
Perceptions and Experiences of Parents of Burn-Injured Children during Hospital Stay: A Need for Integrated Care



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Research Team
2.3. Setting
2.4. Participants and Procedure
2.5. Ethics
2.6. Data Analysis
3. Results
3.1. Participants Characteristics
3.2. Themes
3.3. Diving into the Crisis of the Child Burn Injury
3.3.1. Negative Trauma Responses
3.3.2. Facing Medical Procedures
3.3.3. Changes in the Child’s Functioning
3.3.4. COVID-19 Stressors
3.3.5. Unmet Needs
3.4. Being Together and in Good Hands
3.4.1. Child’s Well-Being and Recovery
3.4.2. Quality of Healthcare and Environment
3.5. Becoming Aware of an Uncertain Future
3.5.1. Ongoing Suffering of the Child and (Potential) Permanent Scarring
3.5.2. Concerns about Being Blamed and That a Burn Might Happen Again
3.6. Enhancing Supportive Care and Environment
3.6.1. Strengthening Support and Adapting the Care Plan
3.6.2. Improvement of Hospital Facilities
3.7. Finding Ways to Guide Parents
3.7.1. Maintaining a Positive Mindset and Activating Coping Resources
3.7.2. Recognizing Parental Distress and Promoting Child’s Well-Being
3.7.3. Raising Awareness
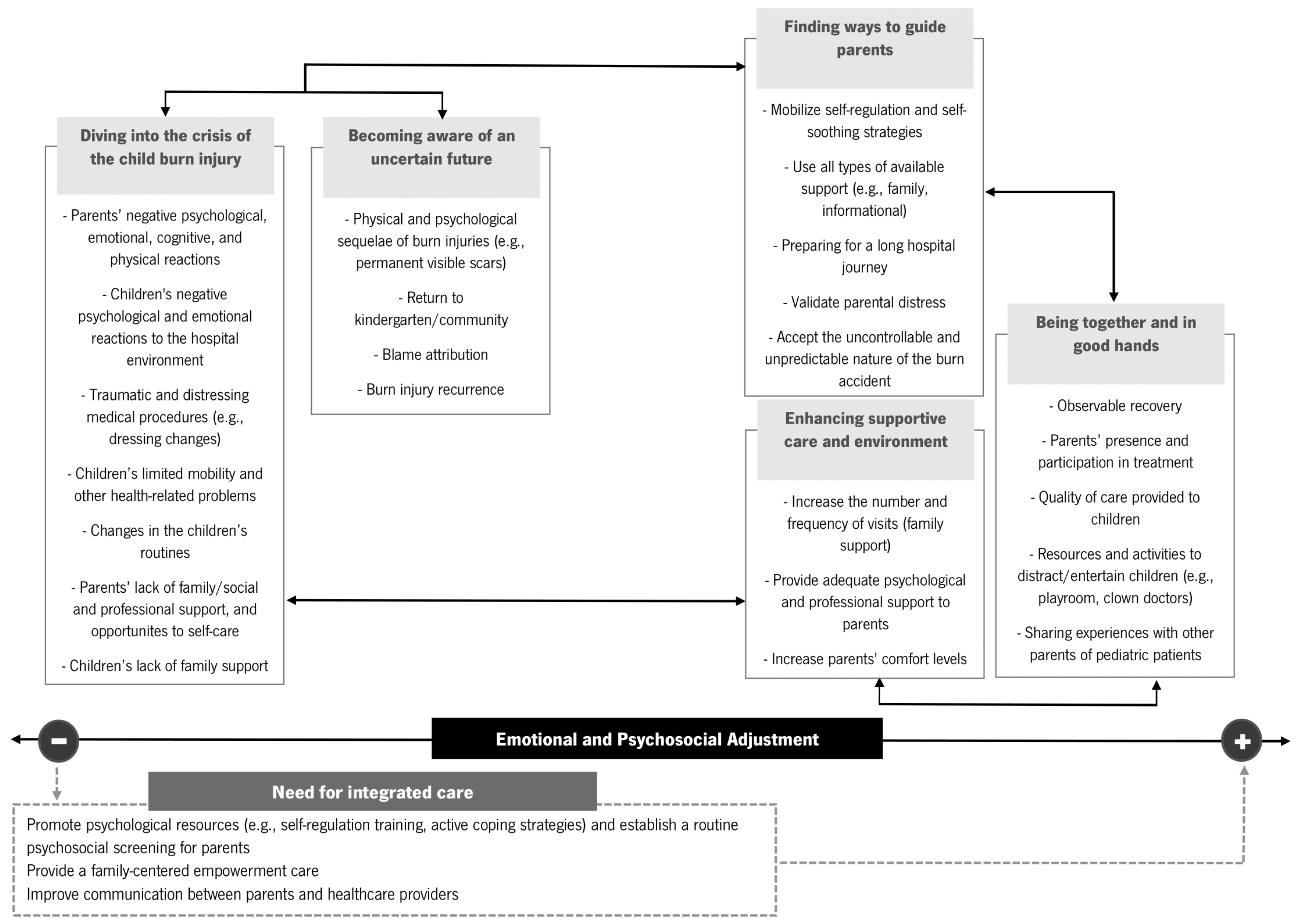
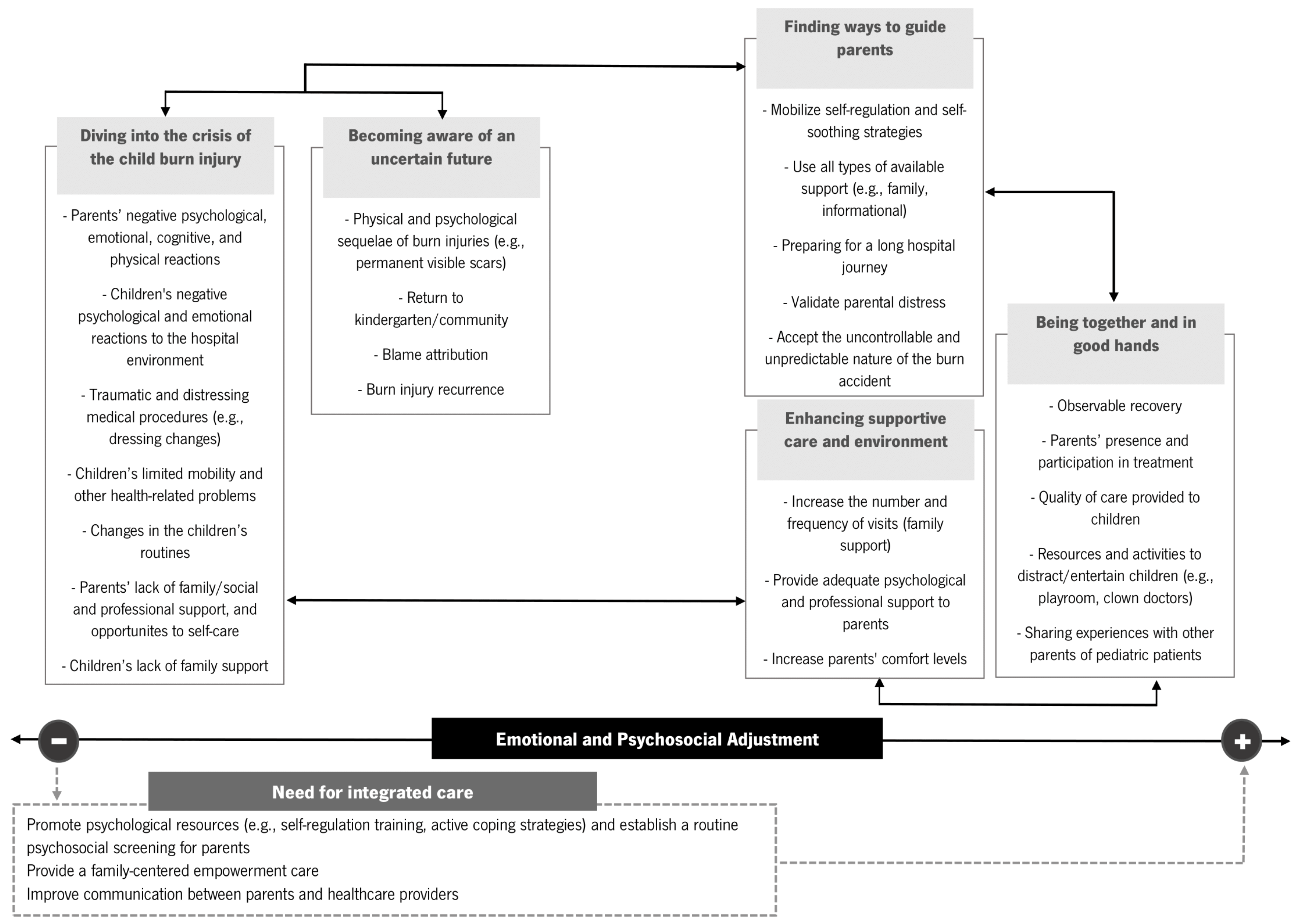
3.8. Summary of the Results and Goals for Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smolle, C.; Cambiaso-Daniel, J.; Forbes, A.A.; Wurzer, P.; Hundeshagen, G.; Branski, L.K.; Huss, F.; Kamolz, L.P. Recent trends in burn epidemiology worldwide: A systematic review. Burns 2017, 43, 249–257. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/burns (accessed on 7 February 2024).
- Yakupu, A.; Zhang, J.; Dong, W.; Song, F.; Dong, J.; Lu, S. The epidemiological characteristic and trends of burns globally. BMC Public Health 2022, 22, 1596. [Google Scholar] [CrossRef] [PubMed]
- Price, K.; Lee, K.C.; Woolley, K.E.; Falk, H.; Peck, M.; Lilford, R.; Moiemen, N. Burn injury prevention in low- and middle- income countries: Scoping systematic review. Burn. Trauma 2021, 9, tkab037. [Google Scholar] [CrossRef] [PubMed]
- Ter Meulen, E.W.; Poley, M.J.; Van Dijk, M.; Rogers, A.D.; Rode, H. The hospital costs associated with acute paediatric burn injuries. S. Afr. Med. J. 2016, 106, 1120–1124. [Google Scholar] [CrossRef] [PubMed]
- Van Balen, N.I.M.; Simon, M.H.; Botman, M.; Bloemers, F.W.; Schoonmade, L.J.; Meij-de Vries, A. Effectiveness of prevention programmes on the rate of burn injuries in children: A systematic review. Inj. Prev. 2023, 30, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Emond, A.; Sheahan, C.; Mytton, J.; Hollén, L. Developmental and behavioural associations of burns and scalds in children: A prospective population-based study. Arch. Dis. Child. 2016, 102, 428–483. [Google Scholar] [CrossRef] [PubMed]
- Kemp, A.M.; Jones, S.; Lawson, Z.; Maguire, S.A. Patterns of burns and scalds in children. Arch. Dis. Child. 2014, 99, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Suman, A.; Owen, J. Update on the management of burns in paediatrics. BJA Educ. 2020, 20, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Wickens, N.; van Rensburg, E.J.; de Gouveia Belinelo, P.; Milroy, H.; Martin, L.; Wood, F.; Woolard, A. “It’s a big trauma for the family”: A qualitative insight into the psychological trauma of paediatric burns from the perspective of mothers. Burns 2024, 50, 262–274. [Google Scholar] [CrossRef]
- Krasnoff, C.C.; Grigorian, A.; Chin, T.; Joe, V.; Kong, A.; Barrios, C.; Kuza, C.M.; Nahmias, J. Pediatric burn-trauma patients have increased length of stay compared to trauma-only patients: A propensity matched analysis. Burns 2021, 47, 78–83. [Google Scholar] [CrossRef]
- Hop, M.J.; Polinder, S.; van der Vlies, C.H.; Middelkoop, E.; van Baar, M.E. Costs of burn care: A systematic review. Wound Repair Regen 2014, 22, 436–450. [Google Scholar] [CrossRef]
- Santos, J.V.; Oliveira, A.; Costa-Pereira, A.; Amarante, J.; Freitas, A. Burden of burns in Portugal, 2000–2013: A clinical and economic analysis of 26,447 hospitalisations. Burns 2016, 42, 891–900. [Google Scholar] [CrossRef]
- Santos, J.V.; Viana, J.; Oliveira, A.; Ramalho, A.; Sousa-Teixeira, J.; Duke, J.; Amarante, J.; Freitas, A. Hospitalisations with burns in children younger than five years in Portugal, 2011–2015. Burns 2019, 45, 1223–1230. [Google Scholar] [CrossRef]
- Bakker, A.; Maertens, K.J.; Van Son, M.J.; Van Loey, N.E. Psychological consequences of pediatric burns from a child and family perspective: A review of the empirical literature. Clin. Psychol. Rev. 2013, 33, 361–371. [Google Scholar] [CrossRef]
- Ciornei, B.; David, V.L.; Popescu, D.; Boia, E.S. Pain Management in Pediatric Burns: A Review of the Science behind It. Glob. Health Epidemiol. Genom. 2023, 2023, e3. [Google Scholar] [CrossRef]
- Patterson, K.N.; Beyene, T.J.; Lehman, K.; VerLee, S.N.; Schwartz, D.; Fabia, R.; Thakkar, R.K. Evaluating effects of burn injury characteristics on quality of life in pediatric burn patients and caregivers. Burns 2023, 49, 1311–1320. [Google Scholar] [CrossRef] [PubMed]
- Spronk, I.; Legemate, C.M.; Polinder, S.; van Baar, M.E. Health-related quality of life in children after burn injuries: A systematic review. J. Trauma Acute Care Surg. 2018, 85, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Lernevall, L.S.T.; Moi, A.L.; Cleary, M.; Kornhaber, R.; Dreyer, P. Support needs of parents of hospitalised children with a burn injury: An integrative review. Burns 2020, 46, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, L.; Centifanti, L.C.; Holman, N.; Taylor, P. Parental adjustment following pediatric burn injury: The role of guilt, shame, and self-compassion. J. Pediatr. Psychol. 2019, 44, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Kornhaber, R.; Childs, C.; Cleary, M. Experiences of guilt, shame and blame in those affected by burns: A qualitative systematic review. Burns 2018, 44, 1026–1039. [Google Scholar] [CrossRef] [PubMed]
- De Young, A.C.; Hendrikz, J.; Kenardy, J.A.; Cobham, V.E.; Kimble, R.M. Prospective Evaluation of Parent Distress Following Pediatric Burns and Identification of Risk Factors for Young Child and Parent Posttraumatic Stress Disorder. J. Child. Adolesc. Psychopharmacol. 2014, 24, 9–17. [Google Scholar] [CrossRef]
- Phillips, C.; Rumsey, N. Considerations for the provision of psychosocial services for families following paediatric burn injury—A quantitative study. Burns 2008, 34, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Egberts, M.R.; van de Schoot, R.; Geenen, R.; Van Loey, N.E.E. Mother, father and child traumatic stress reactions after paediatric burn: Within-family co-occurrence and parent-child discrepancies in appraisals of child stress. Burns 2018, 44, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Willebrand, M.; Sveen, J. Injury-related fear-avoidance and symptoms of posttraumatic stress in parents of children with burns. Burns 2016, 42, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Bayuo, J.; Wong, F.K.Y. Issues and concerns of family members of burn patients: A scoping review. Burns 2021, 47, 503–524. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.; Young, A.; Mitchell, R.; Van, C.; Curtis, K. Experiences and needs of parents of critically injured children during the acute hospital phase: A qualitative investigation. Injury 2017, 48, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Karahan, S.; Ay Kaatsiz, M.A.; Erbas, A.; Kaya, Y. A Qualitative Analysis on the Experiences of Mothers of Children in Burn Intensive Care Unit: “She burned on the outside, me inside…”. J. Burn Care Res. 2023, 45, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.-C. Impact of long-term outcomes on the caregivers of burn survivors. Burns 2023, 49, 317–328. [Google Scholar] [CrossRef]
- Lernevall, L.S.T.; Moi, A.L.; Gjengedal, E.; Dreyer, P. Parents’ lived experiences of parental needs for support at a burn centre. Int. J. Qual. Stud. Health Well-Being 2021, 16, 1855749. [Google Scholar] [CrossRef]
- Ravindran, V.; Rempel, G.R.; Ogilvie, L. Embracing survival: A grounded theory study of parenting children who have sustained burns. Burns 2013, 39, 589–598. [Google Scholar] [CrossRef]
- Rimmer, R.B.; Bay, R.C.; Alam, N.B.; Sadler, I.J.; Richey, K.J.; Foster, K.N.; Caruso, D.M.; Rosenberg, D. Measuring the Burden of Pediatric Burn Injury for Parents and Caregivers. J. Burn Care Res. 2015, 36, 421–427. [Google Scholar] [CrossRef]
- Brown, E.A.; Egberts, M.; Wardhani, R.; De Young, A.; Kimble, R.; Griffin, B.; Storey, K.; Kenardy, J. Parent and Clinician Communication During Paediatric Burn Wound Care: A Qualitative Study. J. Pediatr. Nurs. 2020, 55, 147–154. [Google Scholar] [CrossRef]
- Egberts, M.R.; de Jong, A.E.E.; Hofland, H.W.C.; Geenen, R.; Van Loey, N.E.E. Parental presence or absence during paediatric burn wound care procedures. Burns 2018, 44, 850–860. [Google Scholar] [CrossRef]
- McGarry, S.; Elliott, C.; McDonald, A.; Valentine, J.; Wood, F.; Girdler, S. “This is not just a little accident”: A qualitative understanding of paediatric burns from the perspective of parents. Disabil. Rehabil. 2015, 37, 41–50. [Google Scholar] [CrossRef]
- Egberts, M.R.; Engelhard, I.M.; de Jong, A.E.E.; Hofland, H.W.C.; Geenen, R.; Van Loey, N.E.E. Parents’ memories and appraisals after paediatric burn injury: A qualitative study. Eur. J. Psychotraumatol. 2019, 10, 1615346. [Google Scholar] [CrossRef]
- Bradshaw, C.; Atkinson, S.; Doody, O. Employing a qualitative description approach in health care research. Glob. Qual. Nurs. Res. 2017, 4, 2333393617742282. [Google Scholar] [CrossRef]
- Neergaard, M.A.; Olesen, F.; Andersen, R.S.; Sondergaard, J. Qualitative description–the poor cousin of health research? BMC Med. Res. Methodol. 2009, 9, 52. [Google Scholar] [CrossRef]
- Sandelowski, M. Whatever happened to qualitative description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Bardin, L. Análise de Conteúdo; Edições 70: Lisboa, Portugal, 2022. [Google Scholar]
- Ponterotto, J.G. Qualitative research in counseling psychology: A primer on research paradigms and philosophy of science. J. Couns. Psychol. 2005, 52, 126–136. [Google Scholar] [CrossRef]
- Goodell, L.S.; Stage, V.C.; Cooke, N.K. Practical Qualitative Research Strategies: Training Interviewers and Coders. J. Nutr. Educ. Behav. 2016, 48, 578–585. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef]
- Brown, E.A.; De Young, A.; Kimble, R.; Kenardy, J. The role of parental acute psychological distress in paediatric burn re-epithelialization. Br. J. Health Psychol. 2019, 24, 876–895. [Google Scholar] [CrossRef]
- Stewart, D.; Caradec, J.; Ziegfeld, S.; Reynolds, E.; Ostrander, R.; Parrish, C. Predictors and Correlates of Pediatric Postburn Pruritus in Preschool Children of Ages 0 to 4. J. Burn Care Res. 2019, 40, 930–935. [Google Scholar] [CrossRef]
- Lernevall, L.S.T.; Moi, A.L.; Gjengedal, E.; Dreyer, P. Parents’ lived experience of living with and caring for their burn-injured child in a home setting. Int. J. Qual. Stud. Health Well-Being 2023, 18, 2216032. [Google Scholar] [CrossRef]
- Andrews, N.; Jones, L.L.; Moiemen, N.; Calvert, M.; Kinghorn, P.; Litchfield, I.; Bishop, J.; Deeks, J.J.; Mathers, J. Below the surface: Parents’ views on the factors that influence treatment adherence in paediatric burn scar management—A qualitative study. Burns 2018, 44, 626–635. [Google Scholar] [CrossRef]
- Price, J.; Kassam-Adams, N.; Alderfer, M.A.; Christofferson, J.; Kazak, A.E. Systematic review: A reevaluation and update of the integrative (trajectory) model of pediatric medical traumatic stress. J. Pediatr. Psychol. 2016, 41, 86–97. [Google Scholar] [CrossRef]
- Mohammadzadeh, E.; Varzeshnejad, M.; Masoumpour, A.; Ahmadimehr, F. The impact of the family-centered empowerment model on the children’s quality of life with chemical burns and their parent’s perceived stress. Burns 2023, 49, 838–847. [Google Scholar] [CrossRef]
- Foster, K.; Mitchell, R.; Van, C.; Young, A.; McCloughen, A.; Curtis, K. Resilient, recovering, distressed: A longitudinal qualitative study of parent psychosocial trajectories following child critical injury. Injury 2019, 50, 1605–1611. [Google Scholar] [CrossRef]
- Cartwright, A.V.; Pounds-Cornish, E. The Roles of Clinical Psychologists in Burns Care: A Case Study Highlighting Benefits of Multidisciplinary Care. Eur. Burn J. 2023, 4, 101–107. [Google Scholar] [CrossRef]

{kind=link}
| Parents’ Characteristics | n (%) | Mean (SD) | Range |
|---|---|---|---|
| Age | 46 | 33.54 (5.82) | 22–47 |
| Gender | |||
| Men | 8 (17.4) | ||
| Women | 38 (82.6) | ||
| Residential area | |||
| Urban | 30 (65.2) | ||
| Rural | 16 (34.8) | ||
| Marital status | |||
| Single | 6 (13.0) | ||
| Married | 20 (43.5) | ||
| Living with partner | 19 (41.3) | ||
| Divorced or separated | 1 (2.2) | ||
| Education | |||
| With higher education | 34 (73.9) | ||
| Without higher education | 12 (26.1) | ||
| Employment status | |||
| Inactive | 15 (32.6) | ||
| Active | 31 (67.4) | ||
| Chronic illness | |||
| No | 35 (76.1) | ||
| Yes | 11 (23.9) | ||
| Medication | |||
| No | 33 (71.7) | ||
| Yes | 13 (28.3) | ||
| Witnessed the burn event | |||
| No | 21 (45.7) | ||
| Yes | 25 (54.3) |
| Children’s Characteristics | n (%) | Mean (SD) | Range |
|---|---|---|---|
| Age (in years) | 46 | 2.28 (1.52) | 0.67–6 |
| Gender | |||
| Boys | 28 (60.9) | ||
| Girls | 18 (39.1) | ||
| Number of siblings | 27 | 1.44 (0.80) | 1–4 |
| Enrollment in preschool | |||
| No | 21 (45.7) | ||
| Yes | 25 (54.3) | ||
| Pre-existing medical conditions | |||
| No | 45 (97.8) | ||
| Yes | 1 (2.2) | ||
| Place where the burn occurred | |||
| At home | 44 (95.7) | ||
| Outside the home | 2 (4.3) | ||
| Mechanism of burn | |||
| Scald | 34 (73.9) | ||
| Contact | 4 (8.7) | ||
| Flame | 3 (6.5) | ||
| Friction | 2 (4.3) | ||
| Other (e.g., chemical) | 3 (6.5) | ||
| Number of burn regions sustained | |||
| Single | 13 (28.3) | ||
| Multiple | 33 (71.7) | ||
| Burn depth | |||
| Superficial partial-thickness (2nd degree) | 6 (13.0) | ||
| Deep partial-thickness (2nd degree) | 31 (67.4) | ||
| Full-thickness (3rd degree) | 9 (19.6) | ||
| Visible burns a | |||
| No | 22 (47.8) | ||
| Yes | 24 (52.2) | ||
| Edema | |||
| No | 13 (28.3) | ||
| Yes: Local edema | 33 (71.7) | ||
| Edema texture | |||
| Soft edema | 31 (67.4) | ||
| Hard edema | 2 (4.3) | ||
| Skin graft | |||
| No | 7 (15.2) | ||
| Planned | 39 (84.8) | ||
| Hospital length of stay | |||
| Less than 2 weeks | 8 (17.4) | ||
| 2 weeks or more | 38 (82.6) | ||
| Days since burn injury | 46 | 6.26 (3.09) | 1–17 |
| %TBSA | 46 | 4.71 (3.10) | 1–13 |
| Themes | Sub-Themes (n, %) | Examples |
|---|---|---|
| Diving into the crisis of the child burn injury | Negative trauma responses (44, 95.65%) | “I feel very bad (…) I feel that they look at us like we’re guilty.” (mother of a two-year-old boy) |
| Facing medical procedures (34, 73.91%) | “It was very distressing to see my daughter screaming in pain during the dressing change…” (mother of a ten-month-old girl) | |
| Changes in the child’s functioning (27, 58.70%) | “Because of the bandages on his hands, he can’t do some of the activities he is used to, such as eating, playing with other children…” (mother of a one-year-old boy) | |
| COVID-19 stressors (33, 71.73%) | “(…) a bit apprehensive, afraid that he might get COVID again because that slows down the whole process.” (mother of a five-year-old boy) | |
| Unmet needs (38, 82.61%) | “I miss my family and the support they could give me, for example, here I don’t have anyone to help me feed my daughter. (…) It is in these situations that we see that we’re just the child’s companions…” (mother of a nine-month-old girl) | |
| Being together and in good hands | Child’s well-being and recovery (34, 73.91%) | “The day my daughter (with a facial burn) opened her eyes again was a victory.” (father of a ten-month-old girl) |
| Quality of healthcare and environment (35, 76.09%) | “The medical team made me feel confident (…) The people here in the hospital talk a lot about the experience they’ve had/are having, and that helped me a lot to take it all in.” (mother of a one-year-old boy) | |
| Becoming aware of an uncertain future | Ongoing suffering of the child and (potential) permanent scaring (41, 89.13%) | “I am afraid there will be some rejection from him or his classmates or even bullying episodes. I hope he doesn’t have any physical or emotional marks.” (mother of a six-year-old boy) |
| Concerns about being blamed and that a burn might happen again (8, 17.39%) | “(…) that my daughter blames me when she looks at the scars.” (mother of a one-year-old girl) | |
| Enhancing supportive care and environment | Strengthening support and adapting the care plan (29, 63.04%) | “The food should be more appropriate for children of this age, and we would have more support in this regard, such as helping to feed them, distracting them while they eat, etc.” (father of a three-year-old boy) |
| Improvement of hospital facilities (8, 17.39%) | “We should only have single rooms so that families can have their privacy and feel at ease.” (mother of an 11-month-old boy) | |
| Finding ways to guide parents | Maintaining a positive mindset and activating coping resources (41, 89.13%) | “Have hope that better days will come.” (mother of a one-year-old girl) |
| Recognizing parental distress and promoting a child’s well-being (21, 45.65%) | “This turns out to be more difficult for us than for them.” (mother of a three-year-old boy) | |
| Raising awareness (9, 19.57%) | “People should talk more about this issue of burns, because it happens a lot, especially in children, and you don’t hear about it.” (mother of a one-year-old boy) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, M.; Ferraz, A.; Garcia, M.; Pereira, M.G. Perceptions and Experiences of Parents of Burn-Injured Children during Hospital Stay: A Need for Integrated Care. Healthcare 2024, 12, 614. https://doi.org/10.3390/healthcare12060614
Santos M, Ferraz A, Garcia M, Pereira MG. Perceptions and Experiences of Parents of Burn-Injured Children during Hospital Stay: A Need for Integrated Care. Healthcare. 2024; 12(6):614. https://doi.org/10.3390/healthcare12060614
Chicago/Turabian StyleSantos, Martim, Ana Ferraz, Maria Garcia, and M. Graça Pereira. 2024. "Perceptions and Experiences of Parents of Burn-Injured Children during Hospital Stay: A Need for Integrated Care" Healthcare 12, no. 6: 614. https://doi.org/10.3390/healthcare12060614
APA StyleSantos, M., Ferraz, A., Garcia, M., & Pereira, M. G. (2024). Perceptions and Experiences of Parents of Burn-Injured Children during Hospital Stay: A Need for Integrated Care. Healthcare, 12(6), 614. https://doi.org/10.3390/healthcare12060614