
Association between Post-Hospitalization Psychological Distress, Exercise Capacity, Physical Function and Health Status in COVID-19 Survivors
 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Research Hypothesis
2.2. Design
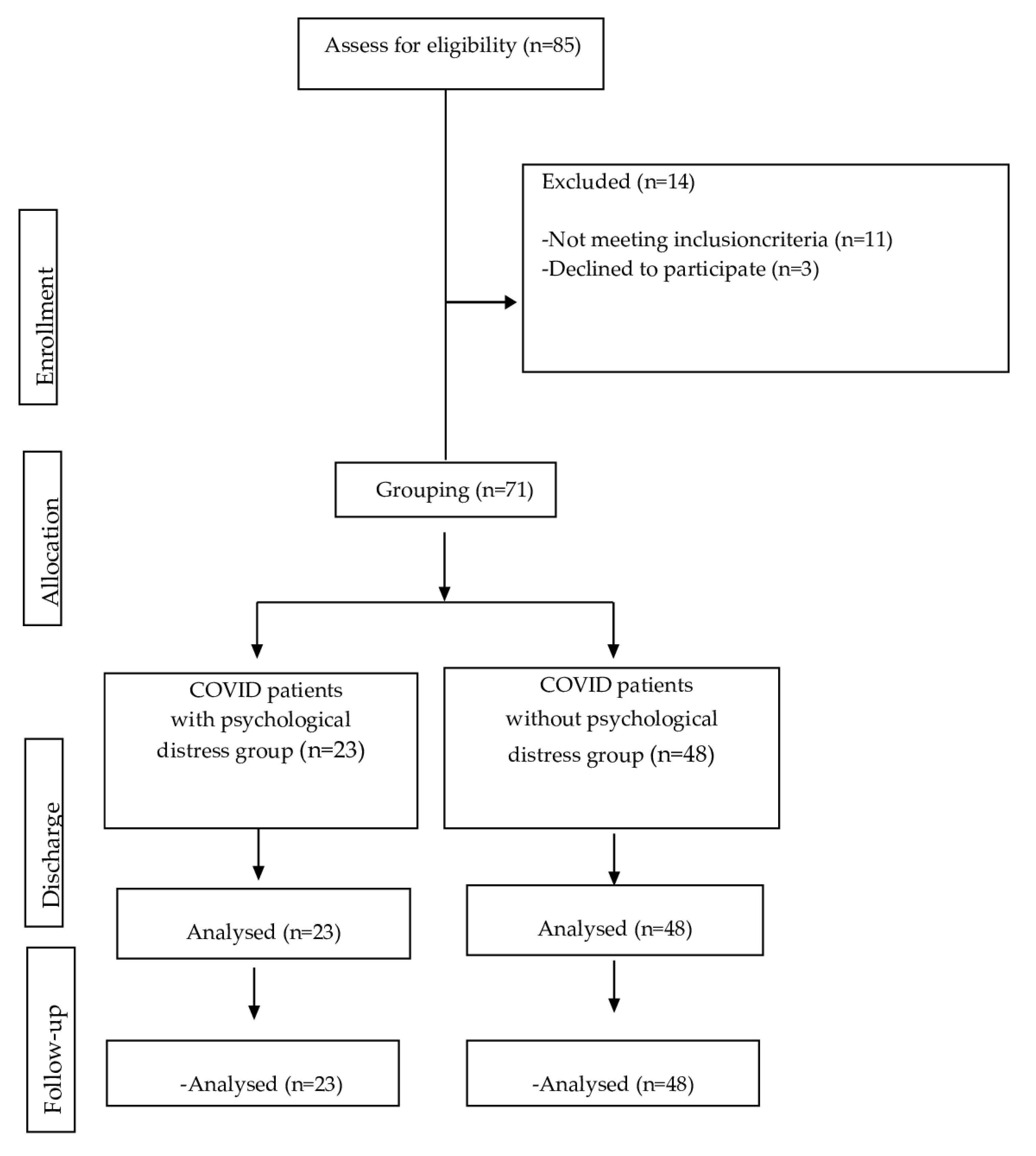
2.3. Participants
2.4. Grouping
2.5. Outcomes
2.5.1. Exercise Capacity
2.5.2. Physical Function
2.5.3. Health Status
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Statista. COVID-26: Número Acumulado de Casos de Coronavirus (COVID-19) en el Mundo, Enero-Marzo [Internet]. Hamburgo: Statista; 26 de Enero de 2024. Available online: https://es.statista.com/estadisticas/1104227/numero-acumulado-de-casos-de-coronavirus-covid-19-en-el-mundo-enero-marzo/#:~:text=COVID%2D26%3A%20n%C3%BAmero%20acumulado%20de,en%20el%20mundo%202020%2D2023&text=A%20fecha%20de%202%20de,geograf%C3%ADa%20europea%20y%20del%20mundo (accessed on 4 January 2024).
- Zhao, S.W.; Li, Y.M.; Li, Y.L.; Su, C. Liver injury in COVID-19: Clinical features, potential mechanisms, risk factors and clinical treatments. World J. Gastroenterol. 2023, 29, 241–256. [Google Scholar] [CrossRef]
- Wang, B.; Yu, Y.; Yu, Y.; Wang, N.; Chen, F.; Jiang, B.; Chen, Y.; Zhang, J.; Liu, J.; Wang, H.; et al. Clinical features and outcomes of hospitalized patients with COVID-19 during the Omicron wave in Shanghai, China. J. Infect. 2023, 86, e27–e29. [Google Scholar] [CrossRef]
- Conti, V.; Corbi, G.; Sabbatino, F.; De Pascale, D.; Sellitto, C.; Stefanelli, B.; Bertini, N.; De Simone, M.; Liguori, L.; Di Paola, I.; et al. Long COVID: Clinical framing, biomarkers, and therapeutic approaches. J. Pers. Med. 2023, 13, 334. [Google Scholar] [CrossRef] [PubMed]
- Lavrentieva, A.; Kaimakamis, E.; Voutsas, V.; Bitzani, M. An observational study on factors associated with ICU mortality in Covid-19 patients and critical review of the literature. Sci. Rep. 2023, 13, 7804. [Google Scholar] [CrossRef] [PubMed]
- Tola, H.H.; Shojaeizadeh, D.; Garmaroudi, G.; Tol, A.; Yekaninejad, M.S.; Ejeta, L.T.; Kebede, A.; Karimi, M.; Kassa, D. Psychological distress and its effect on tuberculosis treatment outcomes in Ethiopia. Glob. Health Action 2015, 8, 29019. [Google Scholar] [CrossRef]
- Spencer-Segal, J.L.; Smith, C.A.; Slavin, A.; Sampang, L.; DiGiovine, D.; Spencer, A.E.; Zhang, Q.; Horowitz, J.; Vaughn, V.M. Mental health outcomes after hospitalization with or without COVID-19. Gen. Hosp. Psychiatry 2021, 72, 152–153. [Google Scholar] [CrossRef]
- Mazza, M.G.; De Lorenzo, R.; Conte, C.; Poletti, S.; Vai, B.; Bollettini, I.; Melloni, E.M.T.; Furlan, R.; Ciceri, F.; Rovere-Querini, P.; et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav. Immun. 2020, 89, 594–600. [Google Scholar] [CrossRef]
- Gutub, A.; Shambour, M.K.; Abu-Hashem, M.A. Coronavirus impact on human feelings during 2021 Hajj season via deep learning critical Twitter analysis. J. Eng. Res. 2023, 11, 100001. [Google Scholar] [CrossRef]
- Huang, H.C.; Huang, L.K.; Hu, C.J.; Chang, C.H.; Lee, H.C.; Chi, N.F.; Shyu, M.L.; Chang, H.J. The mediating effect of psychological distress on functional dependence in stroke patients. J. Clin. Nurs. 2014, 23, 3533–3543. [Google Scholar] [CrossRef] [PubMed]
- Sorel, J.C.; Veltman, E.S.; Honig, A.; Poolman, R.W. The influence of preoperative psychological distress on pain and function after total knee arthroplasty: A systematic review and meta-analysis. Bone Joint J. 2019, 101-B, 7–14. [Google Scholar] [CrossRef]
- Linares-Moya, M.; Rodríguez-Torres, J.; Heredia-Ciuró, A.; Granados-Santiago, M.; López-López, L.; Quero-Valenzuela, F. Psychological distress prior to surgery is related to symptom burden and health status in lung cancer survivors. Support. Care Cancer 2022, 30, 1579–1586. [Google Scholar] [CrossRef]
- Smith, A.B.; Jones, A.D.; Serlachius, A.S.; Johnson, D.W. The impact of acute psychological stress on the immune system: A systematic review. PLoS ONE 2023, 14, e0219821. [Google Scholar]
- Johnson, C.; Smith, L.; Anderson, M. Psychological stress and medication adherence in hospitalized patients. J. Health Psychol. 2020, 25, 673–682. [Google Scholar]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretación de los cuestionarios de salud SF-36 y SF-12 en España: Componentes físico y mental [Interpretation of SF-36 and SF-12 questionnaires in Spain: Physical and mental components]. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Kosinski, M.; Turner-Bowker, D.M.; Gandek, B. How to Score Version 2 of the SF-12 Health Survey (With a Supplement Documenting Version 1); QualityMetric Incorporated: Lincoln, RI, USA, 2002. [Google Scholar]
- Gill, S.C.; Butterworth, P.; Rodgers, B.; Mackinnon, A. Validity of the mental health component scale of the 12-item Short-Form Health Survey (MCS-12) as measure of common mental disorders in the general population. Psychiatry Res. 2007, 152, 63–71. [Google Scholar] [CrossRef]
- Fleishman, J.A.; Selim, A.J.; Kazis, L.E. Deriving SF-12v2 Physical and Mental Health Summary Scores: A Comparison of Different Scoring Algorithms. Qual Life Res. 2010, 19, 231–241. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- American Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Solway, S.; Brooks, D.; Lacasse, Y.; Thomas, S. A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. Chest 2001, 119, 256–270. [Google Scholar] [CrossRef]
- Macchiavelli, A.; Giffone, A.; Ferrarello, F.; Paci, M. Reliability of the six-minute walk test in individuals with stroke: Systematic review and meta-analysis. Neurol. Sci. 2021, 42, 81–87. [Google Scholar] [CrossRef]
- Enright, P.L. The six-minute walk test. Respir. Care 2003, 48, 783–785. [Google Scholar]
- Singh, S.J.; Morgan, M.D.; Scott, S.; Walters, D.; Hardman, A.E. Development of a shuttle walking test of disability in patients with chronic airways obstruction. Thorax 1992, 47, 1019–1024. [Google Scholar] [CrossRef]
- Ingle, L.; Rigby, A.S.; Nabb, S.; Jones, P.K.; Clark, A.L.; Cleland, J.G. Clinical determinants of poor six-minute walk test performance in patients with left ventricular systolic dysfunction and no major structural heart disease. Eur. J. Heart Fail. 2014, 16, 398–406. [Google Scholar] [CrossRef]
- Walker, P.P.; Burnett, A.; Flavahan, P.W.; Calverley, P.M. Lower limb activity and its determinants in COPD. Thorax 2008, 63, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Andrews, A.W. Interrater reliability of hand-held dynamometry. Phys. Ther. 1987, 67, 931–933. [Google Scholar] [CrossRef] [PubMed]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Adair, B.; Pua, Y.H.; Williams, G.P.; McGaw, R.; Clark, R.A. Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: A reliability and validity study. PLoS ONE 2015, 10, e0140822. [Google Scholar] [CrossRef] [PubMed]
- Shephard, R.J.; Montelpare, W.; Plyley, M.; McCracken, D.; Goode, R.C. Handgrip dynamometry, Cybex measurements and lean mass as markers of the ageing of muscle function. Br. J. Sports Med. 1991, 25, 204–208. [Google Scholar] [CrossRef]
- Taekema, D.G.; Gussekloo, J.; Maier, A.B.; Westendorp, R.G.; de Craen, A.J. Handgrip strength as a predictor of functional, psychological and social health. A prospective population-based study among the oldest old. Age Ageing 2010, 39, 331–337. [Google Scholar] [CrossRef]
- Bohannon, R.W. Hand-grip dynamometry predicts future outcomes in aging adults. J. Geriatr. Phys. Ther. 2008, 31, 3–10. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Rodríguez Torres, J.; Cabrera Martos, I.; López López, L.; Torres Sánchez, I.; Granados Santiago, M.; Valenza, M.C. Psychological distress at hospital admission is related to symptoms severity and health status in malignant pleural effusion patients. Eur. J. Cancer Care 2020, 29, e13212. [Google Scholar] [CrossRef] [PubMed]
- Vlake, J.H.; Wesselius, S.; van Genderen, M.E.; van Bommel, J.; Boxma-de Klerk, B.; Wils, E.J. Psychological distress and health-related quality of life in patients after hospitalization during the COVID-19 pandemic: A single-center, observational study. PLoS ONE 2021, 16, e0255774. [Google Scholar] [CrossRef] [PubMed]
- Atlantis, E.; Fahey, P. Cochrane Review: Bidirectional association between depression and chronic disease among women. J. Am. Med. Womens Assoc. 2008, 63, 240–251. [Google Scholar]
- Yohannes, A.M.; Willgoss, T.G.; Baldwin, R.C.; Connolly, M.J. Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: Prevalence, relevance, clinical implications and management principles. Int. J. Geriatr. Psychiatry 2010, 25, 1209–1221. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Collet, J.P.; Shapiro, S.; Lin, Y.; Yang, T.; Platt, R.W.; Wang, C.; Bourbeau, J. Independent effect of depression and anxiety on chronic obstructive pulmonary disease exacerbations and hospitalizations. Am. J. Respir. Crit. Care Med. 2008, 178, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Zhang, W.; Kuo, Y.F.; Sharma, G. Association of Psychological Disorders With 30-Day Readmission Rates in Patients With COPD. Chest 2016, 149, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Herbert, T.B.; Cohen, S. Depression and immunity: A meta-analytic review. Psychol. Bull. 1993, 113, 472–486. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Miller, A.H. Depressive disorders and immunity: 20 years of progress and discovery. Brain Behav. Immun. 2007, 21, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Gudmundsson, G.; Gislason, T.; Janson, C.; Lindberg, E.; Suppli Ulrik, C.; Brøndum, E. Depression, anxiety and health status after hospitalisation for COPD: A multicentre study in the Nordic countries. Respir. Med. 2006, 100, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Pagel, M.D.; Erdly, W.W.; Becker, J. Social networks: We get by with (and in spite of) a little help from our friends. J. Pers. Soc. Psychol. 1987, 53, 793–804. [Google Scholar] [CrossRef]
- Hambisa, S.; Siraj, J.; Mesafint, G.; Yimam, M. Assessment of Psychological Distress and Associated Factors among Hospitalized Patients During the COVID-19 Pandemic at Selected Hospitals in Southwest Ethiopia. Neuropsychiatr. Dis. Treat. 2021, 17, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Saks, B.R.; Glein, R.M.; Jimenez, A.E.; Ankem, H.K.; Sabetian, P.W.; Maldonado, D.R.; Lall, A.C.; Domb, B.G. Patients Obtain Meaningful Clinical Benefit After Hip Arthroscopy Despite Preoperative Psychological Distress: A Propensity-Matched Analysis of Mid-Term Outcomes. Arthroscopy 2022, 38, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Prapa, P.; Papathanasiou, I.V.; Bakalis, V.; Malli, F.; Papagiannis, D.; Fradelos, E.C. Quality of Life and Psychological Distress of Lung Cancer Patients Undergoing Chemotherapy. World J. Oncol. 2021, 12, 61–66. [Google Scholar] [CrossRef]


{kind=link}
| Variable | COVID Patients with Psychological Distress Group (n = 23) | COVID Patients without Psychological Distress Group (n = 48) | p |
|---|---|---|---|
| Age (years) | 56.87 ± 10.70 | 61.63 ± 12.70 | 0.126 |
| Sex (% men) | 78.26 | 95.83 | 0.020 * |
| BMI (kg/m2) | 27.10 ± 3.33 | 30.93 ± 8.48 | 0.008 * |
| Length of hospital stay (days) | 64.74 ± 28.55 | 51.54 ± 31.06 | 0.090 |
| Length of ICU stay (days) | 44.91 ± 25.85 | 21.67 ± 11.90 | <0.001 ** |
| Tabaquism | |||
| Smokers (yes, %) | 39.13 | 0 | |
| Ex-smokers (yes, %) | 17.39 | 41.67 | <0.001 ** |
| Non-smokers (yes, %) | 43.47 | 58.34 | |
| Comorbidities | |||
| Hypertension (yes, %) | 21.73 | 58.33 | 0.004 * |
| Diabetes (yes, %) | 8.69 | 27.08 | 0.076 |
| Cardiovascular diseases (yes, %) | 17.39 | 18.75 | 0.890 |
| Respiratory diseases (yes, %) | 8.69 | 43.75 | 0.003 * |
| Variable | COVID Patients with Psychological Distress Group (n = 23) | COVID Patients without Psychological Distress Group (n = 48) | p |
|---|---|---|---|
| SF-12 total score | 55.29 ± 10.14 | 83.35 ± 16.65 | <0.001 ** |
| Exercise capacity | |||
| 6MWT (meters) | 393.67 ± 73.51 | 441.44 ± 111.12 | 0.225 |
| Borg post-test | 6.44 ± 2.26 | 2.07 ± 1.62 | <0.001 ** |
| Physical function | |||
| Right lower limb (Lb) | 52.66 ± 21.21 | 75.15 ± 30.42 | 0.002 * |
| Left lower limb (Lb) | 38.31 ± 17.36 | 70.75 ± 32.47 | <0.001 ** |
| Health status | |||
| Right upper limb (Lb) | 34.35 ± 13.54 | 43.58 ± 19.87 | 0.048 * |
| Left upper limb (Lb) | 28.60 ± 13.57 | 39.90 ± 22.19 | 0.028 * |
| Variable | COVID Patients with Psychological Distress Group (n = 23) | COVID Patients without Psychological Distress Group (n = 48) | p |
|---|---|---|---|
| SF-12 total score | 61.47 ± 15.20 | 82.47 ± 15.40 | <0.001 ** |
| Exercise capacity | |||
| 6MWT (meters) | 374.10 ± 119.97 | 468.85 ± 101.34 | 0.002 * |
| Borg post-test | 4.70 ± 2.64 | 1.33 ± 1.92 | <0.001 ** |
| Physical function | |||
| Right lower limb (Lb) | 60.90 ± 17.19 | 82.31 ± 27.76 | 0.001 * |
| Left lower limb (Lb) | 62.38 ± 11.34 | 77.91 ± 28.92 | 0.002 * |
| Health status | |||
| Right upper limb (Lb) | 35.52 ± 7.12 | 51.77 ± 20.27 | <0.001 ** |
| Left upper limb (Lb) | 35.53 ± 11.05 | 47.94 ± 23.73 | 0.004 * |
| Variable | COVID Patients with Psychological Distress Group (n = 23) | COVID Patients without Psychological Distress Group (n = 48) | p |
|---|---|---|---|
| SF-12 total score | 70.02 ± 14.20 | 85.20 ± 12.23 | <0.001 ** |
| Exercise capacity | |||
| 6MWT (meters) | 415.15 ± 80.94 | 475.54 ± 107.08 | 0.027 * |
| Borg post-test | 4.70 ± 2.13 | 2.38 ± 2.23 | <0.001 ** |
| Physical function | |||
| Right lower limb (Lb) | 70.81 ± 20.06 | 82.27 ± 28.73 | 0.057 |
| Left lower limb (Lb) | 69.96 ± 15.28 | 81.64 ± 28.05 | 0.027 * |
| Health status | |||
| Right upper limb (Lb) | 64.27 ± 13.42 | 66.73 ± 21.46 | 0.559 |
| Left upper limb (Lb) | 58.56 ± 12.43 | 64.19 ± 27.07 | 0.234 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Ors-Vilardebó, C.; Cebrià i Iranzo, M.À.; González-King-Garibotti, C.; Vázquez-Arce, M.I.; Calvache-Mateo, A.; López-López, L.; Valenza, M.C. Association between Post-Hospitalization Psychological Distress, Exercise Capacity, Physical Function and Health Status in COVID-19 Survivors. Healthcare 2024, 12, 577. https://doi.org/10.3390/healthcare12050577
D’Ors-Vilardebó C, Cebrià i Iranzo MÀ, González-King-Garibotti C, Vázquez-Arce MI, Calvache-Mateo A, López-López L, Valenza MC. Association between Post-Hospitalization Psychological Distress, Exercise Capacity, Physical Function and Health Status in COVID-19 Survivors. Healthcare. 2024; 12(5):577. https://doi.org/10.3390/healthcare12050577
Chicago/Turabian StyleD’Ors-Vilardebó, Clara, Maria Àngels Cebrià i Iranzo, Carola González-King-Garibotti, María Isabel Vázquez-Arce, Andrés Calvache-Mateo, Laura López-López, and Marie Carmen Valenza. 2024. "Association between Post-Hospitalization Psychological Distress, Exercise Capacity, Physical Function and Health Status in COVID-19 Survivors" Healthcare 12, no. 5: 577. https://doi.org/10.3390/healthcare12050577
APA StyleD’Ors-Vilardebó, C., Cebrià i Iranzo, M. À., González-King-Garibotti, C., Vázquez-Arce, M. I., Calvache-Mateo, A., López-López, L., & Valenza, M. C. (2024). Association between Post-Hospitalization Psychological Distress, Exercise Capacity, Physical Function and Health Status in COVID-19 Survivors. Healthcare, 12(5), 577. https://doi.org/10.3390/healthcare12050577