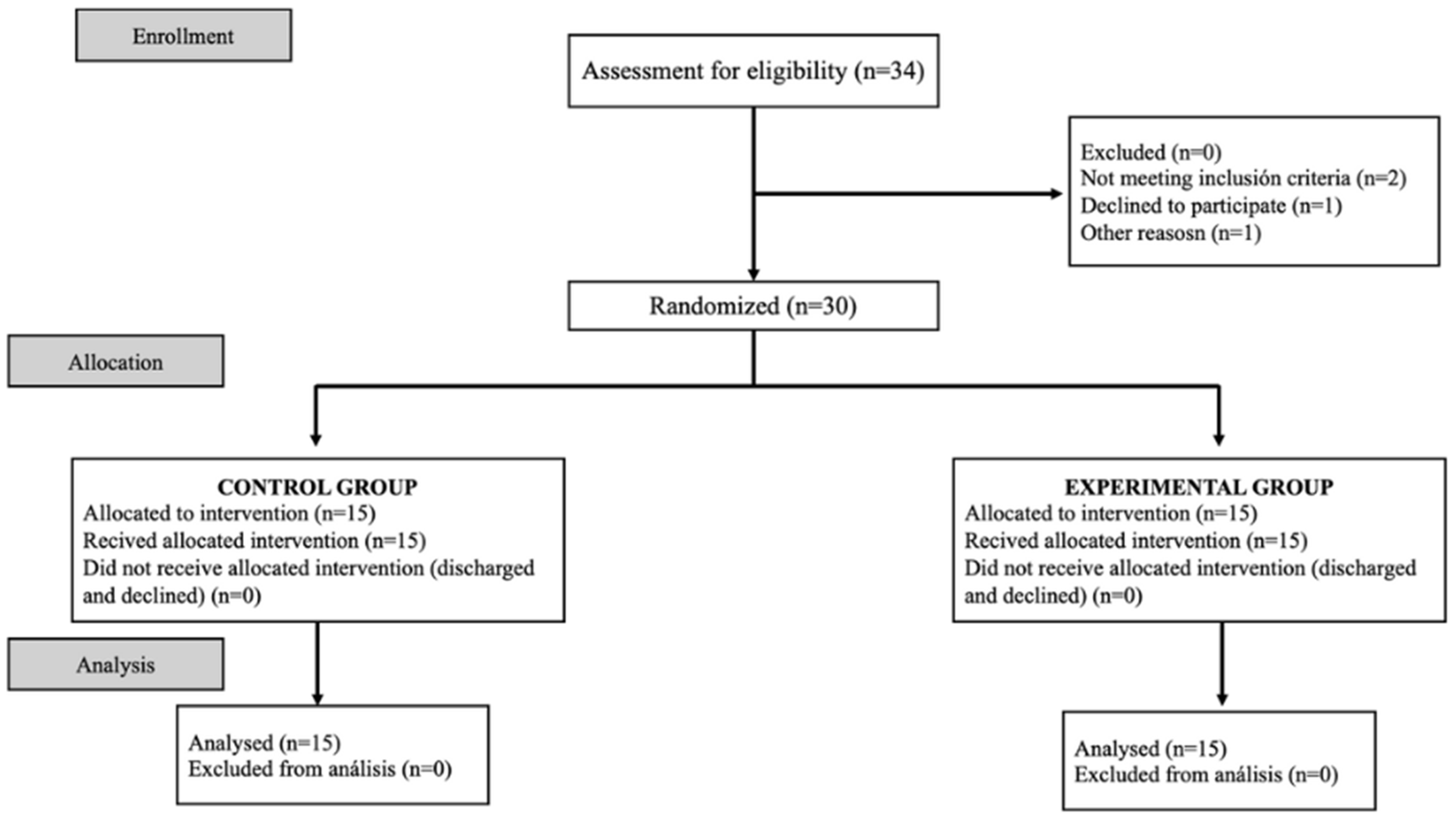
3.1. Attrition Rate
3.2. Baseline Characteristics of Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swirsky, L.T.; Spaniol, J. Cognitive and motivational selectivity in healthy aging. Wiley Interdiscip. Rev. Cogn. Sci. 2019, 10, e1512. [Google Scholar] [CrossRef]
- Behr, L.C.; Simm, A.; Kluttig, A.; Grosskopf Großkopf, A. 60 years of healthy aging: On definitions, biomarkers, scores and challenges. Ageing Res. Rev. 2023, 88, 101934. [Google Scholar] [CrossRef]
- Zhang, Z.D.; Milman, S.; Lin, J.R.; Wierbowski, S.; Yu, H.; Barzilai, N.; Gorbunova, V.; Ladiges, W.C.; Niedernhofer, L.J.; Suh, Y.; et al. Genetics of extreme human longevity to guide drug discovery for healthy ageing. Nat. Metab. 2020, 2, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Banks, W.A.; Reed, M.J.; Logsdon, A.F.; Rhea, E.M.; Erickson, M.A. Healthy aging and the blood-brain barrier. Nat. Aging 2021, 1, 243–254. [Google Scholar] [CrossRef]
- Michel, J.P.; Sadana, R. “Healthy Aging” Concepts and Measures. J. Am. Med. Dir. Assoc. 2017, 18, 460–464. [Google Scholar] [CrossRef]
- Eckstrom, E.; Neukam, S.; Kalin, L.; Wright, J. Physical Activity and Healthy Aging. Clin. Geriatr. Med. 2020, 36, 671–683. [Google Scholar] [CrossRef]
- Laver, K.E. Occupational therapy and the language of healthy ageing. Aust. Occup. Ther. J. 2021, 68, 285–286. [Google Scholar] [CrossRef]
- De Santis, K.K.; Mergenthal, L.; Christianson, L.; Busskamp, A.; Vonstein, C.; Zeeb, H. Digital Technologies for Health Promotion and Disease Prevention in Older People: Scoping Review. J. Med. Internet Res. 2023, 25, e43542. [Google Scholar] [CrossRef]
- Li, G.; Li, X.; Chen, L. Effects of virtual reality-based interventions on the physical and mental health of older residents in long-term care facilities: A systematic review. Int. J. Nurs. Stud. 2022, 136, 104378. [Google Scholar] [CrossRef]
- García-Bravo, S.; Cuesta-Gómez, A.; Campuzano-Ruiz, R.; López-Navas, M.J.; Domínguez-Paniagua, J.; Araújo-Narváez, A.; Barreñada-Copete, E.; García-Bravo, C.; Flórez-García, M.T.; Botas-Rodríguez, J.; et al. Virtual reality and video games in cardiac rehabilitation programs. A systematic review. Disabil. Rehabil. 2021, 43, 448–457. [Google Scholar] [CrossRef]
- Waliño-Paniagua, C.N.; Gómez-Calero, C.; Jiménez-Trujillo, M.I.; Aguirre-Tejedor, L.; Bermejo-Franco, A.; Ortiz-Gutiérrez, R.M.; Cano-De-La-Cuerda, R. Effects of a game-based virtual reality video capture training program plus occupational therapy on manual dexterity in patients with multiple sclerosis: A randomized controlled trial. J. Healthc. Eng. 2019, 2019, 9780587. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Gómez, A.; Sánchez-Herrera-Baeza, P.; Oña-Simbaña, E.D.; Martínez-Medina, A.; Ortiz-Comino, C.; Balaguer-Bernaldo-De-Quirós, C.; Jardón-Huete, A.; Cano-De-La-Cuerda, R. Effects of virtual reality associated with serious games for upper limb rehabilitation inpatients with multiple sclerosis: Randomized controlled trial. J. Neuroeng. Rehabil. 2020, 17, 90. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Xiong, S. Effectiveness and Usability of a Novel Kinect-Based Tailored Interactive Fall Intervention System for Fall Prevention in Older People: A Preliminary Study. Front. Public Health 2022, 10, 884551. [Google Scholar] [CrossRef]
- Béraud-Peigné, N.; Maillot, P.; Perrot, A. The User Experience of an Immersive and Interactive Wall Exergame in Older Adults. Games Health J. 2023, 12, 220–227. [Google Scholar] [CrossRef]
- Vargas Matamala, M.; Tapia, C.; Salvador Sagüez, F.; Guerrero-Henriquez, J. Postural performance assessment in aging people with diabetes and diabetic peripheral neuropathy using a Wii balance board. Disabil. Rehabil. 2023, 45, 1202–1207. [Google Scholar] [CrossRef]
- García-Bravo, S.; García-Bravo, C.; Molina-Rueda, F.; Cuesta-Gómez, A. Training With Wii Balance Board for Dynamic Balance in Older Adults. Top. Geriatr. Rehabil. 2020, 36, 79–85. [Google Scholar] [CrossRef]
- Tuan, S.H.; Chang, L.H.; Sun, S.; Lin, K.L.; Tsai, Y.J. Using exergame-based exercise to prevent and postpone the loss of muscle mass, muscle strength, cognition, and functional performance among elders in rural long-term care facilities: A protocol for a randomized controlled trial. Front. Med. 2022, 9, 1071409. [Google Scholar] [CrossRef]
- Cuesta-Gómez, A.; Martín-Díaz, P.; Sánchez-Herrera Baeza, P.; Martínez-Medina, A.; Ortiz-Comino, C.; Cano-de-la-Cuerda, R. Nintendo Switch Joy-Cons’ Infrared Motion Camera Sensor for Training Manual Dexterity in People with Multiple Sclerosis: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 3261. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel grouprandomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef]
- Guillaumesa, S.; O’Callaghanb, C.A. Spanish version of the free OxMaR software for minimization and randomization of clinical trials. Gac. Sanit. 2019, 33, 395–397. [Google Scholar] [CrossRef]
- Lobo, A.; Saz, P.; Marcos, G.; Día, J.L.; de la Cámara, C.; Ventura, T.; Morales Asín, F.; Fernando Pascual, L.; Montañés, J.A.; Aznar, S. Revalidation and standardization of the Mini-Cognitive Exam (first Spanish version of the Mini-Mental Status Examination) in the general geriatric population. Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Cid-Ruzafa, J.; Damián-Moreno, J. Assessment of Physical Disability: The Barthel. Rev. Esp. Salud Pública 1997, 71, 127–137. [Google Scholar] [CrossRef]
- Moreno-Morente, G.; Hurtado-Pomares, M.; Terol Cantero, M.C. Bibliometric Analysis of Research on the Use of the Nine Hole Peg Test. Int. J. Environ. Res. Public Health 2022, 19, 10080. [Google Scholar] [CrossRef]
- Díaz-Arribas, M.J.; Martín-Casas, P.; Cano-de-la-Cuerda, R.; Plaza-Manzano, G. Effectiveness of the Bobath concept in the treatment of stroke: A systematic review. Disabil. Rehabil. 2020, 42, 1636–1649. [Google Scholar] [CrossRef]
- Huertas-Hoyas, E.; Martínez-Piédrola, M.R.; Sánchez-Herrera-Baeza, P.; Serrada Tejeda, S.; Máximo-Bocanegra, N.; Sánchez Camarero, C.; Pérez-de-Heredia-Torres, M.; Martínez Castrillo, J.C. Alterations in dexterity and manual function in patients with focal hand dystonia. Neurologia 2020, 38, 1–7. [Google Scholar] [CrossRef]
- The Whoqol Group. Development of the World Health Organization WHOQOLBREF Quality of Life Assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Atrkisson, C.C.; Mendias, R.M. Assessing the client satisfaction questionnaire in English and Spanish. Hisp. J. Behav. Sci. 1984, 6, 385–396. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Torres, Á.; Otero, P.; Blanco, V.; Attkisson, C.C. Psychometric properties of the Castilian Spanish version of the Client Satisfaction Questionnaire (CSQ-8). Curr. Psychol. 2019, 38, 829–835. [Google Scholar] [CrossRef]
- Takei, K.; Morita, S.; Watanabe, Y.; Suganami, M.; Inao, M. Safety, feasibility, and acceptability of physiotherapy combined with strength training using active video games for older patients with musculoskeletal conditions. Disabil. Rehabil. Assist. Technol. 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Blázquez-González, P.; Mirón-González, R.; Lendínez-Mesa, A.; Luengo-González, R.; Mancebo-Salas, N.; Camacho-Arroyo, M.T.; Muriel-García, A.; García-Sastre, M.M. Efficacy of the use of video games on mood, anxiety and depression in stroke patients: Preliminary findings of a randomised controlled trial. J. Neurol. 2024, 271, 1224–1234. [Google Scholar] [CrossRef]
- Kim, J.E.; Lee, M.Y.; Yim, J.E. A New Approach to Transcranial Direct Current Stimulation in Improving Cognitive Motor Learning and Hand Function with the Nintendo Switch in Stroke Survivors. Med. Sci. Monit. 2019, 25, 9555–9562. [Google Scholar] [CrossRef]
- Yu, J.; Wu, J.; Liu, B.; Zheng, K.; Ren, Z. Efficacy of virtual reality technology interventions for cognitive and mental outcomes in older people with cognitive disorders: An umbrella review comprising meta-analyses of randomized controlled trials. Ageing Res. Rev. 2023, 94, 102179. [Google Scholar] [CrossRef]
- Baldimtsi, E.; Mouzakidis, C.; Karathanasi, E.M.; Verykouki, E.; Hassandra, M.; Galanis, E.; Hatzigeorgiadis, A.; Goudas, M.; Zikas, P.; Evangelou, G.; et al. Effects of Virtual Reality Physical and Cognitive Training Intervention On Cognitive Abilities of Elders with Mild Cognitive Impairment. J. Alzheimers Dis. Rep. 2023, 7, 1475–1490. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.; Scherer, Y.K.; Montgomery, C.A. Effects of Using Nintendo Wii Exergames in Older Adults. J. Aging Health 2015, 27, 379–402. [Google Scholar] [CrossRef] [PubMed]
- Yen, H.Y.; Chiu, H.L. Virtual Reality Exergames for Improving Older Adults’ Cognition and Depression: A Systematic Review and Meta-Analysis of Randomized Control Trials. J. Am. Med. Dir. Assoc. 2021, 22, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Zenba, Y.; Kobayashi, A.; Imai, T. Psychological distress is affected by fear of COVID-19 via lifestyle disruption and leisure restriction among older adults in Japan: A cross-sectional study. Front. Public Health 2023, 11, 1264088. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Full Sample | Control Group (n = 15) | Experimental Group (n = 15) | H | Sig. p | |
|---|---|---|---|---|---|
| Gender (Fr (%)) | |||||
| Female | 18 (58.1) | 9 (60) | 9 (60) | ||
| Male | 12 (38.7) | 6 (40) | 6 (40) | ||
| Age (Mean ± DS) | 88.83 ± 3.94 | 87.47 ± 4.8 | 90.2 ± 2.27 | 3.76 | 0.052 |
| Barthel Index (Mean ± DS) | 95.00 ± 3.09 | 95.40 ± 3.43 | 94.6 ± 2.77 | 0.449 | 0.503 |
| MEC-Lobo (Mean ± DS) | 29.73 ± 2.72 | 29.93 ± 2.81 | 29.53 ± 2.72 | 0.158 | 0.691 |
| NHPT Right (Mean ± DS) | 39.85 ± 15.7 | 44.38 ± 18.19 | 35.32 ± 11.66 | 1.81 | 0.178 |
| NHPT Left (Mean ± DS) | 43.89 ±19.81 | 49.87 ± 25.32 | 37.91 ± 9.77 | 1.93 | 0.165 |
| BBT Right (Mean ± DS) | 41.23 ± 10.8 | 40 ± 11.408 | 42.47 ± 10.4 | 0.414 | 0.520 |
| BBT Left (Mean ± DS) | 39.90 ± 9.901 | 39.2 ± 10.7 | 40.6 ± 9.32 | 0.209 | 0.647 |
| General Perception Quality of Life (Mean ± DS) | 2.67 ± 0.802 | 2.67 ± 0.72 | 2.67 ± 0.9 | 0.000 | 0.982 |
| General Perception Health (Mean ± DS) | 2.17 ± 0.648 | 2.07 ± 0.704 | 2.27 ± 0.594 | 0.630 | 0.427 |
| Physical Health (Mean ± DS) | 2.17 ± 0.648 | 2.07 ± 0.7 | 2.27 ± 0.59 | 0.021 | 0.884 |
| Psychological Health (Mean ± DS) | 12.85 ± 2.36 | 12.76 ± 2.65 | 12.95 ± 2.12 | 0.011 | 0.915 |
| Social Relations (Mean ± DS) | 12.77 ± 2 | 12.73 ± 2.13 | 12.82 ± 1.92 | 0.610 | 0.435 |
| Environment (Mean ± DS) | 12.44 ± 2.04 | 12.16 ± 2.12 | 12.72 ± 1.98 | 0.074 | 0.785 |
| CSQ-8 | 25.43 ± 4.11 | 22 ± 1.73 | 28.87 ± 2.61 | 18.91 | 0.000 |
| Control Group (n = 15) (Mean ± DS) | Experimental Group (n = 15) (Mean ± DS) | H | Sig. p | dr | |
|---|---|---|---|---|---|
| Barthel Index | 29.33 ± 3.01 | 30.27 ± 3.01 | 0.506 | 0.477 | 0.31 |
| MEC-Lobo | 43.94 ± 18.9 | 33.67 ± 11.44 | 0.739 | 0.39 | 0.65 |
| NHPT Right | 51.67 ± 30.17 | 36.9 ± 9.19 | 3.10 | 0.078 | 0.66 |
| NHPT Left | 38.87 ± 10.65 | 50.07 ± 12.34 | 2.29 | 0.130 | 0.97 |
| BBT Right | 38.4 ± 12.35 | 48 ± 11.47 | 4.58 | 0.032 | 0.80 |
| BBT Left | 2.2 ± 0.86 | 3.47 ± 0.64 | 3.97 | 0.046 | 1.67 |
| General Perception Quality of Life | 2.07 ± 0.59 | 3 ± 0.65 | 12.61 | 0.000 | 1.49 |
| General Perception Health | 12.07 ± 2.61 | 14.3 ± 2.16 | 11.32 | 0.001 | 0.94 |
| Physical Health | 11.91 ± 1.99 | 14.61 ± 2.07 | 5.57 | 0.018 | 1.32 |
| Psychological Health | 11.32 ± 1.95 | 14.06 ± 2.15 | 9.83 | 0.002 | 1.33 |
| Social Relations | 12.06 ± 1.82 | 15.03 ± 2.15 | 9.87 | 0.002 | 1.49 |
| Environment | 29.33 ± 3.01 | 30.27 ± 3.01 | 10.69 | 0.001 | 0.31 |
| Control Group | Experimental Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre (Mean ± DS) | Post (Mean ± DS) | Z | Sig. | dr | Pre (Mean ± DS) | Post (Mean ± DS) | Z | Sig. | dr | |
| Barthel Index | 95.40 ± 3.43 | 29.33 ± 3.01 | −2.442 | 0.015 | 0.99 | 94.6 ± 2.77 | 30.27 ± 3.01 | −2.814 | 0.005 | 0.99 |
| MEC-Lobo | 29.93 ± 2.81 | 43.94 ± 18.9 | −2.714 | 0.007 | 0.46 | 29.53 ± 2.72 | 33.67 ± 11.44 | −1.935 | 0.053 | 0.24 |
| NHPT Right | 44.38 ± 18.19 | 51.67 ± 30.17 | −0.682 | 0.496 | 0.14 | 35.32 ± 11.66 | 36.9 ± 9.19 | −2.442 | 0.015 | 0.07 |
| NHPT Left | 49.87 ± 25.32 | 38.87 ± 10.65 | −1.079 | 0.281 | 0.27 | 37.91 ± 9.77 | 50.07 ± 12.34 | −1.988 | 0.047 | 0.47 |
| BBT Right | 40 ± 11.40 | 38.4 ± 12.35 | −0.915 | 0.360 | 0.06 | 42.47 ± 10.4 | 48 ± 11.47 | −2.955 | 0.003 | 0.24 |
| BBT Left | 39.2 ± 10.7 | 2.2 ± 0.86 | −0.697 | 0.486 | 0.92 | 40.6 ± 9.32 | 3.47 ± 0.64 | −3.270 | 0.001 | 0.94 |
| General Perception Quality of Life | 2.67 ± 0.72 | 2.07 ± 0.59 | −2.121 | 0.034 | 0.41 | 2.67 ± 0.9 | 3 ± 0.65 | −2.762 | 0.006 | 0.20 |
| General Perception Health | 2.07 ± 0.70 | 12.07 ± 2.61 | 0.000 | 1.000 | 0.93 | 2.27 ± 0.59 | 14.3 ± 2.16 | −3.051 | 0.002 | 0.96 |
| Physical Health | 2.07 ± 0.70 | 11.91 ± 1.99 | −2.585 | 0.010 | 0.95 | 2.27 ± 0.59 | 14.61 ± 2.07 | −2.764 | 0.006 | 0.97 |
| Psychological Health | 12.76 ± 2.65 | 11.32 ± 1.95 | −2.294 | 0.022 | 0.29 | 12.95 ± 2.12 | 14.06 ± 2.15 | −2.728 | 0.006 | 0.25 |
| Social Relations | 12.73 ± 2.13 | 12.06 ± 1.82 | −2.392 | 0.017 | 0.16 | 12.82 ± 1.92 | 15.03 ± 2.15 | −2.451 | 0.014 | 0.47 |
| Environment | 12.16 ± 2.12 | 29.33 ± 3.01 | −1.847 | 0.065 | 0.95 | 12.72 ± 1.98 | 30.27 ± 3.01 | −2.963 | 0.003 | 0.96 |
| Age | Gender | BI | MEC-Lobo | NHPT-R | NHPT-L | BBT-R | BBT-L | GPQoL | GPH | PH | PsH | SR | E | CSQ-8 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 0.178 | −0.095 | −0.374 * | −0.151 | −0.055 | 0.202 | 0.064 | −0.062 | −0.053 | 0.171 | 0.024 | −0.082 | 0.104 | 0.416 | 0.178 * |
| Gender | 0.178 | 1.000 | 0.143 | −0.218 | −0.039 | 0.008 | −0.051 | 0.028 | −0.008 | 0.009 | 0.122 | 0.165 | 0.012 | 0.211 | 0.104 |
| BI | −0.095 | 0.143 | 1.000 | 0.260 | −0.370 * | −0.442 * | 0.385 * | 0.547 ** | 0.175 | 0.041 | 0.030 | 0.245 | 0.175 | 0.256 | −0.007 |
| MEC-Lobo | −0.374 * | −0.218 | 0.260 | 1.000 | 0.069 | 0.019 | −0.057 | 0.041 | 0.235 | 0.090 | 0.071 | −0.014 | 0.087 | −0.091 | 0.095 |
| NHPT-R | −0.151 | −0.039 | −0.370 * | 0.069 | 1.000 | 0.878 ** | −0.827 ** | −0.780 ** | −0.122 | −0.259 | 0.190 | 0.141 | 0.077 | 0.072 | −0.259 |
| NHPT-L | −0.055 | 0.008 | −0.442 * | 0.019 | 0.878 ** | 1.000 | −0.782 ** | −0.785 ** | −0.121 | −0.211 | 0.251 | 0.189 | 0.211 | 0.160 | −0.288 |
| BBT-R | 0.202 | −0.051 | 0.385 | −0.057 | −0.827 ** | −0.782 ** | 1.000 | 0.943 ** | 0.142 | 0.236 | −0.068 | −0.185 | −0.084 | −0.060 | 0.246 |
| BBT-L | 0.064 | 0.028 | 0.547 ** | 0.041 | −0.780 ** | −0.785 ** | 0.943 ** | 1.000 | 0.127 | 0.296 | −0.052 | −0.107 | −0.073 | −0.007 | 0.234 |
| GPQoL | −0.062 | −0.008 | 0.175 | 0.235 | −0.122 | −0.121 | 0.142 | 0.127 | 1.000 | 0.397 * | 0.349 | 0.106 | 0.442 * | 0.455 * | −0.084 |
| GPH | −0.053 | 0.009 | 0.041 | 0.090 | −0.259 | −0.211 | 0.236 | 0.296 | 0.397 * | 1.000 | 0.090 | 0.060 | 0.246 | 0.285 | 0.011 |
| PH | 0.171 | 0.122 | 0.030 | 0.071 | 0.190 | 0.251 | −0.068 | −0.052 | 0.349 | 0.090 | 1.000 | 0.317 | 0.355 | 0.580 ** | −0.065 |
| PsH | 0.024 | 0.165 | 0.245 | −0.014 | 0.141 | 0.189 | −0.185 | −0.107 | 0.106 | 0.060 | 0.317 | 1.000 | 0.668 ** | 0.772 ** | −0.124 |
| SR | −0.082 | 0.012 | 0.175 | 0.087 | 0.077 | 0.211 | −0.084 | −0.073 | 0.442 * | 0.246 | 0.355 | 0.668 ** | 1.000 | 0.819 ** | −0.039 |
| E | 0.104 | 0.211 | 0.256 | −0.091 | 0.072 | 0.160 | −0.060 | −0.007 | 0.455 * | 0.285 | 0.580 ** | 0.772 ** | 0.819 ** | 1.000 | −0.134 |
| CSQ-8 | 0.416 * | 0.104 | −0.007 | 0.095 | −0.259 | −0.288 | 0.246 | 0.234 | −0.084 | 0.011 | −0.065 | −0.124 | −0.039 | −0.134 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zegarra-Ramos, M.H.; García-Bravo, C.; Huertas-Hoyas, E.; Fernández-Gómez, G.; Rodríguez-Pérez, M.P.; Pérez-Corrales, J.; García-Bravo, S. The Effectiveness and Usability of a Rehabilitation Program Using the Nintendo Switch to Promote Healthy Aging in Older People with Cognitive Impairment: A Randomized Clinical Trial. Healthcare 2024, 12, 672. https://doi.org/10.3390/healthcare12060672
Zegarra-Ramos MH, García-Bravo C, Huertas-Hoyas E, Fernández-Gómez G, Rodríguez-Pérez MP, Pérez-Corrales J, García-Bravo S. The Effectiveness and Usability of a Rehabilitation Program Using the Nintendo Switch to Promote Healthy Aging in Older People with Cognitive Impairment: A Randomized Clinical Trial. Healthcare. 2024; 12(6):672. https://doi.org/10.3390/healthcare12060672
Chicago/Turabian StyleZegarra-Ramos, Melissa Helen, Cristina García-Bravo, Elisabet Huertas-Hoyas, Gemma Fernández-Gómez, Mª Pilar Rodríguez-Pérez, Jorge Pérez-Corrales, and Sara García-Bravo. 2024. "The Effectiveness and Usability of a Rehabilitation Program Using the Nintendo Switch to Promote Healthy Aging in Older People with Cognitive Impairment: A Randomized Clinical Trial" Healthcare 12, no. 6: 672. https://doi.org/10.3390/healthcare12060672
APA StyleZegarra-Ramos, M. H., García-Bravo, C., Huertas-Hoyas, E., Fernández-Gómez, G., Rodríguez-Pérez, M. P., Pérez-Corrales, J., & García-Bravo, S. (2024). The Effectiveness and Usability of a Rehabilitation Program Using the Nintendo Switch to Promote Healthy Aging in Older People with Cognitive Impairment: A Randomized Clinical Trial. Healthcare, 12(6), 672. https://doi.org/10.3390/healthcare12060672