
The Role of Carotid-Femoral Pulse Wave Velocity in a Metabolic Syndrome Patient with Sudden Cardiac Arrest: A Case Report




Abstract
1. Introduction
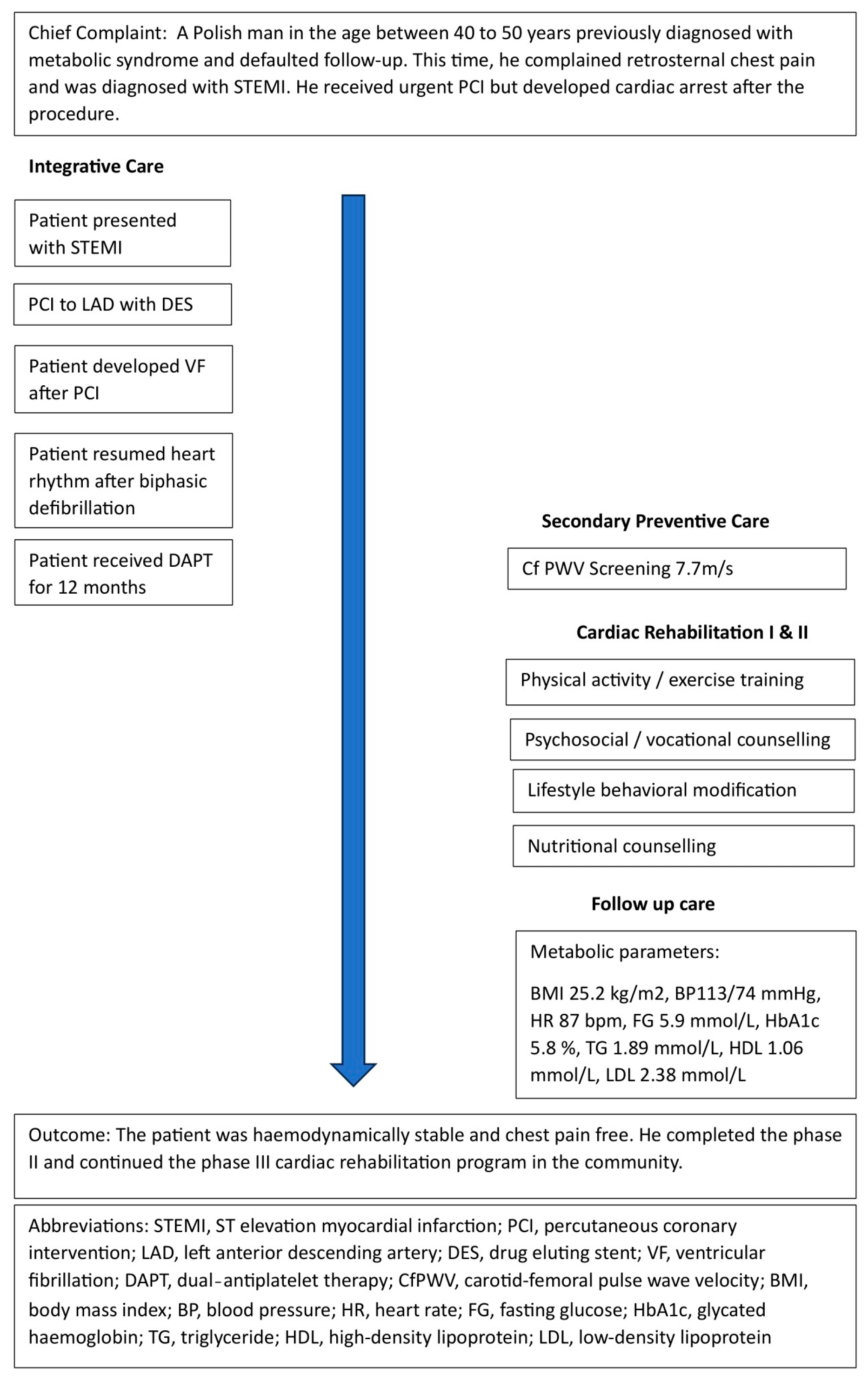
2. Patient Information
2.1. History
2.2. Therapeutic Intervention
2.3. Follow-Up and Outcomes
3. Discussion
Learning Points
- The current case report demonstrated a positive relationship between MetS and SCA.
- MetS increased irreversible arterial stiffness, which may be asymptomatic for patients with borderline conventional cardiovascular risk factors.
- PWV provides additional risk information over the conventional cardiovascular risk stratification.
- PWV screening can be relevant to identify subclinical atherosclerosis in asymptomatic population with MetS.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BaPWV | Brachial-ankle pulse wave velocity |
| CfPWV | Carotid-femoral pulse wave velocity |
| DES | Drug eluting stent |
| ePWV | Estimated PWV |
| HDL | High-density lipoprotein |
| LAD | Left anterior descending artery |
| MetS | Metabolic syndrome |
| MET | Metabolic equivalents |
| PCI | Percutaneous coronary intervention |
| PWV | Pulse wave velocity |
| SCA | Sudden cardiac arrest |
| SCORE | Systematic Coronary Risk Evaluation |
| STEMI | ST Elevation Myocardial Infarction |
| TIMI | Thrombolysis In Myocardial Infarction |
References
- Tougaard, N.H.; Theilade, S.; Winther, S.A.; Tofte, N.; Ahluwalia, T.S.; Hansen, T.W.; Rossing, P.; Frimodt-Møller, M. Carotid-Femoral Pulse Wave Velocity as a Risk Marker for Development of Complications in Type 1 Diabetes Mellitus. J. Am. Heart Assoc. 2020, 9, e017165. [Google Scholar] [CrossRef]
- Townsend, R.R.; Wilkinson, I.B.; Schiffrin, E.L.; Avolio, A.P.; Chirinos, J.A.; Cockcroft, J.R.; Heffernan, K.S.; Lakatta, E.G.; McEniery, C.M.; Mitchell, G.F.; et al. Recommendations for improving and standardizing vascular research on arterial stiffness: A scientific statement from the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef]
- Wilkinson, I.B.; Mäki-Petäjä, K.M.; Mitchell, G.F. Uses of arterial stiffness in clinical practice. Arterioscler. Thromb. Vasc. Biol. 2020, 5, 1063–1067. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Wang, Q.; Cheng, D.; Hu, Y.; Chao, H.; Avolio, A.; Tang, B.; Zuo, J. Comparison of Risk of Target Organ Damage in Different Phenotypes of Arterial Stiffness and Central Aortic Blood Pressure. Front. Cardiovasc. Med. 2022, 9, 839875. [Google Scholar] [CrossRef] [PubMed]
- Tirandi, A.; Carbone, F.; Montecucco, F.; Liberale, L. The role of metabolic syndrome in sudden cardiac death risk: Recent evidence and future directions. Eur. J. Clin. Investig. 2022, 52, e13693. [Google Scholar] [CrossRef] [PubMed]
- Hess, P.L.; Al-Khalidi, H.R.; Friedman, D.J.; Mulder, H.; Kucharska-Newton, A.; Rosamond, W.R.; Lopes, R.D.; Gersh, B.J.; Mark, D.B.; Curtis, L.H.; et al. The Metabolic Syndrome and Risk of Sudden Cardiac Death: The Atherosclerosis Risk in Communities Study. J. Am. Hear. Assoc. 2017, 6, 006103. [Google Scholar] [CrossRef] [PubMed]
- Stepaniak, U.; Micek, A.; Waśkiewicz, A.; Bielecki, W.; Drygas, W.; Janion, M.; Kozakiewicz, K.; Niklas, A.; Puch-Walczak, A.; Pająk, A. Prevalence of general and abdominal obesity and overweight among adults in Poland. Results of the WOBASZ II study (2013–2014) and comparison with the WOBASZ study (2003–2005). Pol. Arch. Intern. Med. 2016, 126, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Dobrowolski, P.; Prejbisz, A.; Kuryłowicz, A.; Baska, A.; Burchardt, P.; Chlebus, K.; Dzida, G.; Jankowski, P.; Jaroszewicz, J.; Jaworski, P.; et al. Metabolic syndrome—A new definition and management guidelines. Arter. Hypertens. 2022, 26, 99–121. [Google Scholar] [CrossRef]
- Butlin, M.; Qasem, A. Large Artery Stiffness Assessment Using SphygmoCor Technology. Pulse 2016, 4, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Piotrowicz, R.; Jagier, A.; Szalewska, D.; Wolszakiewicz, J.; Piotrowicz, E.; Smolis-Bąk, E.; Dylewicz, P.; Eysymontt, Z.; Gałaszek, M.; Łazorczyk, M.; et al. Rekomendacje w Zakresie Realizacji Kompleksowej Rehabilitacji Kardiologicznej: Stanowisko Ekspertów Sekcji Rehabilitacji Kardiologicznej i Fizjologii Wysiłku Polskiego Towarzystwa Kardiologicznego; AsteriaMed Wydawnictwo: Gdańsk, Poland, 2017. [Google Scholar]
- Kim, Y.G.; Han, K.; Jeong, J.H.; Roh, S.Y.; Choi, Y.Y.; Min, K.; Shim, J.; Choi, J.I.; Kim, Y.H. Metabolic syndrome, gamma-glutamyl transferase, and risk of sudden cardiac death. J. Clin. Med. 2022, 11, 1781. [Google Scholar] [CrossRef]
- Li, D.; Cao, F.; Cheng, W.; Xu, Y.; Yang, C. Predictive value of estimated pulse wave velocity for cardiovascular and all-cause mortality in individuals with obesity. Diabetol. Metab. Syndr. 2023, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Masrouri, S.; Moazzeni, S.S.; Cheraghloo, N.; Azizi, F.; Hadaegh, F. The clinical value of metabolic syndrome and its components with respect to sudden cardiac death using different definitions: Two decades of follow-up from the Tehran Lipid and Glucose Study. Cardiovasc. Diabetol. 2022, 21, 269. [Google Scholar] [CrossRef]
- Skrypnik, D.; Skrypnik, K.; Suliburska, J.; Bogdański, P. Cardiac rehabilitation may influence leptin and VEGF A crosstalk in patients after acute coronary syndrome. Sci. Rep. 2022, 12, 11825. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.-P.; Wang, J.-H.; Chen, M.-L.; Yang, C.-F.; Chen, Y.-C.; Hsu, B.-G. Association of serum leptin levels with central arterial stiffness in coronary artery disease patients. BMC Cardiovasc. Disord. 2016, 16, 80. [Google Scholar] [CrossRef]
- van Hout, M.J.; Dekkers, I.A.; Westenberg, J.J.; Schalij, M.J.; Widya, R.L.; de Mutsert, R.; Rosendaal, F.R.; de Roos, A.; Jukema, J.W.; Scholte, A.J.; et al. Normal and reference values for cardiovascular magnetic resonance-based pulse wave velocity in the middle-aged general population. J. Cardiovasc. Magn. Reson. 2021, 23, 1–10. [Google Scholar] [CrossRef]
- Sofogianni, A.; Stalikas, N.; Antza, C.; Tziomalos, K. Cardiovascular Risk Prediction Models and Scores in the Era of Personalized Medicine. J. Pers. Med. 2022, 12, 1180. [Google Scholar] [CrossRef] [PubMed]
- Adamkiewicz, K.; Płatek, A.E.; Szymański, F.M. Risk assessment according to the SCORE risk chart—From history, through present, to the future. Kardiol. Pol. 2018, 76, 63–68. [Google Scholar] [CrossRef]
- SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [CrossRef]
- Townsend, R.R. Arterial Stiffness: Recommendations and Standardization. Pulse 2016, 4, 3–7. [Google Scholar] [CrossRef]
- Wentland, A.L.; Grist, T.M.; Wieben, O. Review of MRI-based measurements of pulse wave velocity: A biomarker of arterial stiffness. Cardiovasc. Diagn. Ther. 2014, 4, 193–206. [Google Scholar] [CrossRef]
- Kolkenbeck-Ruh, A.; Soepnel, L.M.; Kim, A.W.; Naidoo, S.; Smith, W.; Davies, J.; Ware, L.J. Pulse wave velocity in South African women and children: Comparison between the Mobil-O-Graph and SphygmoCor XCEL devices. J. Hypertens. 2022, 40, 65. [Google Scholar] [CrossRef]
- Podrug, M.; Šunjić, B.; Koren, P.; Đogaš, V.; Mudnić, I.; Boban, M.; Jerončić, A. What Is the Smallest Change in Pulse Wave Velocity Measurements That Can Be Attributed to Clinical Changes in Arterial Stiffness with Certainty: A Randomized Cross-Over Study. J. Cardiovasc. Dev. Dis. 2023, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-L.; Kim, S.-H. Pulse Wave Velocity in Atherosclerosis. Front. Cardiovasc. Med. 2019, 6, 41. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). G Ital. Cardiol. 2018, 19, 3S–73S. [Google Scholar]
- Podolec, M.; Siniarski, A.; Pająk, A.; Rostoff, P.; Gajos, G.; Nessler, J.; Olszowska, M.; Nowakowski, M.; Szafraniec, K.; Kopeć, G. Association between carotid-femoral pulse wave velocity and overall cardiovascular risk score assessed by the SCORE system in urban Polish population. Kardiol. Pol. 2019, 77, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Spronck, B.; Terentes-Printzios, D.; Avolio, A.P.; Boutouyrie, P.; Guala, A.; Jerončić, A.; Laurent, S.; Barbosa, E.C.D.; Baulmann, J.; Chen, C.H. 2024 Recommendations for Validation of Noninvasive Arterial Pulse Wave Velocity Measurement Devices. Hypertension 2024, 81, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Park, J.B.; Sharman, J.E.; Li, Y.; Munakata, M.; Shirai, K.; Chen, C.-H.; Jae, S.Y.; Tomiyama, H.; Kosuge, H.; Bruno, R.M.; et al. Expert Consensus on the Clinical Use of Pulse Wave Velocity in Asia. Pulse 2022, 10, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Luengo-Fernandez, R.; Walli-Attaei, M.; Gray, A.; Torbica, A.; Maggioni, A.P.; Huculeci, R.; Bairami, F.; Aboyans, V.; Timmis, A.D.; Vardas, P.; et al. Economic burden of cardiovascular diseases in the European Union: #a population-based cost study. Eur. Hear. J. 2023, 44, 4752–4767. [Google Scholar] [CrossRef]
- Mela, A.; Rdzanek, E.; Poniatowski, A.; Jaroszyński, J.; Furtak-Niczyporuk, M.; Gałązka-Sobotka, M.; Olejniczak, D.; Niewada, M.; Staniszewska, A. Economic Costs of Cardiovascular Diseases in Poland Estimates for 2015–2017 Years. Front. Pharmacol. 2020, 11, 1231. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | In Emergency Department | In Follow-Up Clinic |
|---|---|---|
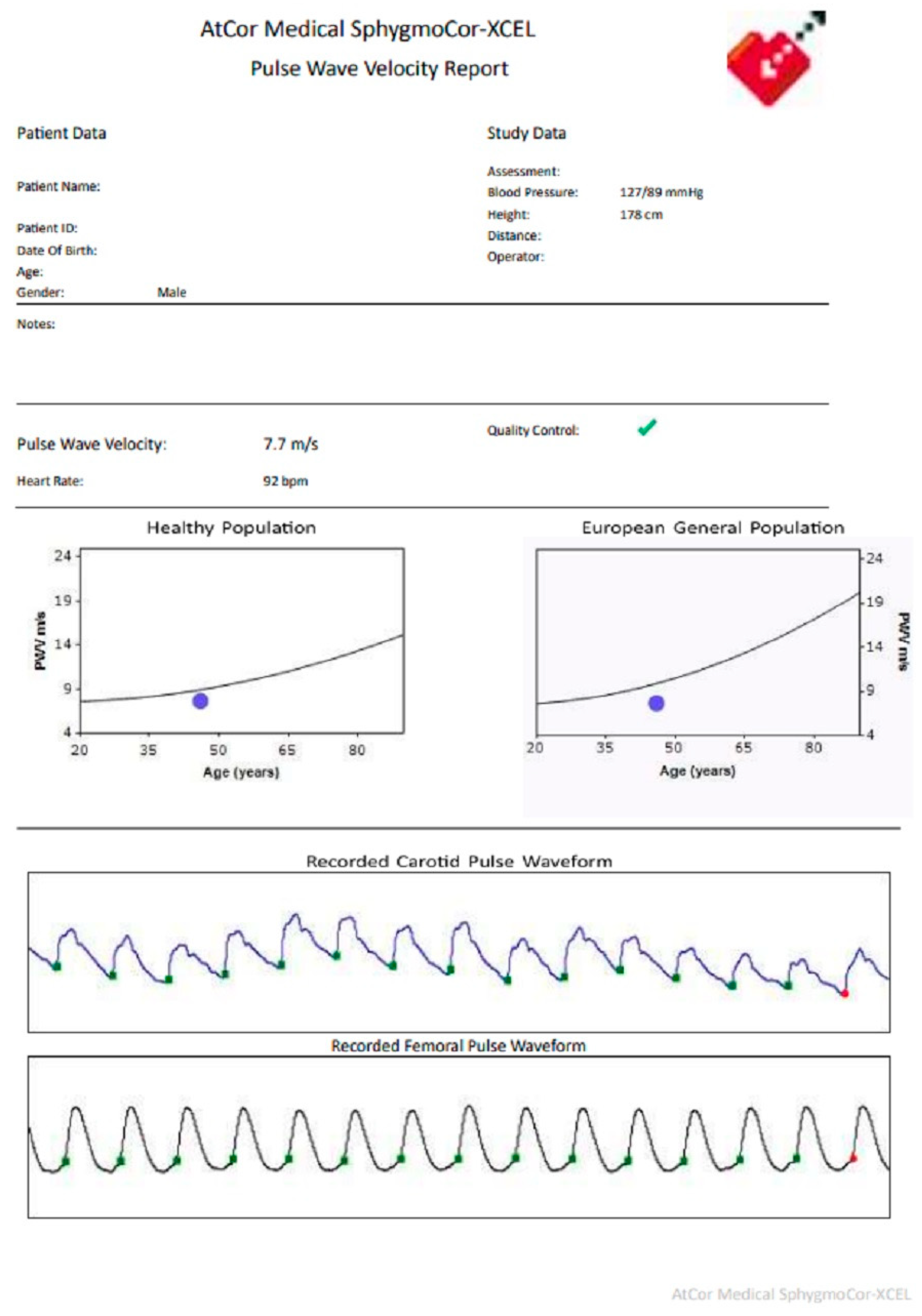
| Carotid-femoral pulse wave velocity (CfPWV) m/s | Not available | 7.7 |
| Body weight (kg) | 80 | 78 |
| Height (cm) | 178 | 178 |
| Body mass index (kg/m2) | 25.83 | 25.2 |
| Blood pressure (mmHg) | 143/104 | 113/74 |
| Heart rate (bpm) | 89 | 87 |
| Random glucose (mmol/L) | 9.2 | Not available |
| Fasting glucose (mmol/L) | Not available | 5.9 |
| Glycated haemoglobin (HbA1c)(%) | Not available | 5.8 |
| Triglyceride (mmol/L) | 2.72 | 1.89 |
| High-density lipoprotein (HDL)(mmol/L) | 0.98 | 1.06 |
| Low-density lipoprotein (LDL)(mmol/L) | 1.94 | 2.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choy, H.K.; Bogdański, P.; Skrypnik, D. The Role of Carotid-Femoral Pulse Wave Velocity in a Metabolic Syndrome Patient with Sudden Cardiac Arrest: A Case Report. Healthcare 2024, 12, 491. https://doi.org/10.3390/healthcare12040491
Choy HK, Bogdański P, Skrypnik D. The Role of Carotid-Femoral Pulse Wave Velocity in a Metabolic Syndrome Patient with Sudden Cardiac Arrest: A Case Report. Healthcare. 2024; 12(4):491. https://doi.org/10.3390/healthcare12040491
Chicago/Turabian StyleChoy, Hau Kim, Paweł Bogdański, and Damian Skrypnik. 2024. "The Role of Carotid-Femoral Pulse Wave Velocity in a Metabolic Syndrome Patient with Sudden Cardiac Arrest: A Case Report" Healthcare 12, no. 4: 491. https://doi.org/10.3390/healthcare12040491
APA StyleChoy, H. K., Bogdański, P., & Skrypnik, D. (2024). The Role of Carotid-Femoral Pulse Wave Velocity in a Metabolic Syndrome Patient with Sudden Cardiac Arrest: A Case Report. Healthcare, 12(4), 491. https://doi.org/10.3390/healthcare12040491