

“I’m Not Only a Body”: Change in Thoughts about the Body after Mirror Exposure Treatment in Women with Obesity—An Exploratory Study
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
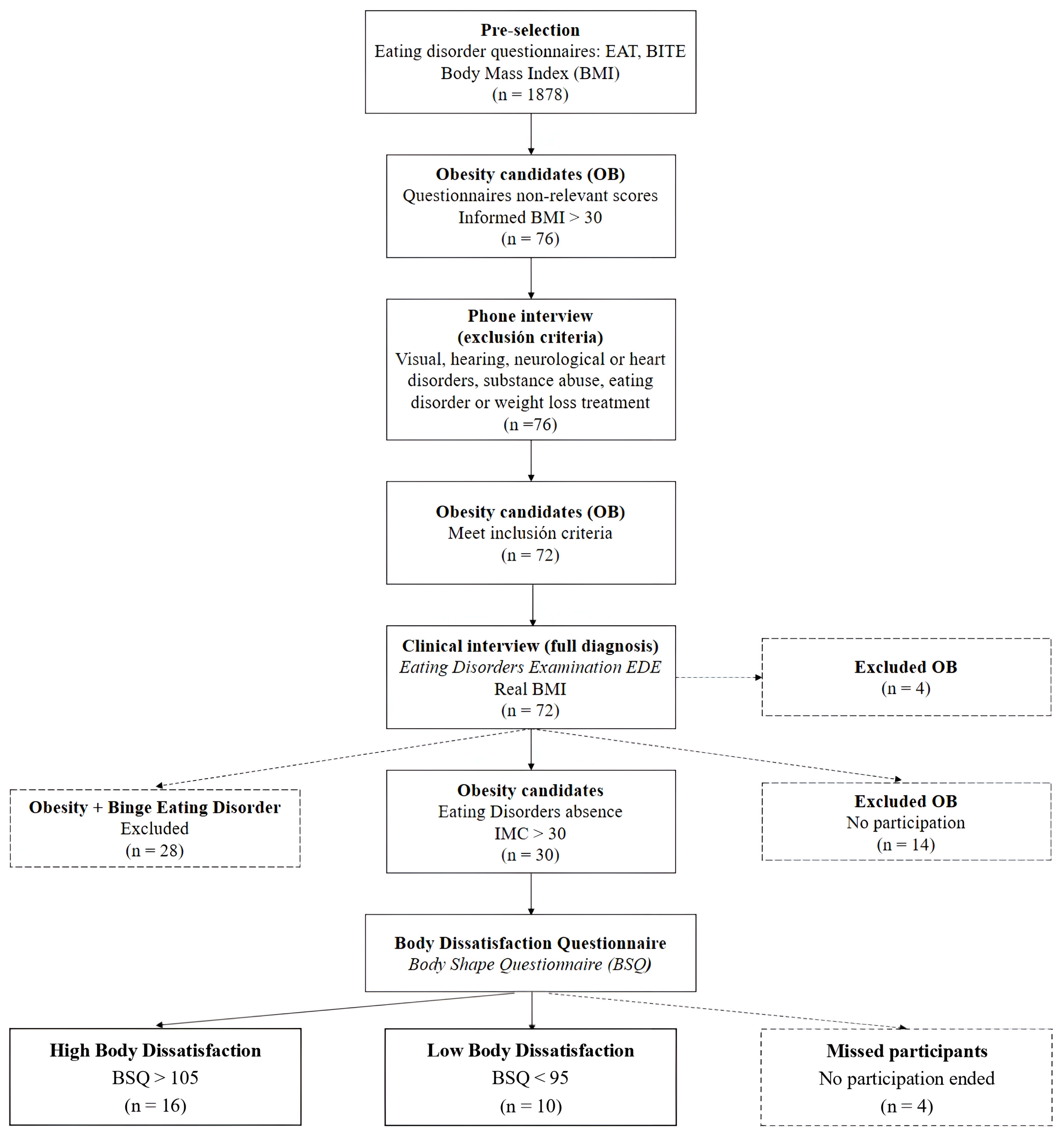
2.1. Participants
2.2. Procedure
2.3. Treatment
2.4. Measures
2.5. Analysis
3. Results
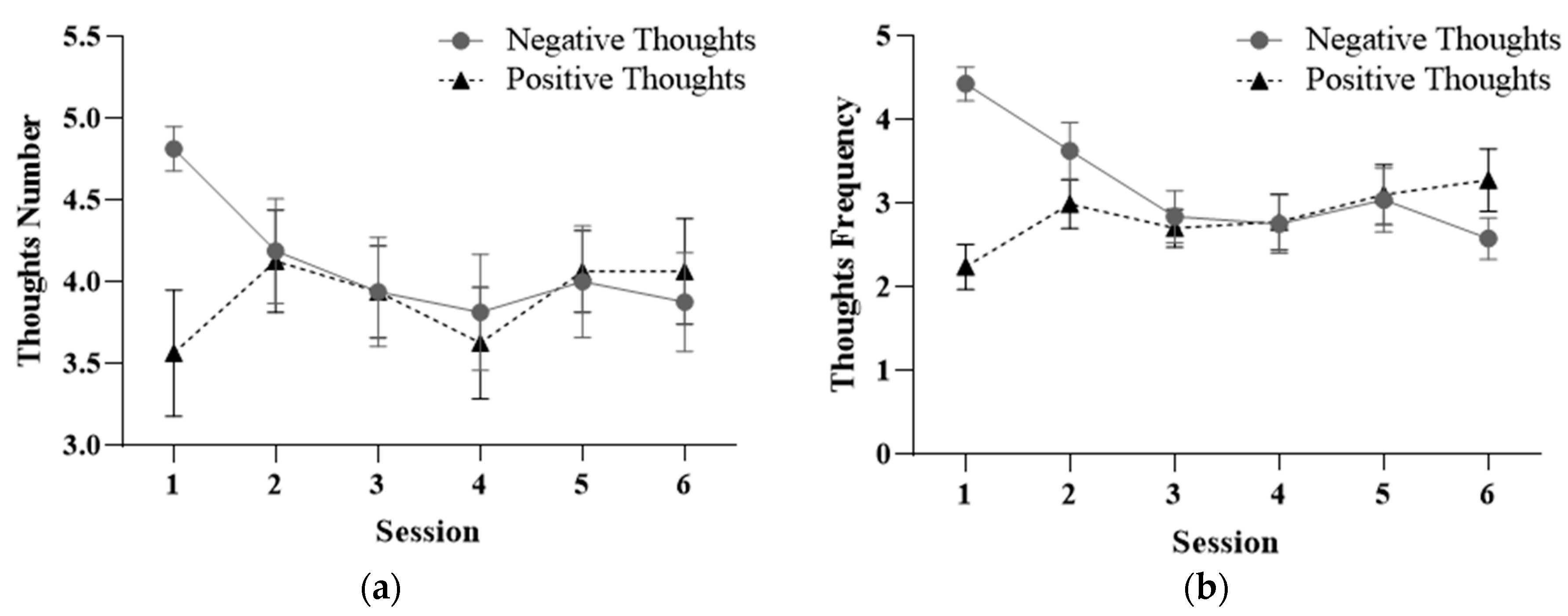
3.1. Negative and Positive Thoughts
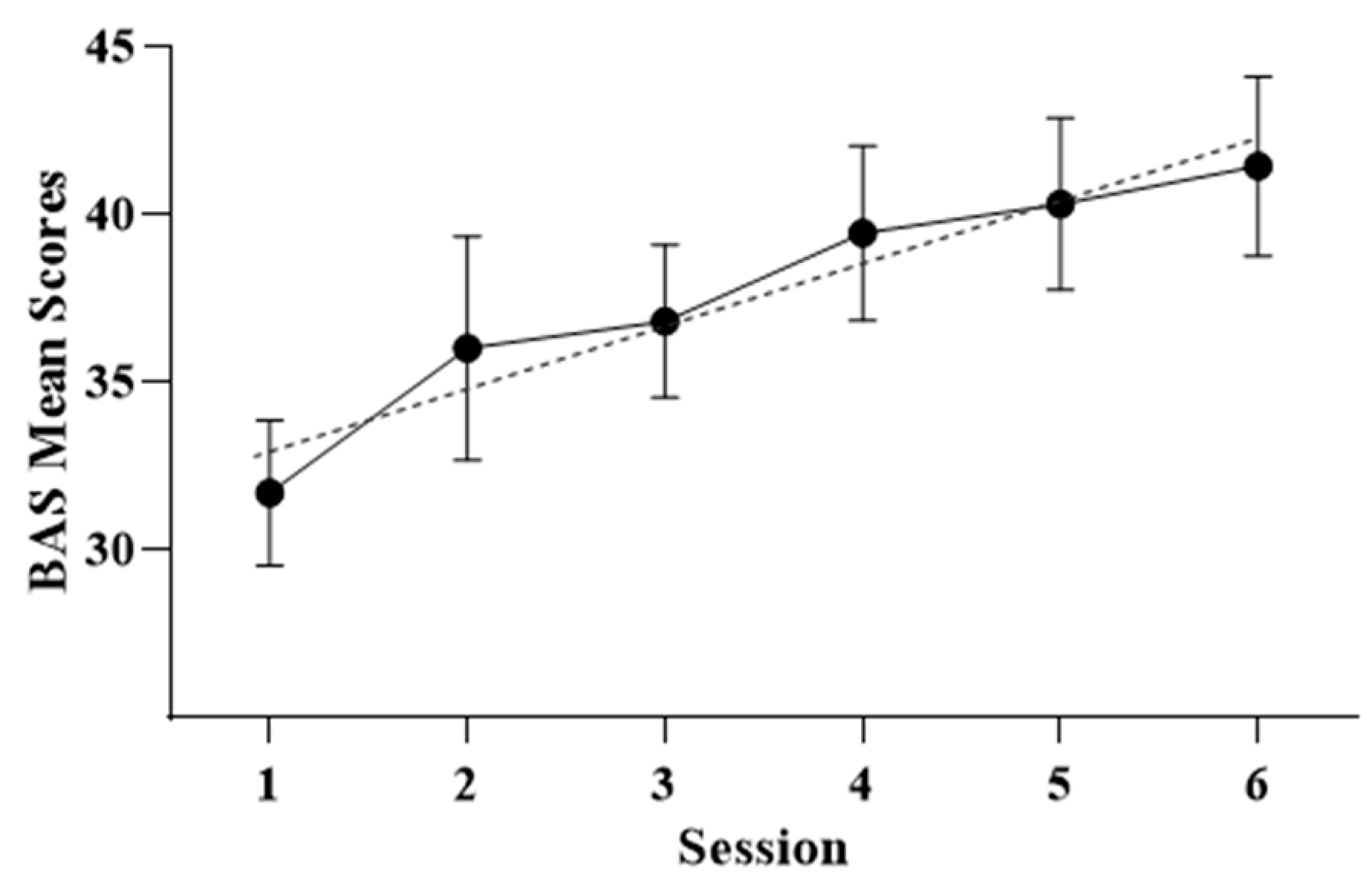
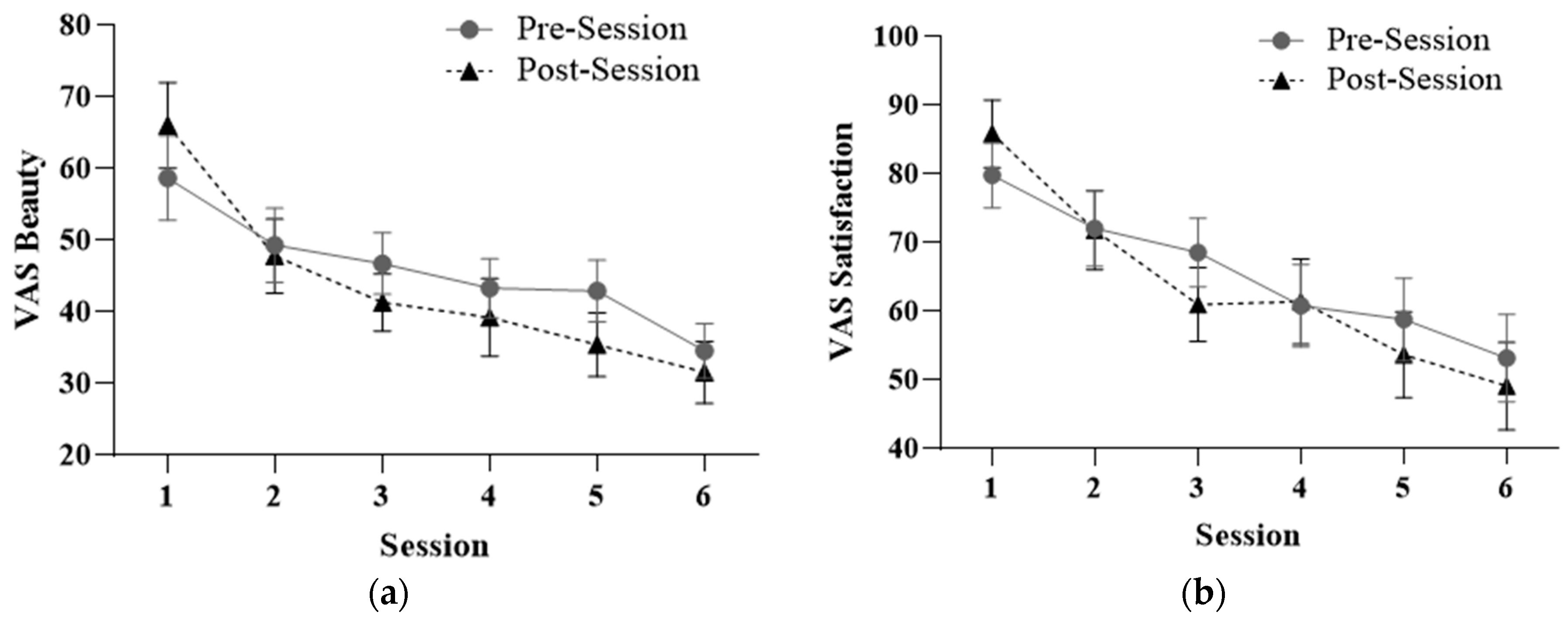
3.2. Body Satisfaction and Perceptions
3.3. Treatment Results
3.4. About Thoughts
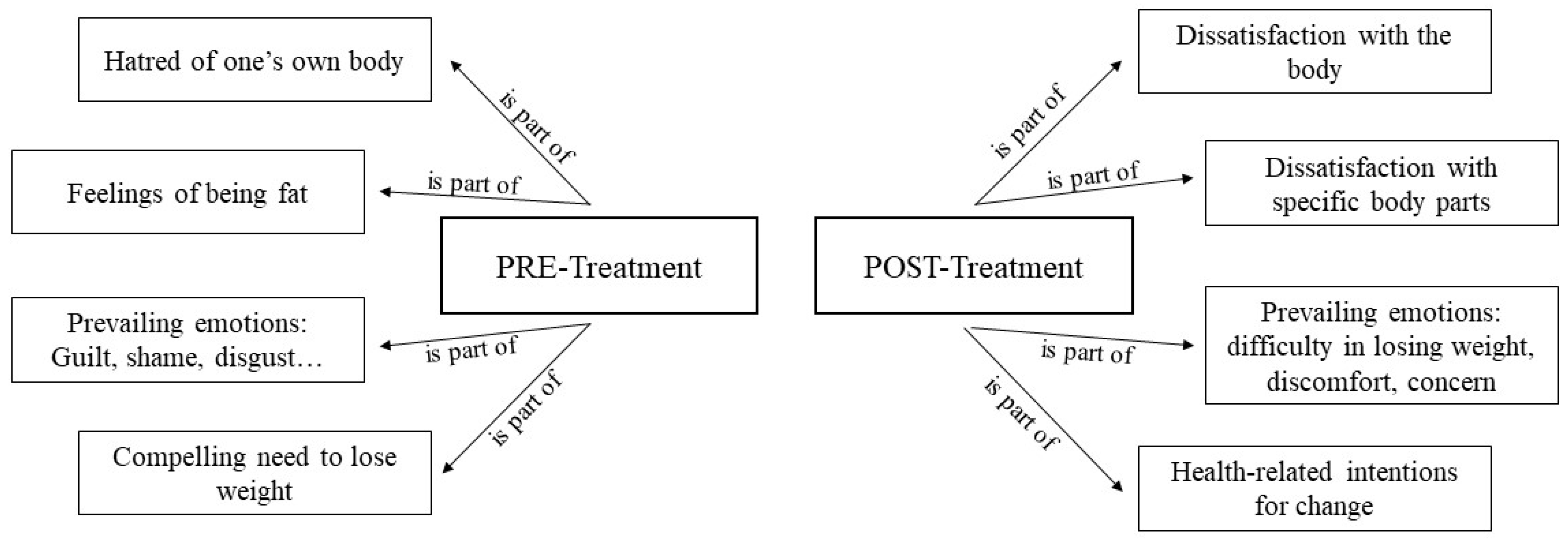
3.4.1. Negative Thoughts in High Body Dissatisfaction
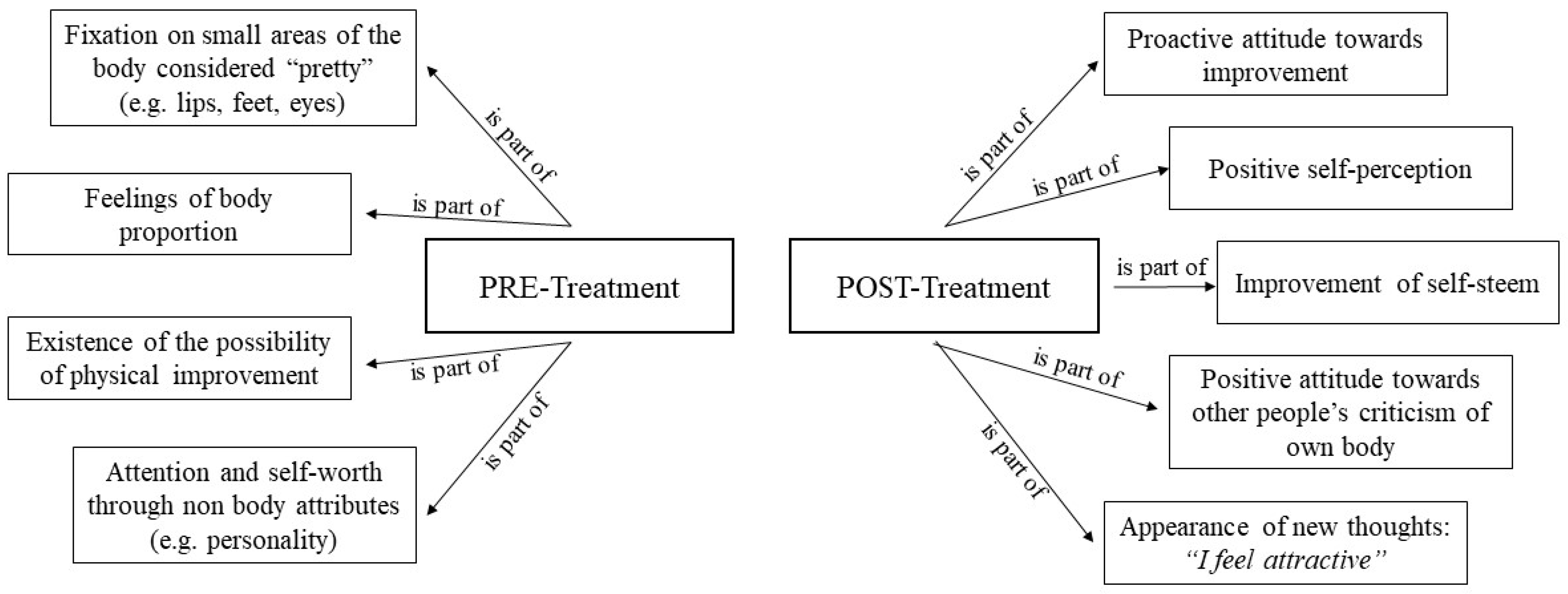
3.4.2. Positive Thoughts in High Body Dissatisfaction
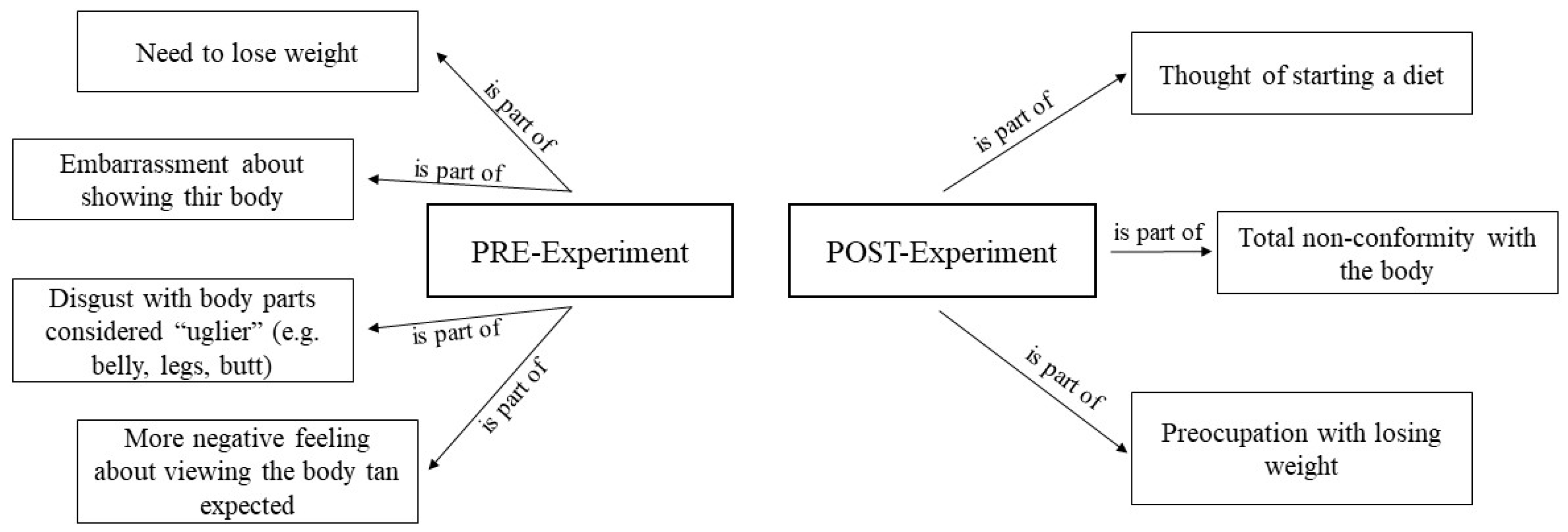
3.4.3. Negative Thoughts in Low Body Dissatisfaction (Control Group)
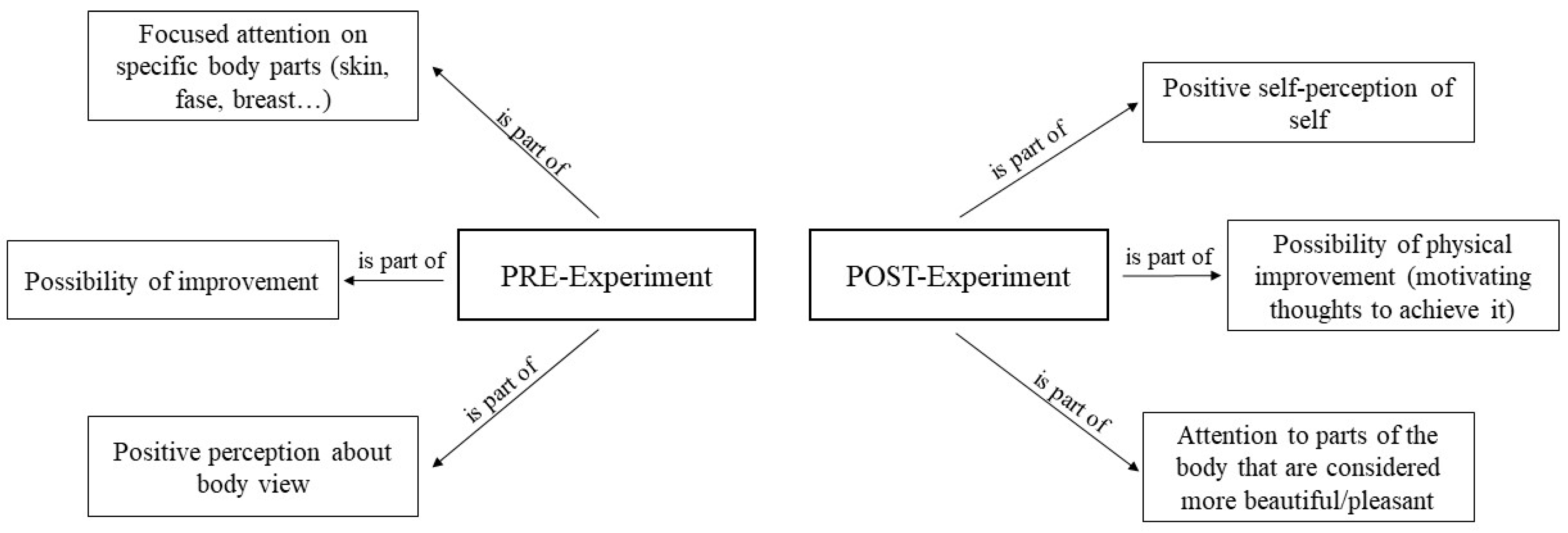
3.4.4. Positive Thoughts in Low Body Dissatisfaction (Control Group)
4. Discussion
5. Limitations and Future Research
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, Pathophysiology, and Management of Obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef]
- Chandler, M.; Cunningham, S.; Lund, E.M.; Khanna, C.; Naramore, R.; Patel, A.; Day, M.J. Obesity and Associated Comorbidities in People and Companion Animals: A One Health Perspective. J. Comp. Pathol. 2017, 156, 296–309. [Google Scholar] [CrossRef] [PubMed]
- Ghanemi, A.; St-Amand, J. Redefining obesity toward classifying as a disease. Eur. J. Intern. Med. 2018, 55, 20–22. [Google Scholar] [CrossRef]
- World Health Organization Media Centre. Obesity and Overweight; WHO: Geneva, Switzerland, 2016; pp. 1–5.
- Busutil, R.; Espallardo, O.; Torres, A.; Martínez-Galdeano, L.; Zozaya, N.; Hidalgo-Vega, A. The impact of obesity on health-related quality of life in Spain. Health Qual. Life Outcomes 2017, 15, 197. [Google Scholar] [CrossRef] [PubMed]
- INE—Instituto Nacional de Estadística. Encuesta Europea de Salud en España 2020; INE-MSCBS: Kyoto, Japan, 2020; Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176784&menu=resultados&idp=1254735573175 (accessed on 23 October 2023).
- Konttinen, H. Emotional eating and obesity in adults: The role of depression, sleep and genes. Proc. Nutr. Soc. 2020, 79, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Minhas, M.; Murphy, C.M.; Balodis, I.M.; Samokhvalov, A.V.; MacKillop, J. Food addiction in a large community sample of Canadian adults: Prevalence and relationship with obesity, body composition, quality of life and impulsivity. Addiction 2021, 116, 2870–2879. [Google Scholar] [CrossRef]
- Rodríguez-Martín, B.C.; Meule, A. Food craving: New contributions on its assessment, moderators, and consequences. Front. Psychol. 2015, 6, 21. [Google Scholar] [CrossRef]
- Keery, H.; van den Berg, P.; Thompson, J.K. An evaluation of the Tripartite Influence Model of body dissatisfaction and eating disturbance with adolescent girls. Body Image 2004, 1, 237–251. [Google Scholar] [CrossRef]
- Reinehr, T. Long-term effects of adolescent obesity: Time to act. Nat. Rev. Endocrinol. 2018, 14, 183–188. [Google Scholar] [CrossRef]
- Thompson, J.K.; Heinberg, L.J.; Altabe, M.; Tantleff-Dunn, S. Exacting Beauty: Theory, Assessment, and Treatment of Body Image Disturbance; American Psychological Association: Washington, DC, USA, 1999. [Google Scholar]
- Hockey, A.; Barlow, F.K.; Shiels, A.L.; Donovan, C.L. Body dissatisfaction in midlife women: The applicability of the tripartite influence model. Body Image 2021, 39, 202–212. [Google Scholar] [CrossRef]
- Verplanken, B.; Tangelder, Y. No body is perfect: The significance of habitual negative thinking about appearance for body dissatisfaction, eating disorder propensity, self-esteem and snacking. Psychol. Health 2011, 26, 685–701. [Google Scholar] [CrossRef]
- Naumann, A.; Biehl, A.; Svaldi, J. Eye-tracking study on the effects of happiness and sadness on body dissatisfaction and selective visual attention during mirror exposure in bulimia nervosa. Eat. Disord. 2019, 52, 895–903. [Google Scholar] [CrossRef]
- Smeets, E.; Jansen, A.; Roefs, A. Bias for the (un) Attractive Self: On the role of attention in causing body (dis)Satisfaction. Health Psychol. 2011, 30, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M.; Garfinkel, P.E. Body Image in anorexia nervosa: Measurement, theory, and clinical implications. Int. J. Psychiatry Med. 1981, 11, 263–284. [Google Scholar] [CrossRef] [PubMed]
- Olson, K.L.; Thaxton, T.T.; Emery, C.F. Targeting body dissatisfaction among women with overweight or obesity: A proof-of-concept pilot study. Int. J. Eat. Disord. 2018, 51, 973–977. [Google Scholar] [CrossRef]
- Griffen, T.C.; Naumann, E.; Hildebrant, T. Mirror exposure therapy for body image disturbances and eating disorders: A review. Clin. Psychol. Rev. 2018, 65, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Jansen, A.; Voorwinde, V.; Hoebink, Y.; Rekkers, M.; Martijn, C.; Mulkens, S. Mirror exposure to increase body satisfaction: Sgould we guide the focus of attention towards positively or negatively evaluated body parts? J. Behav. Ther. Exp. Psychiatry 2016, 50, 90–96. [Google Scholar] [CrossRef] [PubMed]
- McLean, S.A.; Paxton, S.J. Body Image in the Context of Eating Disorders. Psychyatr. Clin. 2019, 42, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Brandt, H.A.; Crawford, S.F. Eating Disorders 2018: New Insights in Diagnosis, Research and Treatment. Psychiatr. Clin. 2019, 42, xiii–xv. [Google Scholar] [CrossRef] [PubMed]
- Portela de Santana, M.L.; da Costa, H.; Mora, M.; Raich, R.M. La epidemiología y los factores de riesgo de los trastornos alimentarios en la adolescencia: Una revisión. Nutr. Hosp. 2012, 27, 391–401. [Google Scholar]
- Cooper, P.J.; Taylor, M.J.; Cooper, Z.; Fairburn, C.G. The development and validation of the Body Shape Questionnaire. Int. J. Eat. Disord. 1987, 6, 485–494. [Google Scholar] [CrossRef]
- Sepúlveda, A.; León, J. Aspectos controvertidos de la imagen corporal en los trastornos de la conducta alimentaria. Clínica Salud 2004, 15, 55–74. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Knowles, K.A.; Olatunki, B.O. Enhancing inhibitory learning: The utility of variability in exposure. Cogn. Behav. Pract. 2019, 26, 186–200. [Google Scholar] [CrossRef] [PubMed]
- Baur, J.; Krohmer, K.; Naumann, E.; Tuschen-Caffier, B.; Svaldi, J. Vocal arousal: A physiological correlate of body distress in women with overweight and obesity. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2020, 25, 1161–1169. [Google Scholar] [CrossRef]
- Mulkens, S.; Jansen, A. Mirror gazing increase attractiveness in satisfied, but not in dissatisfied women: A model for body dysmorphic disorder? J. Behav. Ther. Exp. Psychiatry 2009, 40, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Knejzlíková, T.; Světlák, M.; Malatincová, T.; Roman, R.; Chládek, J.; Najmanová, J.; Theiner, P.; Linhartová, P.; Kašpárek, T. Electrodermal Response to Mirror Exposure in Relation to Subjective Emotional Responses, Emotional Competences and Affectivity in Adolescent Girls with Restrictive Anorexia and Healthy Controls. Front. Psychol. 2021, 10, 673597. [Google Scholar] [CrossRef]
- Díaz-Ferrer, S.; Rodríguez-Ruiz, S.; Ortega-Robles, B.; Mata-Martín, J.L.; Fernández-Santaella, M.C. Psychophysiological changes during pure vs. guided Mirror Exposure therapies in women with High Body dissatisfaction: What are they learning about their Bodies? Eur. Eat. Disord. Rev. 2017, 25, 562–569. [Google Scholar] [CrossRef]
- Trentowska, M.; Bender, C.; Tuschen-Caffier, B. Mirror exposure in women with bulimic symptoms: How do thoughts and emotions change in a body image treatment? Behav. Res. Ther. 2013, 51, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Agüera, Z.; Jiménez-Murcia, S. Advances in Eating Disorders. J. Clin. Med. 2020, 9, 4047. [Google Scholar] [CrossRef]
- Klimek, P.; Wei, B.; Blashill, A.J. Exploring moderators of mirror exposure on pre- to post changes in body image outcomes: Systematic review and meta-analysis. Eat. Disord. 2020, 30, 77–98. [Google Scholar] [CrossRef]
- Quittkat, H.L.; Hartmann, A.S.; Düsing, R.; Buhlmann, U.; Vocks, S. Body Dissatisfaction, Importance of Appearance, and Body Appreciation in Men and Women Over the Lifespan. Front. Psychiatry 2019, 10, 864. [Google Scholar] [CrossRef]
- Barbeau, K.; Guertin, C.; Boileau, K.; Pelletier, L. The Effects of Self-Compassion and Self-Esteem Writing Interventions on Women’s Valuation of Weight Management Goals, Body Appreciation, and Eating Behaviors. Psychol. Women Q. 2021, 46, 82–98. [Google Scholar] [CrossRef]
- Avalos, L.C.; Tylka, T.L.; Wood-Barcalow, N. The Body Appreciation Scale: Development and psychometric evaluation. Body Image 2005, 2, 285–297. [Google Scholar] [CrossRef]
- Raich, R.; Mora, M.; Soler, A.; Avila, C.; Clos, I.; Zapater, L. Adaptación de un instrumento de evaluación de la insatisfacción corporal. Clínica Salud 1996, 7, 51–66. [Google Scholar]
- Jáuregui, L.; Bolaños, R. Spanish version of the body appreciation scale (BAS) for adolescents. Span. J. Psychol. 2011, 14, 411–420. [Google Scholar] [CrossRef]
- Berg, B.L. Qualitative Research Methods for the Social Sciences, 5th ed.; Pearson: Boston, MA, USA, 2004. [Google Scholar]
- Creswell, J.W.; Poth, C.N. Qualitative Inquiry and Research Design Choosing among Five Approaches, 4th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Franzosi, R. From Words to Numbers; Narrative, Data, and Social Science; Cambridge University Press: New York, NY, USA, 2004. [Google Scholar]
- Mayring, P. Qualitative Content Analysis: Theoretical Foundation, Basic Procedures and Software Solution; Gesis: Klagenfurt, Austria, 2014; Available online: https://nbnresolving.org/urn:nbn:de:0168-ssoar-395173 (accessed on 15 September 2023).
- González-Sánchez, C.; Díaz-Ferrer, S.; Aristizabal, J.A.; Mata-Martín, J.L.; Rodríguez-Ruiz, S. I Look at my whole body and I feel better: Attentional bias, emotional and psychophysiological response by pure exposure treatment in women with obesity. Psychother. Res. 2022, 32, 748–762. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Domínguez, S.; Rodríguez-Ruiz, S.; Fernández-Santaella, M.C.; Jansen, A.; Tuschen-Caffier, B. Pure versus guided mirror exposure to reduce body dissatisfaction: A preliminary study with university women. Body Image 2012, 9, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Hilbert, A.; Tuschen-Caffier, B.; Vögele, C. Effects of prolongued and repeated body image exposure in binge-eating disorder. J. Psychosom. Res. 2002, 52, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Craske, M.G.; Treanor, M.; Conway, C.C.; Zbozinek, T.; Vervliete, B. Maximizing exposure therapy: An inhibitory learning approach. Behav. Res. Ther. 2014, 58, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Foa, E.B.; Kozak, M.J. Emotional processing of fear: Exposure to corrective information. Psychol. Bull. 1986, 99, 20–35. [Google Scholar] [CrossRef] [PubMed]
- Linardon, J. Positive body image, intuitive eating, and self-compassion protect against the onset of the core symptoms of eating disorders. A prospective study. Int. J. Eat. Disord. 2021, 54, 1967–1977. [Google Scholar] [CrossRef] [PubMed]
- Tanck, J.A.; Hartmann, A.S.; Svaldi, J.; Hagena, S.; Osen, B.; Stierle, C.; Vocks, S. What happens in the course of positive mirror exposure? Effects on eating pathology, body satisfaction, affect, and subjective physiological arousal in patients with anorexia and bulimia nervosa. Eur. Eat. Disord. Rev. 2022, 30, 797–814. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, A.S.; Naumann, E.; Vocks, S.; Svaldi, J.; Werthmann, J. Body Exposure, its Forms of Delivery and Potentially Associated Working Mechanisms: How to Move the Field Forward. Clin. Psychol. Eur. 2021, 3, e3813. [Google Scholar] [CrossRef] [PubMed]
- Butler, R.; Heimberg, R.G. Exposure therapy for eating disorders: A systematic review. Clin. Psychol. Rev. 2020, 778, 101851. [Google Scholar] [CrossRef]
- Schaumberg, K.; Reilly, E.E.; Gorrell, S.; Levinson, C.A.; Farrell, N.R.; Brown, T.A.; Smith, K.M.; Schaefer, L.M.; Essayli, J.H.; Haynos, A.F.; et al. Conceptualizing eating disorder psychopathology using an anxiety disorders framework: Evidence and implications for exposure-based clinical research. Clin. Psychol. Rev. 2021, 83, 101952. [Google Scholar] [CrossRef]
- Mirabella, M.; Giovanardi, G.; Fortunato, A.; Senofonte, G.; Lombardo, F.; Lingiardi, V.; Speranza, A.M. The Body I Live in. Perceptions and Meanings of Body Dissatisfaction in Young Transgender Adults: A Qualitative Study. J. Clin. Med. 2020, 9, 3733. [Google Scholar] [CrossRef]
- Calugi, S.; Segattini, B.; Cattaneo, G.; Chimini, M.; Dalle, A.; Dametti, L.; Molgora, M.; Dalle, R. Weight Bias Internalization and Eating Disorder Psychopathology in Treatment-Seeking Patients with Obesity. Nutrients 2023, 15, 2932. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group | Experimental Group | |||||||
|---|---|---|---|---|---|---|---|---|
| Clinical Measures | Pre-Treatment | Post-Treatment | T | p Value | Pre-Treatment | Post-Treatment | T | p Value |
| BSQ | 69.60 (17.27) | 73.40 (25.36) | −0.742 | 0.477 | 147.06 (25.88) | 120.19 (40.19) | 2.440 | 0.280 |
| BAS | 50.00 (7.51) | 50.00 (7.51) | 0.445 | 0.668 | 32.38 (8.93) | 42.19 (13.56) | 2.996 | 0.010 * |
| VAS–beauty | 22.40 (15.52) | 27.11 (16.09) | −0.492 | 0.636 | 64.37 (25.88) | 28.50 (17.91) | 5.075 | 0.000 *** |
| VAS–satisfaction | 18.10 (15.84) | 33.22 (15.77) | −2.507 | 0.037 * | 73.93 (24.27) | 47.00 (26.45) | 2.77 | 0.000 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Sánchez, C.; Jiménez-Cabello, J.; Rodríguez-Ruíz, S.; Mata-Martín, J.L. “I’m Not Only a Body”: Change in Thoughts about the Body after Mirror Exposure Treatment in Women with Obesity—An Exploratory Study. Healthcare 2024, 12, 624. https://doi.org/10.3390/healthcare12060624
González-Sánchez C, Jiménez-Cabello J, Rodríguez-Ruíz S, Mata-Martín JL. “I’m Not Only a Body”: Change in Thoughts about the Body after Mirror Exposure Treatment in Women with Obesity—An Exploratory Study. Healthcare. 2024; 12(6):624. https://doi.org/10.3390/healthcare12060624
Chicago/Turabian StyleGonzález-Sánchez, Cristina, José Jiménez-Cabello, Sonia Rodríguez-Ruíz, and José Luis Mata-Martín. 2024. "“I’m Not Only a Body”: Change in Thoughts about the Body after Mirror Exposure Treatment in Women with Obesity—An Exploratory Study" Healthcare 12, no. 6: 624. https://doi.org/10.3390/healthcare12060624
APA StyleGonzález-Sánchez, C., Jiménez-Cabello, J., Rodríguez-Ruíz, S., & Mata-Martín, J. L. (2024). “I’m Not Only a Body”: Change in Thoughts about the Body after Mirror Exposure Treatment in Women with Obesity—An Exploratory Study. Healthcare, 12(6), 624. https://doi.org/10.3390/healthcare12060624